
Abstract
Background:
Arthroscopic rotator cuff repair (ARCR) is among the most commonly performed orthopaedic procedures. Several factors—including age, sex, and tear severity—have been identified as predictors for outcome after repair. The influence of the tear etiology on functional and structural outcome remains controversial.
Purpose:
To investigate the influence of tear etiology (degenerative vs traumatic) on functional and structural outcomes in patients with supraspinatus tendon tears.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Patients undergoing ARCR from 19 centers were prospectively enrolled between June 2020 and November 2021. Full-thickness, nonmassive tears involving the supraspinatus tendon were included. Tears were classified as degenerative (chronic shoulder pain, no history of trauma) or traumatic (acute, traumatic onset, no previous shoulder pain). Range of motion, strength, the Subjective Shoulder Value, the Oxford Shoulder Score (OSS), and the Constant-Murley Score (CMS) were assessed before (baseline) and 6 and 12 months after ARCR. The Subjective Shoulder Value and the OSS were also determined at the 24-month follow-up. Repair integrity after 12 months was documented, as well as additional surgeries up to the 24-month follow-up. Tear groups were compared using mixed models adjusted for potential confounding effects.
Results:
From a cohort of 973 consecutive patients, 421 patients (degenerative tear, n = 230; traumatic tear, n = 191) met the inclusion criteria. The traumatic tear group had lower mean baseline OSS and CMS scores but significantly greater score changes 12 months after ARCR (OSS, 18 [SD, 8]; CMS, 34 [SD,18] vs degenerative: OSS, 15 [SD, 8]; CMS, 22 [SD, 15]) (P < .001) and significantly higher 12-month overall scores (OSS, 44 [SD, 5]; CMS, 79 [SD, 9] vs degenerative: OSS, 42 [SD, 7]; CMS, 76 [SD, 12]) (P≤ .006). At the 24-month follow-up, neither the OSS (degenerative, 44 [SD, 6]; traumatic, 45 [SD, 6]; P = .346) nor the rates of repair failure (degenerative, 14 [6.1%]; traumatic 12 [6.3%]; P = .934) and additional surgeries (7 [3%]; 7 [3.7%]; P = .723) differed between groups.
Conclusion:
Patients with degenerative and traumatic full-thickness supraspinatus tendon tears who had ARCR show satisfactory short-term functional results. Although patients with traumatic tears have lower baseline functional scores, they rehabilitate over time and show comparable clinical results 1 year after ARCR. Similarly, degenerative and traumatic rotator cuff tears show comparable structural outcomes, which suggests that degenerated tendons retain healing potential.
Keywords
Arthroscopic rotator cuff repair (ARCR) is the most frequently performed shoulder surgery in patients aged 50 to 70 years.22,23 The incidence of degenerative rotator cuff tears is clearly age-related, but traumatic events may cause cuff tears in all adult age groups.12,39,40 The distinction between degenerative and traumatic tear etiology is important because the success of tendon repair may be limited by the restricted regenerative properties of degenerated tendons.2,13,28 Nonetheless, these biological observations have limited translation to clinical healing, and the literature on the effect of tear etiology on structural and functional outcomes after ARCR is scarce.1,8,19,25,31,36 Previous studies comparing degenerative versus traumatic tears also lack the necessary adjustments in their analyses to consider tear severity, even though it is one of the most relevant predictors of structural outcome after ARCR.24,26,27 Thus, they are prone to selection bias. By restricting analyses to more homogeneous patient groups, causal associations can be assessed more accurately. Therefore, this study aimed to compare functional and radiologic outcomes of comparable patient groups with isolated degenerative or traumatic full-thickness and nonmassive tears involving the supraspinatus tendon. We hypothesized that patients with traumatic tears would have better functional and structural outcomes over those with degenerative rotator cuff tears and, therefore, would derive greater benefits from ARCR.
Methods
Patient Cohort and Allocation to Degenerative Versus Traumatic Tear Groups
The patient sample was drawn from a prospective multicenter cohort implemented to assess the safety and effectiveness of ARCR, as described elsewhere. 4
Briefly, after ethics approval was obtained, a cohort of 973 patients who had primary ARCR was prospectively enrolled at 19 orthopaedic centers, 18 Swiss and 1 German, between June 2020 and November 2021, and observed for 24 months postoperatively. 4 Procedures were performed all-arthroscopically, with various surgical techniques used in both groups, including single row, conventional double row, or transosseous equivalent (with and without knots) (Table 1). 29
Distribution of Repair Methods Used in the Degenerative and Traumatic Groups a

Data are presented as n (%). SSP, supraspinatus; StdDiff, standardized difference; TOE, transosseous equivalent.
Likewise, postoperative rehabilitation protocols varied among treating surgeons and patients in both groups. Functional and structural outcomes, patient-reported outcome measures, and adverse events were recorded at the 6-week, 6-, 12-, and 24-month follow-ups. Patients with full-thickness rotator cuff tears involving the supraspinatus tendon were selected from this specific cohort. Massive tears—full-thickness tear of ≥2 tendons as defined by Gerber et al 18 —and partial tears were excluded to avoid any imbalances favoring the causes of traumatic tears (64%) and degenerative tears (80%), respectively.
Patients were allocated to 1 of the 2 groups based on the patient’s medical history and the surgeons’ assessment of the cause of the tear. Patients with chronic (ie, symptomatic for >3 months) shoulder pain with no history of trauma or previous shoulder surgery were included in the degenerative group. Patients who recalled an acute onset of symptoms after a traumatic event, had no history of previous shoulder surgery or complaints, and underwent ARCR within 6 months after the traumatic event were allocated to the traumatic group.
Preoperative Baseline Characteristics
Age at surgery, sex, dominance of the affected shoulder, smoking status, body mass index, diabetes status, the American Society of Anesthesiologists physical status classification (I to IV), previous nonoperative interventions (physical therapy or steroid infiltrations), and the number of steroid infiltrations were recorded before surgery. In addition, the following were assessed by physical examination and patient questionnaire: (1) range of motion—that is, active shoulder flexion, abduction, external and internal rotation; (2) strength at 90° of abduction—measured with a handheld dynamometer; mean strength values of 3 consecutive measurements recorded for each patient; (3) pain levels measured based on the numeric rating scale (NRS), ranging from 0 (no pain) to 10 (highest possible pain); (4) the Subjective Shoulder Value (SSV); (5) the Constant-Murley Score (CMS); (6) the Oxford Shoulder Score (OSS); and (7) the EQ5D5L utility index. Osteoarthritis grade (Samilson Prieto classification 34 ), tear pattern adapted from the classification of Collin et al, 10 supraspinatus tendon atrophy by the areal percentage, 38 fatty infiltration of cuff muscles (magnetic resonance imaging [MRI]–adapted Goutallier classification 15 ), and tendon retraction (Patte classification 30 ) were recorded on preoperative baseline MRI and radiographs. Intraoperative findings were also recorded—such as superior labrum anterior to posterior lesions and humeral or glenoid cartilage lesions.
