
Abstract
Background:
Low-load blood flow restriction (BFR) training has attracted attention as a potentially effective method of perioperative clinical rehabilitation for patients undergoing orthopaedic procedures.
Purpose:
To (1) compare the effectiveness of low-load BFR training in conjunction with a standard rehabilitation protocol, pre- and postoperatively, and non-BFR interventions in patients undergoing anterior cruciate ligament reconstruction (ACLR) and (2) evaluate protocols for implementing BFR perioperatively for patients undergoing ACLR.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
A systematic review of the 3 medical literature databases was conducted to identify all level 1 and 2 clinical trials published since 1990 on BFR in patients undergoing ACLR. Patient demographics from included studies were pooled. Outcome data were documented, including muscle strength and size, and perceived pain and exertion. A descriptive analysis of outcomes from BFR and non-BFR interventions was performed.
Results:
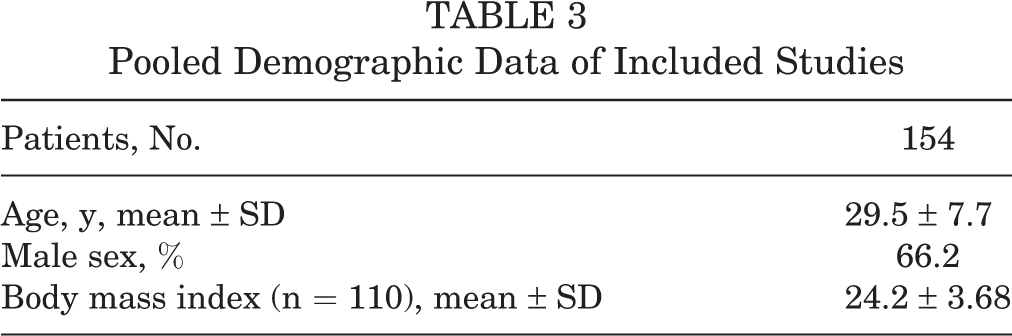
A total of 6 studies (154 patients; 66.2% male; mean ± SD age, 24.2 ± 3.68 years) were included. Of these, 2 studies examined low-load BFR as a preoperative intervention, 1 of which observed a significant increase in muscle isometric endurance (P = .014), surface electromyography of the vastus medialis (P < .001), and muscle blood flow to the vastus lateralis at final follow-up (P < .001) as compared with patients undergoing sham BFR. Four studies investigated low-load BFR as a postoperative intervention, and they observed significant benefits in muscle hypertrophy, as measured by cross-sectional area; strength, as measured by extensor torque; and subjective outcomes, as measured by subjective knee pain during session, over traditional low-load resistance training (all P < .05). BFR occlusion periods ranged from 3 to 5 minutes, with rest periods ranging from 45 seconds to 3 minutes.
Conclusion:
This systematic review found evidence on the topic of BFR rehabilitation after ACLR to be sparse and heterogeneous likely because of the relatively recent onset of its popularity. While a few authors have demonstrated the potential strength and hypertrophy benefits of perioperative BFR, future investigations with standardized outcomes, long-term follow-up, and more robust sample sizes are required to draw more definitive conclusions.
Keywords
High-intensity resistance training can induce limb muscle hypertrophy and strength gains, which are desired outcomes in physical rehabilitation after surgery. 2 However, patients undergoing anterior cruciate ligament reconstruction (ACLR) cannot tolerate high-intensity training, defined as 60% to 85% of the 1 repetition maximum weight, in the immediate perioperative period.
Blood flow restriction (BFR) by the application of a pneumatic cuff to the lower extremity during low-intensity resistance training (approximately 20% of 1 repetition maximum weight) has been shown to significantly increase thigh muscle cross-sectional area, as well as carotid arterial and venous compliance, in healthy volunteers. 1,61 The anaerobic conditions of BFR induce an angiogenic stimulus through upregulation of vascular endothelial growth factor. 19,38 In addition, the hypoxic stimuli may stimulate the mobilization and recruitment of endothelial progenitor stem cells, improving the regenerative potential in healthy volunteers. 54 The muscle hypertrophy induced during low-intensity resistance training with BFR is an attractive method of postsurgical rehabilitation in ACLR in that it avoids placing high loads on the graft in the immediate postoperative period and provides rehabilitation options for the elderly and other patients with severe endurance or strength deficiency.
