
Abstract
Purpose:
Osteochondral lesions of the talus are lesions that are seen particularly in the young age group and are often related to sports injuries and trauma. These lesions, which show late symptoms radiologically, can be determined in the early stages with magnetic resonance imaging. The aim of this study was to present a new osteotomy technique to reduce the complications of mosaicplasty surgery to a minimum and provide an early return to work.
Methods:
A total of 11 patients who had cartilage lesions due to osteochondritis dissecans in the medial aspect of the talus underwent mosaicplasty after a triplanar osteotomy. The dimensions of the lesion and the depth of the triplanar osteotomy were determined preoperatively. Coronal, sagittal and transverse cuts were made at the depth defined arthroscopically. Following the osteotomy, an osteochondral graft taken from the ipsilateral knee was placed in the prepared area. Osteotomy side was fixed with one or two cannulated screws following mosaicplasty.
Results:
With this technique, weight-bearing can be immediate in cases with no need for osteotomy in the joint surface. In cases including the joint surface, partial weight-bearing is permitted after 4 weeks and can be increased as tolerated. In the 11 cases treated with this technique, full weight-bearing was achieved at mean 5 weeks (range, 5–8 weeks). No shift (upward displacement of osteotomized fragment) or non-union was seen in any patient.
Conclusion:
With the triplanar osteotomy technique described here, potential shift complications can be reduced to a minimum. As only the lesion region is targeted, the osteochondral surface formed by the fracture is much less.
Study design:
Case Series; Level of Evidence, 4.
Keywords
Introduction
Osteochondral lesions of the talus (OLT) are defined as injury to the cartilage and bone occurring in the upper joint surface of the talus. This is known as an osteochondritis dissecans (OCD) lesion of the talus. 1 –3 OLT usually occur following trauma and are seen as a result of severe ankle sprain. 2,4,5 It may also be seen because of other reasons such as overloading on a certain point of the talus associated with malalignment of the ankle joint, instability of the ankle or drugs. In addition, cases caused by probable endocrine disorders in which the aetiology cannot be explained are noteworthy. 2,6,7
The majority of OLTs, which initially show an asymptomatic course, are usually normal on X-ray. Lesions, which show late symptoms on X-ray views, can be determined in the early stages with magnetic resonance imaging (MRI). 6,8 Therefore, MRI is applied to many cases with radiological suspicion. More than 60% of OCD lesions are seen in the medial dome of the talus. 6,9 A 9-zone grid plan was described by Raikin et al. for the localization of OCDs. 6 According to the plan applied on MRI axial slices, 62.8% of cases show localization in the medial dome. As closed methods are not sufficient to reach the lesion, there is usually a need for osteotomy of the medial malleolus. 10 –13
Open mosaicplasty surgery becomes mandatory in these cases because of the progressive course of the disease and delay in treatment. Although the early and midterm results of open mosaicplasty surgery have been clinically supported with several successful results, severe surgery-related complications may be seen. The majority of these complications are related to osteotomy applied in the distal tibia. Upward displacement in the medial malleolus, chondral damage in the distal tibia joint surface and non-union or malunion of the osteotomy line are significant problems. 1,2 –7 The osteotomy not allowing the possibility of early weight-bearing, loss of workforce and delayed return to sports are other frequently encountered problems.
In this article, a new osteotomy is described which reduces potential complications to a minimum as a result of the analyses based on kinesiological and radiological measurements. Lesions in zones 1 and 4 can be successfully treated with this technique. Excellent short-term results are obtained by reducing the risk of complications to a minimum. With a minimal osteotomy, sufficient access to the lesion can be obtained and 90% of talar dome lesions with medial localization can be treated. This limited osteotomy reduces chondral damage of the distal tibial joint surface and obtains adequate window for mosaicplasty.
The aim of this study was to present the arthroscopy-assisted triplanar osteotomy technique and the short-term results of a limited number of cases.
Method
All experiments were conducted in accordance with the Ministry of Health of Turkey, the Declaration of Helsinki and the National Institutes of Health (NIH) of the United States. The ethical committee of Health Sciences University Derince Training and Research Hospital approved all surgical and clinical procedures in this study (Ethics number: 2019-142).
