
Abstract
Background:
There are a number of surgical methods for undertaking anterior cruciate ligament (ACL) reconstruction (ACLR), although relatively high rates of ipsilateral retears and contralateral tears exist, with only 65% of patients returning to their preinjury level of sport. ACLR techniques adopting synthetic augmentation have been proposed in an attempt to improve clinical outcomes and reduce reinjury rates.
Purpose:
To determine the efficacy of ACLR using autologous hamstrings augmented with the Ligament Augmentation and Reconstruction System (LARS).
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 65 patients were prospectively treated with arthroscopically assisted single-bundle ACLR using hamstrings augmented with the LARS, of whom 50 were available for 1- and 2-year reviews. Patient-reported outcome measures (PROMs), KT-1000 arthrometer testing, knee range of motion, peak isokinetic knee strength testing, and a battery of 4 hop tests were employed. Limb symmetry indices (LSIs) were calculated. Analysis of variance was used to evaluate differences over time and between limbs. Data on return to the preinjury level of sport, retears, and reoperations were collected.
Results:
High PROM scores were demonstrated at 1 and 2 years. Before the injury, 47 patients (94%) were actively participating in level 1 or 2 sports, with 38 (76%) and 43 (86%) patients having returned at 1 and 2 years, respectively. Normal (<3 mm; 90%) or nearly normal (3-5 mm; 10%) KT-1000 arthrometer side-to-side differences were observed at 2 years. Apart from knee flexion (P < .0001), extension (P = .001), and the 6-m timed hop (P = .039), there were no between-limb differences at 1 year, and there were no differences on any objective measures at 2 years (all P > .05). Mean LSIs across all measures were ≥90%. At 2 years, 84% to 90% of patients were ≥90% on the hop tests, with 72% and 76% of patients having ≥90% for extension and flexion strength, respectively. Two reoperations were undertaken for meniscal tears (7 and 8.5 months), 1 patient (2%) suffered a retear at 7 months, and 2 patients (3%) suffered a contralateral tear (8 and 12 months).
Conclusion:
This augmented ACLR technique demonstrated good clinical scores, a high rate of return to sport, and low rates of secondary ruptures and contralateral ACL tears at 2 years. Some caution should be noted in interpreting these results, as 15 of 65 patients (23%) were not included in the 2-year follow-up.
Keywords
Surgical reconstruction is considered the standard clinical treatment for anterior cruciate ligament (ACL) tears. 50 Secondary reinjury rates after ACL reconstruction (ACLR) have been estimated at 7%, with 8% of patients also proceeding toward a contralateral ACL tear. 62 ACLR aims to maximize knee stability and functional capacity while permitting a safe return to sport (RTS), 5,7 although a systematic review by Ardern et al 4 reported that only 65% of patients return to their preinjury level of sport after ACLR.
While a number of potential causes of graft failure have been reported, 48 graft choice may be the only modifiable surgical factor for young, active patients wishing to RTS. 11 A growing number of graft options exist for the orthopaedic surgeon, 11 with autografts more commonly employed and appearing superior in terms of clinical outcomes and RTS capacity. 11 During the ACLR graft revascularization phase of healing, reduced strength and stiffness occur, 8,15,61 and successful incorporation (and subsequent maturation and function) of the graft is dependent on this process of graft ligamentization. 1,25 Rehabilitation throughout this phase, therefore, needs to accommodate this process, and early and accelerated pathways can potentially lead to graft laxity, which may be associated with subsequent instability and/or reruptures. 41 Synthetic prosthetic ligaments have been employed to bypass the aforementioned issues, remove donor site morbidity, and permit accelerated rehabilitation and RTS. While a recent 10-year longitudinal study 9 demonstrated satisfactory clinical outcomes and failure rates in patients undergoing primary ACLR employing a synthetic ligament and remnant preservation, excessive synovitis and high failure rates have limited their ongoing use in earlier studies. 26,27,29,36,43,45,63,64
In an attempt to improve clinical outcomes and reduce reinjury rates, particularly in patients with higher activity levels and those seeking an earlier RTS, concomitant extra-articular procedures such as anterolateral ligament reconstruction, 10 as well as methods of ACLR employing an autograft or allograft augmented (or reinforced) with a synthetic device, 14,19,20,49,51 have been proposed. As previously reported by Falconer et al, 14 the proposed advantage of the combined intra-articular autograft/Ligament Augmentation and Reconstruction System (LARS; Corin Group) construct is to permit early ACL reinforcement and accelerated rehabilitation without the increased risk of graft stretching and/or failure. This study presents a remnant-sparing surgical technique for ACLR employing autologous hamstrings augmented with the LARS, together with clinical outcomes for 50 patients who underwent the technique. We sought to investigate the initial safety and efficacy of the surgical technique and to evaluate patient-reported and objectively measured clinical outcomes as well as satisfaction, rerupture, and RTS rates over the first 2 postoperative years.