Outcome Parameters
Clinical outcome parameters—including active range of motion, strength at 90° of abduction, and CMS—were assessed 6 months and 1 year after surgery. All consultations with clinical examination were performed in a face-to-face study visit. Overall patient satisfaction, OSS, SSV, pain, and the EQ5D5L utility index were documented via online or paper-based patient questionnaires at the 6-, 12-, and 24-month follow-ups, or if we did not get a response, via phone calls. Adverse events were documented according to a standardized core set 5 on separate adverse event forms throughout the 2-year postoperative period and reviewed for plausibility by 2 fellowship-trained orthopaedic surgeons (C.B. and S.A.M.). Adverse events included symptomatic recurrent rotator cuff defects diagnosed by ultrasound or MRI that led to a change in treatment. Patients also underwent a routine ultrasound check of their operated shoulder 1 year after surgery to document asymptomatic recurrent defects of the repaired tendons. A Delphi process with all ultrasound operators was conducted before the follow-up examinations, and training videos were provided to improve comparability among the ultrasound assessments. The ultrasound operators were radiologists with musculoskeletal specialty training (n = 21), experienced rheumatologists, or orthopaedic surgeons (n = 8). Of all sonographers, 72% had >10 years of work experience. Repair integrity was documented at 12 months via a composite outcome parameter combining the occurrence of a symptomatic rotator cuff adverse event ≤12 months after surgery and the diagnosis of a complete recurrent defect of any repaired tendon by ultrasound. The occurrence of a secondary surgery for any reason was also documented. Finally, patients were asked how satisfied they were with the overall result of their shoulder treatment—with the NRS, which ranges from 0 (not at all satisfied) to 10 (fully satisfied)—and they were asked if they would opt for ARCR again with this knowledge of satisfaction level (no; I do not know; yes).
Data Management and Statistical Analysis
Study data were managed using the REDCap Electronic Data Capture system 20 and exported for statistical analysis using Intercooled Stata Version 17 (StataCorp LP). Baseline patient parameters were tabulated separately per group using standard descriptive statistics and compared using clinical judgment and standardized differences (StdDiffs), 6 where values closest to 0.10 indicate stronger group similarity.
We compared both groups using generalized linear mixed models to account for repeated measurements when outcome data were available at each follow-up time point, as applicable. All models were adjusted for sex and the number of preoperative steroid infiltrations. Regression coefficients (beta) were estimated along with their 95% CIs and the results of the adjusted t test. Dichotomous outcomes were tabulated by the study group with absolute and relative frequencies (risk) and compared between groups using adjusted logistic regression. Relative risks (RRs) were calculated along with their 95% CIs. All analyses were explorative, with a significance level set at .05.
The sample size was not a priori estimated for this analysis, as all eligible patients were selected from the ARCR_Pred cohort. Nevertheless, considering a minimal important difference of 5 points on the CMS 11 and the observed variability of this score in our cohort (SD, 11), this analysis had a power of 99% to identify such a minimal important difference at the 12-month follow-up, with a significance level set at 5%.
Results
Patient Group Baseline Characteristics
From the ARCR_Pred cohort of 973 patients, 421 patients met the inclusion criteria; degenerative rotator cuff tears were diagnosed in 230 patients (55%), and 191 patients (45%) had tears of traumatic origin (Figure 1). Follow-up rates were 90% (377/421) for the study visits at the 12-month follow-up and 95% (400/421) and 84% (223/267) for the patient-reported questionnaires at the 12- and 24-month follow-ups, respectively (Table 2).
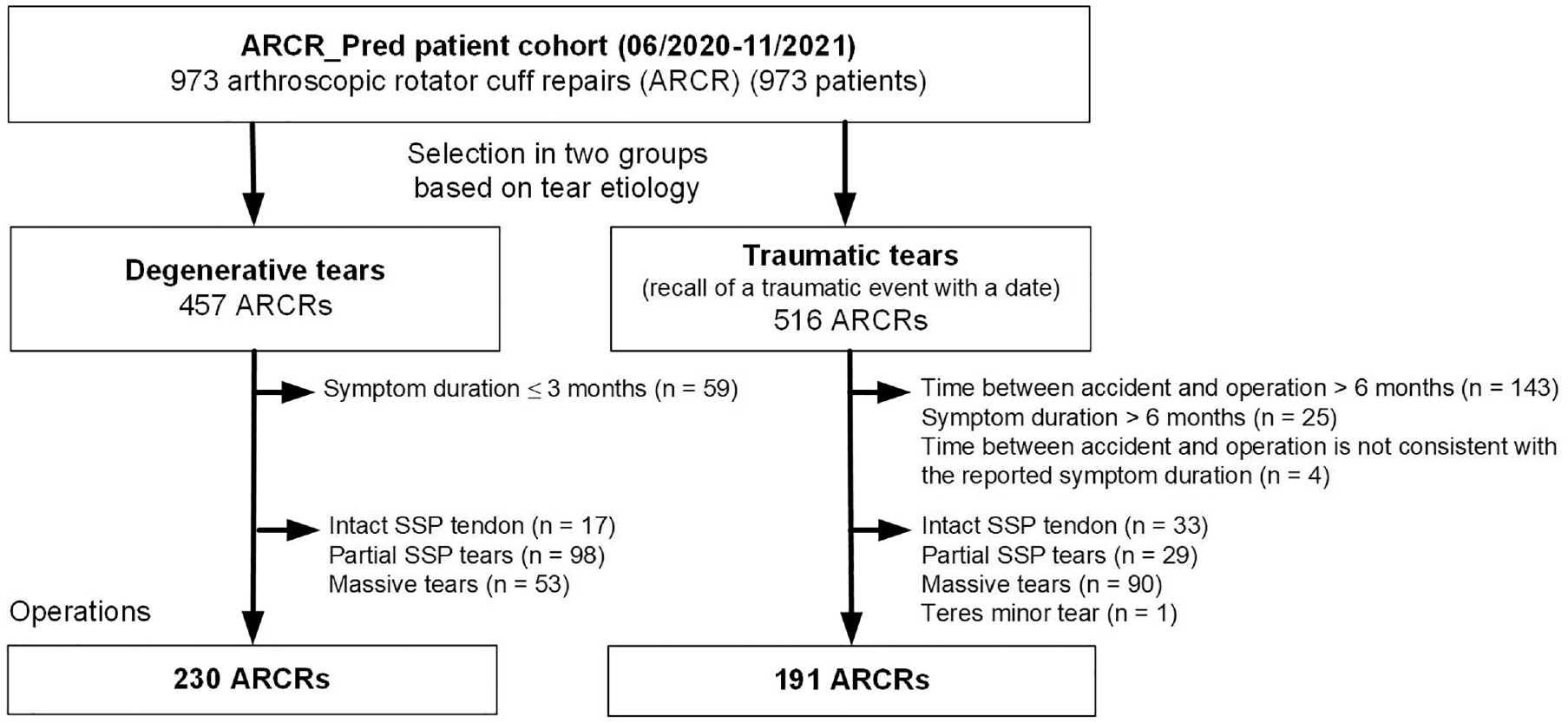
Patient selection flowchart highlighting follow-up rates at 6, 12, and 24 months after ARCR. ARCR, arthroscopic rotator cuff repair; SSP, supraspinatus.
