
Abstract
Background:
The incidence of anterior cruciate ligament (ACL) injuries in children is increasing. However, no standardized core set of outcome measures exists for evaluating pediatric ACL injuries.
Purpose:
To perform a scoping review of the literature to identify patient-reported outcome measures (PROMs) and objective outcome measures used to evaluate pediatric patients after ACL injury and to classify these in accordance with the International Classification of Functioning, Disability, and Health (ICF) domains.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The literature was systematically searched with the PubMed, EMBASE, CINAHL, and PEDro databases. The inclusion criteria were Danish, Norwegian, Swedish, German, or English language; publication between 2010 and 2018; pediatric ACL injury (patients ≤15 years old); and outcome measures. The selected papers were screened for title, abstract, and full text in accordance with predefined inclusion and exclusion criteria.
Results:
A total of 68 papers (4286 patients; mean ± SD age, 12.2 ± 2.3 years) were included. Nineteen PROMs and 11 objective outcome measures were identified. The most frequently reported PROMs were the International Knee Documentation Committee (IKDC) Subjective Knee Form (51% of studies), Lysholm scoring scale (46% of studies) and Tegner activity rating scale (37% of studies). Additionally, return to sport was reported in 41% of studies. The most frequent objective measures were knee laxity (76% of studies), growth disturbances (69% of studies), range of motion (41% of studies), and muscle strength (21% of studies). With respect to the ICF domains, the IKDC covered all 3 ICF health domains, the Lysholm score covered the Body Structure and Function and the Activity Limitation domains, while the Tegner score covered the Participation Restriction domain. Objectively measured knee joint laxity, range of motion, and muscle strength covered 1 domain (Body Structure and Function).
Conclusion:
Pediatric patients with ACL injury were mainly evaluated subjectively with the IKDC and objectively by knee joint laxity. No consensus exists in the evaluation of children after ACL injury. The majority of applied outcome measures are developed for adults. To cover the ICF health domains, future research needs to consider reliable and valid outcome measures relevant for pediatric patients with ACL injury.
Keywords
The incidence of anterior cruciate ligament (ACL) injuries in children has been steadily increasing through the past 10 years. 82,96 Thus, pediatric ACL injuries have attracted substantial interest in clinical research, and the need for prospective research on outcomes after surgical and nonsurgical treatment has been highlighted. 2 However, to provide a scientific basis that can evaluate the consequences of pediatric ACL injuries, it is imperative to have relevant and valid outcome measures. A review of clinical research on adults with ACL injury found high variability in outcome reporting. 53 Furthermore, a 2017 review on reporting trends in youth ACL reconstructions found diverse definitions of skeletal maturity, inconsistently reported objective outcome measures, and the use of patient-reported outcome measures (PROMs) that were developed and validated for adults. 10 Inconsistent and nonstandardized outcome reporting reduces the possibility of comparing and interpreting results across different studies. It is unknown if the high variability in outcome measures seen in adults and adolescents is present in the literature on pediatric ACL injuries.
It is well documented that an ACL injury can have a large impact on function and health in both a short- and long-term perspective. 97 Ideally, outcome assessment should cover every aspect of function and health in pediatric patients with ACL injury. The World Health Organization has formulated the International Classification of Functioning, Disability, and Health (ICF). 100 The ICF is a standardized framework of health and health-related domains (Body Structure and Function, Activity Limitation, and Participation Restriction) that are considered essential for the overall well-being and health of a person. Whether outcome measures used in pediatric patients with ACL injury cover the different ICF domains has yet to be evaluated. Thus, the purpose of this scoping review was to identify outcome measures reported in the literature on pediatric ACL injuries (patients ≤15 years of age) and to examine how the outcome measures were related to the different ICF domains.
Methods
This scoping review was designed according to the methodological framework presented by Arksey and O’Malley. 3 This framework was further refined, and 5 stages were proposed to be followed when conducting a scoping review: (1) the identification of a research question; (2) finding the relevant studies; (3) the selection of studies to be included in the review; (4) data extraction from the included studies; and (5) assembling, summarizing, and reporting the results of the review. 8
Identification of Research Questions
Two research questions were formulated: (1) Which outcome measures are reported in the literature on pediatric ACL injuries (≤15 years of age)? and (2) How do outcome measures reported in the literature on pediatric ACL injuries relate to the different ICF domains? The decision to study participants with an age ≤15 years was a pragmatic solution to focus on children and not adolescents or adults.
