
Abstract
Background:
The incidence of pectoralis major tendon tears is increasing, and repair is generally considered; however, a paucity of comparative data are available to demonstrate the superiority of operative treatment.
Purpose/Hypothesis:
The purpose of this study is to compare the outcomes of operative and nonoperative treatment of pectoralis major tendon tears. We hypothesized that repair would result in superior outcomes compared with nonoperative treatment.
Methods:
In accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a systematic review of the literature was completed by use of MEDLINE, SPORTDiscus, CINAHL, Cochrane, EMBASE, and Web of Science databases. We included English-language studies that had a minimum of 6 months of average follow-up and 5 cases per study. The MINORS (Methodological Index for Non-Randomized Studies) was used to assess the quality of the existing literature. Meta-analysis of pooled mechanisms of injury and outcomes was completed. Pooled effect sizes were calculated from random-effects models. Continuous variables were assessed by use of mixed-model analysis, with the individual study designated as a random effect and the desired treatment for comparison as a fixed effect. Bivariate frequency data were transformed via the Freeman-Tukey log-linear transformation for variance stabilization and then assessed through use of a mixed model with a study level random effect and subsequently back-transformed. Significance was set at P < .05.
Results:
A total of 23 articles with 664 injuries met the inclusion criteria for comparison. All patients were male, with an average age of 31.48 years; 63.2% of injuries occurred during weight training, and the average follow-up was 37.02 months. Included studies had moderately high methodological quality. Operative treatment was significantly superior to nonoperative treatment, with relative improvements of functional outcome by 23.33% (0.70 improvement by Bak criteria which is scored 1-4; P = .027), full isometric strength 77.07% (P < .001), isokinetic strength 28.86% (P < .001) compared with the uninjured arm, cosmesis satisfaction 13.79% (P = .037), and resting deformity 98.85% (P < .001). The overall complication rate for operative treatment was 14.21%, including a 3.08% rate of rerupture.
Conclusion:
Pectoralis major tendon repair resulted in significantly superior outcomes compared with nonoperative treatment, with an associated 14.21% complication rate. Statistically significant improvements were noted in functional outcome, isokinetic strength, isometric strength, cosmesis, and resting deformity.
The first reported case of injury to the pectoralis major tendon (PMT) involved heavy lifting, although the injury was caused by hoisting a large side of beef off a meat hook instead of a maximum lift on the bench press. 33 Widely viewed as rare injuries, 16,26,29,31,45 PMT tears appear to be increasing in incidence, likely a result of increased interest in weight training and participation in athletic pursuits. 3,4,8,10,26 Contemporary injuries to the PMT typically occur during exercise or training, mostly during the eccentric phase of bench press exercises. ¶ Patients typically report a sharp tearing sensation and weakness with resisted adduction and internal rotation of the affected shoulder. Examination of an acute tear generally demonstrates a palpable defect and deformity of the anterior axillary fold. Ecchymosis localized to the anterior arm is relatively specific for distal humeral attachment rupture rather than a musculotendinous junction rupture. 32
The pectoralis major muscle is broad and fan-shaped, with a multipennate origin from the clavicle, costal cartilage of the first 6 ribs, distal sternum, and external oblique aponeurosis. 1,3,10,31,32,43 Although the literature is largely consistent with regard to the anatomic origins of the muscle, some disagreement is found regarding its insertional anatomic features. Most authors have stated that the clavicular and sternal fibers undergo a twist before insertion, such that the fibers insert proximally and posterior to the clavicular fibers on the humerus (Figure 1). 6,13,23,27,31,32 In their anatomic study, ElMaraghy and Devereaux 10 demonstrated that the tendon is a bilaminar structure connected at the distal end, in which the clavicular fibers and superior-most sternal fibers insert in the anterior lamina and the more inferior sternal fibers and oblique fibers insert in the posterior lamina. 10 The unique insertional anatomic features of the PMT place the muscle at a mechanical disadvantage during eccentric contraction with the arm extended and abducted, and the sternal head is particularly at risk. # Such indirect mechanisms typically result in insertional avulsions or ruptures at the level of the tendon or musculotendinous junction, whereas direct trauma results in injury to the muscle belly. 20,31 Given the active population in which the injury occurs, surgical repair of the pectoralis major has generally been considered to offer superior results over nonoperative treatment. 3,5,8,14,16,26,27,31,44 However, these studies were limited in power, drawing conclusions from 112 and 73 total cases. 1,3 We sought to compare the outcomes of operative and nonoperative treatment of pectoralis major tears through an analysis of a larger and more recent body of cases. We hypothesized that repair would result in superior outcomes compared with nonoperative treatment.