Baseline Descriptive Data and Comparison Between Degenerative and Traumatic Groups a
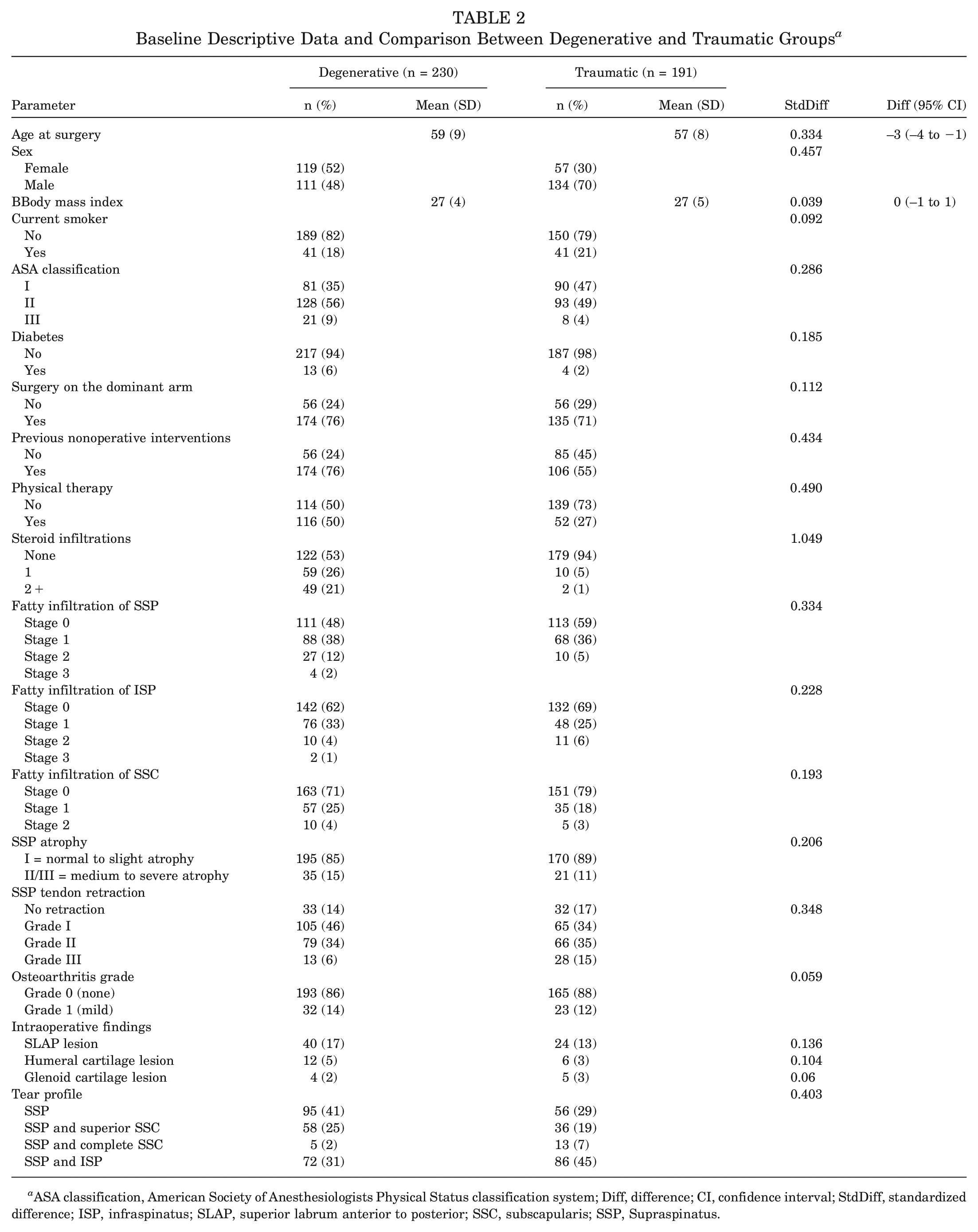
ASA classification, American Society of Anesthesiologists Physical Status classification system; Diff, difference; CI, confidence interval; StdDiff, standardized difference; ISP, infraspinatus; SLAP, superior labrum anterior to posterior; SSC, subscapularis; SSP, Supraspinatus.
The difference in age distribution between groups was negligible (StdDiff, 0.334), and there was a higher percentage of women in the degenerative compared with the traumatic group (StdDiff, 0.457) (Table 2). A higher proportion of patients with degenerative tears (76%) underwent nonoperative interventions before surgery compared with the traumatic group (55%), which was associated with a higher number of steroid infiltrations administered to the degenerative group (StdDiff, 1.049).
Functional Outcome
A detailed overview of the range of motion data per tear group is shown in Appendix Table A1 (available in the online version of this article). Patients in the traumatic group had lower mean baseline values for flexion (109° vs 137°), abduction (96° vs 129°), and internal rotation (34° vs 40°) compared with those with degenerative tears. Even though the absolute values for flexion, abduction, and external rotation at 6 and 12 months after ARCR were similar between the groups, there were significant changes in the mean values of flexion (degenerative [n = 19] vs traumatic [n = 48]), abduction (degenerative [n = 25] vs traumatic [n = 59], and internal rotation (degenerative [n = 6] vs traumatic [n = 14]) from baseline to the 12-month follow-up (P≤ .007). In addition, patients with traumatic tears achieved higher overall internal rotation at the 12-month follow-up over the patients with degenerative tears (49 vs 46, respectively; beta, 6.68 [95% CI, 1.17-12.2]; P = .018) (Figure 2).