Identifying Relevant Studies
The literature was searched in the following databases: PubMed, EMBASE, CINAHL, and PEDro. The end search date for all databases was November 22, 2018. Two members of the research team (M.H.K., M.B.P.) carried out the literature search in the electronic databases. Inclusion criteria were studies (1) reporting results from clinical interventions or treatment of ACL injury including children with a median or mean age ≤15 years; (2) published in the period from 2010 to 2018; and (3) published in Danish, Norwegian, Swedish, German, or English. Exclusion criteria were (1) animal or anatomic studies, (2) reviews/meta-analyses, (3) patients with additional knee injuries (except for meniscal injury), and (4) patients with avulsion fractures. On the basis of the inclusion and exclusion criteria, we constructed a search matrix, which was as follows for PubMed searches: (ACL OR “anterior cruciate ligament” OR “Anterior Cruciate Ligament”[MeSH] OR “Anterior Cruciate Ligament Reconstruction”[MeSH]) AND (“Child”[MeSH] OR “Adolescent”[MeSH] OR “Pediatrics”[MeSH] OR preschool* OR pediatric* OR adolescent* OR child* OR prepubescent*). We customized this matrix for searches in the 3 other databases.
Study Identification
Two members of the research team (M.H.K., M.B.P.) screened all identified studies and removed all duplicates, all studies published earlier than 2010, and those that did not meet the language inclusion criteria. The remaining studies were then screened for eligibility by 5 members of the research team (M.H.K., M.B.P., M.K.Z., S.W., T.A.). Two persons screened the title and abstract of each study independently, and in case of disagreement a third person from the research team was consulted to determine the eligibility. Finally, the full-text of the remaining studies were reviewed for eligibility by 2 persons, and conflicts were resolved by asking a third person. In every case of conflict, it was possible to reach consensus through this procedure. M.H.K. or M.B.P. scrutinized the reference lists of all the included studies to identify studies that did not appear in the searches of the electronic databases. In case new studies were identified, these underwent the same screening procedure as described and were termed “additional records identified through other sources” (Figure 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Data Extraction
Data extraction for each eligible study was performed independently by 3 reviewers (M.K.Z., T.A., S.W.) with a predefined spreadsheet. The reviewers’ spreadsheets were then merged to create an agreed-upon extraction form. The standardized data extraction form included details such as study focus, study design, evidence level, authors and country, participant details, and outcome measures (patient-reported and objective outcomes).
Data Analysis
All analyses were performed by 2 authors (M.B.P., M.K.Z.) and verified by 2 authors (S.W., T.A.). The analyses performed were assessment of the variability and frequency of outcome measures, division into patient-reported and objective outcome measures, outcome measures reported per study, research groups, level of evidence, 71 and classification of outcome measures according to ICF domains. 100 Data are presented as numbers of studies, percentage of studies, and mean ± SD where relevant.
ICF Domains
Outcome measures were classified according to the following ICF domains
100
: (1) Body Structure and Function: Impairments in body structure are problems with the anatomic feature of the body, whereas impairments in body function are problems with the function of the body system. (2) Activity Limitation: This domain refers to the difficulties that an individual may have in executing activities. (3) Participation Restriction: This domain includes normal daily activities, such as working, engaging in social and recreational activities, and obtaining health care and preventive services.
The classification was carried out independently by 2 physical therapists of the research team (S.P.M., M.H.K.) and verified by a third physical therapist who was not a member of the research team.
Results
Included Studies
As Figure 1 demonstrates, 12,689 citations were identified through the search strategy. Sixty-eight papers fulfilled the inclusion criteria # and were included in the review. In total, 4286 patients with a mean age of 12.2 ± 2.3 years were evaluated in the 68 studies included. In 60 studies, surgery/reconstruction was evaluated as treatment; in 3 studies, conservative treatment was evaluated; and in 5 studies, both treatments were evaluated.
In total, 22 scientific journals were represented among the included studies (Table 1). The most frequent journals were Knee Surgery, Sports Traumatology, Arthroscopy (14 studies), Journal of Pediatric Orthopaedics (9 studies), and The American Journal of Sports Medicine (9 studies). The review included 8 studies with an evidence level of 5, 50 level 4 studies, 9 level 3 studies, and 1 level 2 study. On average, 8 ± 3 outcome measures were reported per study, and 85% of the studies used a combination of objective and subjective outcome measures in the evaluation of knee function.