Anatomic features of the pectoralis major. (A) Illustration demonstrating that the orientation of each muscle segment anteriorly overlaps the segment below it. (B) Distally, the insertion is divided into anterior and posterior tendon layers with the most inferior 2 or 3 segments (s5-s7) of the sternal head contributing to the posterior tendon layer. AT, anterior tendon; CH, clavicular head; H, humerus; PT, posterior tendon; s1-s7, sternal segments. (Reprinted with permission from ElMaraghy AW, Devereaux MW. A systematic review and comprehensive classification of pectoralis major tears. J Shoulder Elbow Surg. 2012;21(3):412-422. ©2012, Elsevier.)
Methods
Search Strategy
In accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, a systematic review of the literature was completed using MEDLINE, SPORTDiscus, CINAHL, Cochrane, EMBASE, and Web of Science databases. This search included all literature available up to February 2019. The following keywords were used: “pectoralis major,” “rupture,” “avulsion,” “tear,” and “injury.” Boolean operators “OR” and “AND” were used to combine synonyms and categories. “Pectoralis minor,” “rotator cuff,” “supraspinatus,” “infraspinatus,” “subscapularis,” “teres minor,” “strain,” “sprain,” “tendinopathy”, “tendonitis,” “tendinitis,” and “tenosynovitis” terms were excluded.
Eligibility Criteria
All English-language studies were included if they investigated PMT tears. Included articles must have confirmed the diagnosis of pectoralis major rupture, entailed an average follow-up period of at least 6 months, and reported relevant outcome data after either operative or nonoperative treatment. Accordingly, imaging reviews without outcome data reported, literature reviews, anatomic or histologic studies, surgical technique notes, biomechanical investigations, and animal studies were not eligible for inclusion.
Study Selection
Studies returned from the initial database search (Figure 2) were independently reviewed by 2 reviewers (B.P.M. and W.J.F.). The articles were included or excluded per the aforementioned criteria. When the decision could not be reached for any particular article, the article was submitted to a third author (B.M.B.) for review and ultimate decision. Throughout the duration of the search, the contents of each article, as well as the reference list, were screened for overlap of patients from other studies.
