
Abstract
Background:
Few investigations have examined dance-specific injury prevention programs (IPPs), and no published randomized controlled trials are available that evaluate IPPs for dance.
Hypothesis:
The implementation of an IPP will significantly reduce the risk of injury in professional ballet dancers.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
A randomized controlled trial was designed that entailed a superiority model for the intervention group. All professional dancers from a single ballet company were eligible to participate. Randomization and allocation were performed before the start of the season. The control group practiced and performed without change to preexisting standard operating practice. The IPP group was instructed to perform a 30-minute exercise program 3 times per week over the 52-week study period. Injuries were recorded. Standard continuous and categorical data comparisons and correlations were used. Cox proportional hazards regression models for recurrent failures were used wherein the hazard ratio indicates the relative likelihood of injury in the control versus intervention groups.
Results:
Of the 52 eligible dancers, 75% (n = 39) participated. Of these 39 dancers, 19 (9 males, 10 females; mean age, 26.6 ± 4.0 years) were randomized to the control group and 20 (11 males, 9 females; mean age, 25.1 ± 5.1 years) to the IPP group. No significant (P > .05) difference was found in baseline demographics between groups. A total of 116 injuries were recorded for the entire study population (49 IPP; 67 control). Traumatic and chronic injuries accounted for 54% and 46% of injuries, respectively. The injury rate was 82% less (IPP hazard ratio, 0.18; z = –2.29; P = .022) in the IPP group after adjustment for confounding variables, and time between injuries was 45% longer (IPP hazard ratio, 0.55; z = –2.20; P = .028) than for controls.
Conclusion:
The present study is the first prospective randomized controlled investigation of an IPP for professional ballet. The results showed an 82% decrease in injury rate for the intervention group and an extended period from previous injury to subsequent injury.
Registration:
NCT04110002 (ClinicalTrials.gov identifier).
Dancers experience a variety of musculoskeletal injuries, and most dancers will experience at least 1 significant injury in their career. 13,42,48 The type and incidence of dance injuries are relatively well-represented in the literature, but limited literature is available regarding the cause of those injuries. ‡ The most common injuries that dancers sustain are those of the lower extremity and lower back. 42,48 The most common diagnoses include lumbar strain, ankle sprain, Achilles tendinitis, metatarsal stress fracture, posterior tibialis strain, and hip strain. 42 Causes of injury are thought to include muscular fatigue, muscular imbalance, and balance deficits. 3,12,14,26,27,32,45 Dancers have higher rates of certain anatomic conditions such as hypermobility, hip dysplasia, and hip microinstability. 16,17,36 Prior reports from the same dance company have shown hip instability and dysplasia in nearly 90% of dancers. 17,36 These conditions induce abductor fatigue and hip microinstability, which can be improved by strengthening the core and periarticular musculature. 16,25 Core strengthening also has been shown to decrease rates of back and lower extremity injury. 22,25,45,57 Furthermore, improved balance and lower extremity muscular strength are associated with decreased lower extremity injury rates. 3,12,14,41,43 Thus, a program to reduce muscular fatigue and muscular imbalances and improve balance in dancers would be expected to reduce injury.
Injury prevention protocols in the literature focusing on individual sports have been shown to be effective. FIFA 11+ for soccer is one of the most well-known and well-studied programs. 6,10,24,40 The FIFA 11+ has been shown to reduce muscle strain and tears, 40 noncontact injuries, 24 rates of lower extremity injuries, risk of overuse injuries, risk of severe injuries, time lost to injury, and risk of overall injuries. 6 Many other studies have investigated reduction of a particular injury, such as anterior cruciate ligament tears, 19,31,39 hamstring strain, 32,37 and elbow injury. 11,18 The few ballet dance-specific injury prevention studies in the literature either were inconclusive with regard to reducing injuries or did not use a control group. 2,35,46 At present, no published randomized controlled trials are available evaluating an injury prevention program (IPP) for dance.
We designed an IPP (see the Appendix) to target the core, hip abductor, hip flexor, and hip extensor muscles. The primary purpose of the study was to evaluate the effectiveness of this IPP for professional ballet. We hypothesized that the use of an IPP would significantly reduce the risk of injury in professional ballet dancers.
Methods
Institutional review board approval was obtained for this study. All male and female professional ballet dancers, 18 years of age or older, from a single metropolitan ballet company were eligible. Eligible sample size was predetermined by the number of company members (n = 52). Exclusion criteria included those who chose not to participate, were pregnant, and were younger than 18 years. Informed consent was obtained from all participants. Baseline demographics and measurements were gathered at the annual company physical examinations, which took place at a tertiary care facility over 1 day. Data gathered included body mass index (BMI), age, sex, previous injury, years dancing professionally, rank, single-leg balance, turnout (in degrees based on rotation boards), Beighton score, 7 Brighton criteria, 15 International Hip Outcome Tool (iHOT-12) score, and American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score.
