
Abstract
Background:
Chondral and osteochondral lesions are being detected with increasing frequency. For large-diameter lesions, cell-based treatment modalities are speculated to result in the best possible outcome.
Purpose:
To prospectively evaluate the 2-year clinical and radiological results after the treatment of chondral and osteochondral knee joint lesions by a single-step autologous minced cartilage procedure.
Study Design:
Case series; Level of evidence, 4.
Methods:
From February 2015 to June 2016, a total of 27 consecutive patients suffering from chondral or osteochondral lesions of the knee joint were treated using a single-step autologous minced cartilage procedure. All patients underwent preoperative and postoperative magnetic resonance imaging for the collection of AMADEUS (Area Measurement and Depth and Underlying Structures) and MOCART (magnetic resonance observation of cartilage repair tissue) scores. Clinical analysis was conducted by a numeric analog scale (NAS) for pain and knee function before the intervention and at 12 and 24 months postoperatively.
Results:
A total of 12 female and 15 male patients (mean age, 28.7 years) were evaluated for a mean of 28.2 ± 3.8 months. The mean cartilage defect size encountered intraoperatively was 3.1 ± 1.6 cm2. There was a significant decrease in pain from 7.2 ± 1.9 preoperatively to 1.8 ± 1.6 (P < .001) at 2-year follow-up. Knee function improved from a mean of 7.2 ± 2.0 preoperatively to 2.1 ± 2.3 (P < .001) at 2 years after surgery. The mean preoperative AMADEUS score was 57.4 ± 21.4. Postoperatively, the mean MOCART score was 40.6 ± 21.1 at 6-month follow-up. No correlation was observed between the clinical data and the MOCART or AMADEUS scores.
Conclusion:
Overall, the findings of this study demonstrated that patients undergoing a single-step autologous minced cartilage procedure had a satisfactory outcome at 2-year follow-up. As a result, the single-step autologous minced cartilage procedure does represent a possible alternative to standard autologous chondrocyte implantation. Longer follow-up and larger cohorts are required to define the benefits of this procedure.
Keywords
Chondral and osteochondral lesions of the knee are predisposing factors for premature osteoarthritis and represent an increasing challenge in knee surgery. 25,35,49 There is growing evidence that repair tissue (RT) quality is related to clinical outcomes. 11,35 Foremost, long-term durability, return to normal knee function, and return to sporting activity are the criteria that are considered relevant when treating joint surface abnormalities. 5 The probability of generating the highest possible RT quality, hyaline or hyaline-like cartilage, is connected to cell-based cartilage repair techniques. 42 These include autologous chondrocyte implantation (ACI) and autologous particulate cartilage chips. 7,41
Standard ACI is hampered by the requirement of 2 interventions, a high cell-producing cost, and questionable chondrocyte function as well as phenotype at the time of implantation. 14,35,46 ACI is not available in every country and represents a constant target of national regulations in countries where it is available. A possible alternative to ACI is the application of small cartilage chips that have been previously particulated or minced. Such a technique was first described by Albrecht 1 in 1983 and has been further developed in recent years. 24,44 Since then, many different authors have added to the current evidence when using particulate cartilage chips. 8,41,44 Their advantage over ACI is that they can be applied in a single surgical procedure, do not require a cell culture or a separate scaffold to apply, and are implanting non-dedifferentiated autologous chondrocytes. 4,41,44
The purpose of this study was to show the clinical and radiological results of patients undergoing a 1-step autologous minced cartilage procedure for the treatment of chondral and osteochondral lesions with a follow-up of at least 2 years.
Methods
Study Design
This was a retrospective registry study with a prospective follow-up. It was approved by the local ethical committee of the Canton of Zurich (KEK-ZH-Nr. 2015-0258). Every patient signed an informed consent form before inclusion in this study.
