
Abstract
Background:
The alpha angle used to evaluate cam morphology can be determined on different imaging views; however, 2-dimensional (2D) imaging can present limitations in terms of the reproducibility of the radial alpha angle. Recent developments in 3-dimensional (3D) high-resolution magnetic resonance imaging (MRI) have allowed detailed evaluations of the radial alpha angle.
Purpose:
To determine whether there are any correlations or discrepancies between the 2D alpha angle on plain radiography and the maximum radial alpha angle on 3D MRI.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
A total of 42 hips from 39 patients (19 males, 20 females) were analyzed, including 22 hips with femoroacetabular impingement (FAI; mean age, 41 years) and 20 hips with borderline developmental dysplasia of the hip (BDDH; mean age, 43 years). Radial images were reconstructed from 3D multiple echo recombined gradient echo (MERGE) MRI. Differences in the maximum radial alpha angle on MRI between hips with FAI and BDDH were evaluated. Correlations and discrepancies between the maximum radial alpha angle on MRI and alpha angles on the anteroposterior, cross-table lateral, and 45° Dunn views of radiography were also evaluated.
Results:
The maximum radial alpha angle was significantly higher for hips with FAI than for hips with BDDH. On average, the greatest alpha angle on radial MRI was higher than the alpha angle on each of the 3 radiographic views for both FAI and BDDH. The 45° Dunn view revealed the smallest discrepancy for both FAI (P = .005) and BDDH (P = .002). The cross-table lateral view had the highest correlation with the maximum radial alpha angle for BDDH (P < .001).
Conclusion:
We reconfirmed the utility of the 45° Dunn view, with it presenting the best reproducibility for the maximum radial alpha angle in the evaluation of cam morphology, while the cross-table lateral view revealed the best correlation with the maximum radial alpha angle, particularly for hips with BDDH.
Keywords
The imaging diagnosis of femoroacetabular impingement (FAI) is based on evaluations of pincer or cam morphology, 6 which are performed mainly using plain radiographs. In cam-type FAI especially, the alpha angle is an important parameter that is commonly evaluated on plain radiography. 2 However, 2-dimensional (2D) evaluations conducted solely on plain radiography may not be reliable for measuring the alpha angle, 13 and therefore 3-dimensional (3D) evaluations are needed to achieve a better understanding of cam morphology. 7 Recent developments in 3D imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI) with 3.0 T may potentially facilitate such 3D evaluations. 15
While several recent studies have revealed the utility of the Dunn view, 2,5 investigations into whether differences exist between the radiographic alpha angle and radial alpha angle are still lacking, particularly in cases of borderline developmental dysplasia of the hip (BDDH). It is also important to evaluate cam morphology in BDDH cases. We hypothesized that different radiographic techniques to assess the alpha angle may have discrepancies for the evaluation of cam morphology in FAI and BDDH cases. The purpose of this study was therefore to compare the alpha angle between radial MRI and plain radiography on several different views in cases of FAI and BDDH with cam morphology.
Methods
This retrospective cross-sectional study was approved by the local institutional review board. A total of 42 hips from 39 consecutive patients (19 males; 20 females) who had undergone arthroscopic surgery between October 2013 and May 2018 and had also undergone multiple echo recombined gradient echo (MERGE) MRI before surgery were retrospectively reviewed. The patients were divided into 2 groups: 22 hips with FAI (mean patient age, 41 years) and 20 hips with BDDH (mean patient age, 43 years). FAI was defined as a lateral center-edge angle greater than 25° on the anteroposterior (AP) view of the pelvis and an alpha angle greater than 55° on the cross-table lateral view or 45° Dunn view. BDDH was defined as a lateral center-edge angle between 20° and 25° on the AP view of the pelvis.
The maximum radial alpha angle on MRI was compared with the alpha angles on 3 different radiographic views as previously described: AP view of the pelvis, cross-table lateral view, and 45° Dunn view. 5 The method proposed by Bouma et al 4 was used for measurements of the alpha angle. Briefly, the axis of the femoral neck was defined as the line passing through the center of the femoral head circle, parallel to the line connecting the center of 2 circles placed over the femoral neck (Figure 1).
