
Abstract
Background:
Return to sports (RTS) and patient-reported outcomes (PROs) for elite athletes with femoral version abnormalities undergoing hip arthroscopy have not been well established.
Purposes:
To (1) report minimum 2-year PROs and RTS rates in elite athletes with femoral retroversion who underwent primary hip arthroscopy and (2) compare clinical results to those of a propensity-matched control group of elite athletes with normal femoral version who underwent primary hip arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were prospectively collected and retrospectively reviewed for elite (professional and collegiate) athletes with femoral version <5°, as measured on magnetic resonance imaging scans, who underwent hip arthroscopy for femoroacetabular impingement syndrome between March 2010 and April 2018. Inclusion criteria were preoperative and minimum 2-year follow-up PROs for the modified Harris Hip Score, Nonarthritic Hip Score, Hip Outcome Score–Sports Specific Subscale (HOS-SSS), and visual analog scale for pain. Exclusion criteria were Tönnis grade >1, hip dysplasia, and previous ipsilateral hip surgery or conditions. Rates of achieving the minimal clinically important difference (MCID), Patient Acceptable Symptom State (PASS), and maximum outcome improvement satisfaction threshold were recorded in addition to RTS. Athletes with retroversion were propensity matched in a 1:2 ratio to elite athletes with normal femoral version (5°-20°) for comparison.
Results:
A total of 33 elite athletes (33 hips) with femoral retroversion who underwent hip arthroscopy met the inclusion criteria, and follow-up was available for 30 hips in 30 athletes (90.9%) at an average of 36.1 ± 25.6 months. Elite athletes with femoral retroversion demonstrated significant improvements in all recorded PROs, achieved the MCID and PASS for the HOS-SSS at high rates (86.7%), and returned to sports at a rate of 83.3%. PROs, rates of achieving MCID and PASS for the HOS-SSS, and RTS rates were similar between the study and propensity-matched control group.
Conclusion:
Elite athletes with femoral retroversion undergoing primary hip arthroscopy demonstrated favorable PROs and high RTS rates at a minimum 2-year follow-up. These results were comparable with those of a propensity-matched control group of elite athletes with normal femoral version.
Hip arthroscopy has been increasingly performed in the athletic population, and it has demonstrated favorable results both in the general population and in athletes. 2,11,22,25,38,61 Several studies have evaluated the effect of anatomic variations on outcomes in patients undergoing hip arthroscopy in both the athlete and the nonathlete populations. 4,8,13,34 Femoral version has been an area of interest in the literature, and there is considerable variability of femoral version among the population. A recent study by Kunze et al 37 reported that 39.6% of patients in their cohort had a femoral torsion abnormality. Similarly, Lerch et al 43 established that 52% of patients with symptomatic hips due to femoroacetabular impingement syndrome (FAIS) or dysplasia had femoral version abnormalities.
There has been considerable literature evaluating the effect of femoral retroversion on outcomes after hip arthroscopy in the general population that has produced conflicting results. Originally, Fabricant et al 24 reported that patients with femoral retroversion undergoing hip arthroscopy experienced less improvement compared with patients with normal femoral version. Conversely, recent data have suggested that patients with femoral retroversion achieve similarly favorable outcomes compared with patients with normal version undergoing hip arthroscopy. 37,40 Despite the considerable literature evaluating the effect of femoral version in the general population, scarce literature exists regarding the effect of femoral retroversion in athletes.
The purposes of the current study were to (1) report minimum 2-year patient-reported outcomes (PROs) and return-to-sports (RTS) rates in elite athletes with femoral retroversion undergoing primary hip arthroscopy and (2) compare clinical results with those of a propensity-matched control group of elite athletes with normal femoral version who underwent primary hip arthroscopy. It was hypothesized that (1) athletes with retroversion undergoing hip arthroscopy would demonstrate significant improvement in all PROs and RTS rates at a minimum 2-year follow-up and (2) clinical results in this group would be similar to those of a propensity-matched control group of athletes with normal femoral version undergoing hip arthroscopy.
Methods
Participation in the American Hip Institute Hip Preservation Registry
All patients included in this study participated in the American Hip Institute Hip Preservation Registry and provided informed consent. Although this present study represents a unique analysis, data on some patients in this study may have been reported in other studies. This study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki and with relevant regulations of the US Health Insurance Portability and Accountability Act. Institutional review board approval was received for the study protocol.