Methods
Patients
A total of 65 patients underwent ACLR with a hamstring tendon autograft, augmented with a synthetic LARS ligament, for a primary ACL tear between February 2015 and December 2016. All patients were consulted (and underwent surgery) by a single surgeon in a private orthopaedic clinic. The current study included clinical outcomes for 50 patients with a clinical review at both 1 and 2 years postoperatively (Figure 1). Details of the patient sample are provided in Table 1. Patients were invited to participate in the study if they were deemed candidates for surgery, including whether they were skeletally mature and required isolated primary ACLR, with or without concomitant meniscal surgery. Ethics approval was provided by the relevant hospital ethics committee, and the consent of all participants was obtained before the review.

Study flowchart demonstrating patient recruitment and clinical evaluation over the 24-month period. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; LARS, Ligament Augmentation and Reconstruction System.
Characteristics of Patients (N = 50) a

a ACLR, anterior cruciate ligament reconstruction.
Surgical Technique
All surgical procedures were performed by the senior author (P.T.A.) via an arthroscopically assisted single-bundle surgical technique. Gracilis and semitendinosus hamstrings were harvested from the ipsilateral knee through a 2- to 3-cm transverse incision 1 cm above the pes anserinus. The doubled tendons and a doubled 3.5-mm prosthetic LARS ligament (product code 104.133: LARS anterior cruciate reinforcement) were combined for diameter sizing (Figure 2) in all patients. The LARS ligament added 1 mm of graft diameter, generally creating an overall cross-sectional area of approximately 9 mm2. A 20-mm closed-loop Endobutton (Smith & Nephew) was routinely used for femoral graft fixation, with a 25-mm Endobutton employed when the graft diameter exceeded 8 mm. The grafts and LARS ligament were individually looped through the Endobutton and whipstitched to themselves (Figure 3).

The doubled tendons and a doubled 3.5-mm prosthetic LARS (Ligament Augmentation and Reconstruction System) ligament combined in preparation for diameter sizing.

Individual preparation of the grafts and LARS (Ligament Augmentation and Reconstruction System) ligament, looped through the Endobutton and whipstitched to themselves.
Femoral tunnel preparation was performed through an anteromedial portal, allowing anatomic femoral tunnel positioning. A remnant-sparing technique was employed, 2,16 which was recommended to minimize potential particulate wear, avoid synthetic impingement, and optimize autograft ligamentization. Therefore, only unstable remnant tissue was debrided, with all stable ACL remnants and the notch synovium spared, as was the fat pad and ligamentum mucosum. The graft was passaged within the retained remnant, with the LARS ligament lying in a posteromedial relationship to the autograft tendons and anterior to the posterior cruciate ligament. The LARS ligament therefore appeared “hidden” in the notch, minimizing impingement and exposure to the joint (Figures 4 and 5).
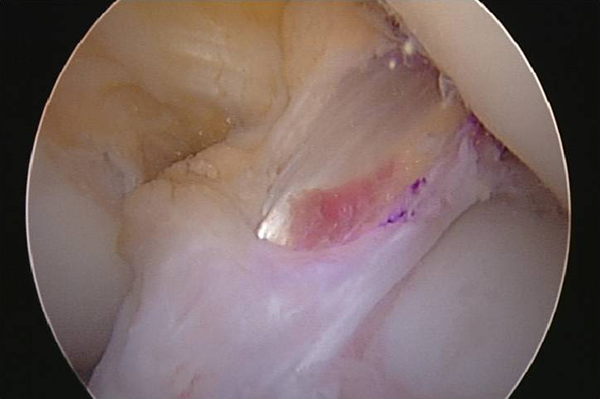
The graft passaged within the retained remnant, with the LARS (Ligament Augmentation and Reconstruction System) ligament lying in a posteromedial relationship to the autograft tendons and “hidden” in the notch, minimizing impingement and exposure to the joint.
