
Abstract
Purpose:
To report midterm outcomes of a series of acute pectoralis major tears repaired surgically in the deployed setting in active duty military personnel.
Methods:
Analysis of acute pectoralis major tears treated at one expeditionary medical treatment facility during a 4-month time frame.
Results:
Nine male patients with a mean age of 32 years (23–52) were diagnosed with tears; seven underwent operative fixation in the forward deployed setting. All injuries occurred during bench press, with the dominant upper extremity involved 56% of the time. With an average final follow-up of 4.1 years, the mean disabilities of the arm shoulder and hand score was 35.71 (range 31–41) and the mean American shoulder and elbow surgeons score was 90.71 (range 87–95). All personnel returned to their preinjury jobs with an average return to full preinjury function occurring at 7 months (range 4.5–10.5 months) in the operative group.
Conclusions:
Combat-deployed active duty US military personnel likely represent a high-risk population for this injury. Our study demonstrates that with at least 4 years of follow-up, surgical repair with a trough and trans-osseous repair technique was technically feasible and clinically successful in the deployed setting. Although this treatment may be considered in rare individual cases moving forward, due to the lengthy postoperative restrictions, inability to return back to duty in a timely manner, and lengthy rehabilitation, we no longer recommend this surgery be performed in theater.
Introduction
Rupture of the pectoralis major tendon has historically been an uncommonly reported injury, however, more recent literature has demonstrated a substantial rise in the number of reported cases. 1 –5 The overwhelming majority of cases have occurred in the last two decades and the frequency continues to climb. 3,6 Injuries associated with weight lifting and cross-training are increasingly more common, coinciding with a rise in bench press injuries. 7 During the nadir of the bench press repetition, the pectoralis major tendon is most prone to rupture during eccentric contraction with the arm positioned in 30 degrees of extension and 40 degrees of abduction. 8 In this position, the caudal-most fibers of the tendon are at a substantial mechanical disadvantage and undergo twice the excursion of the superior fibers. 8 As sport-related activities and weight training surge in popularity, the incidence of pectoralis major tears appears to be growing. 3,9
Due to the relative infrequency of this condition, it may be missed on initial presentation or misdiagnosed as a sprain leading to delay in proper diagnosis and subsequent treatment. 10 Modern articles in the musculoskeletal literature are now focused on the diagnosis, management, surgical options, and identification of independent risk factors. Previous case reports and patient series of pectoralis major repairs in active duty US military personnel have been previously published. 1,2,5 We previously published our experience of pectoralis major tears in forward-deployed active duty troops, highlighting this as a population at risk. 11 The purpose of this follow-up study is to report on the midterm outcomes of the surgical repair of pectoralis major tears at one expeditionary medical treatment facility (MTF) over a 4-month deployment cycle and to affirm that in-theater surgical repair is technically possible.
Materials and methods
After institutional review board approval, retrospective analysis of the medical records and imaging of cases of pectoralis major tears evaluated and treated by the deployed US Air Force orthopedic surgeons at one expeditionary MTF over a 4-month deployment cycle from December 2013 through March 2014 was performed. 9 For purposes of operational security, the exact location of the MTF will remain undisclosed. However, it is important to note that this was a large role 3 permanent theater hospital that served as a tertiary referral center for the entire region and had a robust and sophisticated inter-theater care program. The hospital served as a regional hub for aeromedical evacuation and disposition from Afghanistan, the Middle East, and Africa. The facility had advanced and permanent inpatient, operating room, emergency room, dental, physical therapy, and intensive care unit capabilities. In addition, the hospital had advanced radiology services to include radiographs, ultrasound, and computed tomography scanning. Although still geographically within the area of operation for combat operations, the facility is located on a permanent US military base in an allied foreign country and was remote from any ongoing combat operations. All nine subjects were evaluated and treated by one of the facilities’ two orthopedic surgeons (DHS and WSC). Preoperative radiographs were obtained on each subject, and orthogonal x-ray views of the shoulder were used to rule out avulsion fractures. Diagnosis was made based on history and physical examination (Figure 1). Furthermore, for six of the nine individuals, noncontrast magnetic resonance imaging (MRI) scans were performed at a surrounding local foreign hospital and available for review to confirm the diagnosis and aid in preoperative planning (Figure 2). The MRI scans were performed at an academic modern urban medical center that was within close driving distance from the US military installation. Patient demographic data were recorded and used for comparisons; these included age, gender, rank, hand dominance, mechanism of injury, history of tobacco usage, and preexisting medical conditions. The Tietjen classification system of pectoralis major tendon ruptures was utilized to record the location and severity of each patient’s injury (Table 1). 12 Seven of the nine patients underwent operative pectoralis major repair at the expeditionary MTF and were able to complete their deployment without repatriation back to the United States. At the final follow-up disability of shoulder, arm, and hand (DASH) scores, American Shoulder and Elbow Society (ASES) shoulder scores and a previously published military pectoralis repair questionnaire were administered. 1