Patient Selection
Data were prospectively collected and retrospectively reviewed for all patients who underwent hip arthroscopy by the senior surgeon (B.G.D.) between March 2010 and April 2018. Patients were considered eligible if they were evaluated with femoral version <5° calculated on preoperative magnetic resonance imaging (MRI) scans, underwent hip arthroscopy for FAIS during the study period, and were elite (collegiate or professional) athletes within 1 year before their first surgery. 29 Patients were included in the present analysis if they had preoperative and minimum 2-year follow-up PROs for the modified Harris Hip Score (mHHS), 3 Nonarthritic Hip Score (NAHS), 16 Hip Outcome Score–Sports Specific Subscale (HOS-SSS), 52 and visual analog scale (VAS) for pain 15 and if they had completed an RTS survey. Follow-up was considered complete if patients had all PRO measures and RTS data or if secondary ipsilateral hip surgery, such as revision arthroscopy or conversion to total hip arthroplasty, was recorded.
Patients were excluded from the analysis if they had a Tönnis grade of osteoarthritis >1, hip dysplasia (lateral center-edge angle [LCEA], <18°), 48 prior ipsilateral hip surgery, or prior hip conditions (ie, avascular necrosis, ankylosing spondylitis, Ehlers-Danlos syndrome, Legg-Calvè-Perthes disease, pigmented villonodular synovitis, or slipped capital femoral epiphysis).
Analysis was performed for the included athletes (retroverted group) against a propensity-matched group of elite athletes with normal femoral version (5°-20°) who had undergone primary hip arthroscopy (control group). 31
Preoperative Evaluation and Surgical Indications
A detailed patient history, physical examination, and radiographic analysis were collectively utilized preoperatively by the senior author (B.G.D.) to evaluate surgical candidates. Descriptive variables were collected, including age at surgery, body mass index (BMI), sex, operative side, and follow-up time. Gait, range of motion, strength, points of tenderness, and signs of FAIS or mechanical symptoms (snapping, catching, locking) were noted during physical examination. Radiographs were obtained and evaluated for signs of cam-type and pincer-type morphologies, acetabular dysplasia, and osteoarthritis in all patients using the anteroposterior pelvis, Dunn 45°, and false-profile views. 17 Radiographic measurements included LCEA, 54 anterior center-edge angle (ACEA), 42 alpha angle, 7 Tönnis angle of acetabular inclination, 33 and femoral head-neck offset. 27 Osteoarthritis was graded according to the Tönnis classification. 19 Cam morphology was defined as an alpha angle >55° 18,50 or femoral head-neck offset <0.8 cm. 27 Evaluations of these images were performed using a picture archiving and communication system (General Electric Healthcare). Radiographic measurements have demonstrated good interobserver reliability in previously published studies. 20,44
MRI or magnetic resonance arthrography was obtained on all patients before surgical indication and was used to identify intra-articular pathology, such as labral tears or chondral damage. Additionally, femoral version measurements were calculated using the oblique method as described by Sutter et al. 59,60 Before being recommended for surgery by the senior author, all patients had pain that interfered with activities of daily living for ≥3 months and did not improve with activity modification, nonsteroidal anti-inflammatory drugs, physical therapy, intra-articular ultrasound-guided injections, and rest. Careful surgical indications and preoperative planning were completed in patients with femoral retroversion, as described by Lall et al. 40
Surgical Technique
All arthroscopic surgeries were performed by the senior author. Under general anesthesia, patients were placed in the modified supine position, and traction was applied to a hip. 41 After the anterolateral and midanterior portals were created, 49 a systematic diagnostic arthroscopy was performed to assess the labrum, intra-articular cartilage, and ligamentum teres (LT). Labral damage was reported using the Seldes classification, 58 and articular cartilage damage and cartilage lesions were reported using the acetabular labrum articular disruption and Outerbridge classifications, respectively. 30 LT damage was graded using the Domb and Villar classifications. 45
Under fluoroscopic guidance, acetabuloplasty and femoral osteoplasty were performed to address pincer-type and cam-type morphologies, respectively, when needed. 39 When possible, labral tears were repaired using either a base refixation technique or a controlled-tension anatomic loop stitch. 21 Irreparable labral tears were treated via labral reconstruction or selective debridement. 21,47 At the end of each procedure, repair or plication of the interportal capsulotomy was performed unless excessive stiffness, adhesive capsulitis, or insufficient capsular tissue was noted. 23,55
Rehabilitation Protocol
After surgery, all patients used crutches with a 20-pound (9.1 kilograms) weightbearing restriction and wore a hip brace (DonJoy VersaRom, Enovis, Lewisville, TX) locked at 90° of flexion and 0° of extension for 2 weeks. On postoperative day 1, patients began daily use of a continuous passive motion machine or stationary bicycle. All patients followed our institution’s rehabilitation protocol, with a predetermined goal of RTS 6 months after surgery. The rehabilitation protocol was tailored to the specific procedures performed such that when labral reconstruction or microfracture was performed, the protocol was modified so that the patient was restricted from bearing >20 pounds (9.1 kilograms) for 6 to 8 weeks.