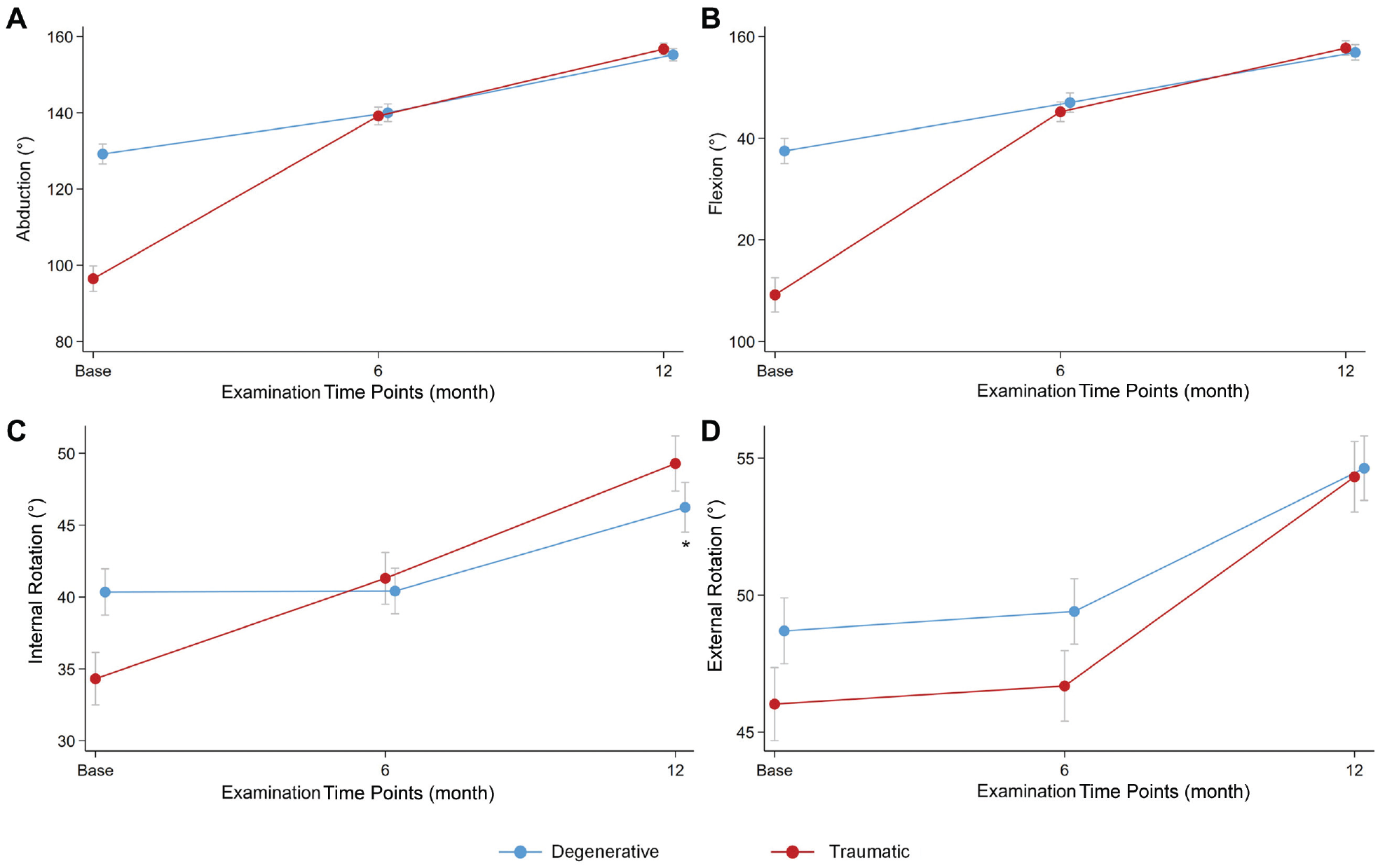
Comparison of (A) abduction, (B) flexion, (C) internal rotation at 90° of abduction, and (D) external rotation at 0° of abduction at the baseline, 6, and 12 months of follow-up for patients with degenerative and traumatic tears. Means and SEMs are presented, where * indicates statistically significant differences between groups.
The mean baseline CMS scores in the traumatic group were lower (44 vs 54). Yet, the score changes by 6 and 12 months after ARCR were significantly higher, with higher overall scores at the 12-month follow-up, when compared with the degenerative group (P≤ .006) (Figure 3 and see Appendix Table A2, available online). Similarly, the traumatic group showed greater improvements in strength at 90° of abduction from baseline to both the 6- and 12-month follow-ups (P < .001); nonetheless, no significant difference was observed in the 12-month strength values between groups (P = .16). For patients with traumatic tears, the OSS was significantly higher at the 6 and 12 month follow-ups (P≤ .032); nevertheless, this score did not significantly differ with that of the degenerative group by the 24 months follow-up (P = .346).
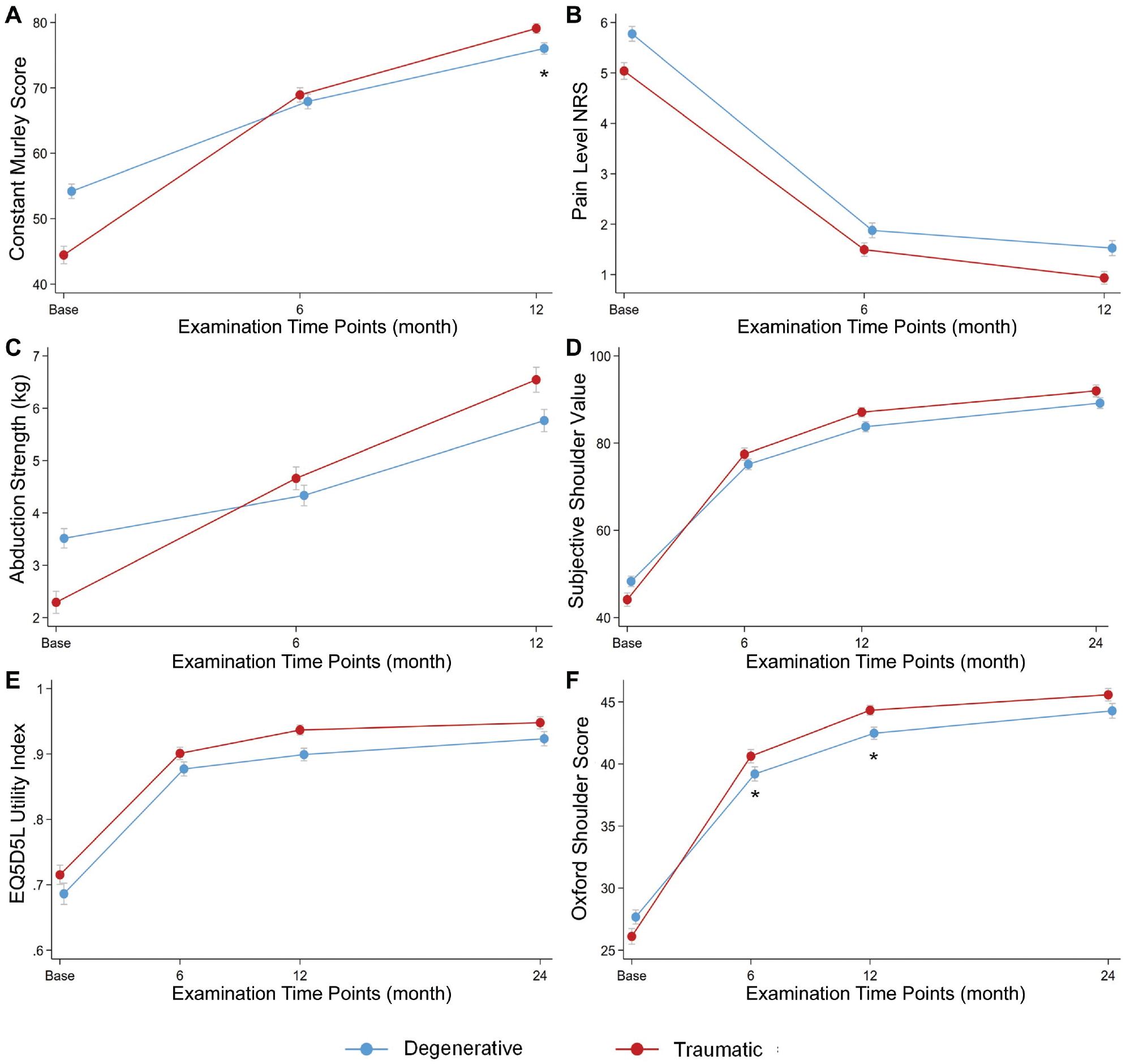
(A) The Constant-Murley Score, (B) the pain level on the Numeric Rating Scale (NRS), (C) abduction strength at 90° of abduction, (D) the Subjective Shoulder Value, (E) the EQ5D5L utility index, and (F) the Oxford Shoulder Score for the degenerative and traumatic groups at 6-, 12-, and 24-month follow-ups. Means and SEMs are presented, where * indicates statistically significant differences.