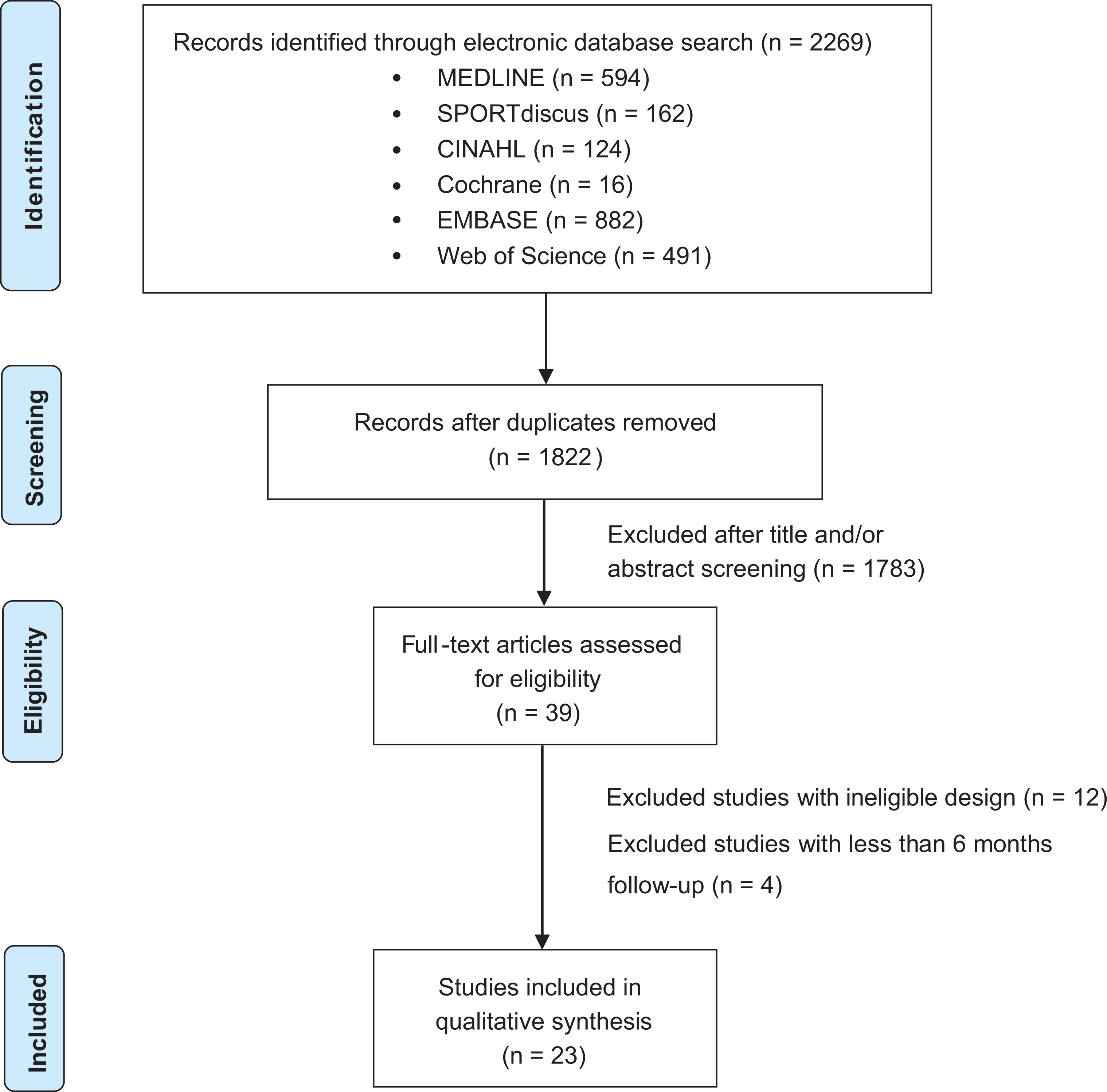
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Data Extraction
Data were extracted by review of each study for the number of participants, mean age, mean duration of follow-up, timing of surgery, and the following outcome measures: Single Assessment Numeric Evaluation (SANE) score, American Shoulder and Elbow Society (ASES) score, Disabilities of the Arm, Shoulder and Hand (DASH) score, functional outcome, range of motion (ROM), return to full isometric strength, isokinetic strength, change in maximum bench press weight, postoperative pain, return to preinjury activity level, presence of resting deformity, satisfaction with cosmesis, overall satisfaction, and postoperative complications. A functional outcome measure was adopted from a composite of the criteria used by Bak et al 3 (pain, ROM, cosmesis, strength, and return to sport or activity). Functional outcome scores were separated into excellent (4), good (3), fair (2), or poor (1) and were assessed as a continuous variable. Each outcome was assessed by comparing operative and nonoperative management. Acute was defined as less than 6 weeks and chronic was defined as 6 weeks or more based on a previous systematic review. 12 In studies that included patients with both acute and chronic repairs without stratifying results based on a 6-week cutoff, all patients were considered to belong to either the acute or the chronic group if 75% or more of the patients belonged to 1 group. Complications were pooled into the following categories: infection, deep venous thrombosis/pulmonary embolism, rerupture, additional surgery, biceps tendinitis, neuropathy (including transient nerve palsy, numbness, and paresthesias), persistent pain, and hematoma formation.
