
Abstract
Background:
Anterior cruciate ligament (ACL) injury can lead to changes in tibiofemoral kinematics during gait, but the detailed short-term kinematic changes after ACL injury are still unknown.
Purpose:
To measure tibiofemoral kinematics during gait in ACL-deficient (ACLD) knees over time after ACL injury.
Study Design:
Controlled laboratory study.
Methods:
The authors categorized 76 patients with unilateral ACLD knees into 4 groups based on the time from injury: <3 months (group 1), 3 to 6 months (group 2), >6 to 12 months (group 3), and >12 months (group 4). The controls were 20 participants with ACL-intact knees. Changes in the knee kinematics and range of motion during gait were compared among ACLD groups and those with ACL-intact knees.
Results:
Compared with controls, the range of motion of flexion in group 1 was significantly lower (6°; P = .033), and the mean knee flexion was significantly increased (0.7°-3.4°) in groups 1 to 4 (all P ≤ .004). There was more internal tibial rotation (2.9°-4.3°) in group 1 and 2, and more anterior tibial translation (4.3 mm) in group 1 during the stance or swing phases than in controls (P ≤ .049 for all). The mean internal tibial rotation and anterior tibial translation significantly decreased from group 1 to group 4 (P < .001 for both). Compared with controls, the mean medial tibial translation was significantly greater (1.2-2.5 mm) in all groups, and more medial tibial translations (2.4-3.7 mm) were observed during the stance phase in groups 1, 3, and 4 (P ≤ .047 for all).
Conclusion:
ACLD knees displayed a motion impairment walking strategy within 3 months, and a higher-flexion walking strategy increased with time after injury. Excessive anterior translation and internal rotation of the tibia tended to return to normal, while excessive medial translation of the tibia increased in ACLD knees after 6 months postinjury. These results may provide new insight into the compensatory mechanisms and risk factors for premature osteoarthritis in ACLD knees.
Anterior cruciate ligament (ACL) injury can lead to joint instability and changes in tibiofemoral kinematics during gait. 27,35,43,47,49 Patients with ACL-deficient (ACLD) knees may develop compensatory gait mechanisms and have an increased risk of early-onset osteoarthritis, which provide support for treatment and rehabilitation for this condition. 2,13,29,45,47,49
There is no consensus regarding the kinematics of the ACLD knee during gait and other activities. 2,32,47,49,50 For instance, Zabala et al 47 have found that compared with the intact knee, the tibia of the ACLD knee exhibits more external rotation during gait relative to the femur, while Zhang et al 49 observed a more internal rotation across the entire gait cycle. Long-term changes in anterior-posterior (AP) translation and internal-external (IE) rotation in ACLD knees have been reported, and these changes are considered to relate to knee osteoarthritis. 47
In addition to AP translation and IE rotation, other aspects of the 6 degrees of freedom (DOF) kinematics of the knee (medial-lateral [ML] and proximal-distal [PD] translation; flexion-extension [FE] and varus-valgus rotation) are related to compensatory mechanisms or early-onset osteoarthritis in ACLD knees. These include patients with ACLD knees walking with less knee flexion throughout the mid- and terminal stance phases in order to decrease the anterior shear force on the tibia 5,19 and excessive medial tibial translation, which may accelerate joint degeneration. 9 Although factors such as walking speed 44 or calculation model 4 contribute to variations in the walking patterns of persons with ACLD knees, time postinjury is also an important factor to consider. 47 However, to our knowledge, the detailed short-term kinematic changes after ACL injury are still unknown.
The purpose of the present study was to systematically measure the 6 DOF tibiofemoral kinematics (translation and rotation of the tibia relative to the femur) during gait in ACLD knees over time after injury. Based on previous studies 29,47 on the general consensus of the timing of the treatment, we hypothesized that (1) kinematics would change over the first year after injury and (2) in addition to AP translation and IE rotation, ML translation and FE rotation would also vary with time after injury.
Methods
Participants and Groups
The study protocol was approved by our institutional review board, and written consent was obtained from all study participants. We enrolled 76 patients with unilateral ACLD knees as well as 20 individuals with ACL-intact (ACLI) knees as the controls for this study. The patients with ACLD knees all had complete ACL rupture as diagnosed by 2 senior orthopaedic surgeons (Y.L., H.X.) via history, clinical examination (Lachman test, anterior drawer test), and magnetic resonance imaging (MRI) scans. MRI evidence of ACL rupture was based on primary and secondary signs, following the guidelines of Vahey et al. 40 Patients in the ACLD group had no symptoms of knee instability during daily activities and were able to perform physical exercise in level 1 or 2 sports. 8 All knees in the ACLD and ACLI groups had full range of motion (ROM), and there was no history of injury, surgery, sign of inflammation, or joint effusion on the contralateral knee of the patients with an ACLD knee and both knees of the patients with ACLI. For the control group, we randomly chose 1 knee from each participant with ACLI for comparison.