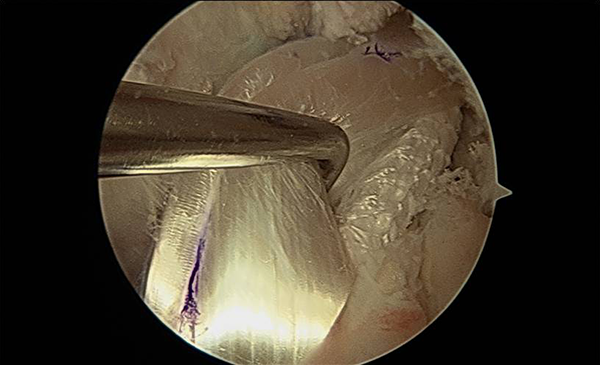
Intraoperative photograph demonstrating exposure of the LARS (Ligament Augmentation and Reconstruction System) ligament after retraction of the hamstring tendon autograft portion of the graft.
Femoral fixation occurred with the Endobutton seated and tensioned with maximal manual tension through 10 cycles of knee flexion. Tibial fixation was performed using Intrafix (DePuy Synthes) with maximal manual tension on the autograft and light tension on the LARS, with the LARS posteromedial to the autografts in full extension (Figure 6). Figure 7 shows final incorporation of the hybrid graft. Postoperative management included early splinting (for 2 weeks, only as a means of reducing movement-associated pain and swelling) and weightbearing as tolerated, with early range of motion (ROM) exercises commencing immediately, and progressive cycling and strengthening exercises being undertaken from 6 to 8 weeks.

Tibial fixation using Intrafix with maximal manual tension on the autograft and light tension on the LARS (Ligament Augmentation and Reconstruction System), with the LARS posteromedial to the autograft in knee extension.

Incorporation of the hybrid graft.
Clinical Assessment
A number of patient-reported outcome measures (PROMs) were undertaken at 1 and 2 years postoperatively. These included the International Knee Documentation Committee (IKDC) subjective knee evaluation form, 23 the Knee Outcome Survey (KOS) Activities of Daily Living subscale, 24 the Knee injury and Osteoarthritis Outcome Score (KOOS), 46 the Lysholm scale, 34 the Tegner activity scale, 52 the ACL–Return to Sport after Injury (ACL-RSI) scale, 57 and the Noyes Sports Activity Rating Scale (NSARS). 40 Furthermore, we used a global rating of change scale to evaluate the patient’s perceived status compared with that before surgery, with scores ranging from –5 (very much worse) to 0 (about the same) to 5 (completely recovered). Satisfaction with the surgical procedure overall was evaluated as well as satisfaction with the surgical procedure to relieve pain, improve the ability to perform normal daily and work activities, improve the ability to return to recreational activities (including walking, swimming, cycling, golf, and dancing), and improve the ability to participate in sport (including sports such as tennis, netball, soccer, and football). A Likert response scale was employed with the following descriptors: very satisfied, somewhat satisfied, somewhat dissatisfied, and very dissatisfied.
Objectively, maximal active knee flexion and extension ROM were initially measured. Graft stiffness was evaluated via the KT-1000 arthrometer (MEDmetric), employed to quantify anterior tibial translation 42 during a maximal manual test; the difference between the operated and nonoperated knees was obtained. Patients underwent a previously validated battery of 4 hop tests in the following order: (1) the single hop for distance, (2) the 6-m timed hop, (3) the triple hop for distance, and (4) the triple crossover hop for distance. 44 Finally, peak concentric knee extension (quadriceps) and flexion (hamstring) isokinetic strength were measured at a single isokinetic angular velocity of 90 deg/s using an isokinetic dynamometer (Isosport). To avoid fatigue, patients were given as much time as they wanted between hop and strength test trials; this time was not standardized and was based on the individual patient’s readiness to proceed.