Journals of the Included Studies

Patient-Reported Outcomes
In total, 19 PROMs were identified in this scoping review (Figure 2). The most frequently reported questionnaires were the International Knee Documentation Committee (IKDC) Subjective Knee Form 35 (51%), the Lysholm scoring scale 90 (46%), and the Tegner activity rating scale 9 (37%), respectively. Knee pain, specifically evaluated as an isolated measure, was assessed and reported in 32% of the studies. The most frequently used outcome for knee pain was a simple yes/no question (9 of 68 studies), followed by visual analog scale score (4 of 68 studies) and numeric rating scale (2 of 68 studies). In 41% of the studies, return to sport was used as a follow-up outcome measure.
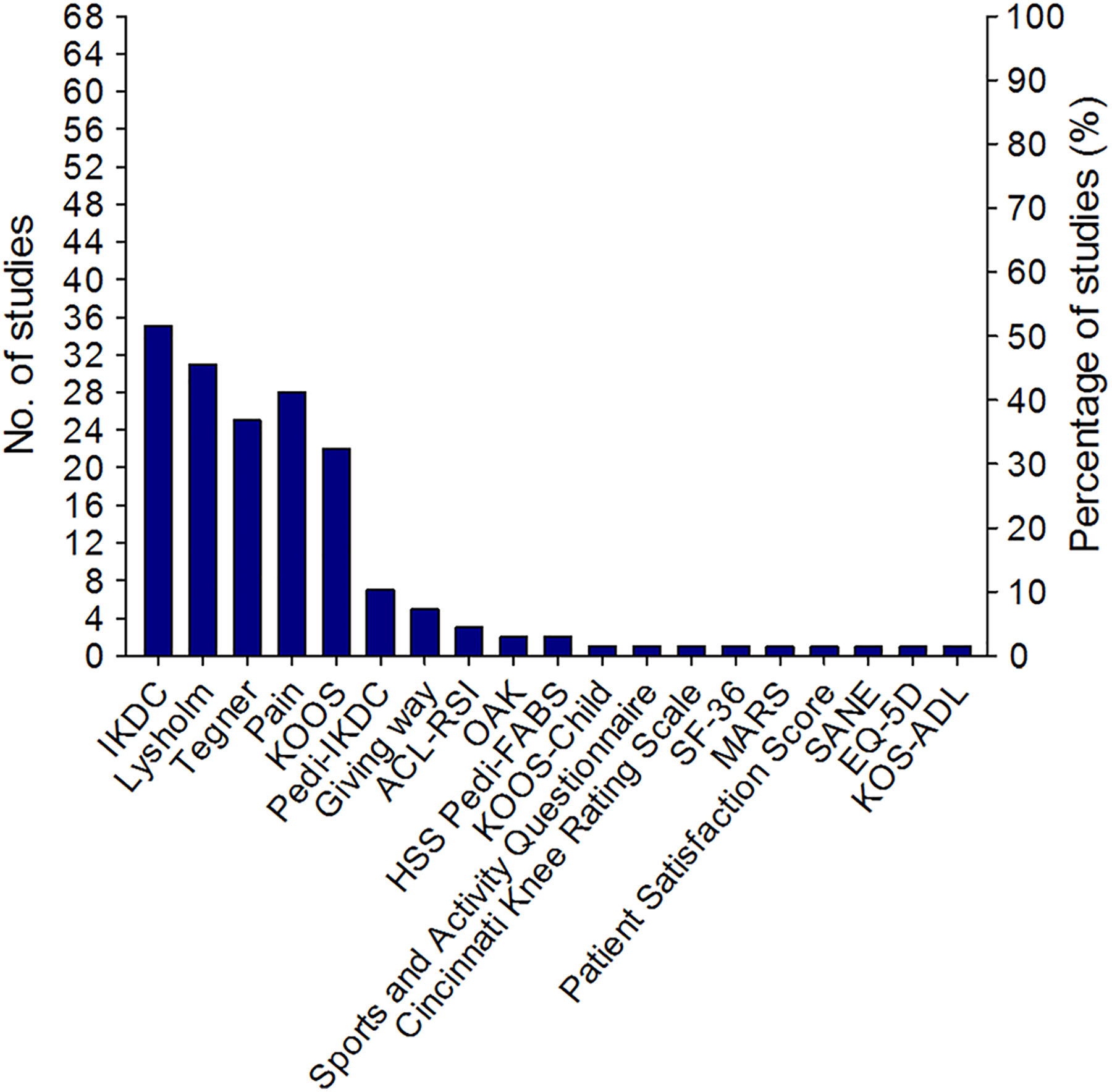
Patient-reported outcome measures. ACL-RSI, ACL–Return to Sport After Injury Scale 95 ; EQ-5D, European Quality of Life–5 Dimensions 86 ; HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale 22 ; IKDC, International Knee Documentation Committee 35 ; KOOS, Knee injury and Osteoarthritis Outcome Score 79 ; KOOS-Child, Knee injury and Osteoarthritis Outcome Score for Children 70 ; KOS-ADL, Knee Outcome Survey–Activities of Daily Living 36 ; MARS, Marx activity rating scale 55 ; OAK, The Orthopädische Arbeitsgruppe Knie Score 65 ; Pedi-IKDC, Pediatric International Knee Documentation Committee 41 ; SANE, Single Assessment Numerical Evaluation 88 ; SF-36, 36-Item Short-Form Health Survey. 94
Three of the identified PROMs were specific measures for pediatric patients—that is, the Pedi-IKDC, 41 Knee injury and Osteoarthritis Outcome Score for Children (KOOS-Child), 70 and the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS). 22 These PROMs were used in 5, 40,61,93,98,99 1, 85 and 1 16 of the 68 studies, respectively. Of the 5 studies including the Pedi-IKDC as an outcome measure, 1 was published in 2013, 61 1 in 2015, 98 1 in 2017, 93 and 2 in 2018 40,99 .
Objective Outcome Reporting
In 76% of the studies reviewed, knee laxity was a reported objective outcome. Knee laxity tests included instrumented assessment in 35 studies (51%), Lachman testing in 32 (47%), pivot-shift testing in 28 (41%), and anterior drawer testing in 6 studies (9%). Of the 35 studies reporting instrumented knee laxity outcomes, the majority used KT arthrometers (29 studies). Range of motion (ROM) was reported in 41% of the studies reviewed. Isokinetic muscle strength was reported in 14 studies (21%); quadriceps muscle strength was reported in all 14 studies and hamstring muscle strength in 11 of the 14 studies. The Limb Symmetry Index was reported in 8 of the 11 studies.