Dancers were separated into 3 rank groups based on their position in the company. Principals and first soloists were designated as rank 1, soloists and demi-soloists as rank 2, and corps de ballet and apprentices as rank 3. The dancers were randomized to 1 of 2 groups through use of Microsoft Excel’s random function stratified by rank to ensure that each rank was equally represented in the intervention and control groups. The random allocation sequence, enrollment, and assignment of participants were executed by the first author (A.M.V.). Funding was provided internally by Houston Methodist Orthopedics and Sports Medicine.
Injury Prevention Program
Participants in the control group were instructed to continue their current dance and exercise practices as usual per standard operating practice for training and performances. The experimental group was instructed to perform as much of a prepared exercise program as they could (details in Appendix). Compliance was measured and defined as having completed at least 4 consecutive weeks of the IPP. No explanation regarding participants’ noncompliance was elicited. The program consisted of three 30-minute exercise programs that the participants were to perform each week for 52 weeks unsupervised unless they requested specific guidance from the athletic training staff. They were not given allotted time by the company to complete these exercises. However, most exercises could be performed without cumbersome equipment. Thus, the exercises could be completed at times and locations that the participants found convenient. They had access to a fully equipped athletic training facility at the company’s combined class, rehearsal, and performance space. Dancers were given a booklet with written (see the Appendix) and graphic descriptions of each exercise. Additionally, custom video descriptions of each exercise were available on YouTube (https://www.youtube.com/channel/UCOrCu9zLaVMsEpPxFqVhqjw). The dancers were instructed to turn in weekly adherence assessments. The program was based on preventing the most common injuries as well as the rehabilitation and prevention protocols that have been shown to target those issues in athletes.
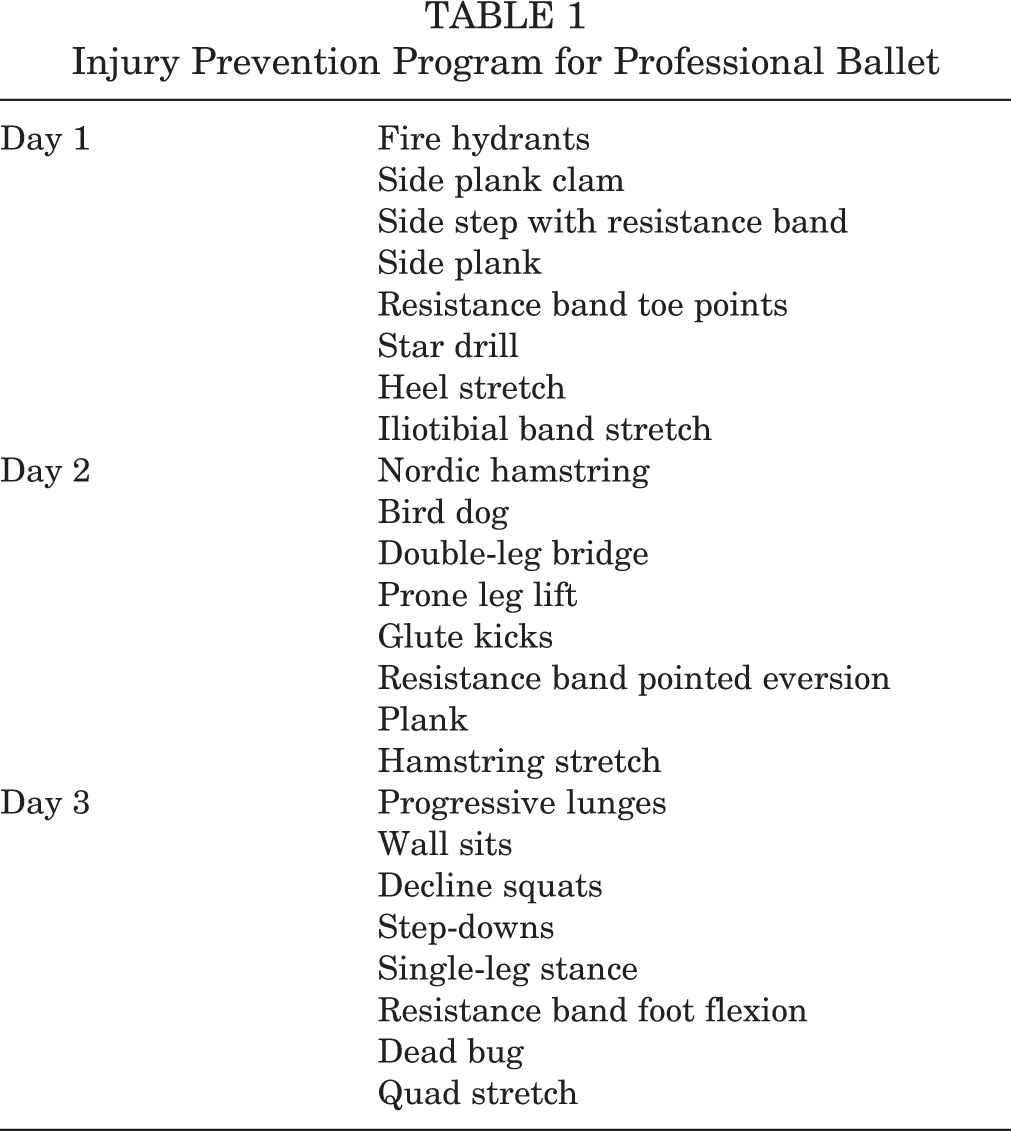
The weekly program was designed for 3 days, each day with different exercises. It was recommended that the dancers choose 3 nonconsecutive days on which to perform these exercises, and they were instructed not to consolidate days. All exercises had progression options that included increasing resistance with elastic bands or free weights. The dancers were to progress through the outlined protocol when each exercise was no longer challenging enough for them. Wherever possible, eccentric aspects of the exercises were emphasized. All exercises are listed in Table 1 (detailed in the Appendix).
Injury Prevention Program for Professional Ballet
Injury Data