RTS and Surgical Outcome Tools
All athletes completed a questionnaire reporting their level of participation in sports within 1 year of their surgical date and identified their sport type. RTS was defined as a patient’s return to competitive participation in his or her sport at the same level as or higher than that of before surgery. 34
To establish baseline scores, patients completed preoperative questionnaires within a month of their surgery date, which included the mHHS, NAHS, HOS-SSS, VAS for pain (scale, 0-10), International Hip Outcome Tool–12 (iHOT-12), 51 and VAS for satisfaction (scale, 0-10). Baseline scores for iHOT-12 were not reported, as this PRO measure was only added to our questionnaire within the study period. Postoperatively, patients completed questionnaires at 3 months, 1 year, and annually thereafter. Secondary ipsilateral hip surgeries were also documented for all patients. Outcomes were recorded at clinical visits, through encrypted email, or telephone interviews.
Preoperative PRO scores were utilized to calculate the minimal clinically important difference (MCID) for the mHHS, NAHS, HOS-SSS, and VAS for pain (scale, 0-10) using a distribution-based calculation, as reported by Norman et al. 53 The rates of patients with retroversion and control group patients achieving the MCID for the mHHS (6.7 points and 8.1 points, respectively), NAHS (8.8 points and 9.1 points, respectively), VAS (1.2 points), and HOS-SSS (11.3 points and 11.9 points, respectively) were recorded. Additionally, threshold values from previously published literature on the number of patients who met the Patient Acceptable Symptom State (PASS) for the mHHS (74 points), NAHS (85.6 points), VAS (2.16 points), and HOS-SSS (75 points) were documented. 10,12,57 The maximum outcome improvement score was also calculated for each patient using the following equation 9 :

In addition, the rates of patients who achieved the maximum outcome improvement satisfaction threshold (MOIST) for mHHS (54.8%), NAHS (52.5%), and VAS (55.5%) were recorded as described by Maldonado et al. 46
Statistical Analysis
Analyses included comparisons between the retroverted and matched control groups and within-group comparisons between preoperative and postoperative values. Descriptive statistics for continuous variables were reported as means with standard deviations and ranges. Categorical variables were reported as totals and percentages. Chi-square and Fisher exact tests were used to compare categorical data. Continuous variables were assessed for normality using the Shapiro-Wilk test and assessed for equal variance using the F test. A 2-tailed t test was used to assess normally distributed data sets with equal variance, and Wilcoxon signed rank test, Mann-Whitney U test, or Welch test was used to analyze nonparametric data. Statistical analysis was performed using Microsoft Excel (Microsoft Corp) with the Real Statistics Add-In and RStudio (Version 1.3.959; RStudio). The threshold for statistical significance was set at P < .05.
Propensity Score Matching
Propensity score matching was utilized to minimize the potential effect of confounding factors. Matching was completed using RStudio (Version 1.3.959). Greedy matching without replacement was used to match athletes with retroversion to control group athletes in a 1:2 ratio. For this process of matching, hips in the control group could only be matched to a hip in the retroverted group once. Previous studies have shown that the optimal method for group comparison is greedy matching without replacement. 1,5,6
The groups were matched according to age at the time of surgery, sex, BMI, Tönnis grade, LCEA, follow-up time, sport type, and competition level. An a priori power analysis was calculated to find the number of patients necessary in each group to detect 80% power with a 1:2 matching ratio. 34 Based on an expected mean difference in the mHHS of 8 points, the power analysis determined that 19 athletes with retroversion and 39 control group athletes would be required.
Results
Patient Characteristics
A total of 33 elite athletes with femoral retroversion who underwent hip arthroscopy met the inclusion criteria. Of those athletes, 30 (90.9%) had a minimum 2-year follow-up and information regarding RTS. All 30 athletes with retroversion were successfully propensity matched to 60 control group athletes who underwent primary hip arthroscopy and had a minimum 2-year follow-up. The overall patient selection process is depicted in Figure 1.

Flowchart summarizing the patient selection process.