Data and Statistical Analyses
First, the mean ± standard deviation (range) of all measures (operated and nonoperated limbs) were calculated at 1 and 2 years. The cohort (N = 50) included patients who underwent ACLR alone (n = 25) and those who underwent ACLR in conjunction with meniscal surgery (n = 25). The cohort was assessed collectively, given that independent t tests revealed no difference (P > .05) in characteristics or clinical outcomes between groups. Clinical differences over time (1 and 2 years), as well as between limbs, were assessed via analysis of variance. Limb symmetry indices (LSIs) were also calculated for all hop and strength tests, further categorized by the number and percentage of patients with LSIs <90% and ≥90%. For KT-1000 arthrometer laxity measures, these were further categorized based on the side-to-side difference as normal (<3 mm), nearly normal (3-5 mm), abnormal (6-10 mm), and severely abnormal (>10 mm). 39 Only 49 of 50 patients were included in the KT-1000 arthrometer analysis, with the 1 patient who had undergone prior contralateral ACLR omitted. The NSARS was employed to present the number and percentage of patients participating in level 1 (4-7 d/wk) or level 2 (1-3 d/wk) activities that included jumping, hard pivoting, cutting, running, twisting, and/or turning sports. The number and type of surgical complications, postoperative adverse events, reoperations, and retears (ipsilateral and/or contralateral ACL retears) were presented. Statistical analysis was performed using SPSS software (version 23.0; IBM). Statistical significance was determined at P < .05.
Results
Subjective Assessment
Per the NSARS, 47 patients (94%) were actively participating in level 1 or 2 sports that included jumping, hard pivoting, cutting, running, twisting, and/or turning before the injury. These activities were being undertaken by 38 patients (76%) and 43 patients (86%) at 1 and 2 years postoperatively, respectively. All PROMs demonstrated high scores at 1 year postoperatively, with further significant improvement (P < .05) observed from 1 to 2 years on the IKDC; KOOS subscales of Pain, Symptoms, and Quality of Life; Lysholm scale; and global rating of change scale (Table 2). At 2 years postoperatively, 100% of patients were satisfied with the ability of their surgical procedure to relieve pain, improve activities of daily living, and improve recreational activities, with 49 of 50 patients (98%) satisfied with their ability to participate in sport (Table 3).
Patient-Reported Outcome Measure Scores a
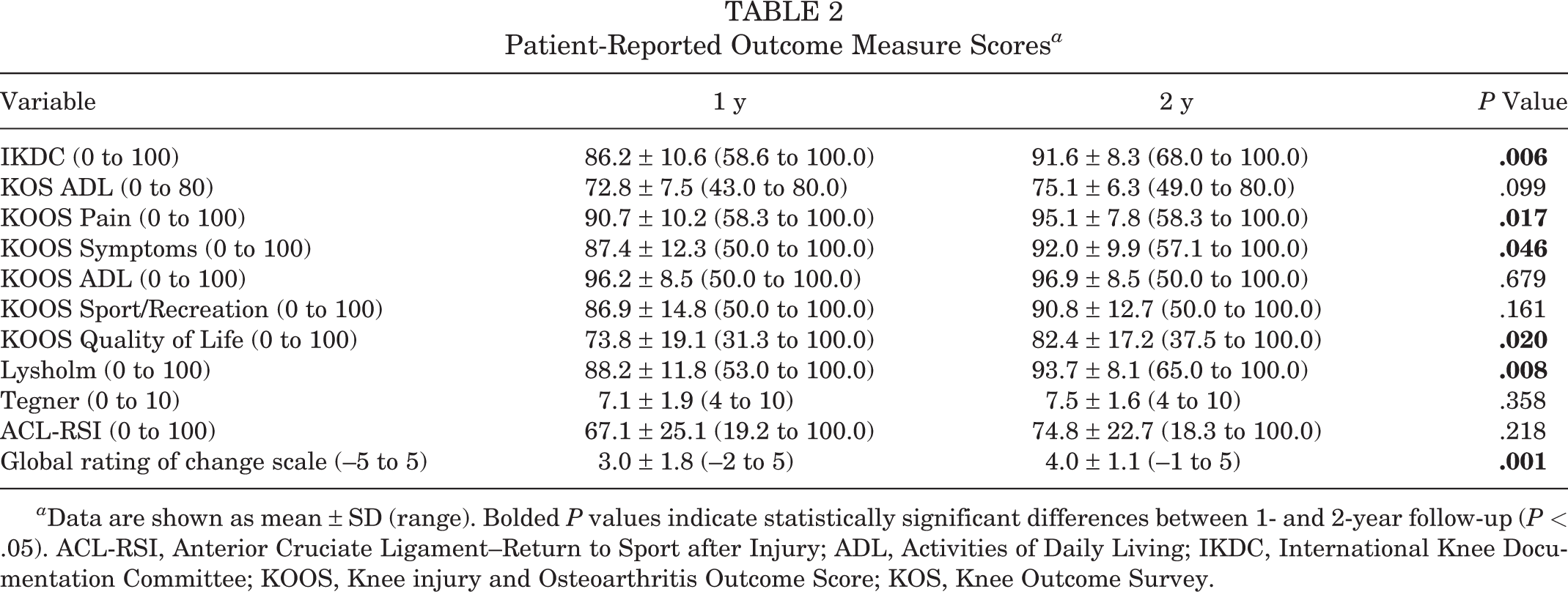
a Data are shown as mean ± SD (range). Bolded P values indicate statistically significant differences between 1- and 2-year follow-up (P < .05). ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; KOS, Knee Outcome Survey.