To date, there is a paucity of clinical data on BFR training and even fewer randomized controlled trials. The duration of the therapy, the intensity of the BFR (pressure), and that required to produce hypertrophic effects remain unclear. 31,47,60,73 Furthermore, given the recent increased awareness of this therapy, there is a myriad of new research with heterogeneous indications and results. For the aforementioned reasons, the purposes of the present systematic review are to (1) compare the effectiveness of low-load BFR (LL-BFR) training in conjunction with a rehabilitation protocol, pre- and postoperatively, versus non-BFR interventions in patients undergoing ACLR and (2) evaluate protocols for implementing BFR perioperatively for patients undergoing ACLR.
Methods
Search Strategy
This review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A literature search was undertaken to identify studies evaluating BFR training as a prehabilitation or rehabilitation protocol after ACLR for the period between January 1, 1990, and May 14, 2019, within the MEDLINE, CINAHL, and EMBASE databases. The following search terms were used: ((((((((vascular occlusion) OR blood flow restriction) OR blood flow occlusion) OR kaatsu)) OR partial occlusion))) AND (((((((anterior cruciate ligament reconstruction) OR ACLR) OR anterior cruciate ligament surgery) OR ACL surgery) OR anterior cruciate ligament)).
Inclusion and Exclusion Criteria
Eligible studies were included after application of the following inclusion criteria: studies involving BFR as a prehabilitation or rehabilitation intervention in patients undergoing ACLR, English language in a scientific peer-reviewed journal, and level 1 or 2 evidence or qualification as a randomized controlled trial. Ongoing level 1 clinical trials without publication of complete data were not included.
Study Selection and Data Extraction
Studies eligible for inclusion were screened independently by 2 reviewers (Y.L. and C.K.). Duplicates and those not meeting the inclusion criteria were excluded. For the included studies, data extraction was inclusive of the following variables: (1) study design and population characteristics; (2) rehabilitation protocol, including device used, occlusion characteristics, exercise performed, and duration of BFR training; and (3) outcome measures, including muscle strength and size, perceived exertion and pain, and physical function. Data extraction was then performed with a custom spreadsheet. As almost all included studies evaluated different outcome measures, precluding a meta-analysis, we elected to proceed with a descriptive analysis of outcomes. Pooled demographic variables were calculated assuming independence of samples.
Study Quality and Reporting
Quality of the included studies was assessed with the Jadad score, 31 which is a criterion for the evaluation and appraisal of randomized clinical trials. It is based on a composite score calculated from the following 3 metrics, with 1 point for an answer of yes and 0 points for an answer of no: (1) Is the study self-described as randomized? (2) Is the study self-described as double-blinded? (3) Does the study provide an adequate description of dropouts and withdrawals? After this initial assessment, secondary grading was performed on the basis of the following: an additional point was given if, for question 1, the method for randomization was described and was appropriate or, for question 2, the method of double-blinding was described and was appropriate. Conversely, a point was deducted if the methods for questions 1 and 2 were described and were inappropriate. Final scores for studies assessed may range from 0 to 5.
Additionally, an assessment of each study was performed with the modified Cochrane Risk of Bias tool, 24 a method created and validated by the Cochrane Collaboration to determine the risk of bias in randomized trials. The tool focuses on the various domains of trial design, conduct, and reporting and proposes a judgment regarding the relevant risk of bias within each domain, graded as “high risk,” “low risk,” or “some concern.” The domains include random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting. If not enough information is provided in the methodology to make a judgment, the domain is listed as “not reported.”
Statistical Analysis
Age and body mass index of the study participants were extracted from the included studies and pooled with weighted means. All statistical analysis was performed with RStudio software (v 1.0.143; R Foundation for Statistical Computing).
