
Abstract
Background:
The pattern and distribution of tears for the complete discoid lateral meniscus (DLM) are not well documented.
Purpose:
To investigate the prevalence and pattern of tear types for the complete DLM using magnetic resonance imaging (MRI) and arthroscopic data.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
We reviewed consecutive series of 1219 patients (1406 knees) who underwent arthroscopic knee surgery for any pathology and were diagnosed with DLM between January 1998 and December 2022. After excluding cases with incomplete DLM (774 knees) and previous history of ipsilateral knee surgery (55 knees), a total of 486 patients (577 knees; mean age, 37.4 years; range, 5-76 years) with complete DLM were evaluated. Preoperative MRI and intraoperative arthroscopic findings were analyzed to classify tears into the following: peripheral tear—including bucket-handle tear; horizontal tear; radial tear; flap tear; and no tear. In addition, preoperative MRI was used to categorize 2 distinct morphological variants of complete DLM: (1) a block-shaped type with a thick blunt free edge; and (2) a wedge-shaped type with a tapering sharp free edge.
Results:
When categorized by meniscal morphology, 435 knees (75.4%) were classified as block-type and 142 knees (24.6%) as wedge-type complete DLM. Peripheral tears (66.7%) were the most prevalent in the block type, followed by horizontal tears (22.5%) and radial tears (0.7%). In the wedge type, horizontal tears (43%) were observed most frequently, followed by radial tears (18.3%), peripheral tears (11.3%), and flap tears (5.6%).
Conclusion:
A block-shaped morphology was the predominant form of complete DLM in this cohort of operatively treated patients. The wedge-type morphology had a distinctly different tear pattern, with horizontal tears being the most common. While the block type exhibited either a peripheral or horizontal tear, the wedge type was characterized by a greater variation in tear pattern.
A discoid lateral meniscus (DLM) involves both structural and morphological anomalies, 18 and its incidence is estimated to be between 0.4% and 17%, depending on the studied population.12,14,15,17,20,23,26,27 There is a wide-ranging spectrum of clinical manifestations. 2 A DLM can often be asymptomatic, but symptoms can occur at any age. 9 Variability is also present in its morphology, from a nearly normal-looking meniscus with minimal differences in width and height, to conspicuously thickened and displaced abnormal menisci.15,22
Traditionally, the Watanabe classification of DLM has been used, in which a complete DLM is a block-shaped meniscus covering the entire tibial plateau, an incomplete DLM is a semilunar-shaped meniscus covering up to 80% of the tibial plateau, and an unstable (Wrisberg-type) DLM lacks the usual posterior attachments, with only the posterior meniscofemoral ligament (Wrisberg ligament) as the anchor. 31 However, the classification scheme has shown incompatibility with concomitant meniscal tears, meniscal shifts, and abnormal height or thickness.1,8,21 Consequently, various authors have proposed additional classification systems that are based on peripheral rim instability and the presence or absence of meniscal tears.13,16,19 A more recently developed system has identified meniscal width, height, peripheral stability, and meniscal tear as the main features providing the basis for classification. 21 This evolving trend reflects the growing understanding of the complex nature of DLM.
Histological studies investigating the microstructure of DLM have shown the collagen fibers to have an aberrant orientation and significant disorganization compared with the circumferential arrangement of a normal lateral meniscus. It has been postulated that such distorted anatomy may diminish the capacity of the meniscus for dissipating hoop stress, thus negatively affecting normal knee biomechanics. The difference in anatomy may also lead to differences in tear pattern and even a difference in prognosis due to the variation in vasculature and subsequent healing potential of meniscal tissue. In particular, pediatric patients with a complete DLM have been reported to be 4.5 times more likely to require surgical intervention compared with those with an incomplete DLM, 25 highlighting the role that meniscal morphology may play in the pathophysiology of DLM.