Patient-Reported Satisfaction Scores at 2 Years Postoperatively a
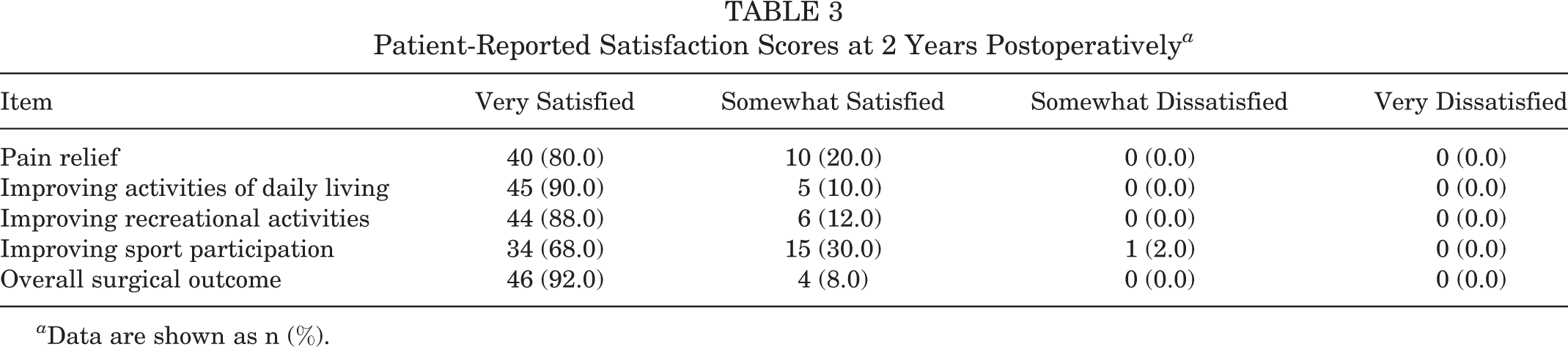
a Data are shown as n (%).
Objective Assessment
KT-1000 arthrometer testing demonstrated normal (44/49; 90%) or nearly normal (5/49; 10%) side-to-side differences at 1 year postoperatively, which were unchanged at 2 years (Table 4). At 1 year postoperatively, active knee flexion (P < .0001) and extension (P = .001) ROM were significantly worse, while the 6-m timed hop was significantly slower (P = .039) in the operated compared with the nonoperated limb. There were no other side-to-side differences at 1 year (Table 5). By 2 years, there were no significant side-to-side differences in any of the objective measures (knee ROM, single-leg hop, or strength) (Table 5). Only active knee flexion ROM significantly improved from 1 to 2 years (P = .023) (Table 5).
KT-1000 Arthrometer Side-to-Side Differences (n = 49) a

a Data are shown as n (%) unless otherwise indicated.
Objective Knee ROM, Single-Leg Hop, and Isokinetic Strength Outcomes a

a Data are shown as mean ± SD (range). Bolded P values indicate statistical significance (P < .05). ROM, range of motion.
