
Abstract
Background:
The rate of return to sport after surgical treatment of femoroacetabular impingement (FAI) syndrome (FAIS) has been studied in high-level athletes. However, few studies examining this rate have focused exclusively on National Collegiate Athletic Association (NCAA) Division I athletes.
Purpose:
To evaluate the return-to-sport rate after hip arthroscopy for FAIS and to examine the influence of sport type on the clinical presentation of FAIS in collegiate athletes.
Study Design:
Case series; Level of evidence, 4.
Methods:
Included in this study were NCAA Division I student-athletes who underwent hip arthroscopy for FAIS at our institution between 2010 and 2017. Exclusion criteria were history of previous hip pathology, pediatric hip disease, radiographic evidence of osteoarthritis (Tönnis grade >0), prior lower extremity procedure, history of chronic pain, osteoporosis, or history of systemic inflammatory disease. Athletes were categorized into 6 subgroups based on the type of sport (cutting, contact, endurance, impingement, asymmetric/overhead, and flexibility) by using a previously reported classification system. Patient characteristics and preoperative, intraoperative, and return-to-sport variables were compared among sport types.
Results:
A total of 49 hip arthroscopies for FAIS were performed in 39 collegiate athletes (10 females, 29 males; mean age, 19.5 ± 1.3 years). A total of 1 (2.6%) cutting athlete, 15 (38.5%) contact athletes, 8 (20.5%) impingement athletes, 6 (15.4%) asymmetric/overhead athletes, and 9 (23.1%) endurance athletes were included in the study. There were no differences among sports groups with respect to the FAI type. Endurance athletes had lower rates of femoral osteochondroplasty (45.5%) and labral debridement (0.0%) (P < .0001). Contact sport athletes had higher rates of labral debridement (50.0%; P < .0001). Patients were evaluated for return to sport at an average of 1.96 ± 0.94 years. Overall, the return-to-sport rate was 89.7%. There were no differences in return-to-sport rates based on the sport type except for endurance athletes, who returned at a lower rate (66.6%; P < .001). No differences in return-to-sport rate (P = .411), duration after return (P = .265), or highest attempted level of sport resumed (P = .625) were found between patients who underwent labral repair versus debridement.
Conclusion:
Collegiate-level athletes who underwent hip arthroscopy for FAIS returned to sport at high and predictable rates, with endurance athletes possibly returning to sport at lower rates than all other sport types. Surgical procedures may be influenced by sport type, but the rate of return to sport between athletes who underwent labral debridement versus labral repair was similar.
Femoroacetabular impingement (FAI) syndrome (FAIS) 11 is a common diagnosis in high-level athletes who present with hip pain. 3,13,19,27 Numerous sports, including popular collegiate activities (soccer, football, ice hockey, etc), have been associated with increased risk for the development of FAIS. 6,22,25 Nawabi et al 19 categorized the different sports into 6 groups (cutting, contact, impingement, endurance, asymmetric/overhead, and flexibility sports) based on the biomechanical demand on the hip, to better understand the development and clinical course of FAIS in athletes. Cruz et al, 6 in a study of National Collegiate Athletic Association (NCAA) athletes using this classification, showed that impingement sports are most commonly associated with hip injuries and have the highest rate of hip procedures among all sport types.
After an unsuccessful trial of nonoperative therapy, arthroscopic hip surgery is the gold standard treatment for FAIS in athletes. 2,3,11,19 The purpose of hip arthroscopy is to correct the FAI-related chondrolabral and/or osseous abnormalities, eliminate the athlete’s symptoms, and facilitate the athlete’s return to sport. 2,26 In addition, this procedure might delay the development of early osteoarthritis. 10 Recent evidence 4,7 –9,21,23 has shown that after arthroscopic hip surgery, high-level athletes (professional, collegiate, and high school) return to sport at predictable levels that range from 83% to 93%. The epidemiology, radiographic findings, and clinical characteristics of FAIS in collegiate athletes have been previously reported. 6,14,15,20 However, there is a lack of sport-specific analysis of the preoperative, intraoperative, and return-to-sport factors focusing exclusively on NCAA Division I athletes.
The purpose of this study was to examine the manifestation of FAIS and return-to-sport parameters (rate of return, time to return, and level of competition) after arthroscopic hip surgery in a group of NCAA Division I athletes, based on the sport type as described by Nawabi et al. 19 We hypothesized that the preoperative, intraoperative, and postoperative parameters would differ according to sport type.