Table 1 presents a full summary of patient characteristics for the retroverted and control groups. Overall, there were 22 (73.3%) collegiate and 8 (26.7%) professional athletes in the retroverted group and 44 (73.3%) collegiate and 16 (26.7%) professional athletes in the control group. The most common sports reported by the retroverted and control group athletes were football (23%) and track/running (15%), respectively (Figure 2). Other than femoral version (retroverted group, 1.3° ± 2.3° vs control group, 10.1° ± 4.2°; P < .001), there were no other significant differences in characteristics found between the 2 study groups.
Patient Characteristics a
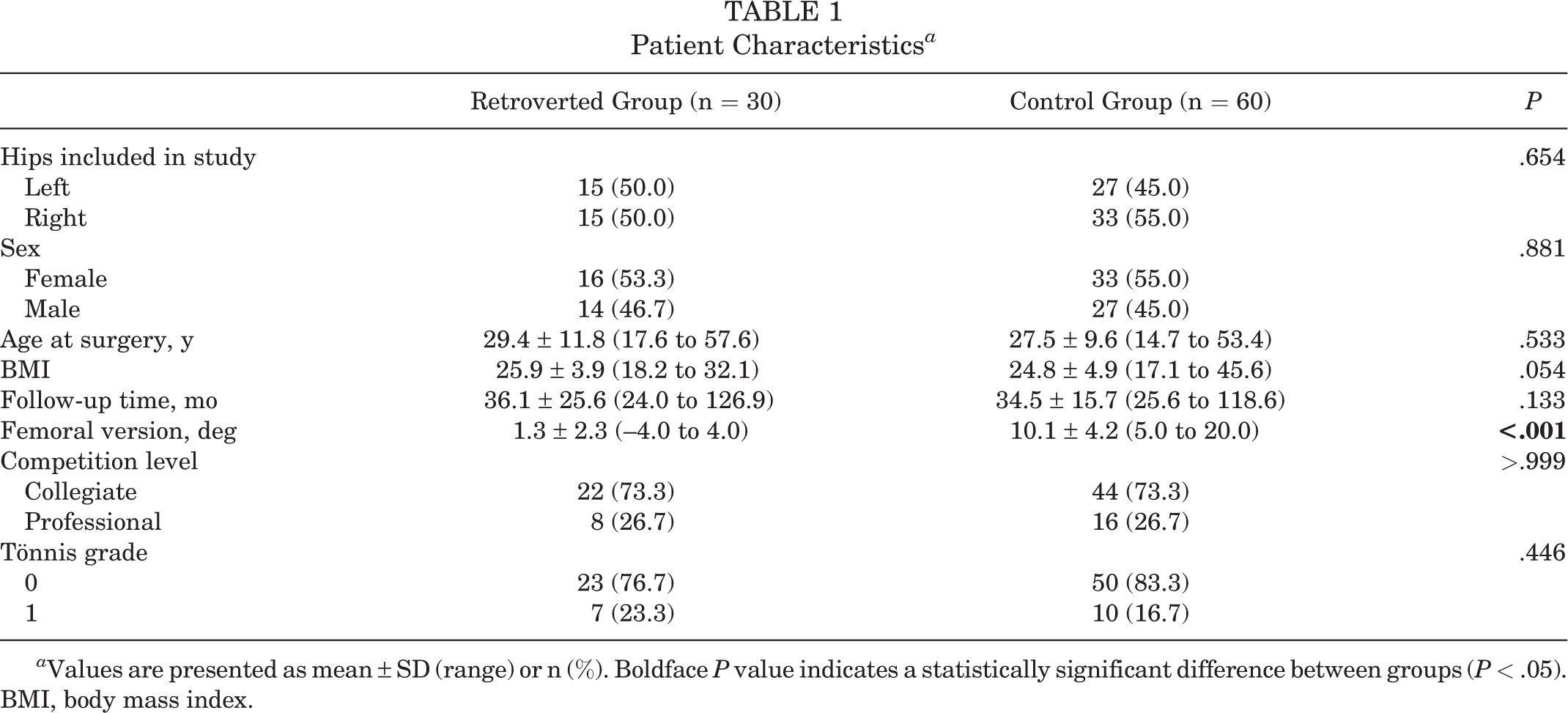
a Values are presented as mean ± SD (range) or n (%). Boldface P value indicates a statistically significant difference between groups (P < .05). BMI, body mass index.

Summary of the preoperative sports played by elite athletes with (A) femoral retroversion (n = 30) and (B) normal femoral version (n = 60).
Intraoperative Findings and Arthroscopic Procedures
Intraoperative data demonstrated similar findings for labral tear type, acetabular and femoral head cartilage damage, and LT injuries between the retroverted and control groups (Table 2) and no significant differences in surgical procedures performed (Table 3).