Excluded were patients with knee pain during ambulation, a positive floating patella test (effusion, ≥50 mL), 49 neurological pathologies, back pain, fractures of the lower extremity, presence of a meniscal tear on MRI scans, or previous surgery (meniscectomies, ligament reconstruction or repair). Also excluded were ACLD knees with radiographic signs of osteoarthritis (Kellgren-Lawrence grades 3 and 4) 35,49 or grade 4 cartilage injuries (following the guidelines of Recht and Resnick 31 ). A clinical examination (medial and lateral stress test, McMurray test, posterior draw test) and MRI scans were utilized to exclude patients with concomitant or symptomatic ligament lesion in grade 3 injuries 5,9,50 and symptomatic or repairable meniscal tears 5,50 at the time of the test.
To analyze changes in tibiofemoral kinematics over time, we divided the patients with ACLD knees into 4 groups according to the time after ACL injury: <3 months (group 1; n = 24); 3 to 6 months (group 2; n = 13); >6 to 12 months (group 3; n = 16); and >12 months (group 4; n = 23) (Figure 1). There were no significant differences in descriptive data between the ACLD and ACLI groups (Table 1).

Flowchart of participant enrollment. ACLD, anterior cruciate ligament deficient; ACLI, anterior cruciate ligament intact.
Participant Characteristics a

a Data are reported as mean ± SD unless otherwise indicated. ACLD, anterior cruciate ligament deficient; ACLI, anterior cruciate ligament intact; NA, not applicable; NS, not significant.
b Statistically significant difference between ACLD and ACLI knees (P < .05).
Imaging Procedure and Gait Analysis
A novel marker-based motion analysis system (Opti Knee; Shanghai Innomotion Inc) was used to collect motion data of the knee during gait. 49,50 The measurement space for this study was 4.0 × 2.0 × 2.5m. 49 Two rigid bodies, each fitted with 4 infrared light-reflecting markers (OK_Marquer; Shanghai Innomotion Inc), were fixed to the participants’ thighs and lower legs using bandages. An integrated 2-head stereo-infrared camera (NDI Polaris Spectra; Canada Northern Digital Inc) at a frequency of 60 Hz was used to track 3-dimensional trajectories of these rigid bodies with an accuracy of 0.3 mm root mean square. 49,50 This system has a repeatability of <0.9 mm in translation and <1.3° in rotation. 49,50 A handheld digitizing probe with 4 infrared light-reflecting markers was used to determine the horizontal plane on the treadmill (Bipace; Shanghai Innomotion Inc), as well as anatomic landmarks of the lower limb, including the greater trochanter, lateral epicondyle, medial epicondyle, lateral plateau, medial plateau, tibial tuberosity, fibular head, medial malleolus, and lateral malleolus 49,50 (Figure 2). To differentiate the gait phases, we applied an integrated synchronous high-speed camera (Basler aca640-90uc; Germany Basler AG) to capture images from the gait activities. Customized software (Opti-Knee Version 1.0; Shanghai Innomotion Inc) was employed to perform real-time calculations of knee motion during gait.
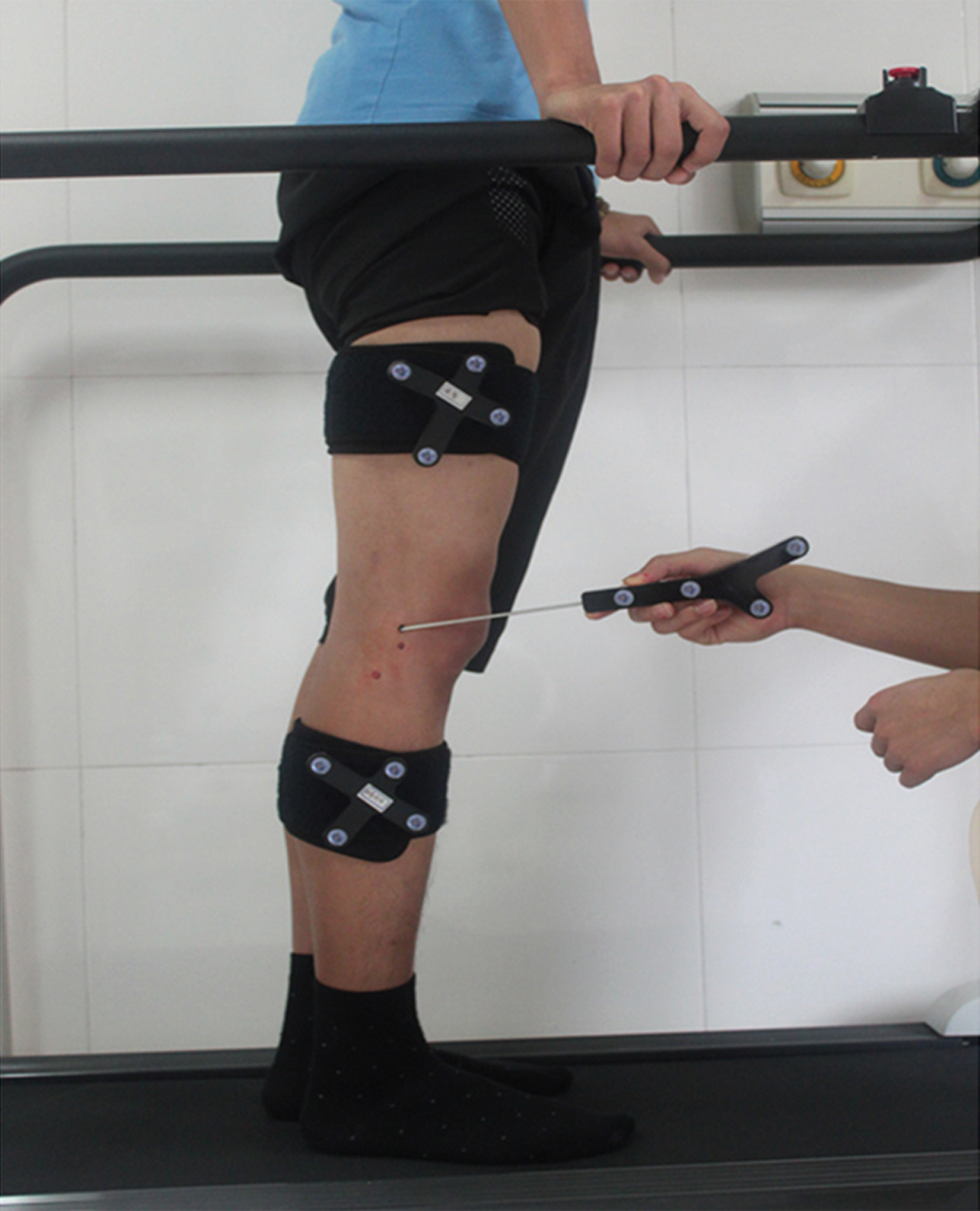
Two rigid bodies, each fitted with 4 infrared light-reflecting markers (OK_Marquer), were fixed to the participants’ thighs and lower legs using bandages. A handheld digitizing probe with 4 infrared light-reflecting markers was used to determine the femoral and tibial anatomic landmarks.
The static standing position (standing with feet placed a shoulder width apart and toes facing forward) was used as a reference for the initial anatomic frame. All participants received 5-minute walk training on the treadmill to ensure that the walking pattern was similar to a normal over-the-ground gait. 49 After adequate training, the patients were asked to walk on a flat treadmill at a normal self-selected speed, 5 and we recorded knee motion for 15 seconds at a frame rate of approximately 60 Hz. A total of 20 gait cycles per participant were recorded, and the mean values of the 6 DOF tibiofemoral kinematics for all cycles were calculated.
