
Abstract
Background:
Osteochondral lesions (OCLs) of the knee, whether occurring secondary to osteochondritis dissecans or a traumatic osteochondral fracture, are commonly encountered in the pediatric and adolescent population. Given the potential for healing in this population, coupled with adequate surgical reduction and stability of OCL fixation, an opportunity exists to avoid a major restorative procedure and the associated substantial costs and potential morbidity.
Purpose:
To analyze the outcomes of bioabsorbable fixation of OCLs in the adolescent knee at a minimum of 2 years.
Study Design:
Case series; Level of evidence, 4.
Methods:
An institutional review board–approved retrospective review was performed of patients younger than 18 years who underwent bioabsorbable fixation of an OCL of the knee with a minimum 2-year follow-up. Patient demographics, operative details, and postoperative clinical findings were detailed and recorded. All cases were performed by a single surgeon.
Results:
There were 38 patients treated surgically for an OCL between 2009 and 2016. Of these, 38 patients (mean age, 14.7 years) were evaluated at a mean of 59 months. OCL fixation consisted of a mean of 1.4 bioabsorbable screws and 1.5 darts. At final follow-up, mean pre- and postoperative Tegner scores were 6.6 and 6.4, respectively, while Lysholm and Pediatric International Knee Documentation Committee scores were 89.8 and 88.1, respectively. A total of 6 patients underwent secondary procedures postoperatively. One patient required a secondary procedure related to OCL fixation, which was secondary to a proud implant. The other secondary procedures included second-look arthroscopic surgery for pain after an injury postoperatively, planned anterior cruciate ligament reconstruction, staged medial patellofemoral ligament reconstruction, and manipulation under anesthesia for arthrofibrosis (n = 2). None of the 32 patients required a revision cartilage procedure at the time of final follow-up.
Conclusion:
The use of bioabsorbable implants in the adolescent knee appears to be a safe and efficacious treatment with good functional outcomes at long-term follow-up and a low revision rate. Additional long-term multisurgeon and multicenter trials with a larger cohort are needed to further elucidate the role of bioabsorbable fixation of an OCL in the adolescent knee.
Osteochondral lesions (OCLs) of the knee, whether occurring secondary to osteochondritis dissecans (OCD) or a traumatic osteochondral fracture (OCF), are commonly encountered in the pediatric and adolescent population. 4,5,7,8,11,13,15,16,22 Influential factors for the treatment of OCLs in the adolescent knee include OCL location, size, stability, and severity of symptoms. Procedures range from microfracture/marrow stimulation and osteochondral autograft/allograft/matrix-associated autologous chondrocyte implantation to, when amenable, OCL fixation. §
The goal of OCL fixation is to preserve the native articular hyaline cartilage and promote healing of the osteochondral layer and subchondral bone. 2,9,10,12,15,29 Fixation can be performed with metal implants that often require a second surgical procedure for implant removal. 11 Bioabsorbable implants are an alternative to metal and may provide stable fixation and obviate the need for a second procedure. 14,15,17 –20,24,25,27 –29
Previous literature on the effectiveness of bioabsorbable fixation of OCLs have been published with favorable results; however, the majority of these studies are focused either on solely OCD or OCFs. 14,15,17,19,20,25,27 –29 Studies that involve both types of abnormalities are few in number and only contain a small sample size. 9,19 The purpose of our study was to review the utility and outcomes of internal fixation with bioabsorbable implants for OCLs, whether from OCFs or OCD of the knee, in an adolescent population.
Methods
Institutional review board approval was obtained for this study. Children treated with internal fixation using bioabsorbable implants for an OCL (OCD or OCF) of the knee at a major tertiary care children’s hospital from 2009 to 2016 were identified from a computerized database.
Inclusion criteria consisted of children and adolescents aged 10 to 18 years at the time of the procedure who underwent surgery for an OCL with bioabsorbable fixation (3.0-mm Bio-Compression Screws and/or Chondral Darts; Arthrex). In addition, they had to have complete medical records and a minimum follow-up of 2 years with validated outcome scores (pediatric International Knee Documentation Committee [Pedi-IKDC], Lysholm knee, and preoperative and postoperative Tegner activity scores).
Surgery was indicated and performed by the senior author (J.A.S.). The decision to perform internal fixation of the OCL was based on the patient’s clinical symptoms, radiographs, magnetic resonance imaging (MRI) and arthroscopic findings of lesion instability, presence of a loose osteochondral fragment, or a fracture.