Injury was defined in 2 ways. The first definition was based on the Standard Measures Consensus Initiative from the International Association of Dance Medicine and Science (IADMS). 30 The second definition was an adaptation of the National Aeronautics and Space Administration (NASA) injury guidelines, 51 as listed in Table 2. Injuries were diagnosed by either a certified athletic trainer or a physician. Injuries were recorded on a physical form created specifically for the study and in an electronic medical record system (Athletic Trainer System).
Injury Definitions a

a The table provides the IADMS injury definition and total number of injuries among both groups, as well as an adaptation of the National Aeronautics and Space Administration (NASA) injury guidelines used to define injury, total number of injuries among both groups, and the percentage of total injuries based on classification.
Additional information collected included injury type (traumatic vs overuse), affected body part, diagnosis, mechanism, duration of time to full activity, and treatment. Information on where the injury occurred (class, rehearsal, performance, other), activity (classical, contemporary ballet, modern, other), and number of hours danced in the preceding week was also collected. Return to full activity was defined as return to unrestricted class, rehearsal, and performance.
Statistical Analysis
Statistical analysis on treatment group differences for continuously scaled baseline and outcome variables was conducted by use of the Student t test, with results presented in the form of groupwise mean and standard deviation and tail probability (P value). As commonly used in outcomes for interventional studies, 52 Cox proportional hazards (PH) regression models for recurrent failures were used, where the hazard ratio (HR) indicates the relative likelihood of injury in the control versus intervention group. Modeling included compliant participants in the IPP group and all controls. Confounders significant across arms and whose P values were less than .25 in univariate models were added to multivariable models that included the IPP treatment effect (0,1) to identify the adjusted HR. The adjusted HR controls for influence by confounders, which are defined as factors associated with both the exposure (IPP) and disease (injury). All statistical analyses were performed using Stata Version 14.
Results
Of 52 eligible dancers, 75% (n = 39) chose to participate. The remaining 13 declined participation because they believed they did not have the time to commit, and none were excluded for not meeting inclusion criteria (Figure 1). Of the 39 dancers, 19 (9 males and 10 females; mean age, 26.6 ± 4.0 years) were randomized to the control group and 20 (11 males and 9 females; mean age 25.1 ± 5.1 years) to the IPP group. No significant (P > .05) differences in age, BMI, and company rank were found among the groups (Table 3). This remained true when the noncompliant individuals were removed from the analysis (Table 4). We noted that 11 participants (11/20; 55%) were compliant with the program, based on the fact that they performed at least 4 weeks of the IPP. Reasons for noncompliance were not elicited from participants. If participants were not compliant, their data were not included in the Cox PH statistical analysis of injury rate and subsequent injury. However, other aspects of their injuries were included, as discussed below.