Results
The database search yielded 25 articles. After initial title and abstract screening, 15 articles regarded the topic in question and were assessed for eligibility. From this selection, 6 studies were of level 1 evidence per the PRISMA statement and were included in the analysis, as illustrated by Figure 1. An overview of study characteristics is provided in Table 1. The Jadad scores for the included studies ranged from 2 to 4, indicating average to rigorous study quality based on randomization and blinding protocols. Using Cochrane risk assessment we found 1 study 26 was at high risk of bias in 1 category and 4 were at high risk in 2 categories (Table 2).

Flowchart of study selection process.
Overview of Study Characteristics a
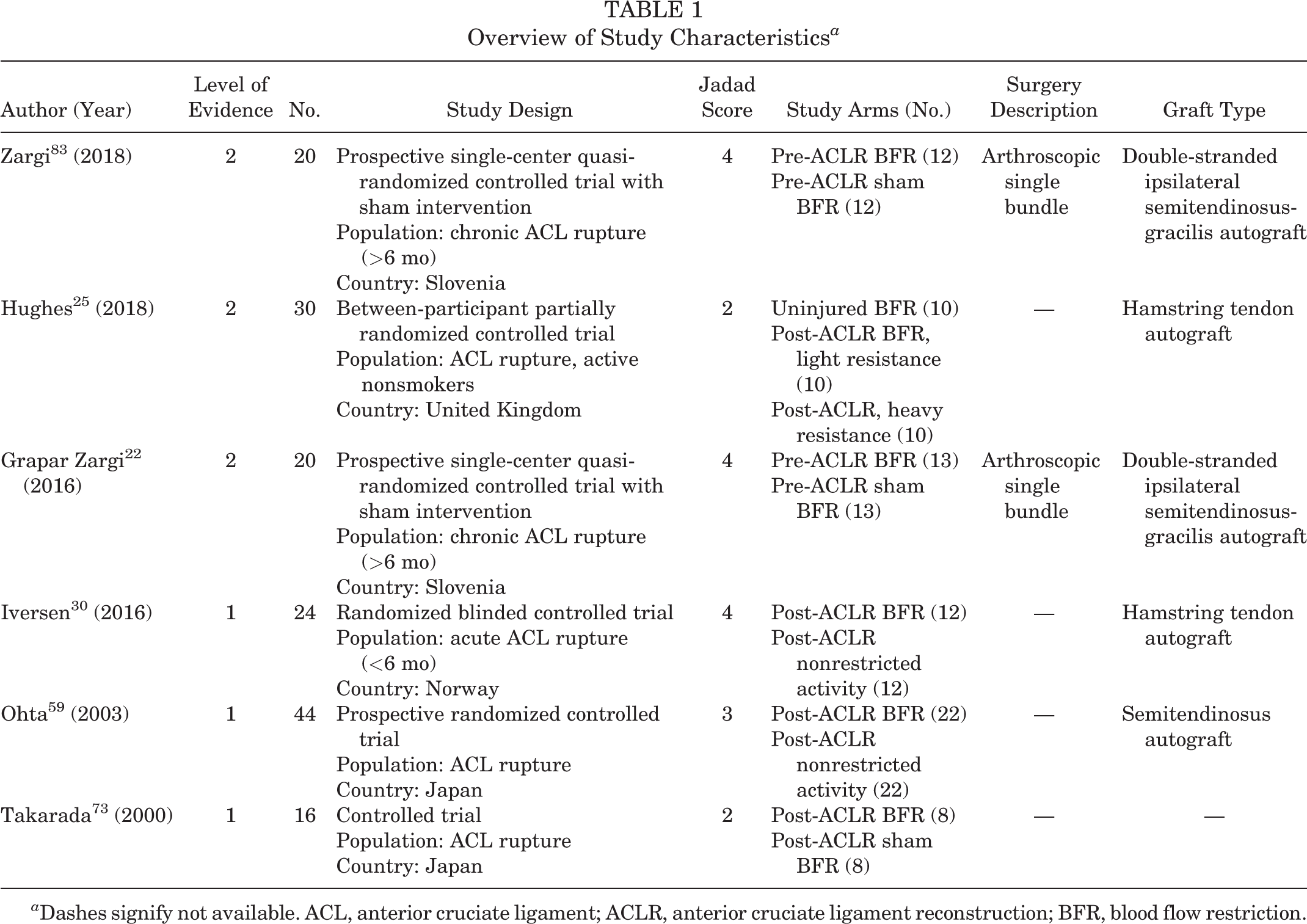
a Dashes signify not available. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BFR, blood flow restriction.