Structural Outcome, Secondary Surgeries, and Adverse Events
Ultrasound examinations at the 1-year follow-up revealed symptomatic recurrent defects in 14 of 230 patients (6.1%) with degenerative tears and 12 of 191 patients (6.3%) with traumatic tears (adjusted RR, 1.4 [95% CI, 0.56-3.5]; P = .934). No significant difference was found regarding the proportions of secondary surgeries for the degenerative (7/230 [3%]) and traumatic (7/191 [3.7%]) groups; 7 additional surgeries were completed in each group (adjusted RR, 0.94 [95% CI, 0.30-2.9]; P = .723). Reasons for these interventions included removal of a displaced anchor (degenerative, n = 2; traumatic, n = 1), intra-articular lavage and wound irrigation due to infection (traumatic, n = 1), additional biceps tenodesis for persistent biceps pain (degenerative, n = 1; traumatic, n = 1), or ruptured tendon and revision rotator cuff reconstruction with or without patch augmentation (degenerative, n = 4; traumatic, n = 4). Similarly, no significant difference was found between groups for any recorded adverse event (Table 3).
Distribution of Local Postoperative Adverse Event Categories and Comparison Between Degenerative and Traumatic Groups a
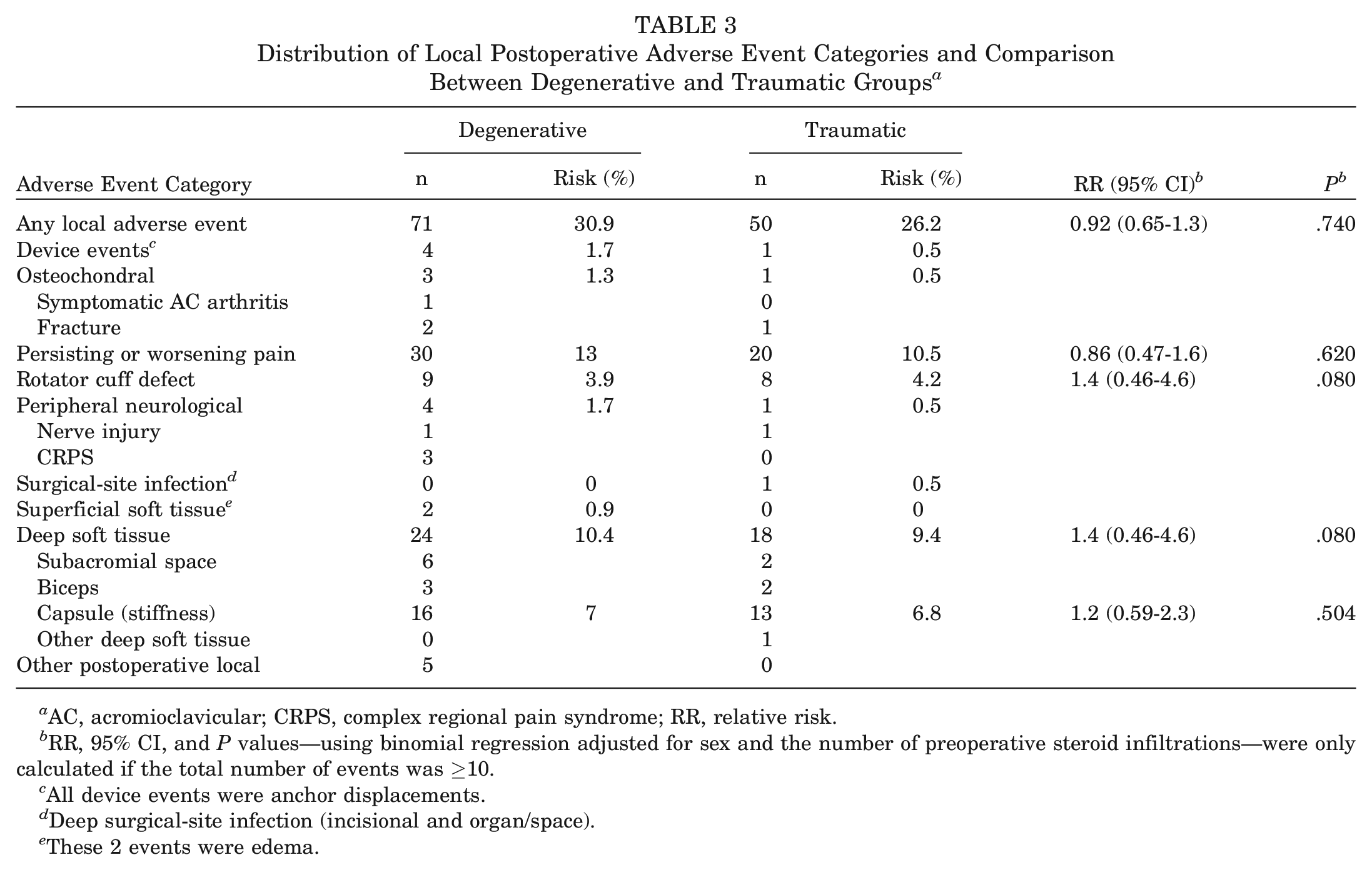
AC, acromioclavicular; CRPS, complex regional pain syndrome; RR, relative risk.