Intraoperative Findings a

a Values are presented as n (%). ALAD, acetabular labrum articular disruption; LT, ligamentum teres.
Surgical Procedures a
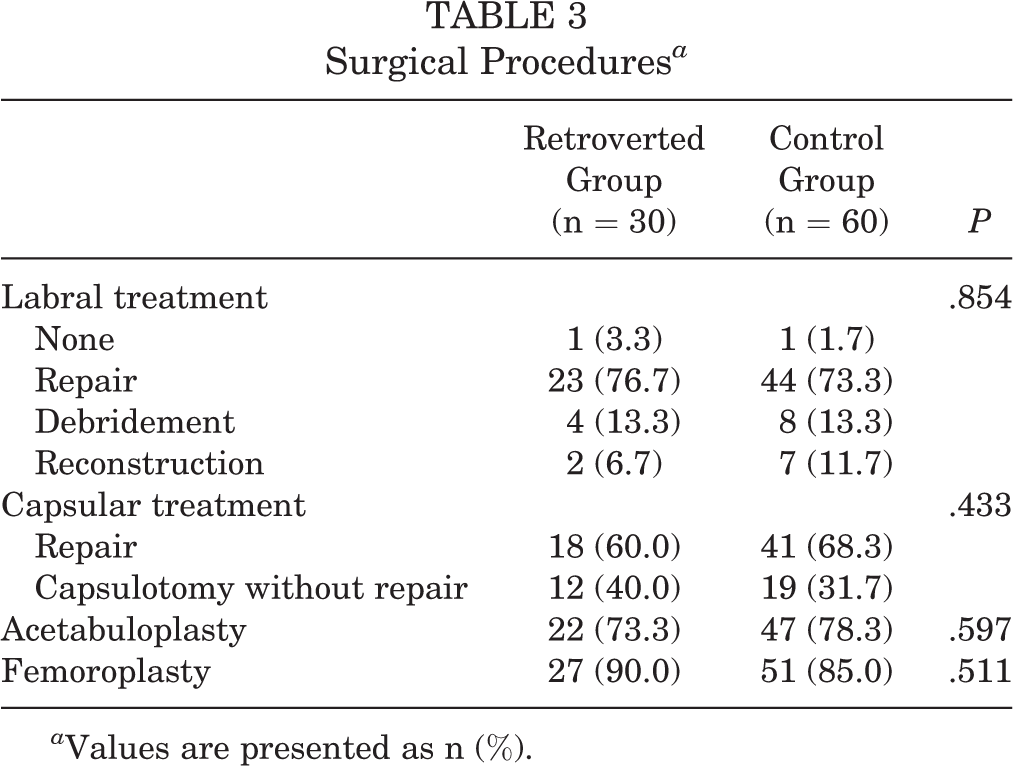
a Values are presented as n (%).
Radiographic Findings
There were no significant differences between groups in any pre- or postoperative radiographic measurement. There were significant pre- to postoperative changes for alpha angle and femoral offset within both the retroverted and control groups (P < .001). Additionally, control group athletes demonstrated significant pre- to postoperative changes in LCEA (P < .001) and ACEA (P = .022) measurements. Radiographic findings are presented in Table 4.
Radiographic Findings a

a Values are presented as mean ± SD (range). Boldface P values indicate a statistically significant difference between preoperative and postoperative (P < .05). ACEA, anterior center-edge angle; LCEA, lateral center-edge angle.
RTS and PROs
All athletes included in the present study experienced significant improvements in mHHS, NAHS, HOS-SSS, and VAS from preoperatively to latest postoperative follow-up (P < .001). Preoperative and postoperative scores for the mHHS, NAHS, HOS-SSS, and VAS were found to be comparable between the retroverted and control groups (P > .05). Additionally, both groups demonstrated similar postoperative scores for the iHOT-12 at a minimum 2-year follow-up (P > .05). The mean satisfaction scores for the retroverted and control groups were 9.0 and 8.0, respectively (P = .072). Further, both groups achieved MCID, PASS, and MOIST thresholds for all PROs at similar rates (P > .05). A full summary of PROs is presented in Tables 5 and 6.