Medical records, plain films, and MRI scans were reviewed. Data collected included age, sex, follow-up time, lesion or fragment location, size of lesion, number of implants (screws and darts), occurrence of subsequent surgery, and surgical outcome on the basis of a postoperative clinical evaluation. Failure of the primary procedure was also recorded and defined as a need for a revision cartilage procedure. Additional information was gathered through 3 standardized knee function questionnaires. Functional outcomes were determined using the Pedi-IKDC subjective knee evaluation form and Lysholm knee scale. The level of activity was determined using the Tegner activity scale.
An arthroscopic evaluation of the OCL was performed primarily in all cases. In cases of OCD where the lesion had an in situ fragment, the lesion was assessed for stability. The peripheral rim of the lesion was stressed with a 5-mm arthroscopic probe. If the peripheral rim demonstrated impending instability (ie, cartilage fissure or breach at the periphery) but the cartilage lesion was not able to be hinged open from the base/crater (ie, locked door), these lesions were fixed in situ arthroscopically with Bio-Compression Screws and/or Chondral Darts. 6 The amount of screws or darts utilized was based on the size and location of the lesion and whether it needed stability. Each implanted screw and/or dart breached the native articular surface of the OCL fragment, and therefore, the fewest number of screws and/or darts necessary to achieve stability were utilized to minimize the effect on the native cartilage of the OCL fragment. The 3.0-mm Bio-Compression Screw is noncannulated and made of poly-L-lactic acid material. The screw is tapered in design, with the implant being 3.7 mm at the screw head and 2.7 mm at the screw tip, and comes in varying lengths from 16 to 26 mm. Each Chondral Dart is made of poly-L-lactic acid material and has a reversed barb design (1.3 mm in diameter and 18 mm in length).
Lesions were deemed unstable if the involved osteochondral fragment could be hinged open and the underlying subchondral bone was able to be visualized (ie, trap door) or where a loose fragment separated from its base and there was an exposed subchondral bone defect/crater. 6 Unstable OCLs were approached via open arthrotomy. The creation of the arthrotomy site was based on the location of the OCL and was made by proximally extending the vertical anteromedial or anterolateral arthroscopic portal approximately 5 cm. After the creation of the arthrotomy site, the site of the OCL was further localized, and the bone at the base of the lesion was prepared with a curette to expose a bleeding cancellous bed. If there was loss of bone, autogenous bone was harvested from the ipsilateral distal femoral metaphysis proximal to the physis and was used to fill the subchondral defect.
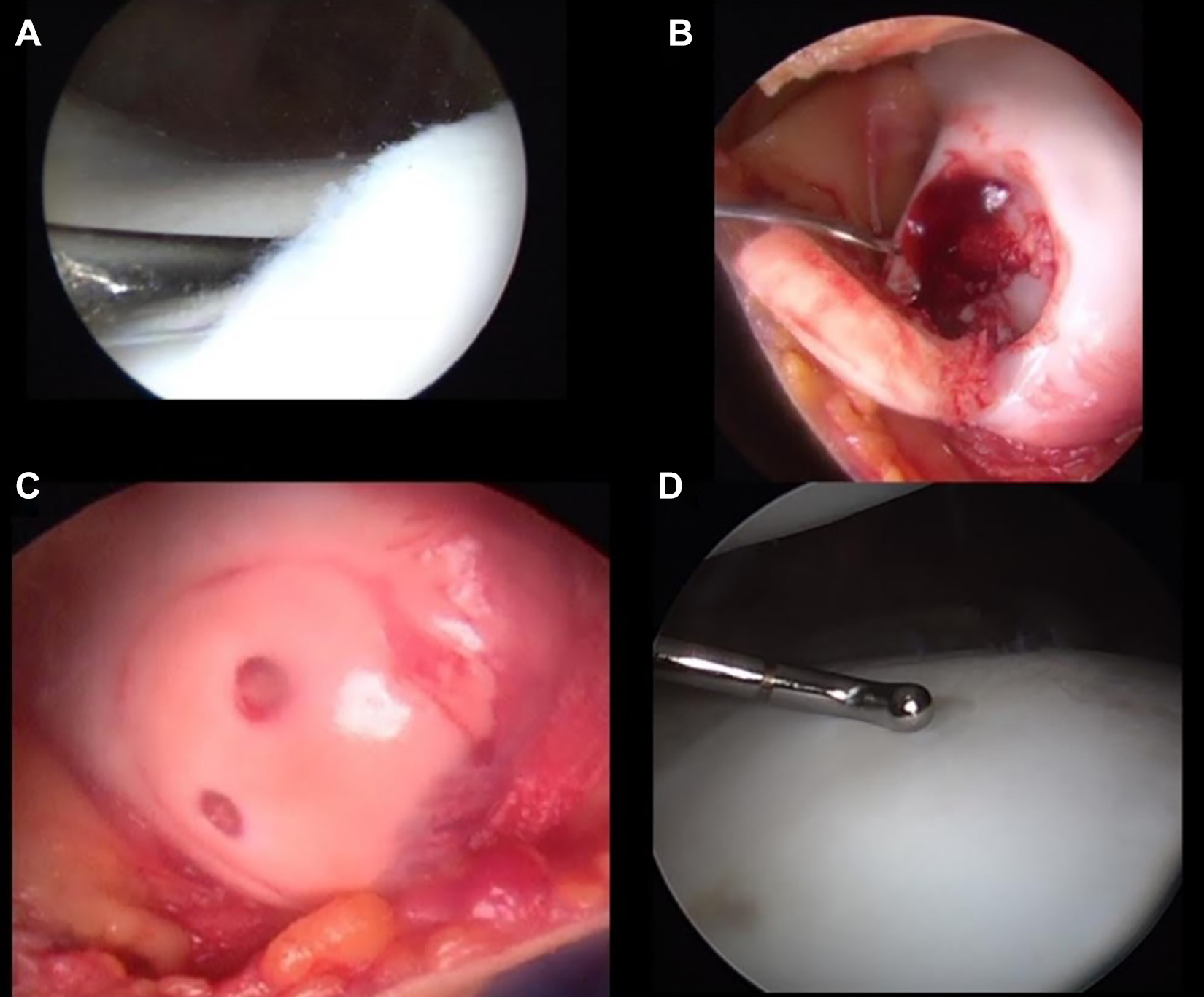