Methods
Patient Selection
Institutional review board approval was obtained before study initiation. All NCAA Division I student-athletes at our institution who had hip arthroscopy for FAIS from January 2010 through December 2017 were identified via a retrospective chart review (Laserfiche Content Management System). Inclusion criteria were diagnosis of FAIS, 11 failure of nonoperative management (including physical therapy, activity modification, and/or oral nonsteroidal anti-inflammatories), and participation in an NCAA Division I athletic team at the University of Southern California.
Preoperative diagnosis was based on the presence of hip pain and radiographic evidence of FAI (cam FAI, pincer FAI, or mixed FAI) as evidenced in the radiology report. The surgical report was used to record the intraoperative procedures performed. Postoperative return-to-sport information was gathered from physical therapy notes and physician clinic notes. Return-to-sport time for players with bilateral hip surgeries was based on time from the most recent procedure. Exclusion criteria included a history of previous hip pathology, pediatric hip disease, radiographic evidence of osteoarthritis (Tönnis grade >0), prior lower extremity procedure, history of chronic pain, osteoporosis, or history of systemic inflammatory disease.
Characteristic Data
Preoperative characteristic data recorded were patient age, sex, and sport type. Athletes were classified into 1 of 6 sport categories based on similar mechanical demands of their individual sports. This system has been used in previous studies 19,29 to group athletes. The categories included cutting sports (soccer, basketball, lacrosse, and field hockey), flexibility sports (dance, gymnastics, figure skating, yoga, and martial arts), contact sports (football, wrestling, and rugby), impingement sports (hockey, crew, water polo, baseball catcher, and breaststroke swimmer), asymmetric/overhead sports (baseball, softball, tennis, golf, and volleyball), and endurance sports (track, cross-country, other running, cycling, and swimming [other than breaststroke]).
Surgical Technique
A total of 5 surgeons performed hip arthroscopy on the athletes during the study period. The major surgical steps and technique did not differ between the surgeons. All hip arthroscopies were performed with the patient in the supine position. Standard anterolateral and midanterior arthroscopic portals were established. A combination of the interportal capsulotomy and T-capsulotomy technique was used. The acetabular labrum was debrided only when it was irreparable; otherwise, labral repair was performed by using suture anchors. The offended acetabular or femoral osseous lesion was resected by using a bur, while excision of soft tissues was accomplished by using an arthroscopic shaver. A radiofrequency ablator was used mainly for hemostasis.
Rehabilitation
Postoperatively, all athletes followed the standard rehabilitation protocol used in our institution for athletes who have undergone surgical management of FAIS. This 24-week long program consists of 5 phases of postoperative activity, with adjustments in the patient’s cardiovascular activity, hip range of motion, and weightbearing status of the operated lower extremity that are specific to each phase (Figure 1).

Standard phase 1-5 rehabilitation protocol after arthroscopic treatment of FAIS. ABD, abduction; ADD, adduction; AROM, active range of motion; DL, double leg; ER, external rotation; EXT, extension; FABER, flexion abduction external rotation; FAIS, femoroacetabular impingement syndrome; FLEX, flexion; GLUTS, gluteals; IR, internal rotation; ITB, iliotibial band; L/S, lumbar spine; PROM, passive range of motion; RDL, Romanian deadlift; SL, single leg; TFL, tensor fascia lata; TKE, thigh knee extension; UE, upper extremity.
Statistical Analysis
Clinical data were analyzed by using the STATA 16 statistical platform (StataCorp). Characteristic data are presented as means and standard deviations or percentages where appropriate. Characteristic, preoperative, intraoperative, and postoperative variables were compared among sport types. Categorical variables were analyzed with the chi-square test, and statistically significant differences between groups were identified by using standardized residuals >2 SDs from the expected values. An alpha value of <.05 was used for evaluating the statistical significance.
Results
Characteristic Data
A total of 49 hip arthroscopies in 39 collegiate athletes were performed between January 2010 and December 2016 (Table 1). The mean patient age at the time of surgery was 19.5 ± 1.3 years, and there were 10 female athletes (25.6%) and 29 male athletes (74.4%). Preoperatively, the majority of hips had mixed-type FAI (65.3%) followed by isolated cam type (32.7%) and 1 isolated pincer type (2.0%). Of the 5 surgeons involved, 1 (J.S.) performed 75.5% (37/49) of the arthroscopies.