Clinical photograph of patient with left pectoralis tendon rupture, notice absence of the anterior axillary fold.

T2 axial MRI image of pectoralis major tear. MRI: magnetic resonance imaging.
Tietjen’s classification of pectoralis major injuries.

Surgery
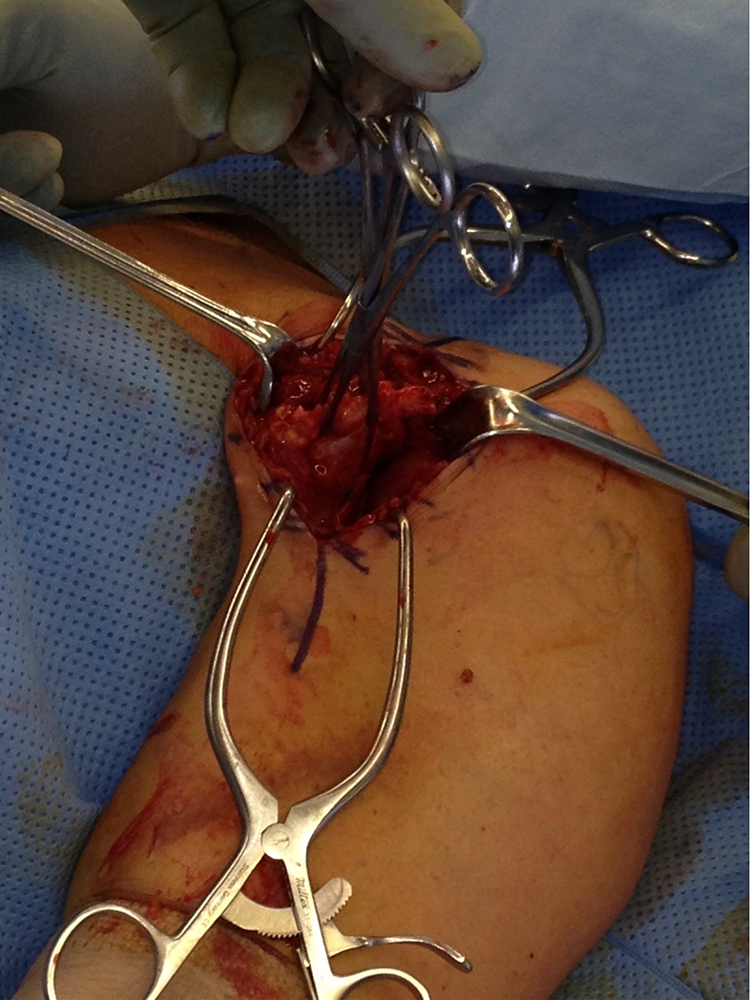
All operations were performed under general anesthesia, and local interscalene blocks were utilized to aid with intraoperative and postoperative pain control. The caudal portion of a standard deltopectoral incision was used for the approach. The cephalic vein was identified and retracted laterally with the deltoid muscle. Using palpation and blunt dissection, the medially retracted stump of the pectoralis major tendon was identified and grasped. Two #2 ultrastrong kevlar core sutures (Arthrex, Naples, Florida, USA) were then placed in a locking fashion into the stump of the pectoralis major tendon (Figure 3). The extra-articular portion of the long head of the biceps’ tendon was then identified in the bicipital groove. In five of the seven cases, a high-speed motorized burr was used to create a trough in the cortex of the anterior humerus in the footprint of the avulsed pectoralis major insertion, just lateral to the long head of the biceps (Figure 4). In the first case of the series (patient 1), the trough was created using a curette alone; however, in the subsequent six cases, it was discovered that the deployed military dentists had motorized burrs that could be sterilized and used in the operating room. Thus, in the successive cases, a 4-mm motorized burr was borrowed from the dental clinic and utilized to create the trough (Figure 5). Next, three 2.0-mm drill holes were placed in the humerus lateral to the trough. Free curved needles were then used to shuttle the #2 kevlar suture through the trough out the drill holes and the tendon was tied down over an osseous bridge (Figure 6). Care was taken to make sure that the tendon stump was docked completely into the trough. The wound was then copiously irrigated, the repair inspected, and hemostasis was obtained using electrocautery. Indwelling drains were not utilized. The braided suture was used to close the deltopectoral fascia. The wound was again irrigated and subcutaneous skin was closed using a 2-0 absorbable monofilament suture that was placed in a buried interrupted fashion with overlying 3-0 nylon placed in a horizontal mattress fashion. All patients were placed into a sling for the operative extremity.
Retrieval of the torn pectoralis major tendon.