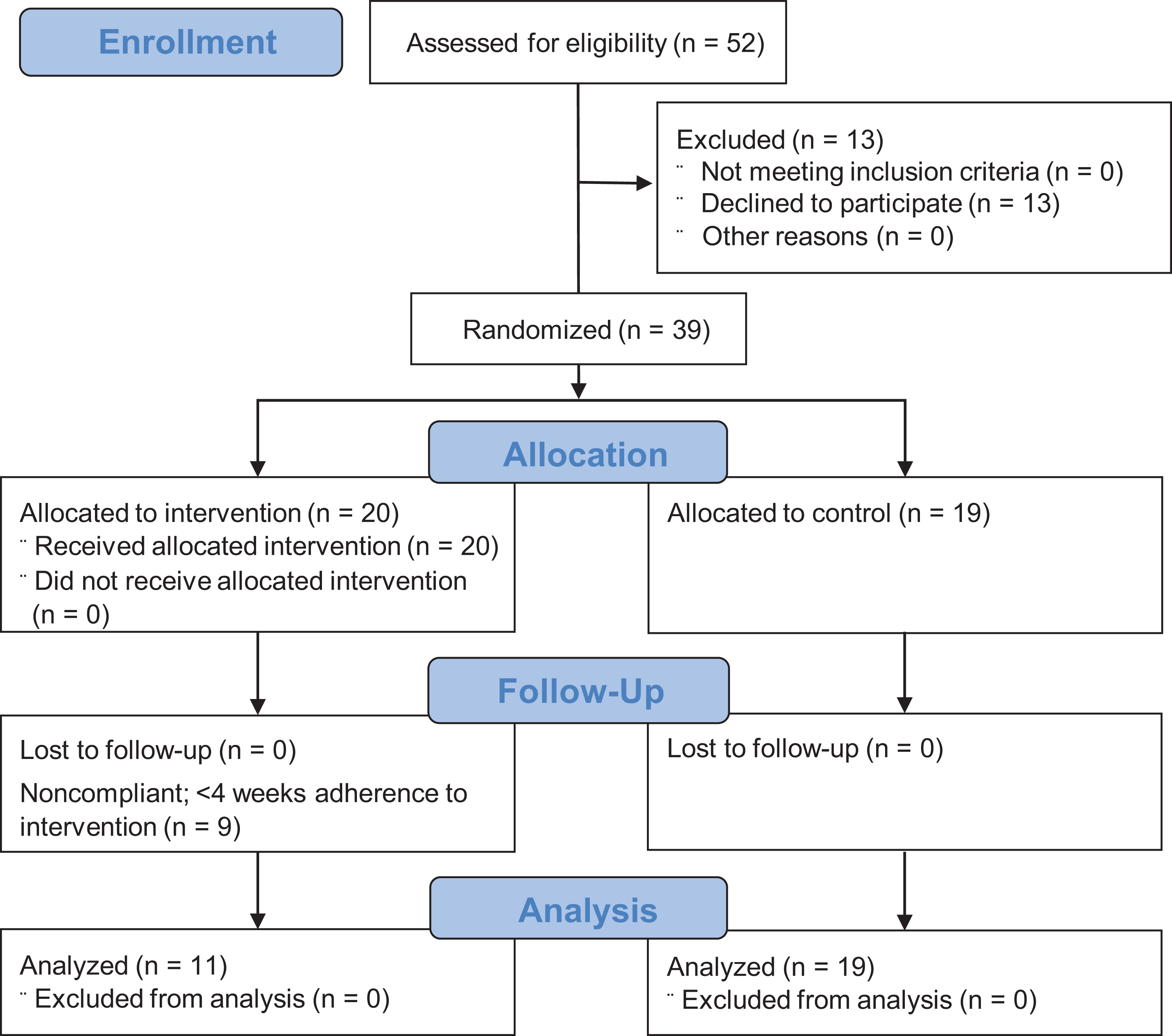
CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Demographics for Control and Intervention Groups (Including Noncompliant Participants)
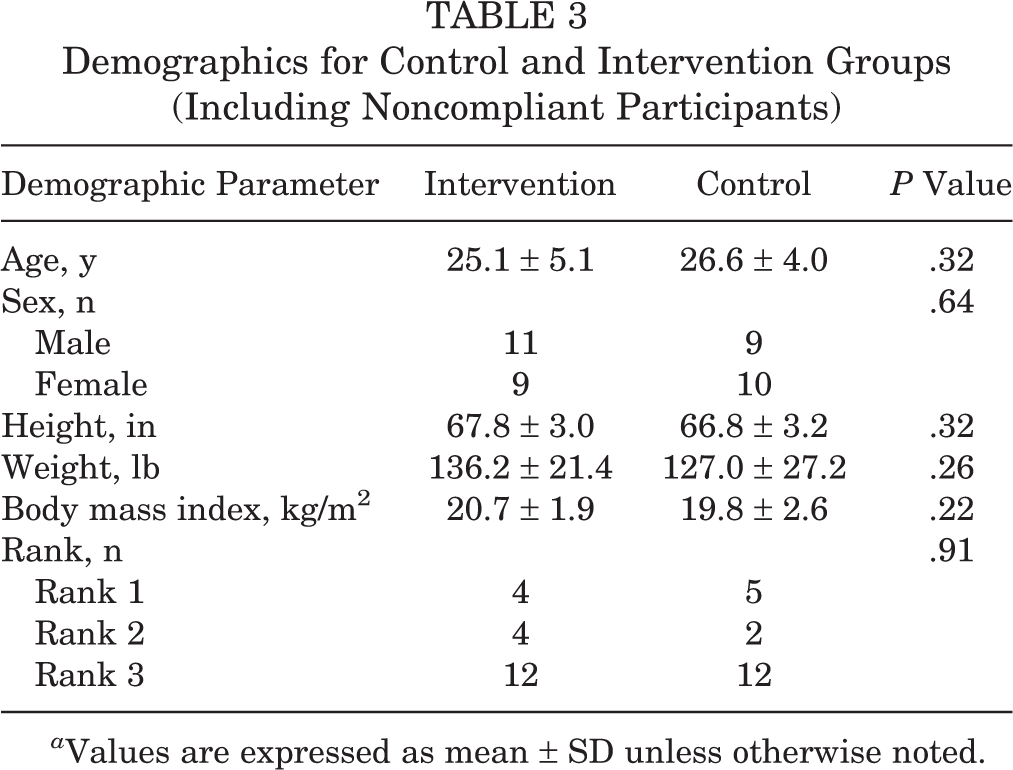
a Values are expressed as mean ± SD unless otherwise noted.
Demographics for the Control Group and Compliant Dancers Within the Intervention Group a

a Values are expressed as mean ± SD unless otherwise noted.
For all participants, 45 injuries were sustained based on the IADMS Standard Measure Consensus Initiative over 52 weeks. Based on the modified NASA guidelines, 116 injuries were sustained (Table 2). The number of injuries by anatomic location can be seen in Table 5. The setting of all injuries was as follows: class, 10.3%; rehearsal, 67.2%; performance, 16.4%; and other, 6.0%. The style danced at the time of injury was contemporary ballet (49%), followed by classical ballet (41%), modern dance (3%), and other activities (7%). Traumatic injuries made up 54% of all injuries, whereas overuse injuries made up 46%. All mechanisms of injury are listed in Table 6. The IPP group had 49 injuries (compliant and noncompliant), whereas the control group had 67 total injuries during the study period. The mean number of days to full activity after injury was not statistically significant between the control and IPP groups (11.9 ± 43.7 vs 14.6 ± 25.2, respectively; P = .49). During the study period, 4 participants underwent surgery. Of these, 1 dancer from the IPP group underwent abdominal wall reconstruction, adductor longus compartment decompression, and tendon release for a chronic abdominal wall injury sustained in the prior season. A further 2 dancers underwent arthroscopic anterior labral repair for chronic shoulder instability; 1 of these dancers was in the