Patient Selection
The study was conducted at a single specialized orthopaedic clinic. Patients between 18 and 40 years of age suffering from a chondral or osteochondral lesion of the knee between February 2015 and June 2016 were identified through the clinical database. The results of the database search were reviewed by 2 of the investigators (C.R.I., G.M.S.). Included in this study were all patients who underwent surgical treatment by an autologous minced cartilage procedure for a unilateral chondral or osteochondral lesion sized 1 to 6 cm2 at the femoral condyles or the patella. All included patients were contacted via telephone for postoperative clinical evaluation.
Treatment Regimen
All patients included in this study underwent the same type of autologous minced cartilage procedure. The decision for the surgical treatment of chondral and osteochondral lesions at our clinic is made according to the standards of ACI, as have been described by Niemeyer et al. 35 Therefore, at our clinic, surgical treatment is recommended for lesions larger than 2 cm2, as these are considered large, 19,36 and for smaller osteochondral lesions in young and very active patients when intraoperative findings do not allow surgeons to perform osteochondral autograft/allograft transplantation (OATS) or microfracture. Acute posttraumatic chondral or osteochondral fragments and osteochondritis dissecans lesions that cannot be internally fixated but have a healthy-appearing cartilage layer are indications as well.
All procedures were carried out by a single specialized knee surgeon (G.M.S.) and were started with diagnostic arthroscopic surgery of the index joint where the final indication was given. If an intra-articular co-abnormality was detected that could be addressed by the use of arthroscopic techniques (ie, partial meniscectomy), it was treated during the same procedure.
Hereafter, medial or lateral arthrotomy (according to the location of the lesion) was performed, and the lesion was repaired using the second-generation autologous minced cartilage repair technique, as previously described in detail. 44 First, the lesion was inspected and measured. In the next step, the defect was excised with a scalpel, and the damaged or unstable cartilage parts were debrided until a healthy surrounding cartilage wall was achieved. The defect size was documented again. The cartilage retrieved from areas marginally defective or from osteochondral cylinders taken from the low weightbearing intercondylar notch was then minced into fragments of about 1 × 1 × 1 mm with the use of several fresh scalpels until a paste-like appearance was achieved. The minced cartilage parts were placed in the defect and covered with fibrin glue. An example of the procedure is given in Figure 1. 44

Intraoperative images of an exemplary case at the medial femoral condyle treated with the autologous minced cartilage procedure. (A) Cartilage lesion after debridement. (B) Minced cartilage chips after fibrin glue fixation within the defect. (C) Final result after (optional) coverage with the Chondro-Gide membrane.
For patellar and trochlear defects, the Chondro-Gide membrane (Geistlich Pharma) was used to cover the fibrin-associated chips to prevent them from dislocating. For femoral condyle defects, isolated fibrin glue fixation was applied in most cases. Other treatments for extra-articular co-abnormalities (ie, patellar stabilization or mechanical axis correction) were also carried out during the same procedure.
Postoperatively, the knee was put in a straight knee brace and rested for 24 hours. Next, the rehabilitation regimen was initiated according to previously published protocols. 32 Patients underwent 6 weeks of partial weightbearing on crutches, limited range of motion depending on the defect location, and the use of a continuous passive motion machine. Afterward, a stepwise increase of range of motion and weightbearing was allowed through the following 3 to 4 weeks.
Clinical Data Collection
Demographic information and the results of a standardized preoperative clinical examination were collected retrospectively from the patients’ records. The clinical outcome was evaluated by a numeric analog scale (NAS) for pain as well as for subjective knee function at 12 and 24 months postoperatively. The scale ranges from 0 (no pain/best function) to 10 (worst pain/worst function).
Radiological Data Collection
Before surgery, all patients underwent standard radiography of the index joint including long-standing hip-knee-ankle radiographs to analyze leg axis dimensions and to decide if any co-abnormalities (eg, correction of the mechanical axis) needed to be addressed during the surgical treatment of the cartilage defects. Furthermore, magnetic resonance imaging (MRI) was performed for soft tissue and (osteo)chondral analysis and final decision making. All MRI analyses were performed at our institution with 3-T MRI and proton density, turbo spin echo, and T2 sequences.