Characteristics and Preoperative and Intraoperative Data for Collegiate Athletes by Sport Type a

a Data are expressed as n (%). FAI, femoroacetabular impingement; HO, heterotopic ossification.
b Significantly different from group by post hoc testing of chi-square–adjusted residuals.
c According to number of hips.
Intraoperative Data
Intraoperatively, 39 hips (79.6%) underwent cam lesion decompression with femoral osteochondroplasty and 15 (30.6%) required acetabular rim trimming. All patients had a labral tear identified intraoperatively, with 36 hips (73.5%) treated with labral repair and 11 hips (22.4%) treated with labral debridement. Ten hips (20.4%) required microfracture for focal, full-thickness chondral defects of the acetabulum. A total of 11 (28.2%) athletes underwent bilateral procedures. All were staged procedures and occurred a mean of 2.8 ± 4.7 months apart, with 1 athlete undergoing the bilateral procedures multiple years apart from one another. There were no significant differences in demographic, radiographic, or operative characteristics between bilateral and unilateral athletes. The return-to-sport data for the bilateral study population were collected with respect to the most recent surgical procedure.
Complications
Table 2 presents the postoperative complications in 4 athletes (4 hips) who required subsequent surgery.
Postoperative Complications, Treatment, and Clinical Outcome a

a NSAID, nonsteroidal anti-inflammatory drug.
Analysis by Sport Type
All 49 hips were classified based on the athlete’s collegiate sport. A total of 1 (2.6%) cutting athlete, 15 (38.5%) contact athletes, 8 (20.5%) impingement athletes, 6 (15.4%) asymmetric/overhead athletes, and 9 (23.1%) endurance athletes (Table 1) were included. No differences in the prevalence of each type of radiographic FAI (cam, pincer, and mixed) were identified between the 6 sport subgroups. Endurance athletes had lower rates of femoral osteochondroplasty (5 of 11 hips; 45.5%) and labral debridement (0 hips) compared with all the other groups (P < .0001). Contact sport athletes had higher rates of labral debridement (8 of 16 hips; 50.0%; P < .0001).
Patients were evaluated for return to sport at an average of 1.96 ± 0.94 years. Out of all patients with return-to-sport data, 89.7% were able to return to at least collegiate-level competition. All cutting, impingement, and asymmetric/overhead athletes returned to sport, and all but 1 contact sport athlete returned to sporting activity (93.3%). There were no differences in return-to-sport rates except for endurance athletes, who returned at a rate of only 66.6% to collegiate or professional competition (P < .001) (Table 3). There was no difference between sport types in the highest attempted level of sport that patients resumed. A total of 9 (23.1%) athletes were able to return to sport participation and move on to professional athletic competition.
A subgroup analysis of patients who underwent labral debridement versus labral repair found no difference with regard to return-to-sport rate (P = .411), duration after return (P = .265), or highest attempted level of sport resumed (P = .625). Female and male athletes returned to sport at a similar rate (P = .8).