IPP group and the other dancer was in the control group, and both had initial episodes of ipsilateral instability in prior seasons. The fourth dancer who underwent surgery was in the IPP group but was noncompliant. He underwent ankle arthroscopy with os trigonum resection.
Frequency of All Injuries by Anatomic Location (Including Control Group and All Intervention Group Participants) a

a N = 116.
Frequency of All Injuries by Mechanism (Including Control Group and All Intervention Group Participants) a

a N = 116.
The median time to injury for compliant IPP participants was 219 days, whereas for control participants the median time to injury was 130 days. See Table 7 for hypothesis testing results. Prior injury, rank, balance left, and iHOT-12 score were not significantly different across the treatment groups. In the univariate Cox PH models for injury rate, the variables female, years dancing, turnout left, turnout right, average Beighton score, and AOFAS ankle-hindfoot scores resulted in P ≤ .25 (indicating significant confounding variables). In the univariate Cox PH models for subsequent injury, the variables years dancing, turnout left, turnout right, average Beighton score, and Brighton criteria resulted in P ≤ .25 (Tables 8 and 9). Participants without values for the confounding variables were excluded from this analysis by statistical necessity. A total of 3 participants from the IPP group and 4 participants from the control group refused to be measured for 1 or more of the confounding variables.
Hypothesis Testing Results for Potential Confounders Used in Multivariable Failure-Time Models a

a AOFAS, American Orthopaedic Foot and Ankle Society; iHOT-12, International Hip Outcome Tool; IPP, injury prevention program; L, left; N, no; NA, not applicable; R, right; Y, yes.