RR, 95% CI, and P values—using binomial regression adjusted for sex and the number of preoperative steroid infiltrations—were only calculated if the total number of events was ≥10.
All device events were anchor displacements.
Deep surgical-site infection (incisional and organ/space).
These 2 events were edema.
Quality of Life and Level of Satisfaction
The mean EQ5DL utility indices were similar for the degenerative and traumatic groups at 12 and 24 months after ARCR (P = .215) (see Appendix Table A3, available online).
The mean overall levels of patient satisfaction at 12 months were 8.8 (SD, 1.8) and 9.1 (SD, 1.4) for the degenerative and traumatic groups, respectively (P = .083). By 24 months, the respective mean satisfaction levels were 9.2 (SD, 1.7) and 9.3 (SD, 1.6) (P = .595). At 12 months, most patients in the degenerative (84%) and traumatic (90%) groups stated that they would undergo the surgery again (adjusted P = .185). By the final follow-up, the proportions of patients with degenerative (92%) and traumatic tears (91%) opting for ARCR again remained high (adjusted P = .777).
Discussion
In this analysis, we compared 2 homogeneous groups of patients with full-thickness supraspinatus tendon tears caused by either degenerative changes or traumatic events. Even though both types of rotator cuff tears can cause pain and disability, our findings suggest that their patterns of baseline characteristics and postoperative recovery of functional outcomes differ. Patients with traumatic tears had significantly lower subjective as well as objective shoulder function scores at baseline, yet with significantly greater recovery at the 1-year follow-up. One year after ARCR, patients with traumatic tears showed significantly better CMS scores; however, with minimal clinically important differences of 5 to 10 reported in the literature, 11 this difference may not be clinically relevant. Moreover, patient-reported outcomes—such as OSS, SSV, EQ5D5L, and overall patient satisfaction—were no longer significantly different by the 24-month follow-up, indicating that the tear etiology no longer affects outcome after this time.
With our 2 sizable and comparable patient groups, this prospective study could address the question of whether the cause of tear influences functional and structural outcomes after ARCR. Previous studies investigating the difference between degenerative and traumatic tear repair used mixed definitions for the latter, included heterogeneous tear patterns, and were not adjusted for additional factors affecting the outcome of ARCR.
Despite its clinical relevance, tear etiology is not uniformly defined, as indicated by a more recent systematic literature review addressing the term definitions of “acute” and “traumatic.” For example, only 24 of 46 studies overall on traumatic rotator cuff tears reported that the injuries occurred in previously asymptomatic patients. 32 It is important, however, to distinguish purely traumatic tears from acute on chronic tears because the latter occurs in predegenerated tendons with potentially reduced healing capacity.2,13,28 Therefore, the term traumatic, as implemented in our study and as suggested by Pogorzelski et al, 32 should be restricted to patients with an acute onset of symptoms after a shoulder trauma and who have had no previous shoulder complaints.
The restriction of full-thickness tears involving the supraspinatus tendon in our study is of great importance. Within the initial cohort of 973 patients, a substantial proportion of partial tears were degenerative (80%), and a significant proportion of massive tears were of traumatic origin (64%). The registry study of Kukkonen et al 25 included 306 patients and reported a higher rate of larger tear sizes in patients with traumatic rotator cuff tears, which is in line with our findings that massive tears are more likely to derive from trauma. Therefore, including massive and partial tears would inevitably introduce selection bias.
Because of previously unaddressed methodological issues, the literature comparing degenerative and traumatic tears has been inconsistent. Tan et al 36 investigated the influence of the cause of tear on outcome in a cohort of 1300 patients at a single center. They found a more restricted range of motion pre- and postoperatively in the traumatic group but no difference in retear rates between groups. Besides the retrospective design and the short follow-up duration of 6 months, a major limitation was the definition of traumatic tears. Patients were considered to have sustained a traumatic tear if a trauma event was recalled. No information was provided regarding previous shoulder complaints. Furthermore, patients in the traumatic group were included until 24 months after trauma. This duration alone can lead to tendon degeneration in the event of a persisting tear. Braune et al 8 reported significantly higher CMS for patients with traumatic rotator cuff tears (94) when compared with those with nontraumatic, degenerative tears (75) at the mean post-ARCR follow-ups of 47 and 41 months, respectively. Besides the small sample size of 46 patients, the traumatic group was younger, with a mean age of 34 years versus 54 years in the degenerative group. In contrast, our patient groups were very comparable with respect to the mean age. Kukkonen et al 25 reported significantly higher CMS in the degenerative group when compared to the traumatic group at baseline (52 vs 46) and 12 months postoperatively (77 vs 73), and both groups had comparable patient ages. Abechain et al 1 reported a lack of significant difference in functional outcomes between their degenerative and traumatic groups that shared similar mean ages of 59.9 and 59.0 years, respectively; the authors applied the University of California, Los Angeles, Shoulder Score tool over the CMS and the study was limited by a small total sample size of 87 patients. Godshaw et al 19 demonstrated higher preoperative functional deficits in the traumatic group but greater improvements in range of motion, strength, and shoulder function compared with their degenerative group, which mirrors our findings. However, it is a single-center study with a smaller sample size (73 traumatic versus 148 atraumatic tears).
It is generally believed that degenerative rotator cuff tears have poorer healing capacity over traumatic rotator cuff tears after repair, although the evidence to prove this theory is meager.1,19,25,31,36 Tan et al 36 assessed postoperative tendon integrity in correlation with tear size and did not find any significant differences in retear rates between the traumatic and degenerative groups for each tear size, but did report higher retear rates for larger tears. Similarly, Raman et al 33 found insufficient evidence for the influence of the cause of tear on postoperative tendon integrity in their systematic review summarizing 490 patients from 3 studies. In line with these published findings, we could not show any significant differences in retear or revision surgery rates between the 2 groups, which indicates that healing potential is preserved, even in the case of degenerated tendons.