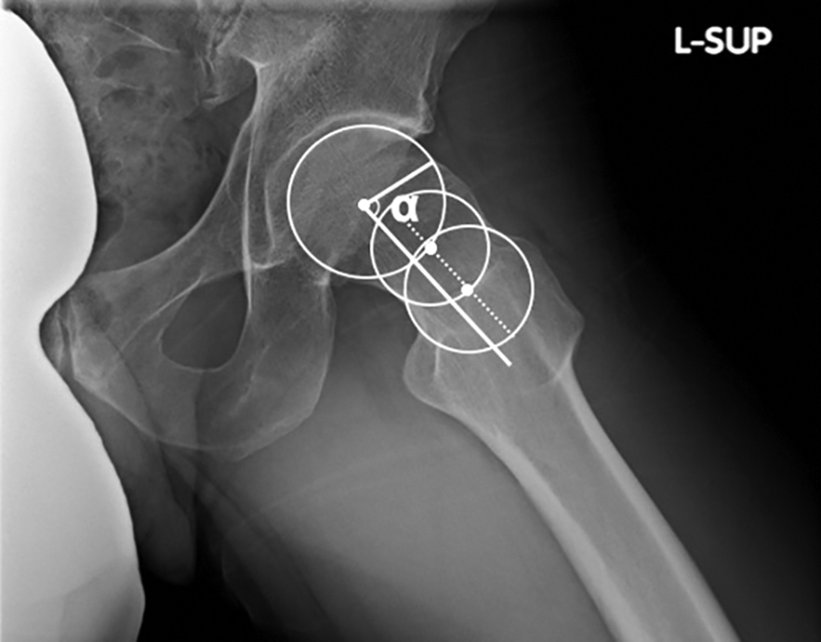
Measurement of the alpha angle on plain radiography. The axis of the femoral neck was defined as the line passing through the center of the femoral head circle, parallel to the dotted line connecting the center of the 2 circles placed over the femoral neck.
MRI and Measurement of Radial Alpha Angle and Signal Intensity
Ultimately, 3D MERGE MRI was performed on a Discovery MR750w scanner (GE Healthcare) using a repetition time of 30 milliseconds, an echo time of 10.9 milliseconds, a field of view of 15 × 15 cm, a matrix size of 300 × 300, 2 excitations, a bandwidth of 50 kHz, a slice thickness of 0.5 to 1 mm, a section gap of 0 mm, and an acquisition time of 5 minutes. Radial images were reconstructed using the multiplanar reconstruction procedure for each 5° increment in the radial plane around the central axis of the femoral neck.
The radial images were evaluated on the basis of a clockface, with 0° (9 o’clock) at the anterior and 90° (12 o’clock) at the lateral. The radial alpha angle was measured at 0° (anterior; 9-o’clock position), 15°, 40°, 65°, and 90° (lateral; 12-o’clock position). Specifically, an oblique axial plane vertical to the femoral neck axis was reconstructed such that the most anterior slice was identified at 9 o’clock and the most lateral slice was identified at 12 o’clock, according to a previously described method. 9 Figure 2 shows the method for measurements of the alpha angle on radial MRI. Briefly, the alpha angle was measured at each clockface position with the same method used for the radiographic alpha angle as described above.

Measurement of the alpha angle on radial magnetic resonance imaging in the 12-o’clock position. The axis of the femoral neck was defined as the line passing through the center of the femoral head circle, parallel to the dotted line connecting the center of the 2 circles placed over the femoral neck.
Statistical Analysis
The significance of the difference in the maximum radial alpha angle between FAI and BDDH was assessed using the Student t test. Significant differences in the discrepancy of the alpha angle across the 3 radiographic views were assessed using the Kruskal-Wallis test and the Steel-Dwass test as post hoc testing. All statistical analyses were performed using EZR Version 1.37 (Saitama Medical Center, Jichi Medical University).
Results
Figure 3 summarizes the alpha angle on MRI for each radial section. The maximum radial alpha angle for hips with FAI was located at 40°, while for hips with BDDH, it was found at 15°; that is, the maximum radial alpha angle was more anterior for BDDH than for FAI. The overall mean maximum radial alpha angle was significantly higher for FAI than for BDDH (P = .0012) (Figure 4).

Mean alpha angle on each radial section for femoroacetabular impingement (FAI) and borderline developmental dysplasia of the hip (BDDH). The maximum radial alpha angle is located at 40° for FAI and more anteriorly at 15° for BDDH.