Suturing of the end of the ruptured tendon.

Anterior humeral bony trough.

Tendon docking in the trough with transosseous repair.
Postoperative management and rehabilitation
All surgical patients underwent the same physical therapist supervised rehabilitation regiment. Patients were seen back for their first postoperative clinic appointment and wound check at 1 week and subsequently again at 2 weeks for suture removal. Postoperative restrictions were as follows:
Phase 1 (postoperative to 6 weeks): Active and active-assisted range-of-motion (RoM) of the elbow, wrist, and hand. Pendulum/Codman’s exercises of the shoulder were initiated. No lifting or weight bearing with the operative upper extremity. No active internal rotation or passive external rotation of the shoulder. No shoulder abduction.
Phase 2 (6 weeks to 4 months): The sling was discontinued completely and patients began therapist supervised progressive active and active-assisted RoM of the shoulder. Terminal forced passive external rotation or abduction was prohibited. No lifting of objects greater than 5 lbs.
Phase 3 (4–6 months) Patients continued in therapy and were advanced to unlimited active, active-assisted, and passive RoM of the left shoulder. Progressive light strengthening was initiated.
Phase 4 (6 months): Patients were allowed unrestricted stretching and strengthening and were allowed to resume full activity. Therapy was discontinued.
Results
The Titjen classification (Table 1) was utilized to classify pectoralis major tears in forward-deployed active duty military personnel. Nine male patients (five US Air Force and four US Army) were diagnosed with pectoralis major tears; their demographics are presented in Table 2. Seven complete tears at the tendinous insertion (Tietjen type IIID), one complete tear at the musculotendinous junction (Tietjen type IIIC), and one incomplete tear (Tietjen type II) with a mean age of 32 years (23–52). Seven of the nine service members underwent surgery in the forward-deployed setting. The patient with the incomplete tear (sternal head only) elected for nonoperative treatment and one patient was sent home and subsequently had surgery performed by an active duty orthopedic surgeon at MTF in the United States. All ruptures occurred during bench press with a mean weight of 258 lbs (135–415 lbs), with the dominant upper extremity involved 56% of the time. Table 3 demonstrates the mean length of deployment was 230 days (120–365), with injury occurring an average of 77 days into the members deployment (3–198 days). Mean time from injury to operative repair in the cohort was 18 days (10–43). Table 4 details the MRI findings of the cohort. For the seven patients who underwent surgery in the deployed setting, all patients had at least 4 years of follow-up (mean 49 months, range 48–51 months). At the final follow-up, the mean DASH score was 35.71 (range 31–41) and the mean ASES score was 90.71 (range 87–95). For the operative group, the average return to full preinjury function at work occurred at 7 months (range 4.5–10.5 months). For all seven patients who underwent surgery in the deployed setting, they rated their overall level of function after surgery as good or excellent. Additionally, 100% (7 of 7) stated that they were either satisfied or very satisfied with the results of the surgery. Full patient-reported outcome scores are detailed for each patient in Table 5. There were no reported complications, reruptures, or revision surgeries in the cohort who underwent surgery while deployed. The one patient who was sent back to his home duty station to have his pectoralis repair performed had a postoperative wound infection that was treated with serial irrigation and debridement and IV antibiotics via a peripherally inserted central catheter (PICC) line.
Patient demographics.

BOF: branch of service; SOI: side of injury.
aWeight = weight on the beach press bar at the time of injury.
bMechanism = mechanism of injury.
Timing of injury and surgery.

aNumber of days into the planned deployment that the injury occurred.
Advanced imaging results and injury classification.