The study included 11 patients who presented at our clinic between February 2016 and January 2018 and were diagnosed with symptomatic OLT. Informed consent was obtained from all the patients. All the surgical procedures were applied by a single surgeon in the same clinic. The inclusion criteria for this prospective, observational study were patient age of 18–55 years, an isolated lesion in the medial talar dome, osteochondral damage of grades 3–4–5 according to the Hepple magnetic resonance grading system and >1 cm distance of the lesion to the posterior border of the anterior joint line on intraoperative measurements. Treatment was applied to lesions in zones 1–4–7 (medial dome) according to the 9-zone anatomic plan used in OLT localization. Preoperative planning was made according to the angle measurements taken on sagittal MRI slices. The OLT zone on the sagittal MRI slices is determined according to the angle measurement (Figure 1). In this measurement, the location of the lesion in zones 1 and 4 is defined and the projection is marked on the lateral X-ray. Thus, evaluation is made of how much of the joint, which will be taken into hyperflexion during surgery, can be seen after osteotomy.
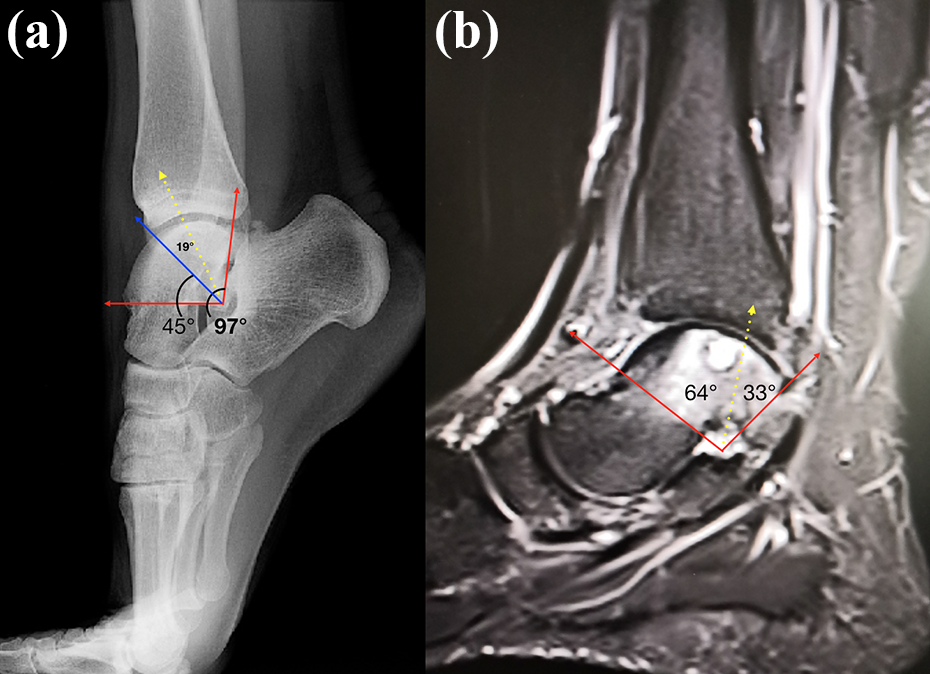
(a) Demonstration of the accessibility of the lesion in hyperflexion on lateral radiography. (b) Zone definition of OLT on sagittal MRI scan. The surgeon can also determine the zones and angles on sagittal MRI scans. The red line indicates the maximum angle (zone 1) that can be achieved without the need for osteotomy. The yellow line indicates the osteotomy line with zone 4 OLTs. OLT: osteochondral lesion of talus; MRI: magnetic resonance imaging.
Surgical technique
Patients were excluded from the study if they had infection, idiopathic, any underlying rheumatological or metabolic disease, malalignment of the ankle, hindfoot deformity, widespread sclerosis narrowing the joint space or >30% reduction in joint range of movement.
All the procedures were performed by a single surgeon. Under a tourniquet, entry was made arthroscopically from anteromedial and anterolateral portals, and diagnostic evaluation was made. After measurement of the OLT dimensions, exposure was provided with an anteromedial incision obtained by lengthening the medial portal.
Intraoperative determination of osteotomy depth
Arthroscopically, the margins of the lesion in the axial and coronal planes are determined when the ankle in plantar hyperflexion. Lesion margins (depth and width) were measured with the aid of 2 mm calibrated arthroscopy probe inserted into the ankle joint from the anteromedial portal. Still, it may not be able to identify the margins of the lesion arthroscopically. If preoperative measurements (lateral plantar flexion radiograph and coronal MRI) are not compatible with arthroscopic measurements, the zone/angle range in which the lesion is located is examined on MRI scans. In this study, 10 mm depth in the axial plane was sufficient in all zone 4 OLTs. The depth of transverse osteotomy and sagittal osteotomy was nearly the same. Because of the shape of anterior tibial plafond, the sagittal plan osteotomy can be 1–3 mm deeper than the axial cut.