The coordinate systems of the femur and tibia were established based on the respective bone landmarks (Figure 3). 49,50 For the femur, the clinical transepicondylar axis (c-TEA) was defined as the ML axis that connected the extremes of the medial and lateral condyles. The AP axis of the femur was drawn perpendicular to the plane defined by the greater trochanter and c-TEA. The PD axis was set to be perpendicular to the other 2 axes. The midpoint of the c-TEA was defined as the origin of the femoral coordinate system. Regarding the coordinate system of the tibia, the ML axis was defined by connecting the prominent medial and lateral points of the tibial plateau. The AP axis of the tibia was drawn perpendicular to the plane defined by the lateral malleolus and ML axis. The PD axis was drawn perpendicular to the AP and ML axes. The origin of the tibial coordinate system was defined as the midpoint of the tibial ML axis.

Definition of local coordinate system of the femur and tibia. For the femur, the clinical transepicondylar axis (c-TEA) was defined as the medial-lateral (ML) axis that connected the extremes of the medial and lateral condyles. The anterior-posterior (AP) axis was drawn perpendicular to the plane defined by the greater trochanter and c-TEA, and the proximal-distal (PD) axis was perpendicular to the other 2 axes. The midpoint of the c-TEA was defined as the origin of the femoral coordinate system. For the tibia, the ML axis was defined by connecting the prominent medial and lateral points of tibial plateau, the AP axis was drawn perpendicular to the plane defined by the lateral malleolus and ML axis, and the PD axis was drawn perpendicular to the AP and ML axes. The origin of the tibial coordinate system was defined as the midpoint of the tibial ML axis.
The marker position data were smoothed using a fourth-order Butterworth low-pass filter (cutoff frequency, 6 Hz). An optimization algorithm was used to determine the 3-dimensional dynamic posture of the thigh and lower leg, including the skin markers on each segment during gait. 36 Subsequently, tibiofemoral joint translations and rotations were quantitatively measured based on the femoral and tibial coordinate systems using a customized program written in MATLAB (MathWorks Inc). 49,50 Knee translation (ie, AP, ML, and PD translations) was defined as the motion of the tibial origin relative to the femoral coordinate system. 28 Rotations of the knee joint (ie, FE, IE and varus-valgus rotation) were calculated using the Cardan angle sequence described by Grood and Suntay. 21
The gait cycle was then normalized (0%-100% heel strike) and divided into a stance phase (0%-62%) and a swing phase (62%-100%). The stance phase was further divided into 3 parts: loading response (ie, early stance; 0%-12%), midstance (12%-52%), and terminal stance (52%-62%). The swing phase was also divided into 3 parts: initial swing (62%-75%), midswing (75%-85%), and terminal swing (85%-100%). 49
Statistical Analysis
Descriptive statistics were recorded as means and standard deviations. A 1-way analysis of variance and post hoc pairwise comparison (Newman-Keuls test) were used to analyze the 6 DOF tibiofemoral kinematics (translation and rotation of the tibia relative to the femur) at key events in the gait cycle (12% [loading response], 52% [midstance], 62% [terminal stance], 75% [initial swing], and 85% [midswing]) (all P values of post hoc testing are shown in Supplemental Material Table S1). Two-way analysis of variance and post hoc testing were performed to compare the tibiofemoral kinematics among the groups. Differences were considered statically significant if P < .05. All statistical analysis was performed using SPSS Version 24 (IBM Corp). A post hoc power analysis was performed using software G*Power (Version 3.1.9), 12 and the relationship between each DOF and time from ACL injury was calculated as follows: 0.99 in knee FE, 0.99 in tibial IE rotation, 0.90 in tibial AP translation, and 0.99 in tibial ML translation.