The fragment was then reduced as anatomically as possible. It was provisionally stabilized with smooth guide pins, which were placed as perpendicular as possible to the OCL such that they would stabilize the fragment during implant insertion and not interfere with the desired screw/dart location. When implanting a screw, a cannulated drill was next placed over one of the smooth guide pins and drilled down to the articular surface to a flat area on the drill bit where the flutes meet the shank. This was followed by a cannulated tap placed over the guide pin and tapped until all threads were buried under the articular cartilage again. The guide pin was then removed, and the screw was inserted. At full seating, the screw was 2 to 3 mm below the articular surface. The provisionally placed guide pin(s) were then removed, used to place a second screw, or removed and replaced by a Chondral Dart. Chondral Dart insertion was preceded by drilling through the reduced OCL, and the dart was placed through a sheath with an inserter and lightly tapped into place until the dart was fully seated 1 to 2 mm below the articular surface. Figure 1 is an example of one of our patients who underwent internal fixation because of an OCF.

(A) Arthroscopic photographs of a 16-year-old boy who sustained an osteochondral fracture at the periphery of the lateral femoral condyle and a concomitant anterior cruciate ligament (ACL) injury after a skateboard accident. (B) The fragment was retrieved, and (C) the procedure was converted to open arthrotomy. The fragment was reduced in the fracture bed and stabilized with 3 Bio-Compression Screws and 2 Chondral Darts. (D) Planned staged ACL reconstruction was performed 5 months after the initial surgery; second-look arthroscopic surgery demonstrated a healed osteochondral fracture with no visibility of the original implants.
Postoperatively, patients were placed in a locked range of motion brace, which was removed for the use of a home continuous passive motion (CPM) machine and range of motion exercises commencing on postoperative day 1. All patients underwent physical therapy, which began within 7 to 14 days postoperatively. Patients were kept nonweightbearing on the surgical side for 6 weeks. Return to sporting activities was permitted at 4 to 6 months postoperatively.
Mean outcome scores were compared between categorical variables utilizing analysis of variance or the nonparametric Mann-Whitney U test or Kruskal-Wallis test if either normality or homogeneity of variance assumptions was violated. The relationship between outcome scores and interval or continuous variables was evaluated with the Spearman rank correlation coefficient. Alpha was set at P < .05 to indicate significance. In addition, correlations were evaluated according to the Cohen effect size: 0.10 indicates a small effect, 0.30 indicates a medium effect, and 0.50 indicates a large effect. SPSS (version 25.0; IBM) was utilized for analyses.
Results
From 2009 to 2016, there were 38 children and adolescents who underwent internal fixation with bioabsorbable implants for OCLs of the knee. Of these patients, 32 were able to be contacted with a minimum 2-year follow-up (84%). The mean follow-up period was 59 months (range, 24-111 months). The mean patient age was 14.7 years (range, 12-17 years).