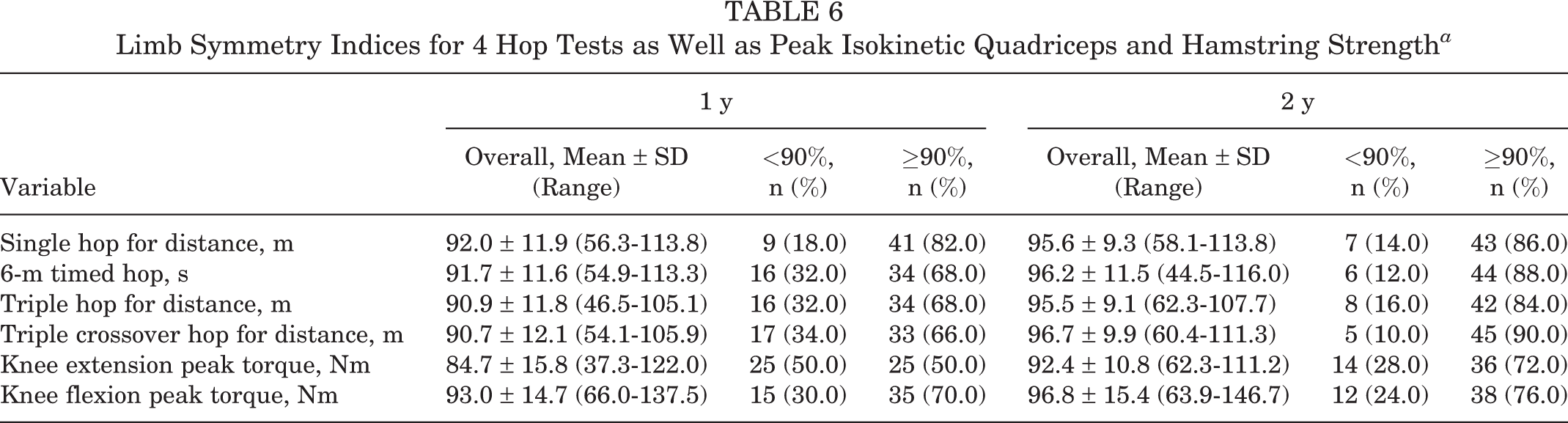
At 1 and 2 years postoperatively, the mean LSIs across all 4 single-leg hop tests and isokinetic strength measures were ≥90% (Table 6). At 1 year postoperatively, 66% to 82% of patients had LSIs ≥90% on the 4 hop tests, with 50% and 70% of patients demonstrating an LSI ≥90% for peak knee extension and flexion strength, respectively. At 2 years postoperatively, 84% to 90% of patients had LSIs ≥90% on the 4 hop tests, with 72% and 76% of patients demonstrating an LSI ≥90% for peak knee extension and flexion strength, respectively (Table 6).
Limb Symmetry Indices for 4 Hop Tests as Well as Peak Isokinetic Quadriceps and Hamstring Strength a
Complications, Reoperations, and Failures
Of all 65 patients who underwent surgery throughout the period (including the 50 patients retained in this analysis with complete 1- and 2-year data), 1 patient had an early wound infection that was treated accordingly without further issue. A further 2 patients underwent secondary surgical procedures, in both cases to debride a torn meniscus at 7 and 8.5 months postoperatively (1 of whom underwent meniscal repair concomitantly with ACLR) and both of whom were largely asymptomatic by 12 months and retained in the 50-patient cohort with complete follow-up data. To better evaluate complication, reoperation, and graft failure rates, all 65 patients who underwent surgery throughout the period were contacted at 1 and 2 years, irrespective of full participation in the follow-up clinical reviews. There were no further complications or subsequent surgical procedures besides those outlined above. However, 1 patient (2%) suffered an ACL retear at 7 months postoperatively because of an accelerated return to higher level activities, while 2 patients (3%) suffered a contralateral ACL tear. These occurred during sport (or sporting activities including training) at 8 and 12 months postoperatively.