Quality Assessment
Each article went through a quality assessment by 3 authors (B.P.M., C.M.C., D.X.W.) using criteria from the Methodological Index for Non-Randomized Studies (MINORS), a validated tool to discern the methodological quality of nonrandomized studies. 37 The 3 authors scored 23 studies. These 3 values were averaged to compose a final score for each study, with higher scores correlating with higher quality studies (Table 1). The highest possible score was 16 for noncomparative studies and 24 for comparative studies. When the MINORS criteria were validated, Slim et al 37 noted that 15 high-quality randomized trials had a mean rating of 23.1.
All Studies Included for Meta-Analysis a

a Data are presented as mean ± SD or mean (range). Dashes indicate not reported. ASES, American Shoulder and Elbow Society score; BMI, body mass index; DASH, Disabilities of the Arm, Shoulder and Hand score; MINORS, Methodological Index for Non-Randomized Studies; MRI, magnetic resonance imaging; NFL, National Football League; ROM, range of motion; SANE, Single Assessment Numeric Evaluation score; SF-12, 12-Item Short-Form Health Survey; SF-36, 36-Item Short-Form Health Survey; VAS, visual analog scale.
b Follow-up preceded by a greater-than symbol (>) was inferred from outcome measures and not explicitly stated in the publication.
Best Evidence Synthesis
Each article’s level of evidence was evaluated with the American Academy of Orthopaedic Surgeons’ levels of evidence system. The majority of the articles were of lower methodological quality, consisting of one level 2 study, 8 four level 3 studies, 14,16,35,43 and 18 level 4 studies. **
Statistical Methods
Means and standard deviations were obtained directly from the eligible studies. Several studies provided only the means for continuous variables without reporting study-level variance data in their results. If such a study provided an absolute range of the data set, standard deviation was estimated as described in the method proposed by Wan et al. 42 If fewer than half of the studies in a given treatment group remained without variance data, standard deviations were imputed by use of Restricted Estimated Maximum Likelihood multiple imputation based on the other studies in that group. If more than half of the variance data were missing, zero imputation was used, and studies without variance data were excluded for that variable. For patients whose bench press results were lost to follow-up, change from baseline values was imputed using a calculated correlation coefficient as specified by the Cochrane Handbook. 19 Pooled effects were calculated with continuous variables assessed via a mixed-model analysis, with the individual study designated as a random effect and the desired treatment groups for comparison designated as a fixed effect. Bivariate frequency data were transformed by use of the Freeman-Tukey log-linear transformation for variance stabilization and then assessed via a mixed model with a study-level random effect and subsequent back-transformation for estimation of summary effects. All statistics were conducted in R version 3.6.0 (R Foundation for Statistical Computing), and models were computed using the metafor package.
Results
We included 23 studies †† that comprised 693 PMT tears; for 664 of these tears, the studies specified operative or nonoperative treatment, and appropriate outcome measures were available for comparison (Table 1). All 23 studies included operative treatment of PMT tears, and there were 603 of these repairs in total. A further 6 studies also reported on nonoperative treatment of 61 tears. 8,14,16,35,43,44 Of the 603 operatively treated injuries, there were 116 acute repairs from 12 studies, ‡‡ 90 chronic repairs from 11 studies, §§ 410 complete repairs from 16 studies, ∥∥ and 134 partial repairs from 4 studies. 20,22,28,30 Partial repair was indicated for patients who sustained an injury without 100% of the insertional footprint avulsed, leading to patient-reported weakness, pain, or deformity, usually with weakness being the major concern. Partial repair was defined as repair of the avulsed portion of the incomplete tear. 20,22,28,30 Included studies scored a mean (±SD) 14.90 ± 4.41 (range, 7-24) by MINORS criteria.