Patient-Reported Outcomes a
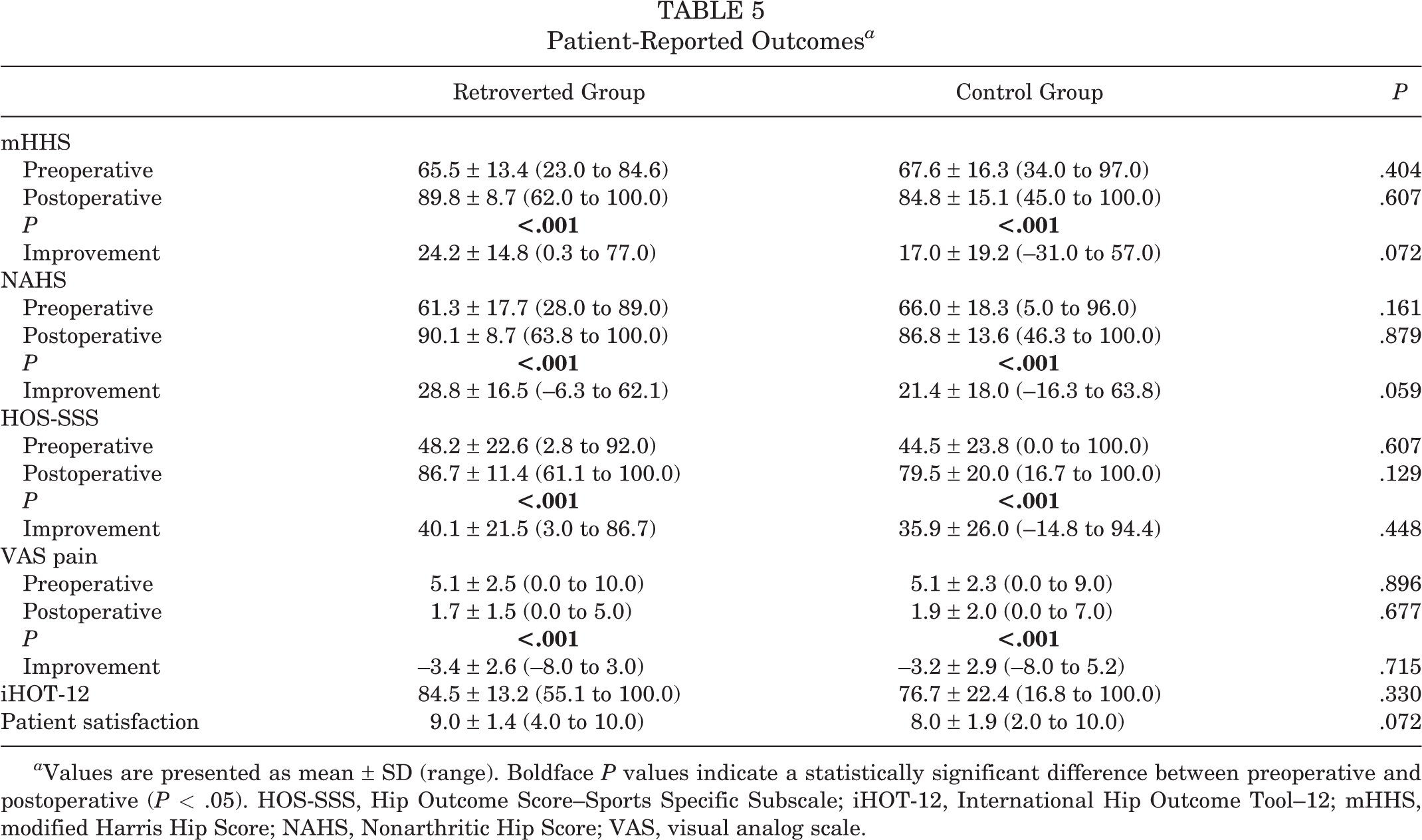
a Values are presented as mean ± SD (range). Boldface P values indicate a statistically significant difference between preoperative and postoperative (P < .05). HOS-SSS, Hip Outcome Score–Sports Specific Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale.
Rates of MCID, PASS, and MOIST a

a Values are presented as n (%). HOS-SSS, Hip Outcome Score–Sports Specific Subscale; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; MOIST, maximum outcome improvement score threshold; NAHS, Nonarthritic Hip Score; PASS, Patient Acceptable Symptom State; VAS, visual analog scale.
Among those that attempted to RTS were 20 (83.3%) athletes with retroversion and 41 (85.4%) control group athletes (P = .817). Athletes who underwent a lifestyle transition (graduation, aging, loss of interest, etc) and did not attempt to RTS for reasons unrelated to the hip were not included in the RTS percentage. Both groups demonstrated similar RTS rates, and characteristics of those who returned to sports and those who did not were comparable between the study and control groups (P > .05). Tables 7 to 9 present a summary of RTS outcomes for both groups.
Return to Sports Outcomes a

a Values are presented as n (%) . The return-to-sport percentage does not include patients who underwent a lifestyle transition and thus did not attempt to return to sport.