Results
Figure 4 shows the mean 6 DOF tibiofemoral kinematics during an entire gait cycle for ACLI and ACLD knees, and Figure 5 shows the ROM for each kinematic parameter. The overall mean values are shown in Table 2, and the values at key events during the gait cycle are shown in Table 3.
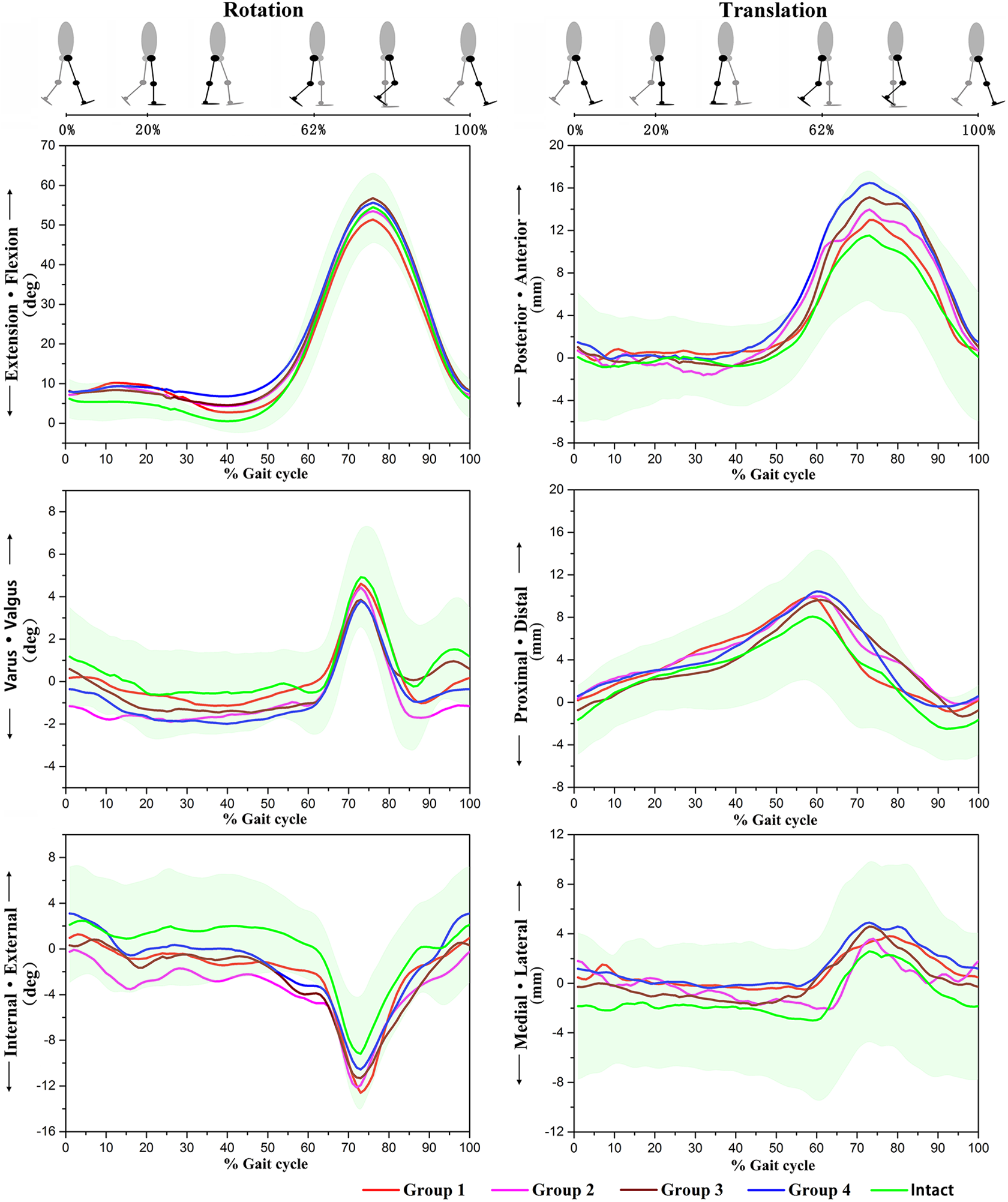
Mean values for the 6 degrees of freedom tibiofemoral kinematics during a single gait in anterior cruciate ligament–deficient knees and –intact knees. Negative values indicate extension, internal, or varus rotation or posterior, lateral, or proximal translation. The shaded area indicates the SD.