Demographic data were gathered and averaged when available. All patients were male. The operative group had a mean age of 31.39 years (range, 18-59 years), whereas the nonoperative group had a mean age of 32.38 years (range, 21-50 years), for an overall average age of 31.48 years (range 18-59 years). Patients treated operatively or nonoperatively were followed for an average of 41.43 months and 13.45 months, respectively, for an overall average follow-up of 37.02 months. The majority of injuries were sustained during weight training (Table 2). Most patients were treated with primary repair without graft augmentation. Reconstruction with graft augmentation was typically used in cases of chronic or subacute tears with retraction to the musculotendinous junction that would compromise retensioning of the repair to the insertional footprint or in cases of poor native tendon quality. A total of 42 pectoralis major tear repairs were augmented with grafts. de Castro Pochini et al 8 included 19 patients with reconstructions performed with both semitendinosus and gracilis autografts. Merolla et al 26 included 4 patients with chronic ruptures repaired with fascia lata allograft. Finally, Neumann et al 29 investigated the efficacy of dermal allografts for reconstruction of chronic tears in their series of 19 patients.
Mechanisms of Injury a

a Data are presented as incidence and sample size alone.
After repair, patients experienced a mean ± SE SANE score of 84.80 ± 0.92 (95% CI, 82.99 to 86.62), ASES score of 95.15 ± 1.36 (95% CI, 92.43 to 97.88), DASH score of 8.52 ± 0.15 (95% CI, 2.18 to 14.85), and loss of bench press of 112.34 ± 4.58 lb (95% CI, 103.23 to 121.44 lb). Patients had a mean rate of return to preinjury activity of 94.57% (95% CI, 88.80% to 98.68%), pain-free proportion of 88.13% (95% CI, 61.95% to 100%), and overall satisfaction of 91.16% (95% CI, 73.09% to 100%). These outcomes were not consistently reported (<5 patients total) in the nonoperative studies and were, therefore, not compared between groups. Whereas no complications were reported in the nonoperative group, the operative group reported a 14.21% (95% CI, 7.98% to 21.54%) complication incidence, including 3.08% rerupture, 3.03% persistent pain, and 2.28% additional surgery (Table 3). Additional surgery was performed in 12 of 17 patients for rerupture, 3 for infection, 1 for hematoma evacuation, and 1 for biceps tendinitis.
Complications of Repair a

a Data are presented as random effects weighted percentage incidence. No. indicates sample size of the patients reported for the specific outcome analyzed. DVT/PE, deep venous thrombosis/pulmonary embolism.
When comparison between operative and nonoperative treatment of pectoralis major tears was possible, operative treatment fared better (Table 4). Of the 6 categories that could be compared between treatment modalities, functional outcome was superior for operative treatment by 23.33% or 0.70 improvement by Bak criteria (P = .027, Figure 3), proportion of injured shoulders that regained full isometric strength was superior for operative treatment by 77.07% (P < .001, Figure 4), change in isokinetic strength compared with the contralateral side was superior for operative treatment by 28.86% (P < .001, Figure 5), proportion of injured shoulders with a resting deformity was superior for operative treatment by 13.79% (P = .037, Figure 6), and overall satisfaction with cosmesis was superior for operative treatment by 98.85% (P < .001, Figure 7) . The proportion of patients with full range of motion was similar between groups.
Comparison of Outcomes Between Operative and Nonoperative Treatment a

a Data are presented as mean ± SE (95% CI) or percentage (95% CI) when available.

Forest plot: functional outcome. Data are presented as mean [95% CI].

Forest plot: percentage of full isometric strength. Data are presented as mean [95% CI].

Forest plot: isokinetic strength change. Data are presented as mean [95% CI].

Forest plot: resting deformity. Data are presented as mean [95% CI].

Forest plot: cosmetic satisfaction. Data are presented as mean [95% CI].
