
Abstract
Background:
Rotator cuff pathology is the most common cause of shoulder pain in adults, accounting for nearly 70% of shoulder-related visits to clinicians. However, physical examination findings may be limited because of pain or patient inhibition.
Purpose:
To establish whether a relationship exists between pain, range of motion, and strength in patients with a full-thickness rotator cuff tear.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A single-blind, randomized controlled study of 40 patients undergoing rotator cuff repair for full-thickness rotator cuff tears was performed. Patients were randomized to receive either a subacromial 10-mL 2% lidocaine injection or a sham injection, with no contents being injected into the subacromial space. Before the injection, patients were assessed using a visual analog scale for pain (VAS-Pain) as well as the Constant-Murley subjective questionnaire and objective physical examination. The examination was repeated 10 minutes after injection and 6 months postoperatively. VAS-Pain after injection was not assessed. The assessment at 6 months was performed to demonstrate improvement of rotator cuff function after operative management. Statistical analysis included Student t and chi-square tests as well as multivariate binomial logistic regression analyses to identify predictors for improvement after injection. Results were considered significant if P < .05.
Results:
Range of motion, strength, and Constant-Murley score significantly improved after a subacromial lidocaine injection (P < .05). Range of motion, strength, Constant-Murley score, and VAS-Pain significantly improved at final follow-up compared with the preinjection assessment for both groups (P < .05); however, there was no difference (P > .05) between groups at 6 months postoperatively.
Conclusion:
After subacromial lidocaine injections, patients exhibited modest but significant improvements in range of motion, strength, and the Constant-Murley score. Pain may limit range of motion and strength in patients with full-thickness rotator cuff tears independent of the mechanical impact of the tear itself.
Registration:
NCT02693444 (ClinicalTrials.gov identifier).
Rotator cuff pathology is the most common cause of shoulder pain in adults, accounting for nearly 70% of shoulder-related visits to clinicians. 21 Although asymptomatic rotator cuff tears occur in 30% of patients older than 60 years of age, symptomatic pathology results in pain, weakness, stiffness, and loss of range of motion. 9,16,21 Assessment of this pathology can be challenging as the sensitivity and specificity of provocative maneuvers are variable. 26 In patients with minor structural damage, physical examination findings may be of limited utility because of pain or patients limiting function secondary to pain avoidance.
Prompt and efficacious diagnosis of rotator cuff tears is imperative to improve patient outcomes. 6,13 Therefore, physicians may consider a subacromial anesthetic injection to improve diagnostic probability. If weakness or limited range of motion persists after an anesthetic injection, it should raise concern for rotator cuff pathology. 11 Previous investigations 2,20 have demonstrated that subacromial anesthetic injections improved external rotation strength in patients with full-thickness rotator cuff tear, while Farshad et al 11 illustrated no effect of subacromial anesthetic injections on the strength of healthy individuals.
The purpose of this investigation was to establish whether a relationship exists between pain, range of motion, and strength in patients with a full-thickness rotator cuff tear as assessed through physical examination after a subacromial anesthetic injection. We hypothesized that (1) patients with full-thickness rotator cuff tears receiving a subacromial anesthetic injection will exhibit improved strength and range of motion in comparison with those who did not receive an anesthetic and (2) there will be no difference in outcomes between both cohorts 6 months after operative management.
Methods
The study was approved by the local institutional review board, and the study was registered on ClinicalTrials.gov A single-blind, randomized controlled study was implemented. Patients were included if they were between the ages of 18 and 65 years at the time of surgery, if they had full-thickness tears of the supraspinatus and/or infraspinatus tendons that were <3 cm, and if they were scheduled to undergo elective rotator cuff repair at our institution. Patients were excluded if they were undergoing a revision procedure, if there was subscapularis tendon involvement (partial- or full-thickness tear), if the tear was partial or irreparable, or if the tear was ≥3 cm. If arthroscopy revealed a partial tear, subscapularis involvement, or an irreparable tear, the patient was removed from the investigation. Patient characteristics such as age, sex, body mass index (BMI), as well as concomitant procedures were collected. A random number generator (Microsoft Excel) was used to assign patients to either treatment group. Patients either received a 10-mL subacromial injection of 2% lidocaine or had a needle with an empty syringe placed into the subacromial space with no contents being injected into the space. The control group was originally designed to receive 10 mL of saline. However, the first 3 patients enrolled in this group experienced significant pain with saline injections, thus, the decision was made to implement a needle with an empty syringe as the control group. Patients who received a saline injection were removed from the analysis.