For the quantification of defect severity, the AMADEUS (Area Measurement and Depth and Underlying Structures) scoring system was applied. 20 It includes the 3 most important parameters that describe a focal chondral or osteochondral defect before possible cartilage repair: (1) the size of the cartilage defect area (“area measurement”), (2) the cartilage defect morphology/depth (“depth”), and (3) the underlying structures with the presence of adjacent osseous defects/subchondral cysts and bone marrow edema–like lesions (“underlying structures”). The AMADEUS score ranges between a total of 100 (no osteochondral defect) and 0 (worst score).
Six months after the intervention, all patients underwent MRI again. The resulting RT was classified using the MOCART (magnetic resonance observation of cartilage repair tissue) scoring system. 26 The MOCART score quantifies hyaline cartilage or the best achievable RT as being 100 points, while the worst RT results in 0 points. The MRI analysis was conducted by a single radiologist not involved in this study who was blinded to all patients.
Statistical Analysis
Statistical analysis was performed using SPSS (version 22; IBM). All data were tested for normal distribution using the Shapiro-Wilk normality test. Afterward, data were compared using the t test, the Mann-Whitney U test, and the Wilcoxon signed-rank test. For a comparison of specific MRI values, the Wilcoxon test was used. Group data were compared using 1-way analysis of variance or Kruskal-Wallis analysis. Differences between groups of patients and defect locations were evaluated using 1-way analysis of variance for all parametric data, such as the NAS scores. Correlations were performed using the Spearman correlation coefficient (r). After using the chi-square test to determine independence, linear regression analysis was conducted to analyze the effects of patient and/or defect characteristics. Hereby, the influence of defect size, age, body mass index, and duration of symptoms was tested on total AMADEUS and MOCART scores as well as preoperative and postoperative pain NAS score. All statistical tests were 2-sided unless otherwise stated, and descriptive results are demonstrated as mean ± SD. The significance level was defined as P < .05 for all tests.