Of the 32 children and adolescents, 17 had OCFs (53%), while the remaining 15 had OCD (47%). The mean number of screws and darts used per case was 1.4 (range, 0-3) and 1.5 (range, 0-4), respectively. Table 1 summarizes the location of the lesions, size of these lesions, and number of implants used based on the type of OCL.
Location of Injury, Size of Lesion, and Number of Bioabsorbable Screws and Darts Used per Case a
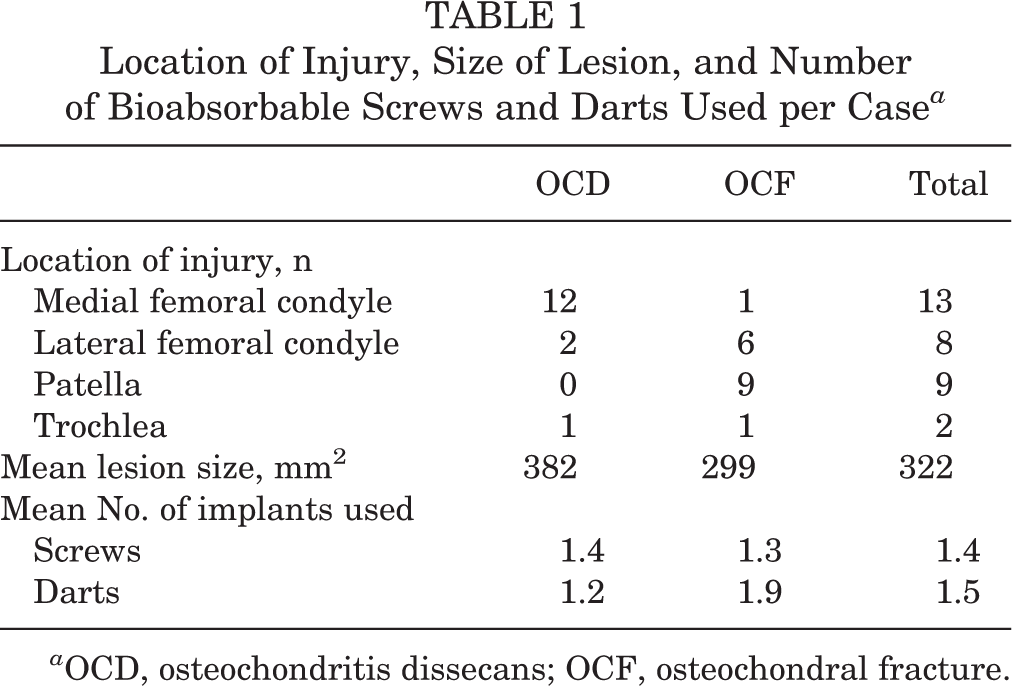
a OCD, osteochondritis dissecans; OCF, osteochondral fracture.
None of the 32 patients required a second cartilage-restoring procedure. There were 6 patients who returned to the operating room after the index procedure; however, only 1 of these was directly related to OCL fixation. This patient had an original diagnosis of OCD of her medial femoral condyle. She underwent open reduction with internal fixation with 2 bioabsorbable darts and 1 bioabsorbable screw. Approximately 8 months after the primary surgical procedure, the patient developed symptoms of intermittent pain and swelling. She returned to the operating room approximately 10 months after the index procedure, during which we found one of the implants protruding less than 0.5 mm from the articular surface. The OCL was found to be stable and fully healed. The piece that was protruding was able to be excised, and afterward, the patient recovered well, and her symptoms were fully alleviated.
Another patient who returned to the operating room after the initial OCL procedure was a 17-year-old boy who was diagnosed with OCD of the lateral aspect of the trochlea and underwent open reduction with internal fixation with 2 bioabsorbable screws. He returned to the operating room 16 months after the primary surgical procedure because of pain after an acute injury. Second-look arthroscopic surgery demonstrated that the lesion fully healed, and he did well postoperatively after a course of physical therapy (Figure 2). Table 2 further summarizes the 6 patients who required a second procedure.
(A, B) Arthroscopic photographs of a 17-year-old boy who was diagnosed with osteochondritis dissecans of the lateral aspect of the trochlea. (C) The patient underwent open reduction with internal fixation with 2 bioabsorbable screws; he returned to the operating room 16 months after the primary surgery because of new symptoms after an acute injury. (D) Second-look arthroscopic surgery demonstrated that the lesion fully healed; the patient did well postoperatively after a course of physical therapy.