With respect to functional testing, 12 studies (18%) reported hop test outcomes. Of these, 10 studies reported the single-legged hop test for distance, and 6 studies reported the single-legged triple-hop test. Additionally, crossover and vertical hop tests were each reported in 4 studies. The Functional Movement Screen test, 60 which consists of 7 dynamic tests, was reported in 2 studies. The remaining objective outcomes were found in 1% of the studies reviewed (Figure 3).

Objective outcome reporting. ROM, range of motion.
Adverse Events
In total, 59 studies reported adverse events as an outcome. In terms of follow-up outcome measures, 69% of the included studies reported growth disturbance, 40% reported reinjury, and 22% reported reoperation.
ICF Domains
The most frequently used outcome measures within the ICF Body Structure and Function domain were laxity testing, ROM, and muscle strength testing (Table 2). The IKDC 35 and the Pedi-IKDC 41 address aspects of physical impairment but they also evaluate the domains Activity Limitation and Participation Restriction. The IKDC and Pedi-IKDC questionnaires provide information about symptoms, daily activity, and sports function owing to a variety of conditions affecting the knee, including ligament injuries. Additional outcome measures that can be allocated to the ICF domain Body Function and Structure include the Lysholm scoring scale, 90 which assesses knee function after knee ligament injury. The scale consists of 8 items: pain, instability, locking, swelling, limp, stair climbing, squatting, and need for support. The Lysholm test also covers the domain Activity Limitation. Functional testing (eg, hop testing) covers the domain Activity Limitation. Information linked to the ICF domain Participation Restriction includes the Tegner activity rating scale. 9
ICF Domain Classification for Commonly Used Outcome Measures in Pediatric ACL Injury Rehabilitation a

a Parentheses represent ICF codes. 100 ACL, anterior cruciate ligament; ICF, International Classification of Functioning, Disability, and Health; IKDC, International Knee Documentation Committee; LSI, Limb Symmetry Index; PROM, patient-reported outcome measure.
b Out of 68 total.