Injury Rate Cox Proportional Hazards Regression Hazard Ratio (HR) for the Injury Prevention Program (IPP) a
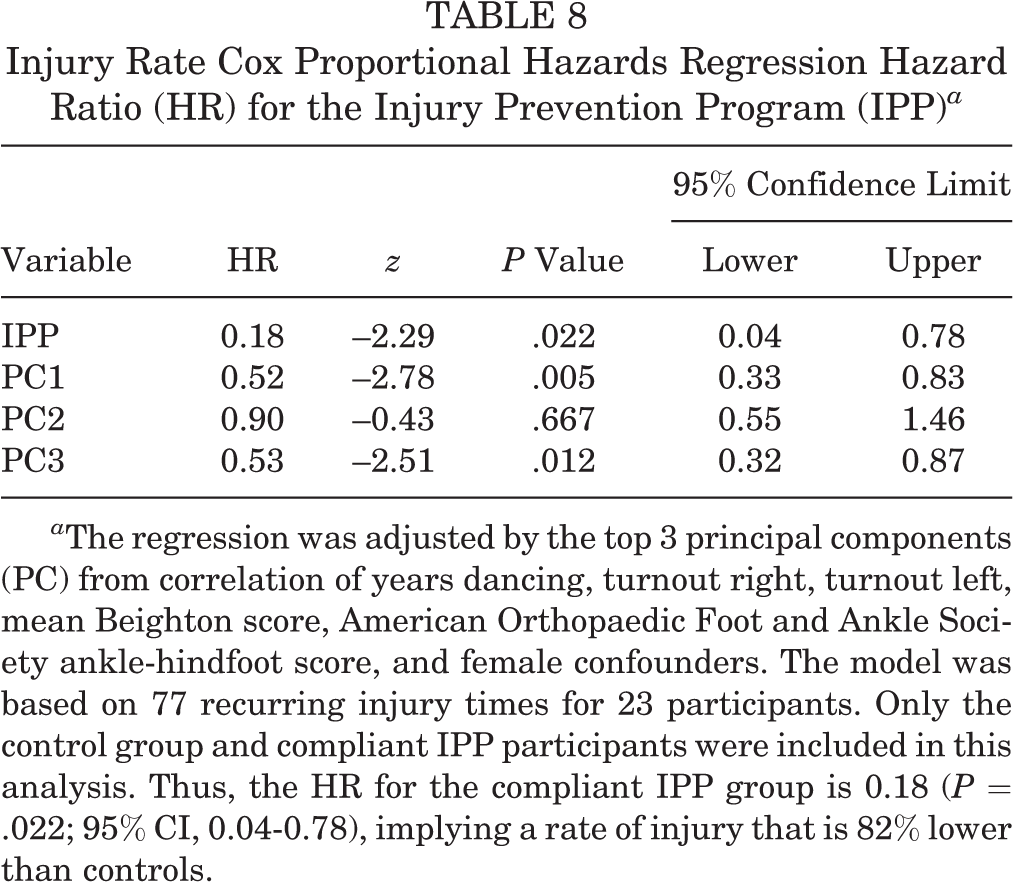
a The regression was adjusted by the top 3 principal components (PC) from correlation of years dancing, turnout right, turnout left, mean Beighton score, American Orthopaedic Foot and Ankle Society ankle-hindfoot score, and female confounders. The model was based on 77 recurring injury times for 23 participants. Only the control group and compliant IPP participants were included in this analysis. Thus, the HR for the compliant IPP group is 0.18 (P = .022; 95% CI, 0.04-0.78), implying a rate of injury that is 82% lower than controls.
Subsequent Injury Cox Proportional Hazards Regression Hazard Ratio (HR) for the Injury Prevention Program (IPP) a
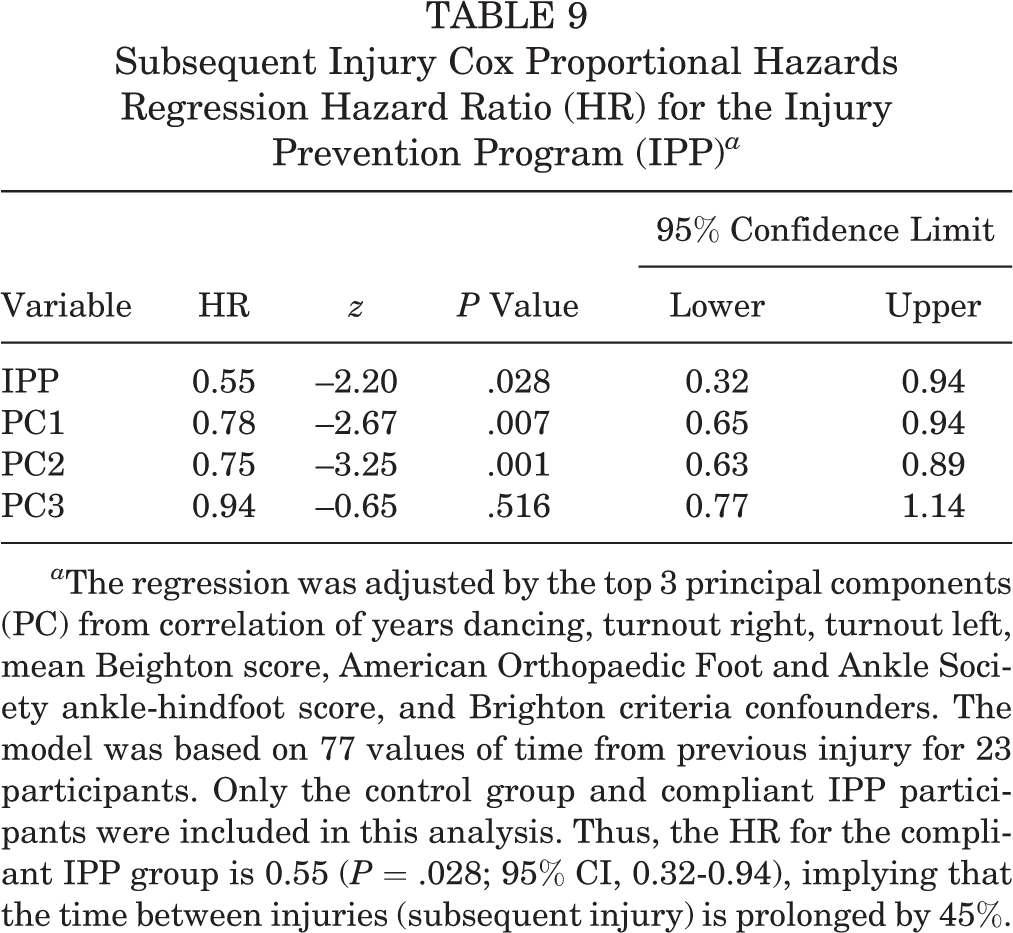
a The regression was adjusted by the top 3 principal components (PC) from correlation of years dancing, turnout right, turnout left, mean Beighton score, American Orthopaedic Foot and Ankle Society ankle-hindfoot score, and Brighton criteria confounders. The model was based on 77 values of time from previous injury for 23 participants. Only the control group and compliant IPP participants were included in this analysis. Thus, the HR for the compliant IPP group is 0.55 (P = .028; 95% CI, 0.32-0.94), implying that the time between injuries (subsequent injury) is prolonged by 45%.
The results of the injury rate Cox PH model as shown in Table 8 suggest an HR of 0.18 (P = .022; 95% CI, 0.04-0.78), implying a rate of injury that is 82% lower in the compliant IPP group than in controls. The results shown in Table 9 suggest that the time between injuries (subsequent injury) is prolonged by 45% (HR, 0.55; 95% CI, 0.32-0.94) among the compliant IPP group compared with controls.
Discussion
The present study is the first prospective randomized controlled investigation of an injury prevention program for professional ballet. The results showed an 82% decrease in injury rate for the intervention group and an extended period from previous injury to subsequent injury. This confirmed our hypothesis. These results suggest that an IPP performed for as little as 4 weeks may reduce injury rate and increase injury-free time over the course of 1 year.