Characteristics for Patients Who Did Return to Sports a
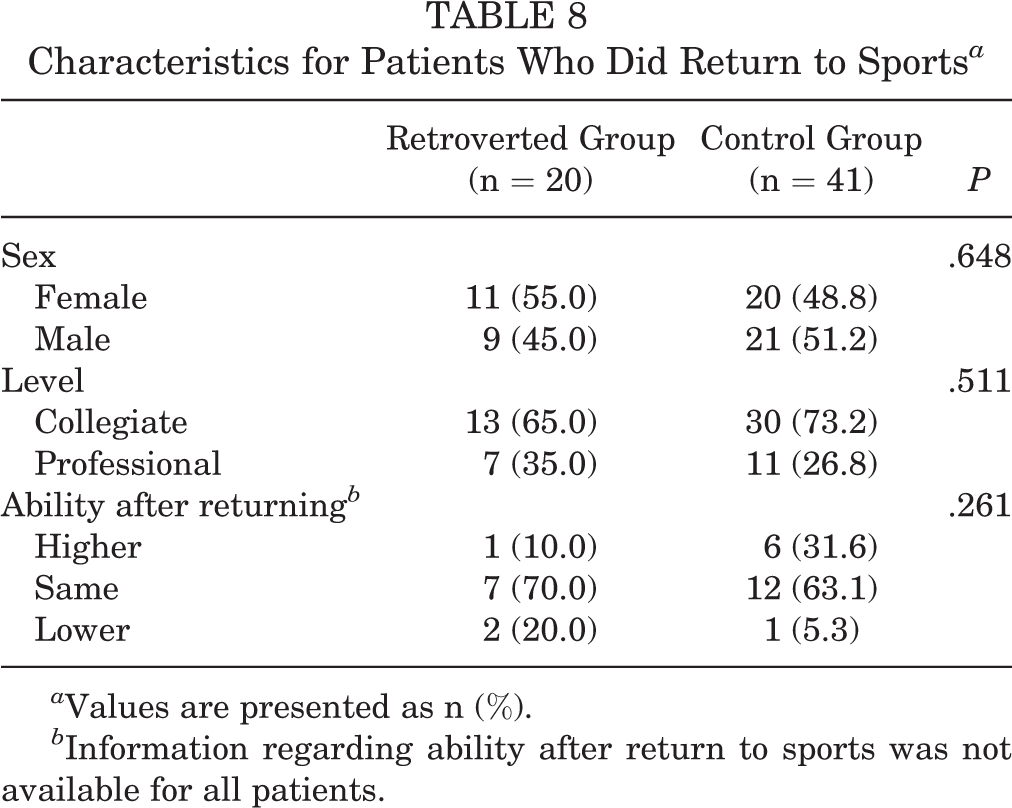
a Values are presented as n (%).
b Information regarding ability after return to sports was not available for all patients.
Characteristics of Patients Who Did Not Return to Sports Because of Hip Symptoms a

a Values are presented as n (%).
Secondary Surgeries
Regarding revision arthroscopies, none of the athletes with retroversion underwent a revision, while 3 (5.0%) control group athletes underwent a secondary arthroscopy. One patient underwent revision labral reconstruction because of acute injury causing labral tear. One patient underwent revision labral debridement because of FAI from recurrent cam-type morphology. One patient underwent revision labral repair because of labral tear. There were similar revision rates and time to revision found between the groups (Table 10). Additionally, by the latest follow-up, none of the included athletes had undergone conversion to total hip arthroplasty.
Secondary Surgeries a
a Values are presented as mean ± SD (range) or n (%). NA, not applicable.
Discussion
The main finding of this paper was that elite athletes with femoral retroversion undergoing primary hip arthroscopy demonstrated significant improvements in all recorded PROs, high RTS rates, and a low rate of revision surgery. From a clinical standpoint, they achieved MCID and PASS for HOS-SSS at high rates. Further, when athletes with femoral retroversion were compared with a propensity-matched control group of athletes with normal version, they demonstrated similar PROs, RTS, and secondary surgery rates.
In the present study, the presence of femoral retroversion in elite athletes did not adversely affect outcomes compared with a propensity-matched control group of elite athletes with normal version. This represents one of the few investigations reporting the effect of femoral version in the elite athlete population after primary hip arthroscopy.