Discussion
The aim of this study was to provide an overview of outcome measures utilized after pediatric ACL injury and to examine how these relate to the 3 domains of the ICF. We included 68 studies published in a variety of international peer-reviewed journals, including journals that address orthopaedic surgeons, team physicians, athletic trainers, and physical therapists specializing in sports medicine (eg, The American Journal of Sports Medicine) and journals mainly addressing specialist orthopaedic surgeons (eg, The Journal of Bone and Joint Surgery).
The level of evidence in most of the included studies (58 of 68) was low. We identified 1 level 2 study and no studies of level 1. This concurs with previous observations. 10,62 In contrast, Makhni et al 53 found that 50% of the included studies in a review of the adult ACL reconstruction literature were level 1 or 2 studies.
We did not find any standardized outcome measure for pediatric patients with ACL injury consistently utilized across the included studies. The majority of the outcome measures were identical to those used among the adult population with ACL injury, 53 which have not been developed and validated for pediatric patients undergoing treatment and rehabilitation after ACL injury.
It is important to stress that we decided to include ACL injury studies with patients of a median or mean age of maximum 15 years. As such, some of these patients may have been skeletally mature. However, the mean age of the 4286 patients was 12.2 ± 2.3 years—thus, it is likely that the majority of the patients were skeletally immature.
This scoping review found the IKDC to be the most commonly used PROM, appearing in 51% of studies, followed by the Lysholm score (46%) and the Tegner score (37%), which demonstrates that the most commonly reported PROMs are not specifically developed for pediatric patients with ACL injury. A similar reporting pattern was found in a review of youth ACL reconstruction studies. 10
Overall, the present review identified only 3 PROMs that were specifically developed for pediatric patients with knee disorders in general—the Pedi-IKDC, KOOS-Child, and HSS Pedi-FABS. The Pedi-IKDC and KOOS-Child questionnaires are adapted from their adult versions, which are PROMs designed to assess self-reported knee function. The Pedi-IKDC has demonstrated overall acceptable psychometric performance for outcome assessment of children and adolescents from 10 to 18 years of age with various disorders of the knee. 41 Likewise, the KOOS-Child has demonstrated good psychometric properties in 7- to 16-year-old children with knee disorders. 69 In a consensus statement by Ardern et al, 2 the Pedi-IKDC and KOOS-Child were suggested as appropriate PROMs for children with ACL injury. In our review, only 5 studies used the Pedi-IKDC, and 1 study used the KOOS-Child. This finding is in accordance with the review by Brusalis et al 10 on youth ACL reconstruction studies, who found that the Pedi-IKDC was reported in only 1 of the 17 included studies. The 8-item HSS Pedi-FABS is a reliable and valid metric to assess activity in children and adolescents 10 to 18 years of age. 22 This PROM was reported in only 1 of the included studies. Thus, although pediatric-specific PROMs exist, the present review indicates that they are not commonly used in clinical research.
The explanation for the lack of pediatric-specific PROMs in research may be that the Pedi-IKDC was first described by Kocher et al 41 in 2011, the KOOS-Child in 2012 by Örtqvist et al, 70 and the HSS Pedi-FABS in 2013 by Fabricant et al. 22 Hence, the present review may not give an accurate description of the use of these PROMs in clinical practice and research today. In support of this, a survey among European Society for Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA) members revealed that 15% of the respondents reported the use of the Pedi-IKDC and 14% used the KOOS-Child. 64 Thus, it is reasonable to expect that the use of validated pediatric PROMs may be more common in the clinical setting and research today than our review indicates. Nevertheless, the recent consensus statement highlights the need for standardized, pediatric-specific PROMs to be applied in future studies evaluating the treatment of children and adolescents after ACL injury. 2 To our knowledge, no studies so far have evaluated the long-term outcomes after pediatric ACL injury, including the risk of developing knee osteoarthritis. Thus, the need for reliable and valid outcome measures that can be applied in both childhood and adulthood seem warranted.