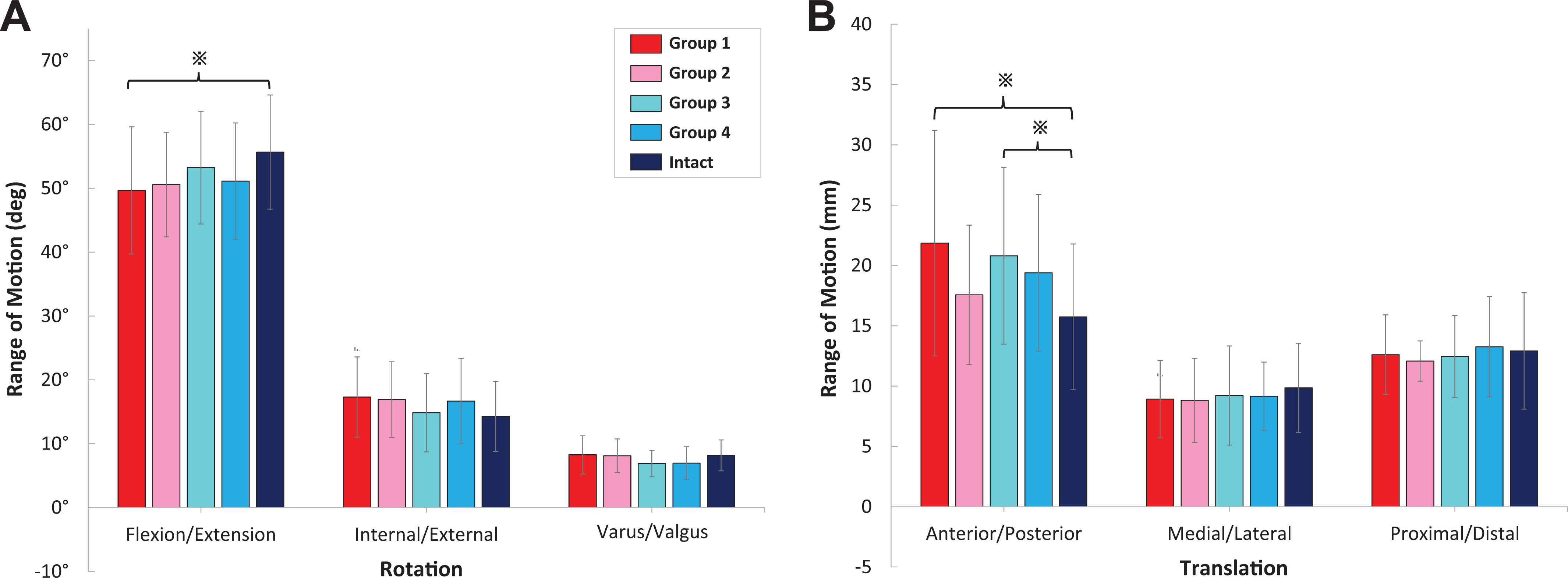
Range of motion for (A) rotation and (B) translation of the anterior cruciate ligament–deficient and –intact groups during the treadmill gait test. Error bars represent SDs. *Statistically significant difference (P < .05).
Overall 6 DOF Tibiofemoral Kinematics During the Treadmill Gait Test in ACLI and ACLD Knees a

a Data are reported as mean ± SD. ACLD, anterior cruciate ligament deficient; ACLI, anterior cruciate ligament intact; DOF, degrees of freedom.
b Statistically significant difference (P < .05) compared with intact group.
c Statistically significant difference (P < .05) compared with group 1.
d Statistically significant difference (P < .05) compared with group 2.
e Statistically significant difference (P < .05) compared with group 3.
6 DOF Tibiofemoral Kinematics According to Key Events of the Gait Cycle for ACLI and ACLD Knees a
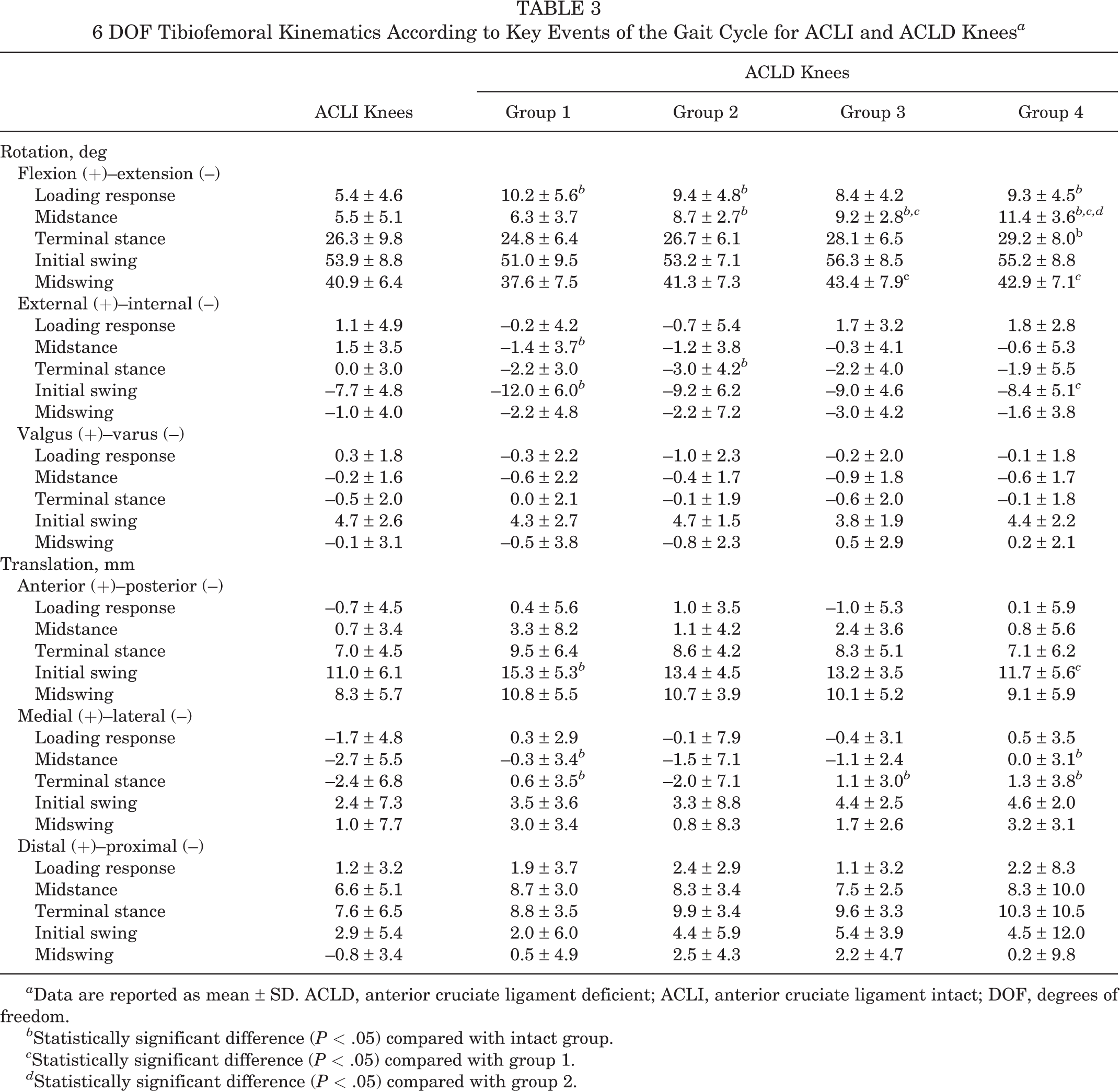
a Data are reported as mean ± SD. ACLD, anterior cruciate ligament deficient; ACLI, anterior cruciate ligament intact; DOF, degrees of freedom.
b Statistically significant difference (P < .05) compared with intact group.
c Statistically significant difference (P < .05) compared with group 1.
d Statistically significant difference (P < .05) compared with group 2.
Rotation
In terms of knee flexion, the mean flexion angle over the gait cycle of the ACLD knees was higher than that of the ACLI knees (P ≤ .008), and the mean knee flexion of the ACLD knees was significantly increased (0.7°-3.4°) in group 1 to 4 (P ≤ .004) (Table 2). During gait, ACLD knees flexed more in the terminal timing of loading response (except group 3) and midstance (except group 1) than did ACLI knees (P ≤ .024) (Figure 4 and Table 3). The total ROM during the entire gait cycle of ACLD knee flexion in group 1 was 6° greater than that of ACLI knees (P = .033). No significant differences were found among ACLI and ACLD knees in groups 2 to 4 (Figure 5A).