Prior literature on the influence of femoral retroversion on outcomes in the general population is inconsistent. Fabricant et al 24 reported the outcomes after hip arthroscopy in a cohort of 243 patients, 37 of whom had femoral retroversion (defined as <5°). They found that patients with decreased femoral version had less improvement in mHHS and iHOT-33 compared with patients with normal femoral version (5°-20°). Similarly, Kelly et al 36 evaluated the effect of femoral version on pre- versus postoperative internal rotation in patients undergoing hip arthroscopy for FAIS. They found that all patients had improvement in internal rotation postoperatively regardless of femoral version but that the improvement was significantly smaller in patients with femoral retroversion.
The negative effect of femoral version morphologies on outcomes after hip arthroscopy has been called into question in more recent literature. Kunze et al 37 performed a computed tomography–based analysis quantifying femoral torsion in patients with FAIS, and they evaluated the relationship between femoral torsion and the rates of achieving clinically meaningful outcome improvement after hip arthroscopy. In the study, the authors did not establish any differences in postoperative outcome scores or in rates for achieving clinically significant outcome improvement based on femoral torsion. These findings were mirrored by Lall et al, 40 who compared minimum 5-year postoperative outcomes between 59 patients with femoral retroversion and 59 control patients with normal femoral version. Their results showed that patients with femoral retroversion demonstrated significantly improved outcomes at midterm follow-up, which were similar to those of a control group of patients with normal femoral version.
Prior literature has established that femoral retroversion leads to decreased femoral internal rotation before impingement of the femoral neck on the acetabular rim compared with normal version. 28,32 Femoroplasty can help to reestablish anatomic head-neck offset and prevent impingement, especially in the setting of femoral retroversion. 36 In the present study, femoral osteoplasty was performed in 90% of the study group, and the alpha angle improved from 62.4 preoperatively to 43.7 postoperatively (P < .001). It is likely that an adequate femoroplasty and restoration of femoral head-neck offset in the study group were responsible for the favorable outcomes in this population.
Strengths of the Study
There are several strengths in the present study, further reinforcing the findings reported. Propensity score matching was utilized in this analysis in order to minimize the effects of potential confounding factors such as sex, age, Tönnis grade, BMI, LCEA, follow-up time, sport-type, and competition level. Based on an a priori power analysis, the sample sizes of the study cohorts were adequately representative to detect statistical differences, diminishing the risk of type 2 error. Further, the use of multiple validated functional hip outcome scores designed to assess outcomes in active patients with nonarthritic hips limits a potential ceiling effect and increases the generalizability of the results. Finally, multiple clinical psychometric tools, including MCID, PASS, and MOIST, were utilized in order to assess clinical importance. 26
Limitations
Limitations of the present study must also be acknowledged. First, as this was a nonrandomized study, additional confounding variables may have influenced the results. Although data were prospectively collected, the retrospective nature of this analysis may have introduced bias. Additionally, analysis was based on patients from a single, experienced, high-volume hip preservation surgeon, which may limit the generalizability of the results or lead to nonreproducible findings at other centers. Surgical technique has evolved and improved substantially over the study period, which may have introduced potential bias to the results. As a result, some patients in the present study cohorts who underwent capsulotomy without repair or selective labral debridement would currently be treated with capsular repair/plication and an alternative labral restoration technique such as labral repair, reconstruction, or augmentation. 14,21,35,55,56 The inclusion of collegiate and professional athletes may have introduced heterogeneity in terms of competition and ability level, limiting the generalizability of the results. Next, there were no data regarding snapping of the iliopsoas tendon and subsequent iliopsoas fractional lengthening, which may affect outcomes. This study included patients with borderline dysplasia and acetabular overcoverage (LCEA >40°); however, new literature from Jimenez et al 34 and Maldonado et al 45 indicates that these populations are able to achieve comparable outcomes to patients without borderline dysplasia or acetabular overcoverage. 13 Additionally, outcomes may be influenced by patients reporting favorable outcomes despite persistent hip symptoms while attempting to RTS. Last, the present study was based on a minimum 2-year follow-up, but longer follow-up is necessary to determine the durability of the results.
Conclusion
Elite athletes with femoral retroversion undergoing primary hip arthroscopy may expect favorable PROs and high RTS rates at a minimum 2-year follow-up. These results were comparable with those of a propensity-matched control group of elite athletes with normal femoral version.
Footnotes
Final revision submitted February 10, 2022; accepted March 22, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.E.J. has received education payments from Medwest. A.C.L. has received grant support from Arthrex and Stryker, education payments from Arthrex and Smith & Nephew, consulting fees from Graymont Professional, and nonconsulting fees from Arthrex. B.G.D. has received education payments from Medwest; consulting fees from Arthrex, Medacta, and Stryker; speaking fees from Arthrex and Stryker; and royalties from Arthrex, DJO, and Medacta. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Advocate Health Care (study No. 5276).