While previous studies have shown that complete and incomplete DLM have significant differences in tear pattern,6,10 the literature specifically addressing tear distribution of complete DLM remains notably absent. In the present study, we aimed to bridge this gap by investigating the prevalence and pattern of meniscal tear types in patients with complete DLM utilizing a comprehensive dataset comprising magnetic resonance imaging (MRI) and arthroscopic findings from a high-volume tertiary center. We hypothesized that a difference in morphology of the complete DLM would be associated with a difference in tear pattern.
Methods
Institutional review board approval for the study protocol was obtained. We reviewed the medical records, radiographic studies, and arthroscopic imaging data of all consecutive patients who underwent arthroscopic knee surgery and were diagnosed with DLM between January 1998 and December 2022 at a single high-volume tertiary center. Diagnosis of DLM was based on a minimal width of >15 mm on coronal-plane MRI and ≥3 consecutive 5 mm-thick sagittal MRI slices showing continuity between the anterior and posterior horns of the lateral meniscus.3,28 The inclusion criteria were (1) confirmed diagnosis of complete DLM; (2) availability of preoperative knee MRI and intraoperative arthroscopic images; and (3) no previous history of ipsilateral knee surgery.
Initially, 1219 patients (1406 knees) were identified, and after excluding cases with incomplete DLM (774 knees) and previous history of ipsilateral knee surgery (55 knees), a total of 486 patients (577 knees) with complete DLM were included in this study (Figure 1). There were no cases of Wrisberg-type DLM. Overall, the mean patient age at the time of surgery was 37.4 ± 17.5 years (range, 5-76 years). There were 158 male (182 knees) and 328 female patients (395 knees) (Table 1). Surgery was performed on 280 right knees and 297 left knees, and 91 patients received surgery for bilateral DLM.

A flow chart of patient selection and complete DLM groups (No. of knees) according to meniscal morphology. DLM, discoid lateral meniscus.
Patient Characteristics a

Values are presented as mean ± SD or No. of knees (%). DLM, discoid lateral meniscus.
Fisher exact test or paired t test.
The location, size, and shape of meniscal tears were systematically assessed during arthroscopic examination. Based on preoperative MRI and arthroscopic findings, tears were classified into peripheral tears, horizontal tears, radial tears, flap tears, or no tears. Bucket-handle tears were considered peripheral tears, as they represent an unstable and displaced peripheral tear.
In addition, preoperative MRI was used to categorize 2 distinct morphological variants of complete DLM: (1) a block-shaped type with a thick central portion and blunt free edge; and (2) a wedge-shaped type with a tapering central portion and sharp free edge. This morphologic variation was best observed on coronal MRI images through the midbody portion of the meniscus (Figure 2). Meniscal and bony dimensions can vary depending on sex, height, and race; thus, instead of a system based on specific measurements, categorization based on morphological traits that can be intuitively recognized was adopted for ease of clinical application.

Coronal MRI scans of the right knee of (A) a 15-year-old female patient demonstrating block-type complete DLM with a thick blunt free edge and (B) a 40-year-old male patient with wedge-type complete DLM that tapers centrally toward a sharp free edge. DLM, discoid lateral meniscus; MRI, magnetic resonance imaging.
To assess the intra- and interobserver reliability of the MRI assessments, 50 knees were randomly selected, and the analysis of the images was performed by 2 clinical orthopaedic fellows (H.Y.K., J.R.).
Statistical Analysis
The primary outcome was the type of meniscal tear. Significant differences in categorical variables between the block-type and wedge-type groups were compared using the Fisher exact test or paired t test as appropriate. P < .05 was considered statistically significant. To evaluate reliability in the MRI assessments, the Cohen kappa coefficient was used for interobserver reliability and the weighted kappa coefficient was used for intraobserver reliability. Data were analyzed using Statistical Package for the Social Sciences software Version 21.0 (IBM Corp).