As used in clinical trials to test the efficacy of an intervention on reducing disease, 52 the Cox PH regression model was used in the present study. This allowed us to adjust for several confounding factors that are thought to contribute to injury, including sex, hypermobility, and turnout. Thus, the present study provides a reliable test of treatment efficacy, which is of upmost interest to the clinician. 52 The results of this investigation confirmed the impression that an IPP program would be beneficial to participants. However, due to the relatively small number of participants included in the statistical analysis, further research is warranted to allow applicability to the larger dance population. Compliance was measured and defined as having completed at least 4 consecutive weeks of the IPP. Nearly half of the IPP participants were compliant. However, this resulted in exclusion of potentially 25% of the baseline and injury follow-up data for the Cox PH data analysis. We conducted dimensional reduction using principal components analysis of significant confounders in failure time models in order to prevent violation of the rule of thumb requiring the addition of 10 records for each potential confounder and outcome measurement made.
Although many reports are available regarding injury prevention techniques for team sport athletes, § very few intervention trials for prevention of injuries in dancers have been conducted. Only 3 studies have attempted to reduce injuries in dancers. Mistiaen et al 35 and a later study by Roussel et al 46 were structured around the same preprofessional dance program. Although those investigators found reduced injuries with an IPP, they did not use a randomized controlled model nor did they include professional dancers. Allen et al 2 reported the effects of individualized conditioning programs on the injury rate of a professional ballet company. Those investigators found significant reduction in injury rates for their population based on using the prior year’s injury data as the control comparison. Their IPP was customized to each dancer. The development of the individualized program was not explained in detail, making replication of the program difficult, and the report does not provide the amount of time each dancer had to commit each week or the duration of the intervention. Additionally, the conditioning sessions were supervised by a professional from the medical team. The present study found a reduction in injury rates using a generalized IPP for ballet based on common weaknesses in the ballet dancer. Although an individualized and supervised program may be ideal for injury prevention, this is difficult for most dance companies to provide. The IPP in the present study can be easily adopted by all ballet dancers. Furthermore, the randomized control group used in the present study takes dancer differences and repertoire into consideration, which is not possible when using prior season data.