Tibias in the ACLD knees rotated more internally than in the ACLI knees within 1 year (groups 1, 2, and 3; P < .001). However, the excessive internal tibial rotation in ACLD knees decreased with time (P ≤ .002), and no significant difference was observed between ACLD knees in group 4 and ACLI knees (P = .224) (Table 2). In terminal timings of midstance (P = .021) and initial swing (P = .010), the internal tibial rotations were 2.9° and 4.3°, respectively, more pronounced in group 1 than in the ACLI knees and 3° more pronounced in group 2 than the intact group in the terminal stance period (P = .048). No more significant differences were observed after 6 months between ACLD and ACLI knees (groups 2, 3, and 4) (Figure 4 and Table 3).
In the frontal plane, ACLD knees rotated with more varus than did ACLI knees on average (P ≤ .004), but ACLD knees in groups 3 and 4 rotated with less varus than did those in group 2 (P = .004 and P < .001, respectively) (Table 2). No other significant differences in knee kinematic parameters or ROM were found between the ACLD and ACLI knees in the frontal plane (Table 2 and Figures 4 and 5A).
Translation
Regarding AP translation, ACLD knees in groups 1, 2, and 4 showed more anterior tibial translation than did intact knees (P ≤ .033). Among ACLD knees, excessive anterior tibial translations relative to normal were less with time in groups 3 and 4 than in groups 1 and 2 (all P < .001) (Table 2). Within 3 months postinjury (group 1), the mean anterior tibial translation was 4.3 mm more than that in the ACLI group in terminal timing of the initial swing (P = .007), but no difference was found between ACLI knees and groups 2, 3, and 4 (Figure 4 and Tables 2 and 4). In groups 1 and 3, the ROM of AP translation was greater in ACLD knees than in intact knees (P = .007 and P = .041, respectively) (Figure 5B).