Results
Patients and Demographics
In total, 27 patients were included in this study. There were 12 female and 15 male patients. The mean age at the time of surgery was 28.7 ± 11.2 years (range, 15-50 years). The mean follow-up period was 28.2 ± 3.8 months. No patient dropped out before the final follow-up. The mean body mass index was 23.9 ± 3.6 kg/m2 (range, 14.9-32.1 kg/m2). There were 7 (25.9%) smokers. An overview of the demographics is given in Table 1. Five patients (18.5%) had undergone previous surgery on the same knee, whereas none had undergone a previous surgical intervention for the index lesion.
Patient Demographics (N = 27) a

a Data are presented as mean ± SD unless otherwise specified.
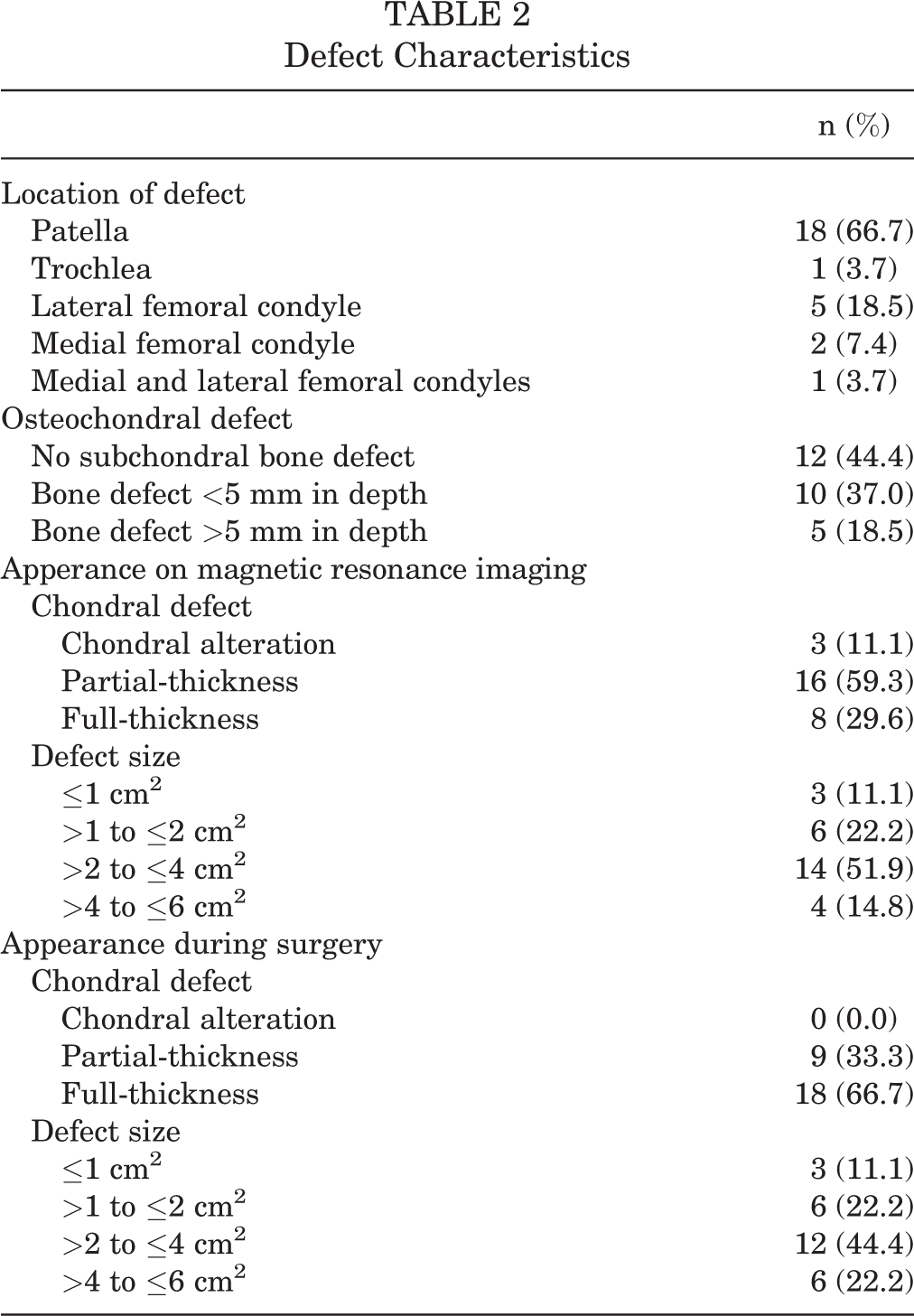
Of the patients, 18 (66.7%) had cartilage lesions at the patella, representing the most common location. In 5 patients (18.5%), the defect was found on the lateral femoral condyle, followed by the medial femoral condyle in 2 patients (7.4%). One patient (3.7%) had a trochlear defect or a combined lesion on the lateral and medial femoral condyles. Taken together, 19 (70.4%) patients suffered lesions in the patellofemoral and 8 (29.6%) in the tibiofemoral joint compartment. The intraoperative appearance (area and depth) of the cartilage defects differed from the appearance in the preoperative MRI scans; the mean defect size as assessed intraoperatively was 3.1 ± 1.6 cm2. The detailed defect characteristics are summarized in Table 2.
Defect Characteristics
Concomitant procedures were performed in 18 patients (66.7%) and included 6 realignment procedures of the patella, 4 reconstructions of the medial patellofemoral ligament, 3 tibial osteotomies, 2 extractions of osteosynthetic material, 2 osteosyntheses, 2 cancellous bone graftings, 1 femoral osteotomy, 1 microfracture, and 1 meniscal debridement.