Osteotomy steps
Medial and lateral sagittal, transverse and coronal osteotomies are made at the depth defined arthroscopically and according to MRI scans, respectively. To displace the fragment, a fracture is made gently by entering the coronal line with the help of osteotome. Where the transverse osteotomy ends in the medial cortex shows the level of the coronal osteotomy. Before removing the osteotomized bone, the preparation of 1 or 2 cannulated screws hole facilitates fixation. OLTs entering the first 65° angle curve (zones 1–4) are easily treated with this technique.
By determining the fixation sites before osteotomising the fragment, the screw sites were prepared with a cannulated drill. A 0.38 mm microsaw, which measures depth, was preferred for the osteotomy cuts. Sagittal, transverse and coronal cuts were made in sequence with the microsaw, which had the depth marked on it. Ensure that the axial incision is at least 1 cm above the joint to allow sufficient space for fixation (Figure 2). The fragment was excised by creating a controlled chondral fracture with the help of a thin osteotomy located in the axial osteotomy line. Autologous osteochondral graft was harvested from the lateral non-weight-bearing aspect of the femoral condyle of the ipsilateral knee. Arthrex osteochondral autograft transplant system (OATS) (Munich, Germany) manual instruments of 6–8–10 mm diameters were used for the mosaicplasty. In all the patients, autologous transplantation was provided with 1 or 2 autografts prepared at a diameter appropriate to the defect. For bone fixation, 1 or 2 headless cannulated compression screws were used according to the size of the fragment. Finally, a haematoma drainage set was placed in the joint under fluoroscopy guidance (Figure 3).
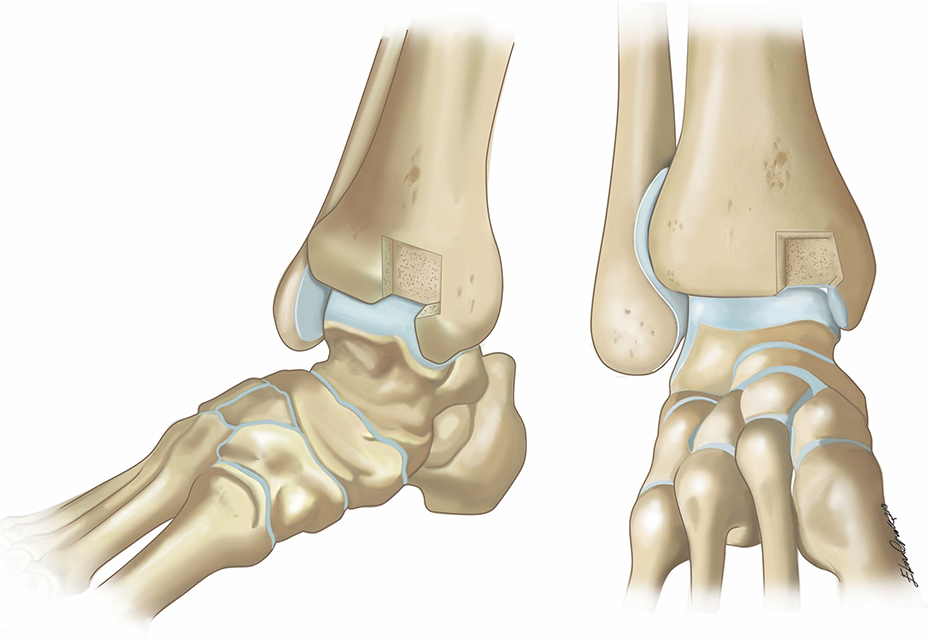
An illustration of surgical technique.

Intraoperative images of a case treated with the triplanar osteotomy technique. (a) Osteotomized ankle joint. (b) Preparation of talar zones 4–7 lesion area. (c) Cylindric autologous osteochondral grafting, (d) Intraoperative lateral fluoroscopic image of OLT and ensuring for the depth of osteotomy. (e) Osteotomized fragment (ruler with cm). (f) OLT with cystic formation. (g) Fragment fixation with a single cancellous screw. OLT: osteochondral lesion of talus.