Summary of 6 Patients Who Required a Return to the Operating Room a

a ACL, anterior cruciate ligament; LFC, lateral femoral condyle; MFC, medial femoral condyle; MPFL, medial patellofemoral ligament reconstruction; OCD, osteochondritis dissecans; OCF, osteochondral fracture; OCL, osteochondral lesion.
The mean preoperative and postoperative Tegner scores at final follow-up were 6.6 (range, 5-9) and 6.4 (range, 5-9), respectively. The mean Pedi-IKDC score was 88.1 (range, 62-100), and the mean Lysholm score was 89.8 (range, 59-100). Table 3 summarizes the outcome scores based on the OCD and OCF groups.
Functional Outcome Scores at Final Follow-up a

a Data are shown as mean (range). Lysholm and Pedi-IKDC scores are from 0 to 100. Tegner scores are from 0 to 10. OCD, osteochondritis dissecans; OCF, osteochondral fracture; Pedi-IKDC, pediatric International Knee Documentation Committee.
Statistical analysis was performed on our independent variables to see if they had any relationship with the functional outcome scores that we measured. No independent variable, which included age, location of the OCL, size of the OCL, and number of implants, was found to be of significance when determining a relationship with the respective patient’s Lysholm and Pedi-IKDC scores. However, there was 1 variable that had a correlation that met the Cohen standard for a medium effect size. This variable was the size of the OCL and its effect on the Lysholm score (rho = –0.303). It appeared that the larger OCLs did not fare as well based on the Lysholm score; however, a larger sample is needed to determine whether this correlation is significant.
Discussion
As participation in youth sports increases, OCLs in the adolescent population will continue to be a common problem that the treating physician will encounter. The milieu of the pediatric and adolescent knee provides an environment favorable to healing. After the development of an OCL, whether from OCD or a traumatic OCF, the preservation of the native articular hyaline cartilage in the population is of paramount importance.
Bioabsorbable implants offer an option for internal fixation to provide patients with stable fixation that promotes healing. The bioabsorbable nature of these implants avoids the need for implant removal. Our current study demonstrates that fixation of OCLs, whether it be from OCD or an OCF, with bioabsorbable implants can be an effective treatment in the adolescent knee. This is supported by our low complication rate, excellent functional outcome scores, and none of the children and adolescents in this cohort requiring a secondary cartilage procedure at a mean follow-up of nearly 5 years.
CPM use may not be standard after surgery for OCLs. However, it has been the senior author’s preferred approach to use CPM in the early rehabilitation period (postoperative days 1-21). CPM is utilized in an attempt to ease anxiety associated with moving the knee after surgery that is sometimes encountered in this population and ideally helps decrease the occurrence of postoperative arthrofibrosis.
Internal fixation of OCLs is indicated when the lesion demonstrates impending instability such as an OCD lesion that has an intact hinge and is at a high risk to displace, an unstable OCD lesion, or an acute OCF that can be anatomically reduced. The benefits of this procedure are that it preserves the native hyaline cartilage, promotes healing between the bone surfaces of the fracture bed and OCL, and restores the natural contour of the knee’s joint surface. These benefits are possible but difficult to mirror in other cartilage-salvaging procedures. Microfracture or marrow stimulation by drilling is less invasive compared with fixation; however, it is limited to only small defects and promotes type I fibrocartilage as opposed to normal type II hyaline cartilage. 4,6 Osteochondral autograft transfer has had promising results for large OCLs; however, it carries a higher morbidity and can be technically demanding. 26 Matrix-associated autologous chondrocyte implantation allows defects to be replaced with autologous type II hyaline cartilage; however, it requires 2 surgical procedures and has substantial financial costs. 21
Bandi and Allgoewer 3 were the first to report fixation of an OCL in the knee using bone pegs in 1959. Afterward, headless metal screws were described for the treatment of OCLs. 18,24 One of the notable complications from this procedure was backing out of the screw that resulted in cartilage damage from screw protrusion. The invention of bioabsorbable implants (screws, darts, pins) for these lesions can theoretically decrease the occurrence of this complication and negates the need for a secondary procedure for screw removal. 15,19,20,26 –29
Previous literature on this technique for adolescent OCLs of the knee has reported similar results to our findings. 15,19,20,26 –28 Tabaddor et al 26 published on juvenile OCD lesions. Their study included 24 children with an average follow-up of 39.6 months. Their average IKDC score was 84.9; in the current study, the overall mean IKDC score was 88.1 and the mean score for the OCD patients was 92.1. Their average Lysholm score was 88.1 compared with our study’s overall mean of 89.8 and mean for OCD patients of 90.5. Their mean preoperative and postoperative Tegner scores were 7.3 and 7.9, respectively, while our study’s postoperative Tegner mean scores were 6.6 and 6.4, respectively. In the Tabaddor et al study, 2 of the 24 patients (8%) required a reoperation because of failure of healing of the OCD lesion, whereas there were no revision cartilage procedures in the current study.