Patient reported outcomes and questionnaire.

aNone, mild, moderate, or severe.
bExcellent, good, average, or poor.
cVery satisfied, satisfied, unsatisfied, or very unsatisfied.
Discussion
Rupture of the pectoralis major is a relatively rare injury, with the majority of cases in the modern literature having occurred in male athletes, in particular, weight lifters. 1 –4,9,13,14 The pectoralis major is a powerful adductor and internal rotator of the humerus. While low-demand or sedentary patients may have no difficulty with activities of daily living after nonoperative treatment, the inability to attain full strength without surgical repair necessitates operative treatment for the majority of athletes, active duty military personnel, and laborers. 3,9,13
In a recent prospective study performed on 60 consecutive patients with pectoralis major ruptures, the bench press exercise during weight lifting was implicated in 80% of the cases. 3 In our all-military cohort, bench press (bench press: seven flat, one incline, and one decline) was the mechanism of injury in all of the cases. The injuries are postulated to have occurred when a maximal force was applied with the pectoralis major eccentrically contracting during an abducted and externally rotated shoulder position. Cadaveric biomechanical studies have demonstrated that in the terminal 30° arc of shoulder extension, the shorter fibers of the inferior sternal head segments of the pectoralis major muscle lengthened 30–40% of their resting fiber length. This is nearly twice the amount of maximal excursion demonstrated in the more superior muscle fibers of the clavicular head and the upper segments of the sternal head. 8 Thus, heavy weights applied during eccentric loading during the nadir of the bench press exercise put the inferior sternal head segments at an extreme mechanical disadvantage and susceptible to injury. Our experience supports this theory; in the sole patient with an incomplete rupture, the clavicular head and a small portion of the superior segments of the sternal head were found intact while the remaining inferior sternal segments were avulsed from their humeral insertion.
Our series was composed of seven complete tears at the tendinous insertion (Tietjen type IIID), one complete tear at the musculotendinous junction (Tietjen type IIIC), and one incomplete tear (Tietjen type II), supporting previous reports that complete tears at the tendinous insertion are the most common type of pectoralis major rupture. 2,3,8,12,15 In a large prospective study of pectoralis major injuries, the anatomic location of the tear was described to be at the humeral insertion of the tendon in 57 of 60 patients (95%). 3 When the location of the rupture or the diagnosis is in question, MRI has been recommended to delineate the site and extent of the rupture, which may help surgeons with treatment options and surgical planning. 16 –19 However, due to the complex local anatomy and the rarity of the injury, it can be difficult on routine MRI to differentiate separate areas of muscle and tendon at the distal myotendinous junction. 16 Previous authors have recommended obtaining images with the upper extremity in the abducted and externally rotated position, the so-called “ABER” position to aid in differentiation. 16 Furthermore, the use of a surface coil is suggested to increase the signal-to-noise ratio, enhance spatial resolution, and increase the conspicuity of the injury. 17 In our cohort, advanced imaging was obtained for the first six patients. Because MRI imaging was not available at the US military treatment facility, we had to rely on local foreign hospitals, which often involved time delays, exorbitant costs, and travel. Table 4 details the MRI interpretations of the patients who underwent advanced imaging. In our experience, the official radiologist’s interpretation of the images correlated poorly with both the intraoperative grade and anatomic location of the injury. Furthermore, in some instances, the images were found to be of lower quality and often difficult for the operating surgeon to interpret. Thus, the practice of obtaining routine MRI imaging in clinically obvious pectoralis major tears was abandoned, as the additional data were not found to impact our treatment plans. We concluded that routine MRI imaging did not aid in the diagnosis or change the planned treatment of acute pectoralis major tears in this setting and was thus of limited value.
While the goal of all surgical repair techniques remains suture restoration to achieve an anatomic reduction of the tendon footprint while avoiding injury to the adjacent long head of the biceps, several methods have been described to reattach the avulsed tendon to its normal humeral insertion. 15,20 These methods have included suture anchors, cortical buttons, and troughs with the transosseous repair. 3,9,13,15,21 –24 Biomechanical studies have compared the strengths of the various techniques in an attempt to guide operative repair. 21 –23 In a recent cadaveric load to failure study of pectoralis major tendon repairs in the extended and abducted position, Rabuck et al. demonstrated that transosseous trough repair was stronger than suture anchor repair. 23 However, a subsequent biomechanical study based on peak failure loads demonstrated that unicortical buttons with #5 kevlar suture demonstrate a 61% greater construct strength over traditional bone trough technique. 15 Additionally, displacement after cyclic loading was substantially smaller with the unicortical bone button and suture/suture tape construct. 15 Thus, the available biomechanical data on ideal repair construct remain conflicted.