Discussion
The use of synthetic ligaments in ACLR was proposed in the 1980s because of their abundant supply and strength, lack of harvest site morbidity, and potential of accelerated rehabilitation and RTS. While various synthetic materials have been employed, 33 excessive synovitis and high failure rates limited their ongoing use. 26,27,29,36,43,45,63,64 However, further work employing the LARS, made of polyethylene terephthalate, reported that under certain conditions, artificial ACLR could be successful. 32,37 Moreover, in vivo and animal studies have suggested that the LARS may permit tissue in-growth properties, 55,56 which, while not necessarily suitable as an ACL replacement, 56 may provide benefit in augmentation as used in the current study. The most important findings from the current study, employing an ACLR technique using a hamstring tendon autograft augmented with the LARS, were the high clinical scores and satisfaction levels, together with comparative side-to-side limb laxity measurements and the high rate of return to preinjury sport levels (86%) by 2 years postoperatively. Furthermore, there were comparatively low ipsilateral retear (2%), contralateral tear (3%), and reoperation (3%) rates, with a relative absence of complications previously reported when employing synthetics such as loss of knee extension and clinical synovitis.
In comparison with other proposed augmented methods, the relative lack of published data makes comparison with the current results employing ACLR with LARS augmentation difficult. Furthermore, the current surgical technique employed remnant preservation, although systematic reviews and meta-analyses have suggested similar clinical outcomes between remnant preservation and debridement methods. 22,35,54 Falconer et al 14 reported on the clinical outcomes of a double-bundle ACLR technique with the anteromedial bundle augmented with the LARS. At a minimum 2-year follow-up, no increase in laxity and a low failure rate were reported, although lower clinical scores and a higher reoperation rate (15.4%) compared with the current cohort were reported. Hamido et al 19,20 reported on the outcomes of augmenting a short and/or undersized hamstring tendon autograft with the LARS. They initially reported the technique to be safe and satisfactory, especially in the presence of a required earlier RTS, 20 and a comparison of outcomes with a 4-strand hamstring tendon autograft revealed comparable PROM scores (albeit better IKDC scores in the augmented LARS group) but a more stable knee with the LARS augmented procedure. 19 There have been 2 other surgical techniques proposed in which FiberTape suture (Arthrex) was employed to reinforce a quadriceps tendon autograft 49 or allograft, 51 although no patient outcomes were reported.
The study patients reported high mean PROM and satisfaction scores. While 100% of patients were satisfied overall, 98% were satisfied with their ability to participate in sport. In the current study, 76% and 86% of patients actually returned to their preinjury level of sport by 1 and 2 years, compared with 94% of patients who were participating in level 1 or 2 sports before the injury. Ardern et al 4 reported that only 65% of patients return to their preinjury level of sport, with 55% returning to competitive sport. A number of factors may be associated with a return to preinjury sport. Physical function may be important, by which patients with perceived “normal” knees (vs nearly normal, abnormal, or severely abnormal) and/or more symmetrical hop performance are more likely to return to their preinjury level of sport. 4 This may be reflected in the current cohort given the high rate of patients with ≥90% LSIs for the hop tests. Psychological readiness to RTS and a lower fear of reinjuries have also been associated with returning to preinjury sport levels, 3 and mean ACL-RSI scores of 67 at 1 year and 75 at 2 years were reported in the current cohort. Interestingly, it has been reported that while patellar tendon autografts may increase the chance of returning to preinjury sport, hamstring tendon autografts may increase the chance of returning to competitive sport. In the current study, it is unknown whether some patients underwent an augmented ACLR procedure with a preconceived idea that it permits an accelerated early recovery and RTS.
The high RTS rates in the current study did not appear to adversely affect anterior laxity or reinjury rates. KT-1000 arthrometer differences were graded “normal” in 90% of patients, with the remaining 10% being “nearly normal.” It has been shown that an elevated retear risk may extend well after the patient’s RTS; Grindem et al 18 reported an increased retear rate up until 9 months postoperatively, after which no further increase in the retear risk was observed. While graft failure may occur because of a number of reasons, including delayed and/or inadequate revascularization of new tissue, earlier RTS may increase the risk of secondary retears, 31 as may returning to higher level sports that involve side-stepping, pivoting, and/or jumping. 18,47,58 Given the majority of patients in this study have returned to their preinjury level of sport, the low incidence of ipsilateral retears and contralateral tears are encouraging. However, it remains important that these patients continue to be followed clinically.