Overview of Study Characteristics

Study Populations
Of the 6 studies, 2 each were from Slovenia and Japan 23,59,73,83 and 1 each from Norway and the United Kingdom. 26,31 Two studied preoperative rehabilitation before ACLR after a chronic injury, 23,83 while 4 studied 26,31,59,73 postoperative rehabilitation. Sample sizes ranged from 16 to 44. All studies were randomized into 2 study arms with 1 exception, which was stratified into 3 study arms. 26 Control arms in the trials were sham BFR in 3 studies, 23,73,83 nonrestricted activities in 2 studies, 31,59 and, for the study with 3 arms, 26 BFR on healthy knees and nonrestricted activity. A total of 154 patients were enrolled in the 6 studies. Pooled demographics of the included studies are as follows: the mean ± SD age was 29.5 ± 7.7 years; body mass index was 24.2 ± 3.68 kg/m2; and 66.2% of the patients were male (Table 3).
Pooled Demographic Data of Included Studies
BFR Protocol
Detailed BFR protocols are provided in Table 4. BFR was used in conjunction with specifically outlined LL resistance training and/or low- to moderate-intensity postoperative rehabilitation. Training load ranged from body weight to 30% of 1 repetition maximum. Constant occlusion pressure was applied in 4 studies, 23,26,59,83 and escalating pressures were utilized in 2 studies. 31,73 Occlusive pressures ranged from 130 to 238 mm Hg, while cuff width ranged from 9 to 14 cm. BFR was achieved with occlusion cuffs in 2 studies 26,73 and tourniquets in 4 studies. 23,31,59,83 Duration of BFR exercise regimen ranged from 1 day 25 (to examine acute perceptual and hemodynamic responses) to 16 weeks, with frequency ranging from a single session over 48 hours to 6 sessions per week. One group reported on 2 daily BFR sessions. 73 Exercise volume ranged from 75 to 100 repetitions per session; in 2 studies, 23,83 volume was determined by number of repetitions to volitional failure. 23,83 BFR occlusion periods ranged from 3 to 5 minutes, with rest periods ranging from 45 seconds to 3 minutes.
Overview of Study Protocols a

a Values are presented as mean ± SD where indicated. ACLR, anterior cruciate ligament reconstruction; bpm, beats per minute; BFR, blood flow restriction; MRI, magnetic resonance imaging; NA, not available; postop, postoperative; preop, preoperative; reps, repetitions; RM, repetition maximum; ROM, range of motion.
Outcome Measures
Muscle strength was assessed through measurement of maximal volitional isometric contraction torque in 2 studies 23,83 and by muscular torque ratio of the knee flexors to the knee extensors in 1 study. 23,60,83 Additional measures of muscle strength and activation included surface electromyography (EMG) of the vastus medialis, EMG amplitude, time of sustained contraction, and blood flow to the vastus lateralis. 83 Muscle size was assessed through measurement of the cross-sectional area and volume of the individual muscles, the extensor groups, and the flexor groups, as well as the femoral muscle group en bloc; anatomic cross-sectional measurements were performed through magnetic resonance imaging. 31,60,73,83 Subjective outcomes assessed included the levels of perceived pain and exertion. Physical function assessments included the single-leg anterior reach distance and tests of anterior instability. 23,60 Two studies performed intergroup and temporal comparisons using factorial analysis of variance to assess for differences between BFR and sham, between pre- and postsurgery, and between operative and healthy legs, with post hoc Tukey test for pairwise comparisons where a significant main effect was determined. 23,83 For the purposes of this review, only significant intergroup (BFR vs sham) differences are reported in Tables 5 and 6.