Return-to-Sport by Sport Type for Collegiate Athletes a
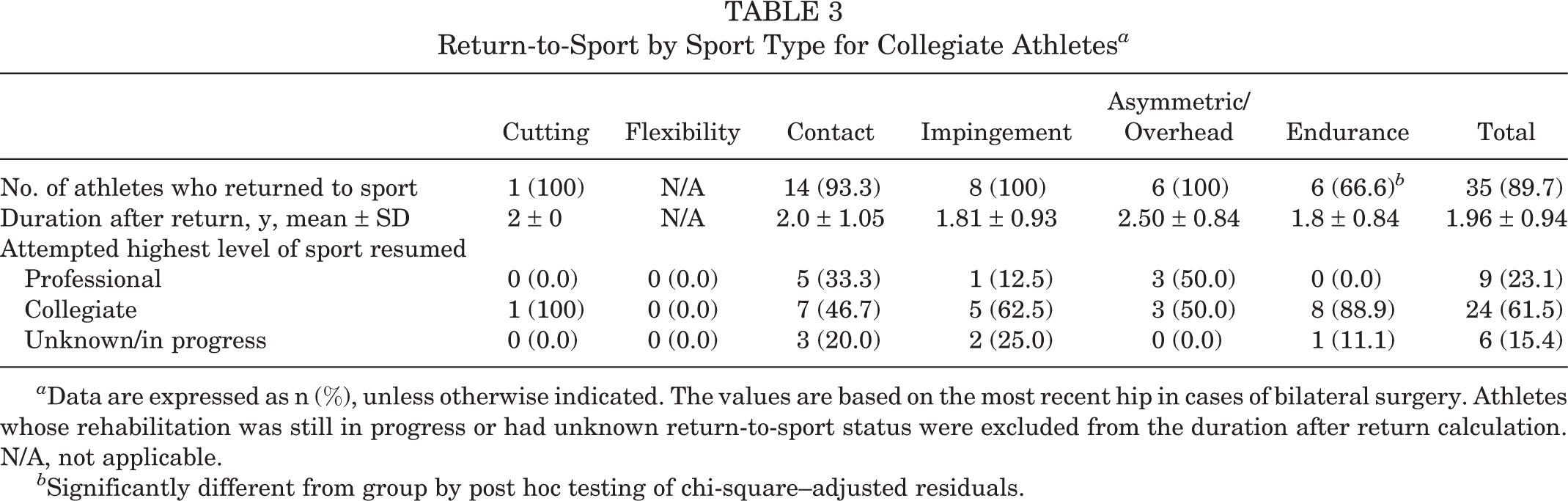
a Data are expressed as n (%), unless otherwise indicated. The values are based on the most recent hip in cases of bilateral surgery. Athletes whose rehabilitation was still in progress or had unknown return-to-sport status were excluded from the duration after return calculation. N/A, not applicable.
b Significantly different from group by post hoc testing of chi-square–adjusted residuals.
Discussion
The primary findings of this present study of collegiate-level athletes undergoing hip arthroscopy for FAIS 11 are that they return to sport at a higher rate and that endurance athletes return to sport at lower rates than other sport-type athletes. Furthermore, contact sport athletes have higher rates of labral debridement versus endurance athletes. However, there were no differences between labral debridement and repair in the return-to-sport rate, duration of return, or highest attempted level of sport resumed.
Previous studies have used this classification system of sport types, established by Nawabi et al, 19 to identify potential differences in the clinical presentation and management of FAIS based on the hip biomechanics. Cruz et al 6 reported that across 25 NCAA sports, impingement athletes had the highest rate of surgical intervention for hip injuries, but this study was not FAI specific. In our cohort of 39 surgically treated NCAA athletes, the majority of athletes (n = 15) participated in contact sports. In addition, Cruz et al 6 found that endurance athletes were the highest proportion of athletes with hip injuries, with time lost being greater than 14 days. We did not examine the time lost from competition in this study, which only included patients with FAIS. Regarding the intraoperative procedures performed, Nawabi et al, 19 in a sports-specific study of high-level athletes, found that ligamentum teres debridement was more commonly performed in flexibility athletes compared with impingement or asymmetric/overhead athletes. We observed that endurance athletes had lower rates of femoral osteochondroplasty (45.5%) and labral debridement (0.0%) compared with all the other groups (P < .0001). In addition, contact athletes had higher rates of labral debridement (50.0%; P < .0001). However, our study was limited by a small number of athletes in each of the subgroups, which reduced the external validity of the subgroup analysis. Finally, Weber et al, 29 in a group of recreational and amateur athletes, found the highest rate of return to sport after hip arthroscopy for FAIS in impingement and endurance athletes, in contrast with our results, where endurance athletes had a significantly lower rate of return to sport compared with all other sport types.
As mentioned previously, 19 high-level athletes were found to have a return-to-sport rate between 83% and 93% after arthroscopic treatment of FAIS. The results of the present study are comparable, except for the return-to-sport rate of endurance athletes, which was significantly lower (66.6%). Endurance sports (track, cross-country, and swimming [other than breaststroke]) 8,19,29 include repetitive hip motion with excessive firing of the hip flexors and application of the biomechanical stress to the anterior hip structures. 8,19 This could explain the lower rate of femoral osteochondroplasty and labral debridement performed in endurance athletes found in our study. Hip structural damage in endurance athletes might begin with overuse injuries to the anterior hip structures, including the muscles, because of repetitive hip flexion. This might be different from the “classic” presentation of FAIS, which primarily manifests with the development of cam lesion and related damage to the acetabular labrum. We observed this type of pathology in contact athletes, who had higher rates of labral debridement compared with all the other groups. Therefore, endurance athletes might face a greater risk of compensatory pathology because of a more chronic mechanism of tear versus a more acute, traumatic injury seen in contact sport athletes, which often results in irreparable labral tears.