Mean LSIs ≥90% were observed for all hop and strength measures at both 1 year (apart from knee extensor strength) and 2 years postoperatively. This may be an associated factor in the comparably higher RTS rates observed. Single-leg hop tests 21,44 and maximal muscle strength assessments 6,28,38 are often employed to determine physical capacity, commonly reported via LSIs. 53 At 1 year, 66% to 82% of patients demonstrated an LSI ≥90% for each of the 4 hop tests, a finding that had increased to 84% to 90% of patients at 2 years. However, the percentage of patients demonstrating an LSI ≥90% for peak knee extension strength was lower (50% at 1 year and 72% at 2 years). Lower LSIs during peak isokinetic testing (vs functional hop testing) have been previously reported 12,59 and may be more sensitive in detecting side-to-side physical asymmetries.
While existing research has suggested an increased reinjury risk if patients do not meet strength and hop test LSIs of ≥90%, 18,30 the current findings suggest that many patients returned to sport at 1 and/or 2 years without adequately meeting currently recommended strength criteria (quadriceps symmetry ≥90%). Despite the low reinjury rates observed, the majority of patients in this study did not undergo a formal test battery before their RTS. Interestingly, another study investigating outcomes in a community-level cohort of patients who underwent ACLR with a hamstring tendon autograft reported significant side-to-side differences on all hop and strength measures at 10 to 14 months, together with mean LSIs that were generally <90%. 12 In that cohort, only 57 of 111 (51%) returned to level 1 or 2 sports, although the mean LSIs were generally ≥90% in patients specifically participating in these sports. This further highlights the aforementioned association between physical capacity and the incidence of postoperative RTS.
A number of limitations exist within the present study. First, it was a prospective study with no comparative group, given the nature and preliminary use of this augmented surgical technique. Nonetheless, despite the encouraging pilot outcomes and the justification that this provides for a randomized controlled trial, the large body of ACLR research that currently exists permitted us to compare our findings with historical outcomes. Second, this pilot case series was performed exclusively with a clinical review, and no magnetic resonance imaging or second-look arthroscopic surgery was undertaken. Synthetic ligaments have previously been shown to cause graft tunnel widening and joint synovitis. While this could have been assessed in the current series, there was no clinical evidence of synovitis. Falconer et al 14 found no evidence of tunnel widening or synovitis on postoperative magnetic resonance imaging at a mean 2.42-year follow-up in patients with combined LARS/hamstring tendon grafts for ACLR. Furthermore, we could not evaluate the incidence of partial retears, although clinical KT-1000 arthrometer measures at 1 and 2 years postoperatively suggested satisfactory graft stability (90% normal and 10% nearly normal).
Third, as mentioned above, we did not assess the actual time to RTS but rather whether patients returned by 1 or 2 years. Actual RTS timing is difficult given that there are other factors that may determine timing out of the patient’s control, such as the fact that RTS (and competitive sport) may be dictated by the playing season. Fourth, it is acknowledged that the level of rehabilitation can affect strength and function after ACLR 13,17 and subsequently RTS ability. While a general rehabilitation plan was provided, this was a community-level cohort of patients (none of whom were elite athletes) that were provided guidance and rehabilitation from an array of physical therapists. Therefore, despite the encouraging strength and functional LSIs observed at 1 and 2 years, together with the comparably higher RTS rates, the rehabilitation among patients differed in content, frequency, and duration and was not closely assessed or strictly standardized. Furthermore, the inherent limitations with using LSIs to report postoperative strength and functional outcomes are acknowledged, 60 although these still remain the most common way of reporting objective measures and provide an effective means of comparing outcomes with that of other studies. Finally, caution should be noted in interpreting these results, as 15 of the original 65 patients (23%) were not included in the 2-year follow-up.
Conclusion
This augmented ACLR technique demonstrated good clinical outcomes, high levels of satisfaction including the ability to participate in sport, and a high rate of return to preinjury sport. In addition to the high rate of RTS compared with that reported in the literature, comparative side-to-side limb laxity measurements were observed, with a low rate of secondary ipsilateral ACL ruptures and/or contralateral ACL ruptures, again compared with the existing literature. Ongoing and close follow-up of this ACLR technique (and other novel and varied surgical techniques) is required to ascertain any longer term benefit to patient outcomes, reinjury rates, and participation in activity, often a primary outcome of the surgical procedure.
Footnotes
One or more of the authors declared the following potential conflict of interest or source of funding: Independent funding in the form of a research grant was provided by Corin Group to assist this research. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethics approval was obtained from the Hollywood Private Hospital Research Ethics Committee (HPH382).