Injury data collected in the current investigation are consistent with reports from other studies with regard to when injuries most commonly occurred and the anatomic location for injuries. 13,20,23,38,42 However, the present population had a higher proportion of traumatic injuries (53%) than previously reported in the literature. 13,20,42,47 This is likely due to the implementation of a new annual winter program, requiring dancers to learn entirely new staging, props, costuming, and choreography, which was significantly more physically demanding. Furthermore, another production performed that year required some of the men to dance en pointe, which is highly unusual.
Limitations of this study include poor compliance over the year-long period. This may have been attributable to lack of motivation or time on the dancer’s part. This is a common plight in studies evaluating IPPs, especially in elite athletes. 35,49,50,53,55 The 3 prior dance-specific IPPs either do not reveal compliance rates at all 2,46 or do not reveal the compliance of the dancers used in their final analysis. 35 However, in the present investigation, when viewed in a per-protocol analysis, the intervention group was found to have a decreased rate of injury. This suggests a protective effect from even a short duration of an IPP for professional ballet dancers. The poor compliance rate also results in selection bias within the cohort. The present study required dancer self-motivation to implement, which may have been the reason for low compliance. We tried to limit all hindrances to compliance by providing multiple modes of instructional delivery, availability of an in-house athletic trainer with full knowledge of the IPP, little need for extra equipment, availability of equipment on-site if needed, freedom to work exercises into the participants’ individual schedules, detailed prelabeled adherence records requiring only checkmarks to indicate completed exercises, and weekly text messages and monthly emails from the athletic trainer with reminders to complete and turn in adherence forms. A scheduled supervised time allotted by the company administration may have increased compliance. The reduction in injury seen with limited compliance during the season argues that greater reductions could be seen if this IPP became a required part of the dancers’ training. The evaluation of professional classical ballet dancers limits the IPP’s applicability to students and other styles of dance.
Other limitations include the small number of participants, which was dictated by the company size and not by a power analysis. However, the uniqueness of the population adds significant value to this study, as it is very difficult to get professional athletes to participate in a randomized controlled trial for an IPP. The ability to gather this type of information on professional athletes is both rare and invaluable. Although 52 dancers were eligible to participate, only 39 choose to do so. This could lead to selection bias in the dancers who chose to participate, who may have been more motivated to comply or already performing their own cross-training regimen. The length of the study was only 1 year; however, 2 years is the standard in most level 1 randomized controlled trials. Diagnoses of most injuries were made by a certified athletic trainer, not an orthopaedic surgeon. Thus, diagnostic accuracy was not confirmed for all injuries unless the injury was severe enough to warrant further investigation. Last, because IPP sessions were not supervised, the level of compliance may have been overestimated by the dancers self-reporting to appease investigators. However, assessment documentation provided by the dancers was made anonymous with the use of participant identification numbers.
Conclusion
The present study is the first prospective randomized controlled investigation of an injury prevention program for professional ballet. The results showed an 82% decrease in injury rate for the intervention group and an extended period from previous injury to subsequent injury.
Footnotes
Acknowledgment
The authors acknowledge the athletic trainers (Zakia Tillis, MS, LAT, ATC; Carina Nasrallah, MS, LAT, ATC, CISSN; and Leanne Wonesh, MS, LAT, ATC); Vijay Jotwani, MD; Jim Nelson; and the dancers of Houston Ballet, who contributed to making this project possible.
Final revision submitted February 21, 2020; accepted March 9, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.M.V. has received educational support from Arthrex/Medinc of Texas and DePuy. P.C.C. has received research support from DePuy and Arthrex/Medinc of Texas and speaking fees from Vericel/Aastrom Biosciences. K.E.V. has received consulting fees from DePuy, In2Bones, and Wright Medical and royalties from In2Bones and Wright Medical, and he has stock/stock options in In2Bones and Wright Medical. J.D.H. has received research support from Arthrex/Medinc of Texas, DePuy, and Smith & Nephew; consulting fees from NIA Magellan and Smith & Nephew; speaking fees from Ossur and Smith & Nephew; and royalties from SLACK. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Houston Methodist Research Institute (study ID: Pro00022554).