Overview of Outcome Measures a
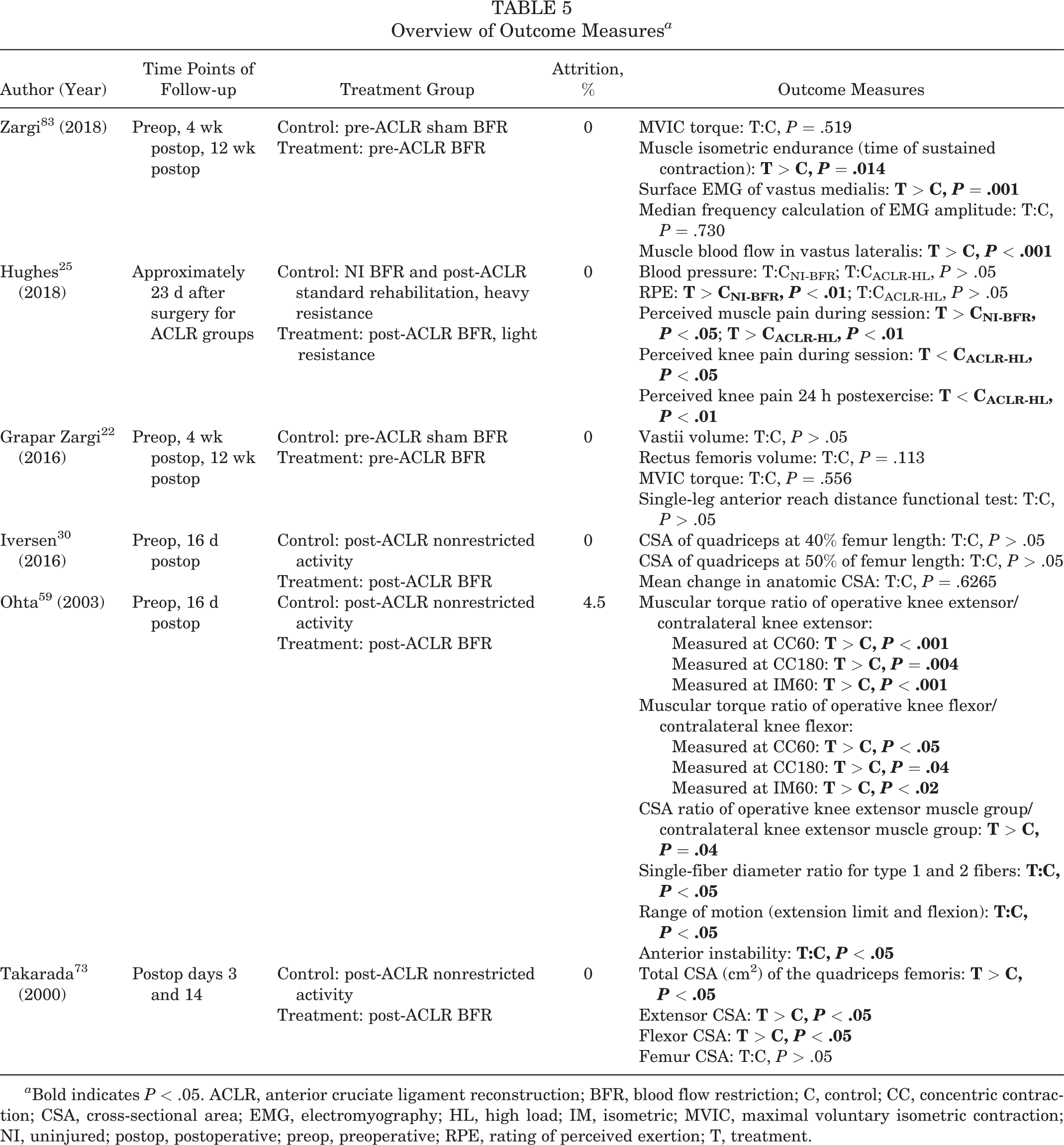
a Bold indicates P < .05. ACLR, anterior cruciate ligament reconstruction; BFR, blood flow restriction; C, control; CC, concentric contraction; CSA, cross-sectional area; EMG, electromyography; HL, high load; IM, isometric; MVIC, maximal voluntary isometric contraction; NI, uninjured; postop, postoperative; preop, preoperative; RPE, rating of perceived exertion; T, treatment.