Postoperative evaluation
Postoperatively, a splint was applied to all patients for the first 2 weeks and knee movements were started immediately. In all patients, sutures were removed and the wound site was checked in the 2nd week, partial weight-bearing and physiotherapy were started in the 4th week and radiological evaluations were made in the 6th and 12th weeks. Clinical evaluation was made at the end of the first 6 months and was repeated every 6 months. All the patients were evaluated clinically according to the American Orthopaedic Foot & Ankle Society (AOFAS)-hindfoot scores in the preoperative and postoperative periods. No second-look arthroscopy was applied to any patient. The follow-up period was shorter than 2 years as the aim of the study was to present a new surgical technique with significant results.
Statistical analysis
Statistical analyses were performed using SPSS version 21.0 software (IBM, Armonk, New York, USA). Comparisons of all preoperative and postoperative follow-up measurements were performed using a paired t-test and analysis of variance and non-parametric Wilcoxon signed-rank tests. A value of p < 0.05 was considered statistically significant.
Results
Evaluation was made of a total of 11 patients, comprising 8 males and 3 females, with a mean age of 31.7 ± 5.9 years (range, 25–42 years). The demographic data are presented in Table 1. The patients treated were those with unilateral, isolated medial zone OLT of diameter 9–15 mm. The ankle complaints were reported to have started after a sporting event in six cases and after trauma in five cases. The time from injury to surgery was mean 6 ± 1.5 months (range, 4–8 months). No patient had a history of ankle surgery other than arthroscopy. Partial weight-bearing was started in the fourth week and full weight-bearing was obtained at mean 5.8 ± 0.9 weeks (Table 1). Weight-bearing was achieved earlier in patients where the osteotomies did not include the joint. The mean follow-up period was 13.1 ± 2.4 months (range, 12–18 months) (Figure 4).
Patient data and outcomes.

TFIS: time from injury to surgery; FWB: full weight bearing; FU: follow-up; OLT: osteochondral lesion of talus; AOFAS: American Orthopaedic Foot & Ankle Society; m: male; f: female; w: week; mo: month; mm: millimetre; pre-o: preoperative.

Case 1: 35-year-old female with medial OLT. (a) Intraoperative assessment of OLT. (b) Triplanar osteotomy, following graft placement, the osteotomy is fixated with titanium screws using the predrilled holes. (c) Osteotomized fragment with no chondral surface of articular side of the tibia. (d) Postoperative lateral view of the ankle. (e) Anterior X-ray view of osteotomized area and fixation. OLT: osteochondral lesion of talus.
The OLT dimensions were recorded according to sagittal and coronal scans of MRI. According to the OLT zone grid, six patients were in zone 4, four patients were in zones 1–4 and one patient was in zones 4–7 (Table 1). The AOFAS score increased from 49.3 ± 10.8 preoperatively to 86.1 ± 7.04 at the final follow-up examination. According to the Wilcoxon signed-rank test, the increase in AOFAS scores was statistically significant (p = 0.003). Effusion developed in the ankle joint and was aspirated in cases 2, 7 and 8. Pain and effusion were seen in the donor site in three patients. No infection, non-union or shift was observed in any patient.
Discussion
The most significant finding of this study was that more than 80% of medial dome lesions of the talus could be reached without osteotomy of the whole malleolus. With the triplanar osteotomy, no shift was seen and the risk of non-union was minimalized. This osteotomy technique was proven to be safe with good clinical results, a minimal complication rate and excellent postoperative scores including improvement of recovery time and function.
Several methods have been described in the literature for the treatment of OLT. 1,3 –8,11,14,15 Different treatment strategies are adopted according to the localization, dimensions and aetiology of the lesion. Successful results have been reported with the use of several different protocols such as nonoperative treatments, arthroscopic drilling and the application of microfracture, fragment excision or curettage, bone grafting or osteochondral transplantation (OCT). 1,3 –8,11,12,15 –17 As the lesion diameter increases, the option of OCT becomes an indispensable treatment option (Figure 5).

Case 2: 42-year-old male patient with zones 4–7 affected OLT. (a and b) Preoperative X-ray views of the ankle in the anterior and lateral position. (c and d) Postoperative X-ray views of ankle AP/L. OLT: osteochondral lesion of talus; AP: anteroposterior; AL: anterolateral.