Results
Based on DLM morphology, 435 knees (75.4%) were classified as block type and 142 knees (24.6%) as wedge type (Table 2). In the block type, peripheral tears (66.7%) were the most prevalent (Figure 3), followed by horizontal tears (22.5%) and radial tears (0.7%). In the wedge type, horizontal tears (43%) were observed most frequently (Figure 4), followed by radial tears (18.3%), peripheral tears (11.3%), and flap tears (5.6%). In addition, 10.1% of the block type and 21.8% of the wedge type did not have meniscal tears (Figure 5). There was a statistically significant difference in the tear pattern distribution between the 2 morphologic variants. Sex, age at surgery, and laterality were not significantly different between the 2 groups.
Meniscal Tear Pattern and Distribution a

Values are presented as No. of knees (%). Bold P values indicate a statistically significant difference between block- and wedge-type morphology (P < .05, Fisher exact test). DLM, discoid lateral meniscus.
Including bucket-handle tear.

Coronal MRI scans of 4 different patients. Peripheral and bucket-handle tears were prevalent in the block-type complete DLM and showed varying amounts of displacement. DLM, discoid lateral meniscus; MRI, magnetic resonance imaging.

Horizontal tears were the most common form of tear in the wedge-type complete DLM. DLM, discoid lateral meniscus.
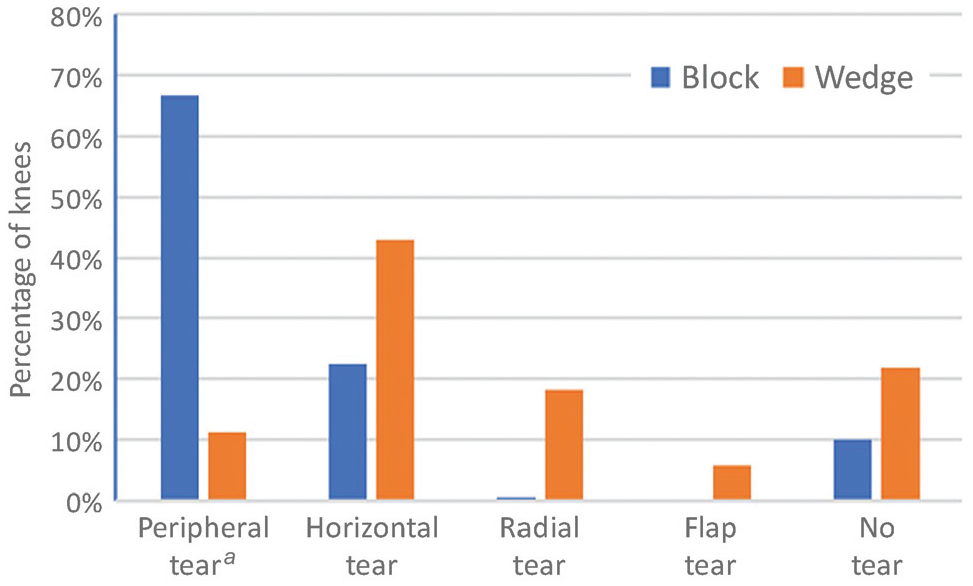
Distribution of tears in block-type versus wedge-type complete DLM. a Peripheral tears included bucket-handle tears. DLM, discoid lateral meniscus.
In the assessment of rater agreement regarding tear pattern and meniscal morphology on MRI, the Cohen kappa coefficient for interobserver reliability was 0.89 and 0.92 respectively, and the weighted kappa coefficient for intraobserver reliability was 0.97 and 0.93, respectively, indicating near-perfect agreement in all cases.