Walsh et al 27 performed a study on adolescent knees that underwent bioabsorbable fixation for OCFs. Their study included 8 patients with a minimum follow-up of 5 years, in which 5 had a normal IKDC score (“A”), 2 were nearly normal (“B”), and 1 was abnormal (“C”). In addition, 7 of the 8 patients had a Cincinnati Knee Rating System score above 90, while 1 patient had a score of 69. They were able to obtain MRI scans of each patient after 5 years from the procedure, and all of them demonstrated intact articular cartilage with no areas of full-thickness loss.
There have been several studies published on this treatment method for OCD or OCFs; however, studies that involve both conditions are sparse. 9,19 After performing a thorough literature review, only 2 studies were found to involve both types of OCLs. Dines et al 9 evaluated 9 cases involving bioabsorbable fixation; however, 8 of the cases involved an OCD lesion, and the remaining case was for an OCF. Their average follow-up was 33 months. The average Lysholm score at final follow-up was 94, and none of the patients required a secondary procedure. Matsusue et al 19 also compared both OCD and OCFs. Their cohort, however, only consisted of 5 cases (3 OCD, 2 OCF). All of their patients achieved satisfactory bone union based on radiographs and had pain-free range of motion at final follow-up.
Based on our literature review, our study involved the largest sample size comparing both OCD and OCFs with a relatively even distribution (47% and 53%, respectively). Our mean follow-up time of nearly 5 years is also of significance and likely one of the longer durations compared with similar studies. Last, we used established and proven validated outcome measures (Tegner, Lysholm, and Pedi-IKDC) that accurately reflect the effectiveness of these procedures. Table 4 summarizes our findings and compares them with those of similar studies that have been published.
Studies Focusing on Osteochondral Lesions of the Adolescent Knee After Bioabsorbable Fixation a

a IKDC, International Knee Documentation Committee; N/A, not available; OCD, osteochondritis dissecans; OCF, osteochondral fracture.
Our study is not without limitations. The first limitation is the retrospective and nonrandom design of the study and lack of control groups. Because of the retrospective nature of this study, preoperative Lysholm and Pedi-IKDC scores were not available for comparison with postoperative scores. Although we had a larger sample size (N = 32) compared with previous studies, smaller numbers in the subgroup analysis by failure, lesion location, lesion size, and number of implants used limited our study power for comparative analyses. Our limited sample size also likely attributed to our inability to demonstrate a relationship of independent variables analyzed with functional outcome scores. Some previous studies were able to include MRI at final follow-up to better evaluate healing of the OCL. The majority of our patients did not have a postoperative MRI scan because of their absence of any clinical symptoms that would indicate a need to conduct imaging. 26,27 Finally, we were only able to include 84% of our initial sample size because the remaining patients were unable to be contacted via telephone and mail.
OCLs of the adolescent knee will always remain challenging injuries to treat because of patient factors, various surgical options with a wide range of effectiveness, and last, the surgeon’s experience. We feel that it is of paramount importance that these unstable lesions be treated to prevent early degenerative changes that can severely alter these children’s functional well-being. Our study demonstrated that internal fixation with bioabsorbable implants in OCLs, whether they be from OCD or an OCF, can lead to excellent functional outcome scores and a low likelihood of requiring a secondary procedure because of failure of the implant to stabilize the lesion.
We have demonstrated promising results at midterm follow-up (59 months) in a pediatric and adolescent cohort. Validated functional outcome scores were good, and no revision cartilage procedures were necessary at last follow-up. Longer term multicenter and multisurgeon data are needed to further elucidate the utility of bioabsorbable implants for OCLs in the adolescent knee.
Footnotes
Acknowledgment
The authors acknowledge Tracey Bastrom for her assistance with statistical analysis.
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: J.A.S. has received speaking fees from Arthrex and educational support from Smith & Nephew, DePuy, and Micromed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Children’s Hospital of Orange County Institutional Review Board (No. 170326).