The retear rates for our patient groups were surprisingly low at around 6% when compared with the reported rates of 5% to 92%.3,7,16,17,21,35,37 Repair failure may be considered a multifactorial issue because of the biological properties of the tendon and biomechanical factors, and expected healing after ARCR correlates with tear size.26,27,33 The retear rate of isolated full-thickness supraspinatus repairs was previously reported to be 13%. 14 Moreover, the relatively younger mean age of our patient groups may also play a role in supporting the healing potential of affected tendons.
Strengths and Limitations
We acknowledge the following limitations of our study. Our classification of rotator cuff tears as traumatic was based on surgeons’ judgment, the history of trauma, and the absence of previous symptoms. Neither preoperative MRI findings nor the mechanism of injury were recognized and documented for these patients at the baseline patient assessments and cannot be accurately assessed at a later stage. Histopathologic differences between degenerative and traumatic tendons were also not evaluated because implementation was not clinically feasible. Thus, we cannot completely rule out that some primary tendon degeneration may be evident in patients classified with traumatic tears.
Another limitation is that repair integrity was measured by ultrasound in a multicenter setting, which may be associated with examiner-dependent variations in accuracy. In addition, patient recruitment was conducted during the COVID-19 pandemic. Thus, we cannot rule out that some enrolled patients experienced a delay in time to the surgical theater and had increased use of steroid infiltrations when compared with similar patient cohorts.
As a strength of our work, the follow-up time of 2 years adequately reflects functional results after ARCR, as it extends beyond the 1-year period in which functional recovery is known to improve after surgery and is followed by stabilization. 9
Conclusion
Patients with degenerative and traumatic full-thickness tears involving the supraspinatus tendon both show satisfactory functional results at the short-term follow-up after ARCR. Although patients with traumatic tears have lower baseline functional scores, such as the CMS, they rehabilitate over time and demonstrate significantly greater score changes up to the 6- and 12 -month follow-ups. At 12 to 24 months after ARCR, clinical differences in functional and patient-reported outcomes are no longer evident. Likewise, structural outcomes are comparable between degenerative and traumatic rotator cuff tears, which indicates that degenerated tendons retain healing potential.
Authors
Cornelia Baum, MD (Department of Orthopaedic and Trauma Surgery, University Hospital Basel, Basel, Switzerland); Laurent Audigé, PhD (Surgical Outcome Research Center, Department of Clinical Research, University Hospital of Basel, Basel, Switzerland; Research and Development, Shoulder and Elbow Surgery, Schulthess Klinik, Zurich, Switzerland); Thomas Stojanov, MSc (Department of Orthopaedic and Trauma Surgery, University Hospital Basel, Basel, Switzerland; Research and Development, Shoulder and Elbow Surgery, Schulthess Klinik, Zurich, Switzerland); Sebastian A. Müller, MD (Department of Orthopaedic and Trauma Surgery, Shoulder and Elbow, Cantonal Hospital Baselland, Bruderholz, Switzerland; Faculty of Medicine, University of Basel, Basel, Switzerland); Christian Candrian, MD (Trauma and Ortho Unit, Ospedale Regionale di Lugano, Lugano, Switzerland); ARCR_Pred Study Group; and Andreas M. Müller, MD (Department of Orthopaedic and Trauma Surgery, University Hospital Basel, Basel, Switzerland).
Members of the ARCR_Pred Study Group are listed below per site and partner institution:
ARTHRO Medics, Basel, CH: Claudio Rosso (Principal Investigator [PI]), Lena Fankhauser, Gernot Willscheid; Charitè Medicine University, Berlin, DE: Philipp Moroder (PI), Doruk Akgün, Victor Danzinger, Henry Gebauer, Jan-Philipp Imiolczyk, Katrin Karpinski, Lucca Lacheta, Marvin Minkus, Alp Paksoy, Eduardo Samaniego, Kathi Thiele, Isabella Weiss; Cantonal Hospital Baselland, Bruderholz, CH: Thomas Suter (PI), Julia Müller-Lebschi, Sebastian Mueller, Markus Saner, Claudia Haag-Schumacher, Giorgio Tamborrini-Schütz; Public Hospital Solothurn, Solothurn, CH: Mai Lan Dao Trong (PI), Carlos Buitrago-Tellez, Julian Hasler, Ulf Riede, Sandra Weber; Hôpital du Valais–Centre Hospitalier du Valais Romand, Martigny, CH: Beat Moor (PI), Matthias Biner, Sarah Fournier, Nicolas Gallusser, Deborah Marietan, Sebastien Pawlak; Endoclinic, Zurich, CH: Christoph Spormann (PI), Britta Hansen, Nadja Mamisch; Klinik Gut, St Moritz, CH: Holger Durchholz (PI), Jakob Bräm; Hirslanden Clinique la Colline, Geneva, CH: Gregory Cunningham (PI), Abed Kourhani, Sarah Ossipow, Patricia Simao; La Tour Hospital, Meyrin, CH: Alexandre Lädermann (PI); Inselspital, Bern, CH: Rainer Egli, Stephanie Erdbrink, Remy Flückiger, Paolo Lombardo, Tawan Pinworasarn, Philipp Scacchi, Johannes Weihs, Matthias Zumstein; In-Motion, Wallisellen, CH: Matthias Flury (PI), Ralph Berther, Christine Ehrmann, Larissa Hübscher; Institute of Social and Preventive Medicine, University of Bern, Bern, CH: David Schwappach; Cantonal Hospital of Baden, Baden, CH: Karim Eid (PI), Susanne Bensler, Yannick Fritz, Nisha Grünberger, Philipp Kriechling, Daniel Langthaler, Richard Niehaus, Raffaela Nobs; Cantonal Hospital of Winterthur, Winterthur, CH: Emanuel Benninger (PI), Quintin de Groot, Aleksis Doert, Sebastian Ebert, Philemon Grimm, Fabian Mottier, Markus Pisan, Jan Schätz, Ariane Schwank, Julian Wiedenbach; Schulthess Klinik, Zurich, CH: Markus Scheibel (PI), Laurent Audigé, Frederik Bellmann, Daniela Brune, Marije de Jong, Stefan Diermayr, David Endell, Marco Etter, Florian Freislederer, Nikitas Gkikopoulos, Michael Glanzmann, Cécile Grobet, Christian Jung, Fabrizio Moro, Philipp Moroder, Ralph Ringer, Jan Schätz, Hans-Kaspar Schwyzer, Béatrice Weber, Martina Wehrli, Barbara Wirth, Manuela Nötzli, Anne Franz, Jörg Oswald, Birgit Steiger, Yacine Ameziane, Christopher Child, Giovanni Spagna; Ospedale Regionale di Lugano, Lugano, CH: Christian Candrian (PI), Filippo Del Grande, Pietro Feltri, Giuseppe Filardo, Francesco Marbach, Florian Schönweger; Cantonal Hospital of St. Gallen, St. Gallen, CH: Bernhard Jost (PI), Michael Badulescu, Stephanie Lüscher, Fabian Napieralski, Lena Öhrström, Martin Olach, Jan Rechsteiner, Jörg Scheler, Christian Spross, Vilijam Zdravkovic; Orthopädie Sonnenhof, Bern, CH: Matthias A. Zumstein (PI), Adrian Chlasta, Kate Gerber, Annabel Hayoz, Julia Müller-Lebschi, Frederick Schuster; University Clinic Balgrist, Zurich, CH: Karl Wieser (PI), Paul Borbas, Samy Bouaicha, Roland Camenzind, Sabrina Catanzaro, Christian Gerber, Florian Grubhofer, Anita Hasler, Bettina Hochreiter, Roy Marcus, Farah Selman, Reto Sutter, Sabine Wyss; University Library Basel, University of Basel, Basel, CH: Christian Appenzeller-Herzog; University Hospital of Basel, Basel, CH: Soheila Aghlmandi, Ilona Ahlborn, Cornelia Baum, Franziska Eckers, Kushtrim Grezda, Simone Hatz, Sabina Hunziker, Thomas Stojanov, Mohy Taha, Giorgio Tamborrini-Schütz, Andreas Marc Mueller (PI).