Discussion
The most important finding of this study was that complete DLM followed a distinct tear pattern depending on meniscal morphology. Notably, we observed that the block-shaped morphology predominated with 75.4% of knees assessed, while the wedge-shaped morphology accounted for the remaining 24.6% of knees. With block-type DLM, peripheral tears were overwhelmingly prevalent, constituting 66.7% of observed tears, followed by horizontal tears at 22.5%; the other tear types were negligible. In contrast, wedge-type DLM exhibited a noticeably more diverse and varied tear pattern, with horizontal tears being the most common at 43%, followed by radial tears (18.3%), peripheral tears (11.3%), and flap tears (5.6%). This dichotomy in tear patterns suggests that the structural differences between these morphological variants may influence the biomechanical stress distribution and susceptibility to specific types of tears. Bin et al 6 reported that the extent of meniscal resection in DLM tears was dependent on the tear pattern, and that subtotal or total meniscectomy was performed significantly more frequently in longitudinal/peripheral tears. Thus, block-type complete DLM, with its higher prevalence of peripheral tears, can be assumed to be at higher risk for increased meniscal resection when receiving surgical treatment.
Histological studies have shown irregularly oriented collagen fibers in the DLM.4,7,30 Papadopoulos et al 24 demonstrated the marked disorganization and heterogeneous course of the circumferentially arranged collagen network in DLM compared with the normal meniscus. 24 Such a distorted anatomy may hinder the meniscus’ ability to absorb load and dissipate hoop stress effectively and be more susceptible to injury. Moreover, the disorganized collagen matrix may not function as efficiently as a scaffold to hole the glycosaminoglycans necessary for normal meniscal function. 30 Differences in the microstructure (collagen network) and macrostructure (meniscus morphology) may contribute to the variation in tear pattern. 4
A recently developed DLM classification system from the Pediatric Research in Sports Medicine (PRiSM) group 21 distinguished between normal and abnormal meniscal height. However, the authors did not discuss the implications of the height difference. 5 Our study sheds light on the ramifications of DLM with markedly increased height, as this can be considered an equivalent of the block type. Meniscal height is a key characteristic of DLM that has until now been neglected in most classification systems,1,13,19 and the proposed binary distinction is a simple and effective method to categorize this morphologic variation.
There was an absence of tears in 10.1% of block-type and 21.8% of wedge-type complete DLM. These patients were diagnosed with DLM incidentally while receiving treatment for a different pathology of the knee such as ligament injury or medial meniscal tears. Because of the high proportion of asymptomatic patients, determining the true incidence of DLM and the prevalence of symptomatic DLM remains elusive.29,32
The findings of this study underscore the importance of preoperative MRI evaluation for characterizing DLM morphology, as it can aid in surgical planning by providing a roadmap for expected tear patterns. The ability to anticipate tear types based on meniscal morphology may contribute to more tailored surgical approaches and personalized treatment strategies.
Limitations
This study has several limitations. Because the study was limited to patients who were diagnosed with DLM by both MRI and arthroscopic examination, patients who did not undergo surgery were not included; thus, the presented findings may not apply to patients with DLM who were treated nonoperatively. Also, the retrospective nature of the study may introduce bias and confounding variables that were not controlled for during initial data collection. In addition, the study was conducted at a single high-volume tertiary center, which may limit the generalizability of the results because the study population was not representative of the broader population. Also, the definitions for block- and wedge-type menisci are not based on objective and precise measurements but rather are descriptive. However, we believe that this is an intuitive and easily usable method that showed high intra- and interobserver reliability.
The results of this study suggest that in most cases, block-type complete DLM is torn in 1 of 2 ways: horizontally and peripherally. Cho et al 11 reported that horizontal DLM tears, even if left untreated and observed, often do not lead to significant cartilage damage for an extended period compared with other types of tears, suggesting a relatively benign prognosis. Further research focusing on the clinical outcomes of peripheral tears of complete DLM is necessary to gain additional insight.
Conclusion
A block-shaped morphology was the predominant form of complete DLM in this cohort of operatively treated patients. The wedge-type morphology had a distinctly different tear pattern, with horizontal tears being the most common. While the block type exhibited either a peripheral or horizontal tear, the wedge type was characterized by a greater variation in tear pattern.
Footnotes
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Asan Medical Center (reference No. 2023-0967).