Comparison of BFR and Non-BFR Outcomes a

a Values are presented as mean ± SD where indicated. Bold P values indicate P < .05. ACLR, anterior cruciate ligament reconstruction; BFR, blood flow restriction; CC, concentric contraction; CSA, cross-sectional area; EMG, electromyography; HL, high load; IM, isometric; MVIC, maximal voluntary isometric contraction; NA, not available; NI, uninjured; postop, postoperative; preop, preoperative; RPE, rating of perceived exertion.
b Muscular torque, concentric contraction at 60 deg/s, expressed as operated:healthy ratio.
c Muscular torque, concentric contraction at 180 deg/s, expressed as operated:healthy ratio.
d Muscular torque, isometric contraction at 60° of knee flexion, expressed as operated:healthy ratio.
e CSA expressed as ratio to femur on same image.
f Anterior instability measured with knee ligament arthrometer KT2000 at 133 N.
Descriptive Outcomes
With respect to BFR as a preoperative intervention, 1 study 23 observed no significant differences in outcome measures, including postoperative changes in vastii or rectus volume. However, a second study by the same group observed that several outcome measures were significantly greater in the BFR group as compared with the sham BFR controls at 12-week follow-up, including muscle isometric endurance (P = .014), surface EMG amplitude of the vastus medialis (P = .001), and muscle blood flow to the vastus lateralis (P < .001). 83
With respect to BFR as a postoperative intervention, 2 of 3 studies 59,73 observed significantly less muscle atrophy as measured by cross-sectional area of the knee extensor muscles when compared with controls (P < .05). Postoperative BFR was also associated with significantly greater cross-sectional area of the flexor and total quadriceps muscle group in 1 of 2 studies (all P < .05) 73 and with significantly greater strength of the operative limb in the other study (all P < .05), as measured by muscular torque ratio of the injured extensor and flexor to their counterparts in the healthy limb. 60 One study comparing subjective outcome measures by Hughes et al found that BFR was associated with significantly increased rates of perceived exertion and reduction of muscle pain during session but significantly decreased levels of knee pain during and after session, as compared with non-BFR ACLR rehabilitation (all P < .05) 26 (Table 5). One study provided data regarding complications, where 2 patients in the LL-BFR group dropped out because of lower limb “dull pain” related to the tourniquet. 60
Study Quality and Reporting
The Jadad score was utilized to assess the quality of the trials included, with scores ranging from 2 to 4. All studies included were self-described as randomized and provided appropriate description of the randomization procedure. Four studies 23,26,31,83 were double-blinded, while 3 provided descriptions of appropriate blinding methods. 23,31,83 Only 1 study included a description of participants who dropped out or withdrew from the study. 60
Discussion
The main findings from this descriptive analysis were as follows: (1) literature surrounding the topic of BFR rehabilitation in patients with ACLR is limited and heterogeneous, and (2) some but not all of the available evidence suggests that BFR as a pre- or postoperative intervention is beneficial to muscle volume and strength/endurance, at least in the early postoperative period, when compared with nonrestricted postoperative activity. These observations are in line with existing literature that has demonstrated increases in muscle hypertrophy with BFR application in healthy 8,51,52,55,80 and injured/postoperative 22,35,74 populations. Additionally, comparison of acute subjective outcomes between LL-BFR and high-load conventional rehabilitation found increased ratings of perceived exertion and reduced in- and postsession knee pain with LL-BFR. With comparable increases in muscle cross-sectional area between LL-BFR and heavy-load training, 60 -62,73 this new observation highlights the appeal of LL-BFR as a potentially effective alternative that can lead to reduced residual knee pain. Ultimately, definitive assessment of the effects of BFR in this population remains uncertain because of the quality of the present literature.