After informed consent was obtained, patients were randomized into either group. Before injection, patients were assessed using the visual analog scale for pain (VAS-Pain) as well as the Constant-Murley subjective questionnaire and objective physical examination 17 by members of the study staff (A.A., R.N.P.). The physical examination was performed with the patient standing upright. Maximal isometric forward flexion strength and abduction strength with the arm initially positioned at the patient’s side without elbow support were measured with a dynamometer (Manual Muscle Tester; Lafayette Instruments) until severe pain further limited muscle contraction. Forward flexion and abduction range of motion were measured using a goniometer. Internal and external rotation range of motion were also assessed. Patients performed active unassisted range of motion until severe pain further limited their motion. Strength and range of motion were measured in foot-pounds and degrees, respectively.
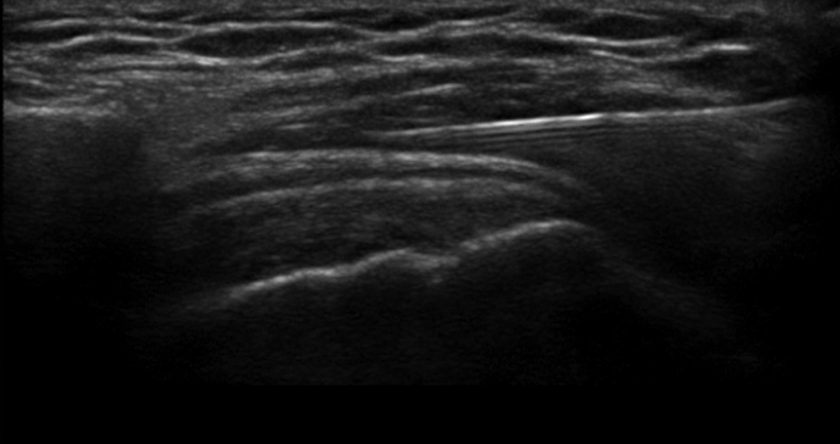
After initial physical examination, the patient then received either the injection or the control, which was performed by the first author (B.F.) under ultrasound guidance. The injection consisted of a 10-mL injection of 2% lidocaine hydrochloride into the subacromial space (Figure 1). An injection of this volume represents the volume of the subacromial space 22 and is the standard protocol implemented in our institution. The control injection consisted of a needle with an empty syringe placed into the subacromial space (Figure 2). To ensure proper blinding, patients were positioned to face away from the ultrasound monitor and the syringe during the injection. Patients were positioned in a seated position with the hand of the injected arm placed on their hip. The area was prepared with chlorhexadine, and an ultrasound probe was then placed on the shoulder skin surface to visualize the subacromial space. A 22-gauge needle was inserted 2 cm lateral to the acromion at an angle of 45°. The fluid was injected after visualization of the needle in the subacromial space.

Ultrasound imaging of lidocaine injection into the subacromial space (study group).
Ultrasound imaging of needle with empty syringe entering the subacromial space (control group).
Ten minutes were allowed to pass after the subacromial injection to allow enough time for the lidocaine to perfuse the tissue, and the Constant-Murley physical examination was then performed again by members of the study staff (A.A., R.N.P). VAS-Pain after injection was not assessed. The patient underwent standard arthroscopic rotator cuff repair performed by the first author on the same day of the examination and the standard rehabilitation protocol ensued. The size of the rotator cuff tear was measured intraoperatively with an arthroscopic hook probe. At the 6-month postoperative clinical visit, the time from which the majority of improvement in strength and ROM is seen, 32 patients were assessed once again using the VAS-Pain scale and Constant-Murley subjective questionnaire and objective physical examination. 17 The assessment at 6 months was performed to demonstrate the improvement in rotator cuff function after operative intervention.