The tibia exhibited 1.2 to 2.5 mm more medial shift relative to the femur in all groups compared with that of ACLI knees (all P < .001), and excessive medial translation in group 4 was greater than that in the other ACLD groups and intact knees (all P < .001) (Table 2). More medial tibial translations (2.4-3.7 mm) were observed during the stance phase in groups 1, 3, and 4 (P ≤ .047 for all). Regarding PD direction, tibias in all groups of ACLD knees translated less than 2 mm more distally relative to the femur compared with the intact knees (all P < .001) (Table 2).
Discussion
Our findings supported our hypothesis that all 6 DOF in ACLD knee kinematics would vary with time after injury. ACLD knees showed a significant decrease in FE ROM and knee function scale during gait within 3 months after injury and displayed high degrees of flexion with time. The increases in anterior translation and internal rotation of ACLD knees were significant within 3 to 6 months after injury but gradually returned to normal. Significantly increased medial translation of the tibia was observed 6 months after ACL injury.
Gait is a common activity of daily living. 7 Knee kinematics during gait have been used as the baseline reference for the diagnosis, treatment, and rehabilitation of knee injuries and osteoarthritis. 9,47 Many techniques can be applied to study knee kinematics during gait. The biplane imaging technique is highly accurate for measuring knee kinematics in vivo during gait 24,41 ; however, it provides only limited fields of view and involves radiation exposure from computed tomography or radiography. 3 Optical motion analysis systems, the technique we used in this study, integrate data from the stereo-infrared and high-speed camera to measure knee kinematics and provide visual data simultaneously. The accuracy of this system is comparable with that of other conventional motion systems, with no need for x-ray beam exposure. This system has been used in previous studies to measure kinematics in knees with or without ACL injuries. 47,49,50
The study results showed that the FE rotation of ACLD knees during gait changed with time postinjury. In the early stage after ACLD, we observed a significant reduction in the FE ROM of the ACLD knees during gait. Knee motion impairments in patients with acute ACLD knees have been reported in a previous study because of the insufficient muscle strength in the quadriceps and hamstring. 18 The strategy to reduce knee movement and muscle activities may prevent patients with ACLD from being injured again. 18 These lower muscle activities may be because of nervous system adaption, anxiety of patients, or pain from the “bone bruise” on the distal lateral femur (which would see more pressure with terminal knee extension) after ACLD. 16,18,19 However, there was no significant difference in FE ROM between the ACLD knees and the ACLI knees 3 months after injury. Apart from the possibility that the bone bruises are resorbed with time, 20,39 symmetry movement and physical function of ACLD knees has been shown to be related to the restoration of muscle strength after injury. 10,25 Therefore, this phenomenon indicates that the patients might gradually recover their muscle strength within 3 to 6 months after injury. In addition, we observed that the ACLD knees had a greater flexion angle than did the ACLI knees and the flexion angle differences were greater with more time after injury. Higher knee flexion angles during gait after ACL injury have also been reported previously, 15,22 and this may mainly be because of the greater degree of hamstring activation or less quadriceps forces (quadriceps avoidance) to avoid excessive anterior tibial displacement, thus reducing the need for ACL function. 6,14,30,32 Since the current study indicated that this high-flexion angle became greater with more time after injury, this suggests that the high-flexion compensatory strategies with activation of compensated hamstring contractions might increase with time postinjury. In general, motion impairment strategies might mainly occur within 3 months after ACL injury, and high-flexion gait strategies occur and increase with time from injury. These relations between time postinjury and the compensatory strategies in ACLD knees were the novel finding in the present study.
We found that the tibia translated more anteriorly by an average of 1.8 mm and rotated more internally by an average of 2.2° in ACLD knees than in intact knees within 3 months after injury. There was significantly greater anterior translation with an average of 4.3 mm in the swing phase and more internal rotation with an average of 3° in the stance phase of the tibia in ACLD knees than in intact knees between 3 and 6 months. Previous studies reported similar results for patients soon after ACL injury during gait. 17,46 However, with time, more normal tibiofemoral kinematics in IE rotation and AP translation in ACLD knees was gradually restored, and no significant abnormalities were found in the stance or swing phase during gait 6 months after injury. The time dependency of the kinematic changes in AP translation and IE rotation suggests a compensatory phenomenon of ACLD knees such that abnormalities in AP translation and IE rotation would gradually return to normal 3 to 6 months after the injury. Conversely, it is plausible to consider that there are no effective mechanics of ACLD knees to compensate for the excessive anterior tibial translation and internal tibial rotation within 3 months of ACL injury. Longitudinal studies are needed to validate this inference. Some studies have reported that excessive internal tibial rotation and anterior tibial translation in ACLD knees could result in injuries to the meniscus and cartilage. 33,34 There is a possibility that knees may have a higher risk of reinjury or further injury to the cartilage and menisci within 3 to 6 months of ACL deficiency because of kinematic abnormalities in AP translation and IE rotation, so patients should avoid performing intense sports related to knee torsion or hyperextension within this period of time. In addition, when ACL reconstruction is required to restore the abnormal kinematics of ACLD knees, earlier reconstruction may be recommended to lower the risk of reinjury, especially within 3 to 6 months after injury.