In our case series of forward-deployed active duty military personnel, seven complete ruptures were surgically repaired using bone trough and transosseous repair. This repair technique was not chosen solely due to the current biomechanical literature, but rather also out of necessity. Due to the deployed operating room setting, orthopedic implants such as cortical buttons and suture anchors are unavailable. The supply chain mechanism to source, stock, and maintain such implants at forward military hospitals does not currently exist.
Due to the infrequent nature of this injury, the literature is lacking large prospective studies, which makes identification of statistically significant modifiable risk factors and high-risk populations difficult. However, the male gender has been nearly ubiquitous in the reported cases throughout history and clearly remains a risk factor. 2 –4,6,9,14,16,25,26 Additionally, in a prospective study of 48 patients who sustained pectoralis major ruptures during bench press, 95.8% were found to have used anabolic steroids. 3 In a retrospective study of 257 military patients, Nute et al. demonstrated that 94% of individuals were able to return to the full preoperative level of function for active military duty following surgical repair of pectoralis major tendon rupture and only 5.4% of patients experienced rerupture after primary repair. 5 In their cohort, increasing body mass index and active psychiatric diagnoses were significant risk factors for an inability to return to preoperative functional levels and postoperative failures. 5 Our series included all males, however, none admitted to anabolic steroid usage. Because steroid usage among active duty military personnel is punishable under the Uniformed Code of Military Justice, there is a disincentive for the disclosure, and thus candid answers cannot be assured in this patient population.
Although pectoralis major ruptures have previously been described in the US military personnel, 1,2,5 there has never been a description of an increased incidence among forward-deployed troops. In a 4-month time period from December 2013 to March 2014, we saw acute pectoralis major ruptures in a forward-deployed patient population with an alarming occurrence rate. We hypothesize that this can be attributed to the increase in both intensity and frequency of physical training that occurs during deployments to the combat zone. We attempted to identify a time period during deployment that subjects were more vulnerable to this injury; however, no temporal relationship could be identified as we had one patient rupture 3 days into his deployment, while another patient ruptured 7 days prior to completion of his tour of duty. The mean time to injury on the deployment was 77 days into deployment.
This cohort demonstrates that in the appropriately indicated patient, surgery in the forward-deployed setting is technically possible and comparable clinical outcomes are achievable. With at least 4 years of postoperative follow-up, the mean DASH score was 35.71 (range 31–41) and the mean ASES score was 90.71 (range 87–95) for the seven patients who underwent surgery at a single expeditionary MTF during their deployment. The average return to full preinjury function at work for this cohort occurred at 7 months (range 4.5–10.5 months). All of the patients who underwent surgery in the deployed setting rated their overall level of function after surgery as good or excellent. Additionally, all seven patients reported they were either satisfied or very satisfied with the results of the surgery. There were no operative complications, reoperations, or reruptures in this series at final follow-up. These results are as good or better than the results published in other military personnel with pectoralis majors tears fixed operatively. 1,2,5
Due to the population makeup and size of our study, there are numerous limitations. First, because of the rigorous physical demands of the US military and the unique environment of a forward-deployed combat zone, our findings may not be generalizable to other patient populations. Additionally, due to the relatively small size of our cohort, identification of independent modifiable risk factors is statistically impossible. The constant cycle of forward deployment, geographic separation, operational tempo, and repatriation to home station for both the military physicians and patients limits the ability to perform routine follow-up or obtain advanced imaging to confirm tendon healing.
Conclusion
In conclusion, as we have previously published, deployed active duty US military personnel likely represent a high-risk population for pectoralis major ruptures. Future studies designed to identify the true incidence, report long-term outcomes, and investigate modifiable patient risk factors in this population are warranted. Our study demonstrates that surgical repair with a trough and transosseous repair technique was technically feasible and successful at this permanent US military in-theater tertiary referral medical center. Although this treatment may be considered in rare individual cases moving forward, due to the lengthy postoperative restrictions, inability to return back to duty in a timely manner, and lengthy rehabilitation, we no longer recommend this surgery be performed in theater.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Internally funded.