Statistical Analysis
Statistical analysis was performed with R Studio software version 1.0.143 (R Foundation for Statistical Computing) and Microsoft Excel (Microsoft Corporation). The Student t test was performed for comparisons of range of motion, strength, and overall Constant-Murley score. Patient characteristics were compared using chi-square analysis. Predictors of change in the Constant-Murley score after intervention were assessed through a multivariate binomial regression analysis controlling for patient characteristics, rotator cuff tear size, preoperative pain level, as well as lidocaine injection. Statistical significance was determined (P < .05).
As described by Yian et al, 31 an a priori power analysis was performed (α = 0.05, β = 80%) using average range of motion, strength, and Constant-Murley scores in healthy shoulders receiving an injection of lidocaine. Assuming that a 20% change in these metrics provided a clinically detectable difference, 31 it was determined that 16 patients per group was sufficient to provide a statistically significant difference. Last, to account for 20% attrition at the final follow-up, 4 additional patients were enrolled in each group.
Results
Forty patients with full-thickness rotator cuff tears were enrolled in the study from September 2017 until August 2018, with the first author (B.F.) completing all 40 procedures. A single patient underwent reverse total shoulder arthroplasty secondary to failure of her rotator cuff repair within 3 months of surgery, leaving 39 patients eligible for analysis at the final follow-up. Figure 3 provides a CONSORT (Consolidated Standards of Reporting Trials) flow diagram demonstrating the patients included in the final analysis. In total, 33 patients (84.6%) presented at the final follow-up for physical examination and patient-reported outcomes at 5.2 ± 0.8 months (range, 4-7 months). The mean age of patients in the lidocaine group was 54.8 ± 11.1 years, whereas the mean age of patients in the control group was 56.6 ± 6.9 years (P = .5). The mean anterior-posterior and medial-lateral sizes of the rotator cuff tear in the lidocaine group was 19.1 ± 7.4 × 17.5 ± 7.5 mm, whereas the respective mean size of the rotator cuff tear in the control group was 23.8 ± 11.7 × 19.4 ± 8.0 mm, which was not statistically different in either direction (P = .1 and P = .5, respectively). Baseline patient characteristics and concomitant procedures for each group were not significantly different (P > .05) (Table 1).

CONSORT (Consolidated Standards of Reporting Trials) flow diagram illustrating the inclusion of patients for final analysis.
Patient Characteristicsa

a BMI, body mass index; SLAP, superior labral tear from anterior to posterior.