Of the 3 studies assessing strength as an outcome, the 1 with the longest training duration found a difference in muscular torque ratio between the operative knee extensor and the contralateral extensor in patients who underwent 84 sessions of LL-BFR, as opposed to unrestricted low-load training. 60 This was likely due to the presence of a dose-dependent relationship between training and strength gain such that more sessions lead to greater differences. 71 Evidence on other populations in the literature supports a difference in strength gains between LL-BFR and low-resistance training alone prescribed between 6 and 8 weeks of rehabilitation. 10,22,27,32,33 In contrast, evidence on the effect of BFR on post-ACLR muscle atrophy is conflicting. Of the 2 studies reviewed, 1 found almost a 50% reduction in muscle atrophy with BFR, 73 while the other found no difference in quadriceps cross-sectional area between the control and intervention groups. 30 However, authors of the latter study acknowledged subtherapeutic training intensity as a possible reason for this difference and suggested the incorporation of neuromuscular electrostimulation into future research models to detect the effects of BFR on a more granular level. 30
The implementation of BFR has generally been indicated for patients with debilitation undergoing clinical rehabilitation, such as the elderly or surgical candidates 5,11,34,35,68,75,76 or athletes involved in sports at a competitive level. 2,21,30,68,78 While these 2 populations may ostensibly have distinct needs, their goals of rehabilitation or training make BFR an optimal intervention. Initial studies applied hemodynamic occlusion to low-resistance strength training in healthy and active athletes. Since then, several randomized trials and systematic reviews have established its effectiveness in improving muscle hypertrophy, strength, and fiber-type distribution, independently and as a complement to conventional training, while minimizing joint stress and risk of adverse effects. ‡
For this reason, low-intensity resistance training with occlusion can be an effective and safe alternative in patients with sufficient extent of frailty or debility. 41,43,76 BFR also has appeal in rehabilitation of active patients after sports-related injuries, for maintenance of muscle mass and function while injuries heal, to facilitate a more rapid return to preinjury competition. 27,35,74
Isolated incidents of adverse events have been documented in the literature, including 3 cases of syncope, 53 1 case of rhabdomyolysis, 72 1 case of vision loss secondary to central retinal vein occlusion, 4 and 1 case of thoracic venous outflow obstruction in a patient with thoracic outlet syndrome. 59 However, multiple trials and several systematic reviews have supported the safety of BFR rehabilitation with regard to ischemic and hemostatic risks. § With the heterogeneity in quality of evidence, firm recommendations have been difficult to produce, 7,48 but a consensus among clinicians has pointed toward individualizing occlusion pressures, which has important implications for safety and effectiveness. 3,17,27,37,46,48,79
Currently, it is recommended that individual occlusion pressures be calculated as a percentage of the total arterial occlusion pressure (AOP), with individual protocols ranging from 60% to 80%. 35,40,69,84 The gold standard method of measuring AOP and true occlusion is Doppler ultrasound, 6,9,29,56,66 although recent investigations have begun to assess the feasibility of pulse oximetry as a lower maintenance alternative. 77,84 A previous method in the literature attempted to predict the AOP as a percentage of the brachial systolic blood pressure. 48 However, a more recent investigation identified thigh circumference as the greatest predictor of AOP. 44 Therefore, limb circumference is being investigated as a highly effective nonmodifiable factor that can predict pressures applied for complete to partial occlusion. 17,28,44,81 Additionally, considerations for setting initial pressures according to tourniquet material (nylon vs elastic) has been highlighted. 46 Of note, none of the studies included in this systematic review completely employed these guidelines in their methods.
The current paradigm in training protocol is experiencing a similar transition toward individualized prescriptions to maximize gains. Studies in the literature have observed a domain-specific timeline for LL-BFR to demonstrate a significant advantage over non-BFR low-resistance training. Significant hypertrophy has been noted after as short as 6 days of training 21 and can be effectively achieved by most protocols: rehabilitation trials for patients undergoing surgery typically last 2 to 6 weeks and as long as 20 weeks. 16 Those for the elderly last longer, averaging 10 to 12 weeks. 42,54,61,62,65,76 However, there is the observation that improvements in muscle strength require a longer duration of training. 63 A comparative study demonstrated that while high-load resistance training (without BFR) yielded greater strength increases initially, results were equivalent to LL-BFR at 12 weeks of training. 12 This implies that an appropriate period of familiarization may yield hormonal and neural adaptations to more effectively utilize occlusion training. 67
A comparison of pre- and postoperative BFR training in patients undergoing ACLR in this review found the strongest evidence of significant improvements in muscle hypertrophy and strength over standard rehabilitation protocols in candidates for postoperative BFR. Of the 2 studies on preoperative BFR, only 1 found a significant improvement over sham intervention in muscular endurance, activation, and perfusion. These outcomes were likely confounded by the significantly reduced training durations of preoperative BFR (5 sessions over 10 days). 23,83 Additionally, both trials enrolled only patients with chronic ACL rupture, where there is a greater likelihood of functional adaptation after injury. An ongoing trial is examining 4 weeks of BFR prehabilitation as part of an overall perioperative protocol for ACLR, providing further insight to the optimal timing of BFR intervention 16 (Appendix Table A1). The strong evidence for the increased benefit of combined pre- and postoperative BFR rehabilitation after orthopaedic surgery 18,64 makes it imperative to continue evaluating BFR as a prehabilitation intervention.