We found that the restoration of the kinematic abnormalities of ACLD knees in IE rotation and AP translation with time was accompanied by an increase in the mean knee flexion angle during gait. Studies have reported that greater degrees of knee flexion or knee flexion moment in ACLD knees were related to greater activity of hamstrings during walking. 14,26 Furthermore, hamstrings have been shown to provide rotational stability for the knee and prevent the knee from excessive anterior tibial translation. 1,37,38 It is plausible to speculate that the activities of hamstrings may gradually increase with time postinjury to compensate for the loss of ACL function. Building hamstring strength may be important for nonoperative treatment for patients with ACLD knees. Therefore, orthopaedic surgeons and physical therapists should consider this when choosing hamstring autografts for reconstruction, especially for elite athletes. However, we did not measure muscle strength in the current study. Future studies are needed to investigate the relationship between changes in the activities of the muscles of the lower limb (especially the hamstrings) and the time post–ACL injury during all kinds of daily activities.
More medial translation of the tibia was observed in ACLD knees than ACLI knees during gait, comparable with findings that were previously reported. 9 This indicates that ACL has function to limit excessive medial translation of the tibia relative to the femur. The excessive medial shift of the tibia in ACLD knees might be associated with cartilage degeneration and osteoarthritis in patients with chronic ACLD knees. 9 ACL rupture has been considered to be associated with increased risk for early-onset osteoarthritis, and the progression of the knee OA is related to the altered kinematics of the knee after injury. 11,23,42 Since the primary function of the ACL is considered to limit excessive anterior translation and internal rotation of the tibia relative to the femur, previous studies have focused on the role of the changes in AP translation and IE rotation in early-onset osteoarthritis after ACL injury. 11,42,47 Although our data also demonstrate the abnormalities in AP translation and IE rotation after ACL injury, these abnormities tend to return to normal after 6 months postinjury. On the contrary, abnormality in ML translation increased with time 3 to 6 months after injury. Thus, abnormality in ML translation might be an important long-term factor for knee joint degeneration in chronic ACLD knees, which has not been reported previously. Therefore, even for ACLD knees in the absence of instability symptoms, reconstruction surgery may be recommended to reduce the risk of premature osteoarthritis. Future longitudinal studies are needed to verify these two inferences mentioned above.
Limitations
There were several limitations in this study. This system did not include a pressure sensor or force plate to objectively measure the key events during gait. Nevertheless, a synchronous high-speed video camera that captured 60 snapshot images per second was used to record and distinguish the key events of the heel strike and toe-off, 48,49 both of which require additional knowledge and are time-consuming. The time after injury in patients with ACLD knees was generally short during the current investigation (average, 43.1 ± 31.6 months in group 4), and the relatively small sample size may also be considered a limitation. More prospective studies with larger numbers of patients with long-term and chronic ACLD knees would be beneficial for understanding the relationships among ACL injuries over time, as well as the kinematics and compensatory mechanisms of ACLD knees. Additionally, for the safety of patients with ACLD knees while they were tested on the treadmill, the current study only included those who were able to perform physical exercise in level 1 or 2 sports and had no symptom of knee instability during daily activities. Thus, the results do not represent the gait abnormalities of those with instability or unable to perform physical exercise in level 1 or 2 sports as a result of their ACL injury. Another limitation was the use of marker tracking techniques that could lead to soft tissue artifacts. 47 The technology we used was stereo-infrared technology with a high-speed camera that measured knee kinematics with an accuracy of 0.3 mm root mean square. 49,50 The system has a repeatability of less than 0.9 mm in translation and 1.3° in rotation. 1 This is comparable with the conventional motion capture analysis systems 1 and has been applied in previous studies. 49,50 Finally, no muscle activities were measured in the present study; therefore, there could be no clear conclusions drawn regarding compensatory muscle contractions in ACLD knees. Further relevant investigations using electromyograms and force plate data are needed to validate these results.
Conclusion
ACLD knees displayed a motion impairment walking strategy with lower knee function within 3 months and a high-flexion walking strategy with time postinjury. Excessive anterior translation and internal rotation of the tibia tended to return to normal after 6 months postinjury, while the excessive medial translation of the tibia increased with time. Walking strategies and kinematic abnormalities have been shown to relate to muscle adaption, increased risk of cartilage injury, meniscal tear, and premature osteoarthritis in ACLD knees. Therefore, this kinematic study may provide new insight into the compensatory mechanism, timing of ACL reconstruction, and osteoarthritis mechanism in ACLD knees.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671221110160.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221110160 - Effect of Time After Injury on Tibiofemoral Joint Kinematics in Anterior Cruciate Ligament–Deficient Knees During Gait
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221110160 for Effect of Time After Injury on Tibiofemoral Joint Kinematics in Anterior Cruciate Ligament–Deficient Knees During Gait by Changzhao Li, Yulin Lin, Willem A. Kernkamp, Hong Xia and Zefeng Lin in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank the volunteers who participated in this study.
Final revision submitted March 1, 2022; accepted March 22, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Key Laboratory of Trauma & Tissue Repair of Tropical Area of China, the Science and Technology Planning Project of Guangdong Province of China (grant No. 2017B030314139), the Natural Science Foundation of Guangdong Province of China (grant No. 2015A030312004), and the Medical Research Foundation of Guangdong Province (No. A2019228). The results of the present study do not constitute endorsement by the American College of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the General Hospital of Southern Theatre Command.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.