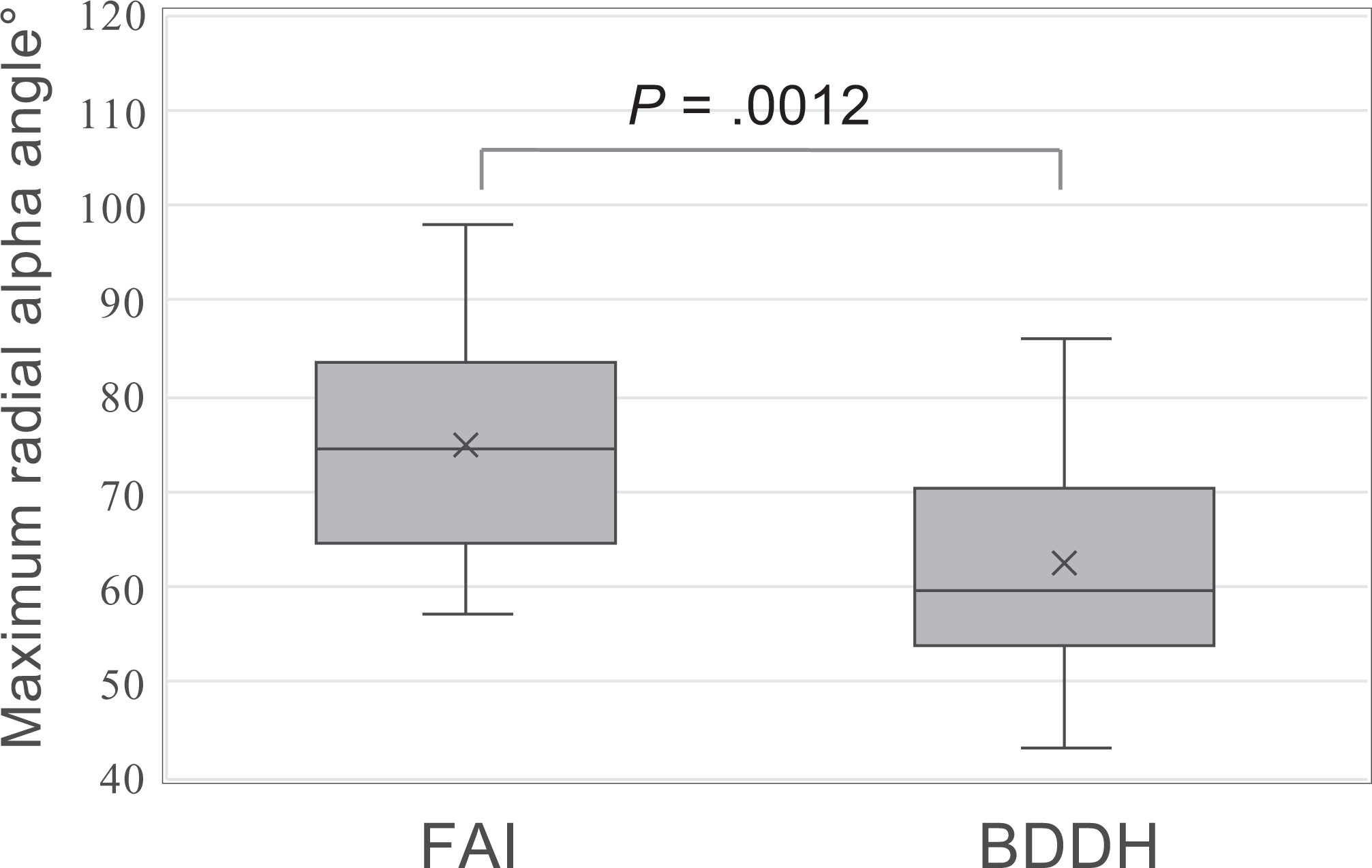
Difference in the maximum radial alpha angle between femoroacetabular impingement (FAI) and borderline developmental dysplasia of the hip (BDDH). The maximum radial alpha angle was significantly higher for FAI than for BDDH. The shaded box shows the interquartile range, the horizontal line in the box indicates the median, and the “x” indicates the mean. The error bars indicate the maximum and minimum values.
On average, the greatest alpha angle on radial MRI was higher than the alpha angle on each of the 3 radiographic views for both FAI and BDDH. When comparing radiography and radial MRI, the 45° Dunn view showed the smallest discrepancy for both FAI and BDDH (Figure 5).

Measurement of the discrepancy between the maximum radial alpha angle and radiographic alpha angle for femoroacetabular impingement (FAI) and borderline developmental dysplasia of the hip (BDDH). (A) In the hips with FAI, the measurement discrepancy on the 45° Dunn view was significantly smaller than on the cross-table lateral view. (B) In the hips with BDDH, the measurement discrepancy on the 45° Dunn view was significantly smaller than on the anteroposterior (AP) view. However, there was no significant difference between the 45° Dunn and cross-table lateral views. The shaded box shows the interquartile range, the horizontal line in the box indicates the median, and the “x” indicates the mean. The error bars indicate the maximum and minimum values.
Table 1 summarizes the results of the radiographic alpha angles, and Table 2 summarizes the Pearson correlation coefficients and P values between the maximum radial alpha angle on MRI and each radiographic alpha angle. In the hips with BDDH, the cross-table lateral view showed the strongest correlation (r = 0.90; P < .001) with the maximum radial alpha angle on MRI. There were no significant correlations between the maximum radial alpha angle and the alpha angle on the AP view for either FAI or BDDH.
Radiographic Alpha Angle a

a AP, anteroposterior; BDDH, borderline developmental dysplasia of the hip; FAI, femoroacetabular impingement.