Range of motion, strength, and the total Constant-Murley score significantly improved after a subacromial lidocaine injection (P < .05), whereas patients in the control group demonstrated a statistically insignificant improvement in all parameters after a sham injection (P > .05) (Table 2). Patients in the lidocaine and control groups demonstrated a 15.3% and 9.1% increase in the Constant-Murley score after injection (P < .001 and P = .5, respectively); however, there was no difference in the net improvement between both groups (P = .3). Furthermore, there was no difference in strength or range of motion between both groups after the injection (P > .05).
Physical Examination Findings Before/After Injection and at 6 Months Postoperatively a
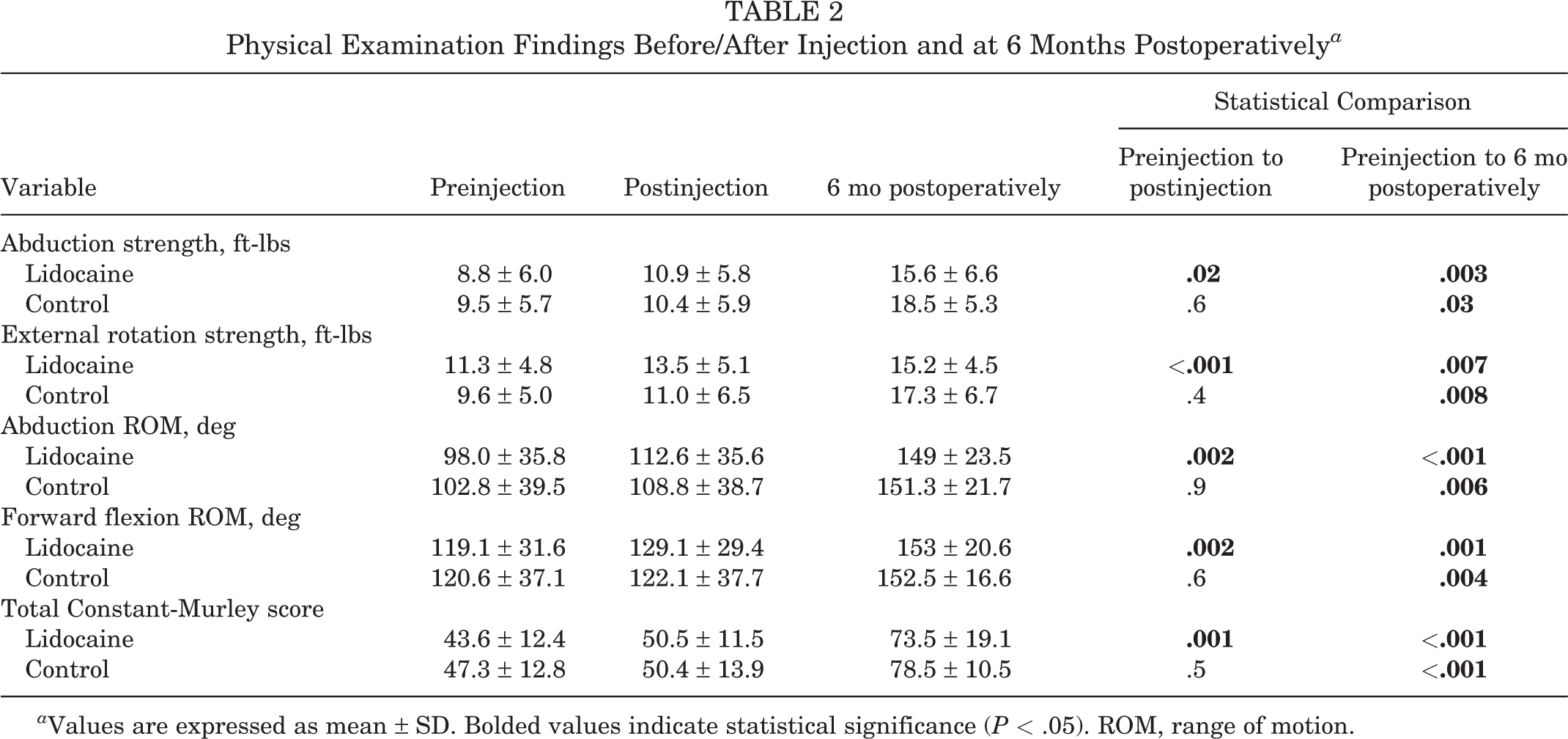
a Values are expressed as mean ± SD. Bolded values indicate statistical significance (P < .05). ROM, range of motion.
Before surgery, the mean VAS-Pain for the lidocaine and control groups was 50.8 ± 26.2 and 58.7 ± 25.9, respectively (P = .7). Although there was no difference in VAS-Pain scores at the final follow-up between the lidocaine and control groups (9.9 ± 13.9 and 13.1 ± 15.7, respectively; P = .6), both groups demonstrated an improvement in overall pain scores from the preinjection state (P < .001 and P = .001, respectively). Furthermore, the Constant-Murley scores significantly increased at final follow-up compared with those at preinjection assessment for the lidocaine and control groups (P < .001 and P < .001, respectively) (Table 2). At final follow-up, there was no difference in abduction strength, external rotation strength, abduction or forward flexion range of motion, and Constant-Murley score between both groups (P > .05).
On multivariate binomial regression, age at time of surgery (P = .99), BMI (P = .8), sex (P = .3), VAS-Pain (P = .3), size of rotator cuff tear (P = .4), and lidocaine injection (P = .2) were not predictors of change in Constant-Murley score after injection.
Discussion
The results of this investigation demonstrate that a subacromial lidocaine injection significantly improved patients’ comfort, which resulted in increased range of motion, strength, and Constant-Murley score in the setting of full-thickness rotator cuff tears. Patients who received the sham injection as a control displayed an increase in all these metrics, but none reached statistical significance. At the time of final follow-up, both groups demonstrated statistically significant improvement in range of motion, strength, and Constant-Murley scores compared with their preinjection state. However, there was no difference in these outcomes between the groups 6 months postoperatively. It is important to note that the improvements in motion and strength after injection were modest (ie, 10º increase in flexion); however, the improvements after surgery were of a much greater magnitude (ie, 30º increase in flexion). Furthermore, the improvement in Constant-Murley score at final follow-up in both groups exceeded the minimal clinically important difference of 4.6. 8 These results illustrate that pain and self-induced inhibition may play significant roles in functional limitation and the clinical evaluation of patients with full-thickness rotator cuff tears independent of the mechanical impact of the tear itself, which may ultimately obscure clinical evaluation.