There are several limitations to consider while interpreting the results of this study. While significant differences in short-term muscle strength and hypertrophy were demonstrated in some of the studies, none provided follow-up data with regard to changes in primary clinical outcomes or return to sports. The heterogeneity in outcome variables precluded a meta-analysis. Torque and cross-sectional areas are common outcome measurements, are readily obtained, 2,5,8,10,11,73,81 -83 and warrant inclusion in the design of future trials. The study by Hughes et al 26 examining immediate subjective perspectives during and after BFR performed only a single session. Their results may not be generalizable to patients who are well-adapted to the volume and intensity of BFR protocols. Overall, there was a small number of patients in the collective cohort of studies reviewed and poor reporting of adverse events. Long-term follow-up data in these studies were sparse, and firm recommendations regarding safety cannot be made.
Conclusion
The evidence for the benefits of BFR rehabilitation after ACLR is sparse and heterogeneous possibly because of the novel nature of the technique. Although several studies have shown potential muscle strength and hypertrophy benefits in patients undergoing perioperative BFR in the setting of ACLR, future investigations with standardized outcomes, long-term follow-up, and more robust sample sizes are required to draw more definitive conclusions.
Footnotes
Notes
Final revision submitted November 11, 2019; accepted November 25, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.U.N. has received educational support from Smith & Nephew and hospitality payments from Stryker, Wright Medical, and Zimmer Biomet. B.F. has received research support from Arthrex, Smith & Nephew, and Stryker; educational support from Medwest; consulting fees from Sonoma Orthopedics and Stryker; honoraria from Arthrosurface; and royalties from Elsevier and has stock/stock options in Jace Medical. J.C. has received educational support from Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Protocols of Ongoing Level 1 Trials on Perioperative BFR in Patients Undergoing ACLR a

| Author (Year) | Device Used | Exercises | Volume and Frequency | Duration |
|---|---|---|---|---|
| Erickson 15 (2019) | Pressurized cuff to the proximal thigh that partially occludes blood flow as the patient exercises | Primary outcome measure: quadriceps strength (peak torque, rate of torque development) Secondary outcome measures: knee extensor movement, knee flexion excursion, knee flexion angle, quadriceps cross-sectional area, quadriceps muscle physiology |
Not published in abstract | Presurgical blood flow restriction therapy 3×/wk for 4 wk leading up to surgery Postsurgical blood flow restriction therapy 3×/wk for 4-5 mo |
| Lambert 36 (2019) | Automated tourniquet around the proximal thigh outfitted with Doppler (Delfi) | Weeks 1-3: quadriceps contractions Weeks 3-12: bilateral leg press Weeks 4-6: hamstring curl Weeks 4-12: eccentric leg press Weeks 7-12: eccentric hamstring curl |
All exercises preformed at 20% predicted 1 repetition maximum of contralateral leg All exercises, 4 sets of 30-15-15-15 repetitions separated by 30-s rest BFR group performed exercises with cuff at 80% arterial limb occlusion |
12 wk of rehabilitation (2 sessions/wk) beginning at 10 d postsurgery Functional assessments performed at weeks 8 and 12 postsurgery DEXA scan performed pre- and postoperatively at weeks 6 and 12 |
a Occlusion pressure/cuff width was not published in either abstract. ACLR, anterior cruciate ligament reconstruction; BFR, blood flow restriction; DEXA, dual-energy x-ray absorptiometry.