Correlations Between Maximum Radial Alpha Angle on MRI and Each Radiographic Alpha Angle a

a AP, anteroposterior; BDDH, borderline developmental dysplasia of the hip; FAI, femoroacetabular impingement; MRI, magnetic resonance imaging.
Discussion
The clinical relevance of the current study is that the correlation between the alpha angle on radial MRI and that on the cross-table lateral view was found to be very high, with the best reproducibility being observed for the maximum radial alpha angle on the 45° Dunn view. It is important to be aware of these factors when evaluating cam morphology on plain radiography.
The radiographic alpha angle is a fundamental measurement for evaluating cam morphology. 3 Several imaging views have been validated for determining the alpha angle, including the AP, cross-table lateral, Dunn, and frog-leg lateral views. 2,13 Barton et al 2 evaluated the accuracy and reproducibility of the AP, cross-table lateral, and Dunn views of plain radiography for the diagnosis of cam-type deformities. They concluded that the Dunn view had the best accuracy, with a sensitivity of 91% and a specificity of 88%. Similarly, several other studies recommend the 45° Dunn view for the accurate evaluation of cam morphology. 5,10,16 Indeed, our current results show that the 45° Dunn view had the best reproducibility for the maximum radial alpha angle, particularly in hips with FAI. On the other hand, our results also revealed that the cross-table lateral view had the highest correlation with the maximum radial alpha angle, particularly in hips with BDDH. Another recent study comparing 2D radiographic measurements with 3D metrics of the proximal femur also reported that the 3D scores were most strongly correlated with the alpha angle on the cross-table lateral view. 1
Although the location of actual impingement and cam morphology may not be concordant, the most appropriate radiographic view for evaluating the alpha angle should depend on the actual cam morphology location, which might reveal a different distribution between FAI and BDDH cases. A previous study demonstrated that the impingement points tend to appear more proximal and on the medial side rather than on the lateral side in BDDH cases. 12 Although the actual impingement point was not identified in our study, this characteristic of the impingement point might be why the cross-table lateral view showed the highest correlation with the maximum radial alpha angle for hips with BDDH. Uemura et al 17 investigated various radiographic views using imaging models based on CT data, which showed that radiographic views could be used to visualize cam morphology in different clockface positions. Thus, we should note that each radiographic measurement has different characteristics in terms of the evaluation of cam morphology. Moreover, the measurement method itself needs to be strictly standardized if it is to be used as a highly reproducible method as previously reported. 4 This concept of strict standardization was adopted in the current study.
Moreover, in the current study, we made use of 3D MERGE MRI, which allows the reconstruction of images in the radial plane based on the femoral neck axis and thereby facilitates measurements of the radial alpha angle. Samim et al 15 reported 100% agreement between 3D MRI and 3D CT for the diagnosis and location of cam deformities. Basically, we need imaging information concerning soft tissue or chondral status, including labrum tears revealed by MRI in patients with FAI. 11 In addition, it is possible to obtain morphological information, particularly on recent 3D MRI. 9
The coexistence of cam morphology and BDDH is an important clinical issue. Harris et al 8 investigated the prevalence of radiographic abnormalities in elite ballet dancers, among whom cam deformities were recognized in 25.5% and dysplasia or BDDH in 89%. In a previous study using a 3D computer simulation model, virtual cam resection in BDDH cases showed the most significant improvement in hip range of motion compared with that in FAI cases 14 ; thus, a detailed evaluation of cam morphology should be performed also in BDDH cases. In fact, the results of this study showed that the mean maximum radial alpha angle for hips with BDDH was more than 60°, which indicates the existence of cam morphology, although it was 58.2° on the 45° Dunn view.
It is difficult to rate the importance of variations in the discrepancy or correlation between radiographic and radial alpha angles. In the clinical setting, the 45° Dunn view may be preferred when estimating the actual radial alpha angle. On the other hand, the alpha angle on the cross-table lateral view may be an effective parameter when evaluating cam morphology in BDDH cases.
There are several limitations in this study. First, the availability of 3D MERGE MRI was limited in our department; therefore, the number of patients was relatively small, and selection bias may have occurred. Second, radiography was limited to 3 major views. Other radiographic views might have yielded different results. In addition, the 3D evaluation was also limited to 5 representative radial sections, which did not include 45°. The 3D measurement on a 45° radial section might represent the 45° Dunn view more accurately.
Conclusion
We reconfirmed the utility of the 45° Dunn view, with it presenting the best reproducibility for the maximum radial alpha angle as an evaluation of cam morphology. Furthermore, the cross-table lateral view revealed the best correlation with the maximum radial alpha angle for hips with BDDH.
Footnotes
Final revision submitted February 13, 2020; accepted March 1, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the research clerkship program of Yokohama City University. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Yokohama City University Medical Center.