Full-thickness rotator cuff injuries are associated with severe pain, loss of active motion, and severe disability. 1,5 Rotator cuff tear severity may be assessed radiographically by the size of the tear, number of involved tendons, and degree of retraction and atrophy. BMI and medical comorbidity, as well as preoperative patient mental health, have previously been shown to be associated with subjective patient metrics. 23,27,28 However, Dunn et al 10 and Wylie et al 28 demonstrated that the size of the tendon tear does not correlate with pain or functional status as assessed through patient-reported outcome measures. The relationship between pain perception and the progression of rotator cuff tear is variable, as patients can remain asymptomatic or develop increasing levels of pain because of tear progression. 10,30 Therefore, clinical examination can produce misleading results as it can be influenced by pain, concomitant pathology, or patient adaptability to the present pathology. The presence of pain may be considered a pertinent positive in clinically assessing rotator cuff tears. However, unless pain is controlled, range of motion and strength measurements cannot reliably assess for the presence and severity of rotator cuff tears. Functional deficit from a rotator cuff tear is a multifactorial malady in which pain is a contributing factor that may obscure the clinical impression of tendon integrity. Therefore, it may be efficacious for physicians to administer a subacromial injection of lidocaine for assessing patients with suspected rotator cuff pathology. For example, the continued presence of weakness and decreased range of motion after a subacromial injection may be more indicative of a full-thickness tear. It is important to note that rotator cuff tears can present asymptomatically, particularly in elderly patients. 15,29 Although this population of patients may be at risk for developing pain, they may not exhibit limitations in strength or range of motion. 29
Patients in the control group of this investigation demonstrated a modest yet nonsignificant improvement in objective measurements after a placebo injection. This increase was sufficient enough to prevent the experimental group from demonstrating a statistically significant change in objective measurements in comparison with the control group. The act of performing an injection may cause a placebo effect, leading to improved outcomes. 3,19 It is possible that patients may exhibit improvement owing to a “learning” effect because of repeated testing. In this investigation, patients underwent physical assessment only before and after a subacromial injection. The learning effect is likely minimal; however, it remains a plausible contributor to postinjection improvements in both groups. The control group allows for a true evaluation of the investigated injection; however, the perception of an anesthetic in this cohort may have enabled patients to improve functionality. These results further suggest that functional deficit in rotator cuff deficiency is not exclusively because of the integrity of the rotator cuff tendons, 1 but also because of patient inhibition as a protective measure or mechanism for pain avoidance. Nevertheless, statistically significant improvements in strength and range of motion were observed at final follow-up in comparison with the postinjection state in both groups. This suggests that the majority of strength deficit remains attributable to reduced functional tendon integrity, a significant finding in informing management of patients who experience profound weakness on physical examination. Nonetheless, the results of the control group were nonsignificant and may be attributable to chance. Despite a power analysis demonstrating adequate power, the sample size in this investigation was relatively small (n = 20). Thus, this investigation may be repeated with a larger sample size to assess the effect of sham injections on objective clinical measures in patients with full-thickness rotator cuff tears.
As patient-centered models of care have become more prevalent, patient-reported outcome measures can be developed to clinically guide treatment decisions, determine prognosis, and evaluate response to treatment. 24 The Constant-Murley score is one of the most frequently reported patient outcome measures for rotator cuff tears. 25 However, the Constant-Murley score does not exhibit the responsiveness to changes in subjective patient measures, as 65% of the score is embedded in objective measures. 7 Other subjective outcome measures, such as the American Shoulder and Elbow Surgeon (ASES) score and Simple Shoulder Test (SST), are more significantly weighted in pain assessment. 12,18 In patients with rotator cuff pathology, pain is the primary factor in determining patient outcomes 25 ; thus, the additional range of motion and strength testing required by the Constant-Murley score may be unnecessary and may place an added burden on physicians treating patients in this cohort. The inability of patients to complete the objective portion of the Constant-Murley assessment remotely or without the assistance of a clinician further inhibits its utility. Thus, the ASES and SST assessments may be more effective longitudinal measures of patient function in patients with rotator cuff pathology. Nonetheless, the results of this investigation suggest that the Constant-Murley score is responsive enough to detect changes in objective function after elimination of pain or patient-induced inhibition.