After reconstruction with graft augmentation, patients experienced a mean ± SE SANE score of 80.00 ± 10.26 (95% CI, 59.89 to 100), ASES of 90.30 ± 12.30 (95% CI, 66.19 to 100), DASH of 8.00 ± 12.90 (95% CI, 0 to 33.28), functional outcome of 3.51 ± 0.46 (95% CI, 2.60 to 4.42), and isokinetic strength loss compared with the contralateral side of 10.41% ± 14.79% (95% CI, –39.39% to 18.57%). The proportion of patients who achieved full ROM was 100% (95% CI, 76.34% to 100%); return to full isometric strength, 100% (95% CI, 59.52% to 100%); return to preinjury activity, 50.00% (95% CI, 0% to 100%); pain-free status, 100.00% (95% CI, 24.60% to 100%); and cosmetic satisfaction, 100.00% (95% CI, 58.86% to 100%). No complications were reported for reconstruction with graft augmentation. Comparing these outcomes with the results for nonoperative treatment revealed superior return to full isometric strength in the reconstruction group (P < .006). No statistically significant differences were found between outcomes for primary repair without graft augmentation and reconstruction with graft augmentation. Due to lack of separate reporting of outcomes for patients with complete or partial repairs (n = 3), it was not possible to separately analyze or compare these outcomes with other subgroups of interest.
Discussion
This is the largest and most comprehensive study to compare the outcomes of PMT repair versus nonoperative treatment. The most important findings from this analysis are that repair led to improvement in functional outcome, isokinetic strength, isometric strength, cosmesis, and resting deformity with an overall complication rate of 14.21% compared with nonoperative treatment. The majority of patients sustained their injury during weight training. Patients had similar demographics, but patients treated nonoperatively were followed for a shorter period of time (mean 13.45 vs 41.43 months). Comparison of other outcomes, including SANE, ASES, DASH, bench press, return to preinjury activity, pain, and overall satisfaction, was not possible given the lack of reported data for patients treated nonoperatively. With the exception of 1 article, the data reported came from studies of lower methodological quality with level 3 or 4 evidence. Despite this, included studies had a moderately high methodological quality, as supported by MINORS scores.
Before the present study, the largest and highest level of evidence study examining operative and nonoperative treatment of PMT tears was conducted by de Castro Pochini et al. 8 In their prospective cohort of 60 patients (31 repairs and 29 patients treated nonoperatively) with an average follow-up of 48.25 months, patients treated nonoperatively experienced poor outcomes in 31% of cases, fair outcomes in 41.4% of cases, good outcomes in 27.6% of cases, and no excellent outcomes by Bak criteria. In contrast, patients who underwent repair experienced poor outcomes in 9.7% of cases, no fair outcomes, good outcomes in 22.6% of cases, and excellent outcomes in 67.7% of cases. Additionally, patients treated nonoperatively had a loss of 41.7% of isokinetic strength at 60 deg/s compared with 14.3% loss for patients whose injury was repaired. These differences were all statistically significant.
In 2 previous meta-analyses, Bak et al 3 and Äärimaa et al 1 analyzed outcomes of PMT rupture treatment. However, both of these studies were limited in the power of their meta-analysis, with only 112 and 73 cases total, respectively. Bak et al concluded that repair had significantly better outcomes compared with nonoperative treatment or chronic repair. Notably, the operative and nonoperative groups had only 57 and 15 patients, respectively. Äärimaa et al compared acute repairs, chronic repairs, and nonoperative treatment and concluded that acute repair had superior outcomes to both chronic repair and nonoperative treatment. However, that study included only 32 acute repairs, 19 chronic repairs, and 22 nonoperatively treated injuries. The largest study to date comparing operative and nonoperative treatment of PMT tears was conducted by de Castro Pochini et al. 8 That study entailed 31 repairs and 29 patients treated nonoperatively and 4 years average follow-up, and the authors concluded that repairs were superior in functional outcome and isokinetic strength.