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465231219253 – Supplemental material for Functional and Radiologic Outcomes of Degenerative Versus Traumatic Full-Thickness Rotator Cuff Tears Involving the Supraspinatus Tendon
Supplemental material, sj-pdf-1-ajs-10.1177_03635465231219253 for Functional and Radiologic Outcomes of Degenerative Versus Traumatic Full-Thickness Rotator Cuff Tears Involving the Supraspinatus Tendon by Cornelia Baum, Laurent Audigé, Thomas Stojanov, Sebastian A. Müller, Christian Candrian, Andreas M. Müller, Claudio Rosso, Lena Fankhauser, Gernot Willscheid, Philipp Moroder, Doruk Akgün, Victor Danzinger, Henry Gebauer, Jan-Philipp Imiolczyk, Katrin Karpinski, Lucca Lacheta, Marvin Minkus, Alp Paksoy, Eduardo Samaniego, Kathi Thiele, Isabella Weiss, Thomas Suter, Julia Müller-Lebschi, Sebastian Mueller, Markus Saner, Claudia Haag-Schumacher, Giorgio Tamborrini-Schütz, Mai Lan Dao Trong, Carlos Buitrago-Tellez, Julian Hasler, Ulf Riede, Sandra Weber, Beat Moor, Matthias Biner, Sarah Fournier, Nicolas Gallusser, Deborah Marietan, Sebastien Pawlak, Christoph Spormann, Britta Hansen, Nadja Mamisch, Holger Durchholz, Jakob Bräm, Gregory Cunningham, Abed Kourhani, Sarah Ossipow, Patricia Simao, Alexandre Lädermann, Rainer Egli, Stephanie Erdbrink, Remy Flückiger, Paolo Lombardo, Tawan Pinworasarn, Philipp Scacchi, Johannes Weihs, Matthias Zumstein, Matthias Flury, Ralph Berther, Christine Ehrmann, Larissa Hübscher, David Schwappach, Karim Eid, Susanne Bensler, Yannick Fritz, Nisha Grünberger, Philipp Kriechling, Daniel Langthaler, Richard Niehaus, Raffaela Nobs, Emanuel Benninger, Quintin de Groot, Aleksis Doert, Sebastian Ebert, Philemon Grimm, Fabian Mottier, Markus Pisan, Jan Schätz, Ariane Schwank, Julian Wiedenbach, Markus Scheibel, Laurent Audigé, Frederik Bellmann, Daniela Brune, Marije de Jong, Stefan Diermayr, David Endell, Marco Etter, Florian Freislederer, Nikitas Gkikopoulos, Michael Glanzmann, Cécile Grobet, Christian Jung, Fabrizio Moro, Philipp Moroder, Ralph Ringer, Jan Schätz, Hans-Kaspar Schwyzer, Béatrice Weber, Martina Wehrli, Barbara Wirth, Manuela Nötzli, Anne Franz, Jörg Oswald, Birgit Steiger, Yacine Ameziane, Christopher Child, Giovanni Spagna, Christian Candrian, Filippo Del Grande, Pietro Feltri, Giuseppe Filardo, Francesco Marbach, Florian Schönweger, Bernhard Jost, Michael Badulescu, Stephanie Lüscher, Fabian Napieralski, Lena Öhrström, Martin Olach, Jan Rechsteiner, Jörg Scheler, Christian Spross, Vilijam Zdravkovic, Matthias A. Zumstein, Adrian Chlasta, Kate Gerber, Annabel Hayoz, Julia Müller-Lebschi, Frederick Schuster, Karl Wieser, Paul Borbas, Samy Bouaicha, Roland Camenzind, Sabrina Catanzaro, Christian Gerber, Florian Grubhofer, Anita Hasler, Bettina Hochreiter, Roy Marcus, Farah Selman, Reto Sutter, Sabine Wyss, Christian Appenzeller-Herzog, Soheila Aghlmandi, Ilona Ahlborn, Cornelia Baum, Franziska Eckers, Kushtrim Grezda, Simone Hatz, Sabina Hunziker, Thomas Stojanov, Mohy Taha, Giorgio Tamborrini-Schütz and Andreas Marc Mueller in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank M. Wilhelmi, PhD (medical writer at Schulthess Klinik), for language editing the final manuscript.
Submitted June 16, 2023; accepted October 2, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was funded by the Swiss National Science Foundation (SNF Project ID 320030_184959, ![]() ). Complementary grants were provided by Swiss Orthopedics to support project site documentation. The following sites are funding their participation in the project: Charitè Medicine University, Berlin, Germany; Public Hospital Solothurn, Solothurn, Switzerland; Endoclinic, Zurich, Switzerland; Inselspital, Bern, Switzerland; and University Clinic Balgrist, Zurich, Switzerland. C.B. received funding for her research salary from the University Hospital Basel, Department of Surgery. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
). Complementary grants were provided by Swiss Orthopedics to support project site documentation. The following sites are funding their participation in the project: Charitè Medicine University, Berlin, Germany; Public Hospital Solothurn, Solothurn, Switzerland; Endoclinic, Zurich, Switzerland; Inselspital, Bern, Switzerland; and University Clinic Balgrist, Zurich, Switzerland. C.B. received funding for her research salary from the University Hospital Basel, Department of Surgery. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.