Clinical Results
The clinical results showed continuous improvement over time. The mean preoperative NAS pain score of 7.2 ± 1.9 (range, 2-10) decreased significantly at 1 year after surgery to 2.3 ± 2.0 (range, 0-7) (P < .001) and further to 1.8 ± 1.6 (range, 0-5) (P < .001) at the 2-year follow-up. In the same manner, the mean preoperative values for function improved. Preoperatively, the mean of 7.2 ± 2.0 (range, 2-10) showed significant improvement, with a decrease to 3.0 ± 2.2 (range, 0-7; P < .001) after 1 year and to 2.1 ± 2.3 (range, 0-7; P < .001) after 2 years. The comparison of preoperative and postoperative mean values of pain and function is displayed in Figure 2. The subgroup analysis for a comparison of patients with patellofermoral lesions (n = 19) and tibiofemoral lesions (n = 8) did not show significant differences after 1 (P = .269) and 2 years (P = .457). The linear regression model revealed patient age as a significant predictor for preoperative pain (R 2 = 0.12; P < .045), while the other variables had no significant predictive effect on the outcome measurements.

Mean numeric analog scale (NAS) scores for subjective pain and function preoperatively and at 1- and 2-year follow-up. Pain: 0 = no pain, 10 = worst imaginable pain. Function: 0 = normal function, 10 = no function. Error bars indicate standard deviations. ***P < .001, difference compared to preoperatively.
At the final follow-up, a total of 25 patients (92.6%) indicated that they would undergo the procedure again, while 2 patients stated that they would not consider having the same surgery. No complications occurred during the procedure or until final follow-up, and no patient needed revision surgery because of other reasons.
Radiological Results
The preoperative AMADEUS score ranged from 10 to 85 points, with a mean of 57.4 ± 21.4. Postoperative MRI was performed after a mean of 6.0 ± 1.9 months. The postoperative MOCART score ranged from 25 to 70 points, with a mean of 40.6 ± 21.1. There was no correlation between the clinical data and either of the radiological scores (AMADEUS or MOCART). No significant difference between patients with patellofemoral and tibiofemoral lesions could be observed (P = .522). The linear regression model revealed that patient age is a significant predictor for the total MOCART score (R 2 = 0.36; P < .001). The comparison of the preoperative AMADEUS score to the postoperative MOCART score is displayed in Figure 3.

Comparison of preoperative AMADEUS (Area Measurement and Depth and Underlying Structures) score and postoperative MOCART (magnetic resonance observation of cartilage repair tissue) score. AMADEUS: 0 = most severe cartilage defect, 100 = no cartilage defect. MOCART: 0 = poor/no repair tissue, 100 = optimal repair tissue. Error bars indicate standard deviations.
Discussion
Chondral and osteochondral lesions of the knee joint are a major risk factor for the development of premature osteoarthritis. 25,35,49 Based on recent clinical data and basic scientific research, this risk is even increasing depending on the degree and chronicity of the initial cartilage lesion, whereas there is a broad variability in the origin. 10,13,25,35,49
The treatment of such chondral and osteochondral lesions of the knee joint still poses a challenge for the surgeon, while it represents an important part in the prevention of further cartilage loss and ultimately of total knee arthroplasty. 13 Only clinically symptomatic cartilage lesions are an indication for surgical treatment, despite the fact that even asymptomatic defects might progress. 10,35 Based on the available literature, acute focal cartilage defects as well as limited degenerative or chronic defects represent an indication for cartilage repair if they are clinically symptomatic. 16,30,34,35
The general surgical techniques for the treatment of cartilage defects can be categorized into transplant procedures, such as ACI and OATS, as well as bone marrow stimulation techniques (microfracture, abrasion arthroplasty, and drilling procedures). It is important to note that these surgical procedures do not necessarily compete with one another, as they are used in different settings or indications. 19,35
Techniques for surgical cartilage repair have the ultimate goal of generating the best possible RT to promote a better clinical outcome. 11,35 In this context, it is accepted that, up to now, ACI results in the best proportion of hyaline-like tissue in the former defect area, which has a beneficial effect on durability. 22,35,40,47 Unfortunately, ACI is not available in every country, and it has the further disadvantage of being a 2-step procedure.