Return to sport has been found to be one of the most important outcomes to adult patients undergoing ACL reconstruction. 38 In our review, return to sport following ACL injury treatment in children was reported in 41% of the included studies. In comparison, Makhni et al 53 found that return to sport following ACL injury in adults was reported in 24% of the studies included. The authors advocated for increased and enhanced reporting of return to sport from both a patient care perspective and a research perspective. It seems reasonable to advocate for this outcome measure in pediatric patients with ACL injury as well. A frequently used PROM to specifically measure psychological readiness to return to sport after ACL injury and reconstruction surgery is the Anterior Cruciate Ligament Return to Sport After Injury scale (ACL-RSI), 95 which was developed and published in 2008. In our review, this scale was identified as an outcome measure in 2 of the included studies—both published in 2018. 40,99 The psychological aspect of return to sport is important to include in the evaluation of the pediatric patient; however, to our best knowledge, the current version of the ACL-RSI was not developed for children and has not been validated in pediatric patients, which is why future work should address this issue.
The most commonly used objective measures were knee joint laxity (76%) and ROM (41%). Knee joint laxity was most frequently measured with the Lachman test (32 studies) performed by the clinician and/or by the use of instruments (35 studies). Of the 35 studies reporting instrumented knee joint laxity, 29 studies used the KT instruments. As the KT instruments are not customized for children 44 and the variety of knee joint laxity testing techniques is substantial, the need for agreement on a reproducible and standardized objective measurement of ACL laxity in pediatric patients is emphasized. Furthermore, muscle strength testing in pediatric patients with ACL injury was reported in only 14 of 68 studies (21%), which seems remarkably low since both quadriceps and hamstring muscle strength is important for dynamic knee joint stabilization 5 and likely important for future outcome after ACL injury.
It is highlighted in the pediatric ACL injury literature that it is essential when surgical treatment is undertaken to include appropriate measures of skeletal development both pre- and postoperatively. 64 In our review, the majority of the studies evaluated surgery as one of the applied treatments (65 of 68 studies), but growth disturbances were assessed in only 47 (69%) of these studies. In addition, the surgical techniques are highly diverse, and consensus could not be reached in a recent survey among orthopaedic surgeons in pediatric ACL injuries. 64 Thus, clinical guidelines on surgical treatment in relation to skeletal development seem difficult to provide.
ICF Domains
The analysis of how the identified outcome measures were related to the ICF model revealed that while the domain Body Function and Structure are well covered, only a few of the measures cover Activity Limitation and Participation Restriction. Table 2 provides insight that may be useful when selecting outcome measures in future studies. The IKDC/Pedi-IKDC captures all 3 ICF domains and is one of the instruments most commonly used to determine results following various knee procedures, including ACL reconstructions. 28 Oak et al 68 found no clinically significant difference between scores on the Pedi-IKDC versus the adult IKDC in adolescents aged 13 to 17 years. The authors concluded that if the adult questionnaire is used in adolescent patients, it can be consistently used during long-term follow-up. In contrast, it has been found that children had difficulties in comprehending several aspects of the adult form of the IKDC. 37 Thus, the question stands if the adult form can be used longitudinally or if the pediatric version (specifically validated for this age group 73 ) should be used during childhood and later exchanged with the adult version.
All the outcome measures that we identified in the present scoping review may be useful for describing knee function. However, as long as no standardized core set of outcome measures exists to evaluate pediatric patients with ACL injury, it is difficult to compare results across studies. The consensus statement by Ardern et al 2 addressed this issue, and it is likely that their recommendations will influence future outcome reporting in pediatric ACL injury research in the direction of more uniformity.
Conclusion
The 68 included studies showed that outcome measures developed for adults—namely, the IKDC Subjective Knee Form, the Lysholm scoring scale, and the Tegner activity rating scale—are the most frequently used PROMs in children with ACL injuries. Knee joint laxity was the most frequent reported objective parameter, with the KT instruments as the most commonly used method of assessing passive knee joint laxity. A mean of 8 outcome measures per study were reported, with no uniformity among studies in how to evaluate children after ACL injury. This highlights the need for establishing consensus over a standardized core set, covering all of the ICF health domains, for pediatric patients with ACL injury.
Footnotes
Acknowledgment
The authors would like to thank Linda Fernandes for verifying the ICF classification carried out by the research team.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.