Difficulty in the adaptation of a “previously trained” hip joint to the altered biomechanical environment after hip arthroscopy might also affect the anterior hip musculature, which is subject to overuse injuries in endurance sports. This might be an additional challenge during the recovery period of endurance athletes who undergo hip arthroscopy for FAIS. Hip flexor tendinitis has been reported as a common complaint after arthroscopic FAI surgery, and most of the published rehabilitation protocols prohibit active hip flexion for the first 1 or 2 weeks postoperatively. 5,12,17,24,28 In addition, Adib et al 1 have reported the incidence of iliopsoas tendinitis after hip arthroscopy for FAIS to be 24%.
The present study confirms the effectiveness of hip arthroscopy in treating FAIS and successfully returning high-level athletes to the preoperative level of competition. 16,18 Unfortunately, endurance athletes returned to sport at a lower rate, which requires further investigation. Our study highlights the importance of identifying sports that place young athletes at risk for developing FAIS requiring hip arthroscopy. It also stresses the importance of developing the appropriate preventive measures, screening tools, and surgical plans for athletes who tend to respond poorly to surgical intervention, such as endurance sport athletes. Furthermore, with proven data on return-to-sport times and postoperative outcomes, an athlete’s expectations can be better managed, and treatment can be further tailored to the specific athlete and sport.
Limitations
There are several limitations to the present study. First, the population size was relatively small, and cutting sports as well as flexibility sports were underrepresented or not represented at all. As mentioned above, however, our study population is unique by representing a group of collegiate athletes from a single institution. Second, return to sport is a difficult outcome to measure as there are varying levels of participation, and it is difficult to quantify performance. We tried to use specific criteria to define not only the level of competition but also the return to sport. Additionally, some athletes in our study were still in college and had not played at a higher level. Even with a chance to return to sport in college, progressing to the professional level has external factors besides the level of hip function after hip arthroscopy. The majority of the procedures were performed by a single surgeon, although 4 more surgeons contributed to the data of this study, which might complicate the interpretation of the results. Other than the labral procedures (repair versus debridement), we did not examine the effect of additional procedures (such as microfractures), revision hip arthroscopy, or the management of the capsule on the return-to-sport rate. This was because of insufficient documentation of this information, which prevented us from performing further analysis. Similarly, we were unable to gather any details regarding the preoperative duration of symptoms, the nonoperative treatment protocol followed, or any modifications to the postoperative rehabilitation protocol based on the individual needs of each athlete. Finally, limitations in our database prevented us from calculating the incidence of symptomatic FAI in the different sport types.
Conclusion
Collegiate-level athletes undergoing hip arthroscopy for FAIS return to sport at high and predictable rates, with endurance athletes possibly returning to sport at lower rates than all the other sport types. Surgical procedures may also be influenced by sport type, but the rate of return to sport between athletes who underwent labral debridement versus labral repair was similar.
Footnotes
Acknowledgment
The authors acknowledge The Cappo Family Research Fund.
Final revision submitted January 8, 2020; accepted January 29, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.E.W. has received educational support from Arthrex and Smith & Nephew, speaking fees from Arthrex, and hospitality payments from Stryker. M.J.P. has received educational support from Linvatec; speaking fees and consulting fees from Smith & Nephew; royalties from DJO, Linvatec, and Smith & Nephew; and hospitality payments from Siemens Medical Solutions. J.S. has received speaking fees from Arthrex; consulting fees from Arthrex, Medical Device Business Services, and Stryker; and hospitality payments from Radlink. J.E.T. has received educational support from Micromed; speaking fees from Arthrex, Pacira Pharmaceuticals, and Smith & Nephew; royalties from Arthrex; and hospitality payments from Stryker. S.C.G. has received educational support from Arthrex, consulting fees from Zimmer Biomet, and speaking fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Southern California (proposal No. HS-15-00565).