Therefore, it may not be a feasible option for a large number of patients. The autologous minced (or particulate) cartilage procedure represents a possible alternative. 4,8,44 After initial reports from Albrecht 1 in the early 1980s, Lu et al 24 were the first to pick up the topic of cartilage piece implantation in the 2000s again. Animal models demonstrated that articular chondrocytes that are brought into a defective region are capable of migrating from their surrounding matrix and establishing a new matrix or that transplanted chips can incorporate within the lesion. 4,15,23,52 In addition, after a surgical procedure, the knee joint is filled with a heterogeneous “cocktail” of anabolic, inflammatory, and catabolic cytokines that promote matrix breakdown and chondrocyte proliferation. 48 Chondrocytes that are challenged and brought close to the surface of their surrounding matrix start to divide and proliferate again as part of a natural healing process, which has been described in spontaneously healing small cartilage lesions and in animal models. 33 Furthermore, a physiological articular in vivo environment is subject to constant biomechanical input. 17 These findings are supported by satisfying 2-year data among a small collective of patients treated by autologous cartilage chips held in place by the use of fibrin glue. 8
The findings of this study demonstrate positive results in knee function, pain, and satisfaction after a 1-step autologous minced cartilage procedure in 27 consecutive patients with a mean follow-up of 28.2 ± 3.8 months. The subjective evaluation of knee pain at the index joint showed a low mean score of 1.8 ± 1.6 (0 = best, 10 = worst) at 2-year follow-up. In the same manner, the evaluation for knee function showed a good result of 2.1 ± 2.3 (0 = best, 10 = worst) after 2 years. As the final return to full function after transplant procedures such as ACI often requires ≥24 months, 5 there is a good possibility that our cohort of patients may improve even further. Furthermore, we found that 25 patients (92.6%) would undergo the procedure again because of the satisfying result. Despite the simple assessment by an NAS, the presented clinical outcomes are comparable to the outcomes after ACI. 5,12,31,35
The presented radiological outcomes at 6 months after surgery resulted in a not entirely satisfying mean MOCART score of 40.6 ± 21.1 (a score of 100 represents completely healthy cartilage). However, these results seem to be comparable to those of previously published studies. Christensen et al 8 observed a MOCART score of 52.5 at 1 year after a particulate cartilage procedure, and Niemeyer et al 38 observed a long-term (follow-up of 10.9 years) MOCART score of 44.9 ± 23.6 after first-generation ACI. We chose the mean time point of 6.0 ± 1.9 months after surgery for an MRI assessment so we would not miss potentially unknown issues when using a novel technique, even though the patients showed a regular postoperative course. It is well known that cartilage repair processes require longer time spans (≥2 years) to generate the final tissue morphology and that the MOCART score shows continuous improvement over time. 39 Therefore, we expected the MOCART score to be within the observed range at 6 months. Furthermore, there was no significant correlation between the MOCART score and the clinical results of our patients. This is supported by previous studies that showed that MRI and clinical data do not truly correlate after cartilage repair procedures. 9,38
In the linear regression model, patient age was found to be a significant predictor for the MOCART score and therefore for the RT, as younger patients showed higher values. Previous studies showed similar results. Bone marrow stimulating procedures (eg, microfracture) are known to be more effective in patients younger than 40 years, 21,35 while transplant procedures (eg, ACI, OATS) also showed satisfying results even in older patients. 35,37 Therefore, we did not limit the indication for the minced cartilage procedure to patients aged ≤40 years.