OCT in the current OLT treatment, for which joint-preserving surgeries and minimally invasive methods are widely used, is applied by completely osteotomising the medial malleolus. However, osteotomy of the medial malleolus may cause chondral lesions on the distal tibia joint surface and may lead to very serious problems such as non-union and shift. Although the fundamental aim of mosaicplasty is to treat osteochondral damage, the safety of the surgical technique has been questioned because of osteochondral damage formed associated with the surgical technique. Early and midterm results of the treatment of OCD lesions with OCT have been reported in a limited number of case series in the literature. The OCT technique by osteotomising the medial malleolus is widely accepted. However, the publication of case series with a limited number of cases, and exclusion of patients with comorbidities, masks the complications of the technique. 4,13,17 Clinical experience and literature data have shown that in cases with medial malleolus osteotomy, the recovery time was not as short as planned, and there have been serious problems such as effusion, shift, non-union or intraarticular step-off following surgery. Other problems encountered in the AOTS technique are pain and effusion in the donor site. 12,17
According to data in the literature, arthroscopic curettage and bone marrow stimulation (BMS) therapy are still accepted as the gold standard treatment option. Despite excellent results obtained with AOT surgery, complication rates of up to 3% are seen. 1 Patients, who are not responsive to nonoperative treatments, curettage and BMS, are ideal candidates for the AOTS treatment. However, as stated above, osteotomy of the malleolus also brings potential complications.
In a retrospective study by Kim et al., second-look arthroscopy was applied to 52 ankles that had undergone AOTS with medial malleolar osteotomy, and after 13.1 months, the joint surface and graft area of the osteotomized tibia plafond were evaluated. 7 It was reported that the tibial joint surface was regular in 39 ankles and irregular in 13 ankles, and the difference between these two groups was observed to be statistically significant. It can be understood from this that in cases with problem-free union observed radiographically, intraarticular irregularity cannot be discounted and osteoarthritis may develop in the future. The decrease in functional scores in subsequent periods strengthens the hypothesis that it could originate from the medial malleolar osteotomy. Therefore, the triplanar osteotomy is a technique that could minimalize potential joint surface irregularities. The compression strength of the screws applied in malleolar osteotomy fixation may be the main reason of chondral irregularity. When the thickness and cutting angle of the saw selected for osteotomy is considered, it is also possible that the joint irregularity is formed with force.
BMS is obtained with the drilling or microfracture technique described for lesions of limited dimensions. 14 Good results are known to have been obtained with curettage and BMS but some authors have suggested that there is a fibrous structure of the cartilage formed with BMS and joint damage could be renewed in repeated injuries. 1,14 Imhoff et al. reported that worse visual analog scale and AOFAS scores were obtained in the group where OLT drilling (BMS) was applied before AOT surgery compared with a group where OATS was applied in the first stage without drilling. 16
According to the brief literature search made in the planning of this study, although an absolute treatment protocol has not been defined in the OLT treatment, arthroscopic curettage and BMS are primarily preferred. 1,7 In cases of failure, techniques such as OATS, allograft and autologous chondrocyte implantation (ACI) are applied. 1,15,18 As ACI is a more expensive technique and OATS has morbidity rates reaching 36% in the knee and ankle, there is a clear need for new developments in the OLT treatment. 1
Limitations of the current study can be said to be the low number of cases, the lack of midterm follow-up data. There was no control group, but its strength was increased as it was a prospectively organized study. The surgical procedures were performed by the same surgeon and the same rehabilitation programme was applied to all patients. OLTs cases were chosen at the same age range with particular etiologic factors. Nevertheless, despite the short follow-up period, the data and rapid recovery obtained demonstrate the success of the technique.
Conclusion
Selection of the ideal osteotomy with good preoperative surgical planning is the most important stage of the treatment. Reaching the OLT area to be grafted with the least damage, stable bone fixation applied as simply as possible, and the application of surgery without disruption of the joint surface are very important for AOTS. With the triplanar osteotomy technique, it is possible to reach 56% of all talus osteochondral lesions and more than 80% of medial dome lesions. Second-look arthroscopic evaluations and MRI examinations could be of guidance for the success of the treatment in subsequent periods. In the light of all these data, the triplanar osteotomy technique can be said to have minimalized the potential complications of malleolar osteotomy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.