It is imperative that the results of this investigation be assessed within the context of its limitations. The control group would have been strengthened if it included a 10-mL saline injection to account for subacromial expansion; however, this caused the initial patients significant discomfort, which could have hampered accurate data collection. This investigation was single-blinded, and evaluators were instructed to remain objective; however, the results would have been strengthened if it were double-blinded to reduce the potential bias of the clinical evaluators. The method of inserting a needle into the subacromial space without injecting any material has not been previously validated and is subject to variation in the data. Objective clinical measurements from the contralateral shoulder could have been used as a comparison with the study shoulder; however, these metrics were not collected. Abduction strength was collected in accordance with the Constant-Murley assessment with the arm in abduction. However, the supraspinatus muscle could have been better isolated with the “empty can” test 14 or champagne toast, 4 which may enable our results to be more accurate. Improvements in Constant-Murley score after injection were attributable to improvements in strength and range of motion. Baseline pain during activities of daily living was assessed and would be unchanged in the setting of this investigation. The results of this investigation would be furthered strengthened if pain after each administration of the Constant-Murley evaluation was collected. It is important to note that there are no direct data to suggest that lidocaine improved pain after injection. However, since lidocaine is an anesthetic, it is reasonable to state that lidocaine reduced pain after injection, which allowed patients to exhibit improvements in range of motion and strength. It is important to note that postinjection VAS-Pain scores were not obtained. An a priori power analysis based on the results of previous investigations determined the required sample size to demonstrate a relevant sample size. 11,20 However, the sample size of this investigation could have been larger. If sample sizes are not adequate, inaccurate statistical significance may be elucidated.
Conclusion
After subacromial lidocaine injections, patients exhibited modest but significant improvement in range of motion, strength, and the Constant-Murley score. Pain may limit the range of motion and strength in patients with full-thickness rotator cuff tears independent of the mechanical impact of tear itself.
Footnotes
Final revision submitted September 6, 2019; accepted September 28, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.F. has received research support from Arthrex and Stryker; educational support from Medwest, Smith & Nephew, and Ossur; consulting fees from Arthrex, DJO, Smith & Nephew, Ossur, Sonoma Orthopedics, and Stryker; speaking fees from Arthrex; honoraria from Arthrosurface; and royalties from Elsevier and Arthrex; and has stock options in Jace Medical. N.N.V. has received research support from Arthrex, Arthrosurface, DJO, Ossur, Athletico, ConMed Linvatec, Miomed, and Mitek; consulting fees from Minivasive, Orthospace, Smith & Nephew, Medacta, and Arthrex; speaking fees from Pacira and Arthrex; and royalties from Arthroscopy, Smith & Nephew, and Vindico Medical–Orthopaedics Hyperguide; and has stock options in Cymedica, Minivasive, and Omeros. A.A.R. has received consulting fees and royalties from Arthrex. B.J.C. has received research support from Aesculap/B.Braun, Arthrex, Geistlich, Sanofi-Aventis, and Zimmer; educational support from Medwest; consulting fees from Arthrex, Genzyme, Pacira Pharmaceuticals, Anika Therapeutics, Vericel, Zimmer Biomet, Bioventus, Geistlich Pharma, Smith & Nephew, Acumed, and Flexion Therapeutics; speaking fees from Arthrex, Carticept Medical, Pacira Pharmaceuticals, and Lifenet Health; royalties from Arthrex, DJO, Elsevier, and Operative Techniques in Sports Medicine; honoraria from Vericel; hospitality payments from Lifenet Health, Geistlich Pharma, and GE Healthcare; and has stock options in Aqua Boom, Biometrix, Giteliscope, Ossio, and Regentis. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center Institutional Review Board (FWA No. 00000482).