With regard to our internal indication policy for cartilage repair, all 27 patients would have undergone ACI instead of the autologous particulate cartilage procedure. Yet, health insurance regulations in Switzerland did not allow for ACI among the patients of this cohort. As most defects (n = 18) were localized at the patella and/or showed a larger diameter (>2 cm2), we did not consider microfracture to be a suitable option because of its lack of RT quality and inferior long-term results compared to ACI. 11,29,35,40,45 On the other hand, the clinical outcomes of the patients after treatment with the autologous particulate cartilage procedure presented in this study are comparable to published results after ACI. 5,12,31,35
Our motivation to conduct this surgical technique and clinical trial was that ACI is not available to every patient in Switzerland. The advantage of autologous minced cartilage chips is that they can be applied as a 1-step procedure and therefore are a more economical option when compared with ACI. In addition, it is a feasible treatment option in incidental findings of larger cartilage defects during other joint-preserving knee procedures, as it can be spontaneously added to the primary procedure. 8,43 Donor cartilage can be taken from the periphery of the existing lesion, where it is necessary to debride into the healthy cartilage. Different publications have clearly described that such chondrocytes are viable and could be used for further transplantation. 2,6 If there is not enough donor material available from the defect itself, further donor cartilage can be taken from a typical ACI donor site such as the femoral notch. 27,28 When performing the minced cartilage procedure, there are a few crucial things that need to be kept in mind. The degree of fragmentation is very important. When the cartilage chips are left too large, the surface is too small for the chondrocytes to become active. Additionally, large pieces might not well incorporate into existing/newly built cartilage. Bonasia et al 3 reported that a paste-like appearance provides optimal circumstances for the generation of high-quality RT.
Furthermore, if an osseous defect has to be addressed as well, osteochondral cylinders can be harvested in the femoral notch. While the cartilage is minced, the bony part can be utilized to fill the osseous defect. In addition, osteochondral perforations at the distal femur are a temporary origin of stem cell influx into the joint, which may aid in early regeneration processes at the repair site. 18
There are some limitations of the present study that need to be discussed. First, there is the quite short clinical follow-up of 28.2 ± 3.8 months and the short radiological follow-up of 6.0 ± 1.9 months. Therefore, the results are not entirely comparable to those of previous studies on competing techniques such as ACI or microfracture with long-term follow-up of more than 10 years. 30,38 Yet, it has to be noted that our goal was not to present long-term data but to provide evidence for short-term safety and feasibility. This cohort of patients will be continuously followed and re-evaluated at 5 years postoperatively.
Another limitation is the absence of a control group. As previously described, the patients of the presented collective underwent the autologous minced cartilage procedure because ACI would not have been covered by their medical insurance and therefore was not a possible option. As none of the patients suffered cartilage lesions that had been an indication for microfracture, this was also no option for a possible control group. Lastly, it was not our intention to design a comparative trial but to analyze and describe an initial series of patients who underwent a novel surgical procedure. It is clear that after the presentation of initial data, longer follow-up and comparative trials are needed to possibly underline further and potentially broader uses of the autologous particulate cartilage procedure.
Lastly, the heterogeneity of the patients included in this study demonstrates a limitation, as their different co-abnormalities and the different locations of the cartilage defects cause difficulties in interpreting the clinical and radiological results. Eighteen (66.7%) patients of the study population suffered relevant co-abnormalities and needed additional procedures besides cartilage repair. Cartilage lesions are regularly accompanied or caused by concomitant defects and traumatic injuries such as patellofemoral malalignment, varus/valgus deformity of the knee, patellar dislocations, ligament ruptures, or fractures. 50,51 Therefore, we considered the concomitant procedures as essential for proper treatment and the possible confounding as unavoidable.
Conclusion
This series of patients treated by the described technique showed significant improvement in pain and knee function during a follow-up of 2 years. Based on the short-term clinical results of this study, we consider it a safe surgical procedure. With the knowledge that certain techniques have a chance to fail and the need to reduce health-associated costs, we consider the autologous minced cartilage procedure as a possible alternative to ACI and other cartilage repair options. Nevertheless, further high-quality studies and long-term results are needed.
Footnotes
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the local ethical committee of the Canton Zurich (KEK-ZH-Nr. 2015-0258).