Generally, our findings are in line with these previous studies’ findings, but we believe we add a significant contribution to the literature because of our large sample size and analysis of nearly all published outcomes. We included 61 nonoperative cases in our analysis, whereas de Castro Pochini et al 8 reported 29 cases. Additionally, the largest meta-analysis before ours included a total of 112 injuries, and our present analysis included 664 injuries. Because of these factors, we believe our study is better suited to compare outcomes between these groups.
Limitations
Several limitations of this study deserve mention. The majority of studies from which the data were extracted had low methodological quality. Limitations in quality were mostly the result of differing surgical techniques, limited long-term follow-up, and lack of randomization or blinding. Also, the diversity of reported outcomes in each of the included studies required aggregation of the results into large groups for data analysis. The assorted patient population, which ranged from professional athletes to recreational athletes, may reflect what a clinician would encounter in practice. However, this heterogeneity of patients could have confounded the results, which may be more accurately assessed in a subgroup analysis for future studies. Lack of clear injury descriptions across studies could have produced discrepancies in the type or extent of PMT tears. Subgroup comparisons between acute and chronic repairs, between complete and partial repairs, and among repairs by the various methods of fixation were outside the scope of the present study, but this analysis will be presented as part of another study. Because studies did not typically discuss the rehabilitation protocols that patients were prescribed, this was also not analyzable. We believe this information is especially important in regard to the nonoperatively treated patients. Furthermore, although the number of cases incorporated in the nonoperative group in this study represents the largest in the literature to date (N = 61), this is still a relatively smaller sample size than the aggregated number in the operative group (N = 664). This may have provided a limited representation of the true outcomes seen in these specific patients. In particular, the small sample size of the nonoperative group, which represents the aggregated data available in the literature, weakens any comparison between operative and nonoperative groups. With these numbers, our results and conclusions comparing operative and nonoperative outcomes should be regarded as speculative. Although we found statistically significant differences for outcomes between operative and nonoperative treatment, it is not possible to fully comment on the clinical significance of these differences because minimal clinically important differences have not been established in the literature for PMT tears. Although a link between the use of anabolic steroids and PMT tears has been reported, this topic was outside the scope of the present study and merits further consideration and study. 1 Additionally, although we analyzed return to preinjury activity level as part of the composite functional outcome, the specific sports or activities to which the patients returned were not analyzable due to heterogeneous or absent reporting. The greatest strength of this study is the large aggregated sample size of 664 PMT tears, which is more robust than any previous study. This allowed for a more comprehensive data analysis and reduced the effect of bias from any individual study. Also, this is the first study of PMT tears to provide a quality assessment of the included studies using a validated tool (MINORS criteria) designed specifically for nonrandomized trials. 37 Larger prospective studies are necessary to compare outcomes of repaired and nonoperatively treated PMT tears.
Conclusion
The results of this meta-analysis suggest that patients with PMT ruptures who undergo operative repair have significantly better functional outcome, isokinetic strength, isometric strength, cosmesis, and resting deformity compared with nonoperative treatment. Additionally, when necessary, reconstruction with graft augmentation appears to have an advantage over nonoperative treatment for isometric strength. Operative treatment was associated with a 14.21% complication rate. The aggregated sample size of the nonoperative group, although the largest in the literature to date, was still relatively small compared with the number in the operative group, which underscores the need for larger prospective studies examining outcomes of nonoperative treatment of these injuries.
Footnotes
Acknowledgment
We would like to acknowledge both Benjamin Campbell and Samir Abu-Hamad for their assistance with the literature review and organization.
Final revision submitted October 22, 2019; accepted October 25, 2019.
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or US government. J.A.K. is a military servicemember. This work was prepared as a part of his official duties. Title 17 USC 105 provides that “copyright protection under this title is not available for any work of the United States Government.” Title 17 USC 101 defines a US government work as a work prepared by a military servicemember or employee of the US government as part of that person’s official duties.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.F.P. has received educational support from Arthrex and hospitality payments from Smith & Nephew. E.S.C. has received educational support from Arthrex, Smith & Nephew, and Supreme Orthopedic Systems. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.