
Abstract
Background:
Osteochondral lesions of the tibial plafond (OLTPs) remain less common than osteochondral lesions of the talus (OLTs), but recognition of the condition has increased.
Purpose:
To systematically evaluate the literature on lesion locations and treatment outcomes of OLTPs, whether in isolation or in combination with OLTs.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A search was performed using the PubMed, Embase, and CINAHL databases for studies on lesion locations or with imaging or treatment outcomes of OLTPs. Case reports and reports based on expert opinion were excluded. Lesion locations as well as outcome measure results were aggregated. The Methodological Index for Non-randomized Studies score was used to assess methodological quality when applicable.
Results:
Included in this review were 10 articles, all published in 2000 or later. Most studies were evidence level 4, and the mean Methodological Index for Non-randomized Studies score was 8.6 (range, 8-10). Overall, 174 confirmed OLTP cases were identified, and the mean patient age was 38.8 years. Of the 157 lesions with confirmed locations, the most common was central-medial (32/157; 20.4%). Of 6 studies on treatment outcomes, all but 1 evaluated bone marrow stimulation techniques. Microfracture of small lesions (<150 mm2) was the most common treatment utilized. Imaging and functional outcomes appeared favorable after treatment. The data did not support differences in outcomes between isolated OLTPs and OLTPs with coexisting OLTs.
Conclusion:
Osteochondral lesions of the distal tibia most commonly occurred at the central-medial tibial plafond. Microfracture of small lesions was the most common treatment utilized, and clinical and magnetic resonance imaging results were favorable, although data were heterogeneous. Areas for future research include the following: the effect of patient factors and additional pathologies on outcomes; larger or deeper lesion treatment; more direct comparisons of outcomes between kissing or coexisting lesions and isolated lesions; and head-to-head comparison of treatments, such as microfracture, bone marrow–derived cell transplantation, and osteochondral autografts/allografts.
Keywords
Although osteochondral lesions of the talus (OLTs) have been well described and characterized, descriptions of osteochondral lesions of the tibial plafond (OLTPs) are less common, with early reports on OLTPs beginning in the 1980s. 4,30 Cited OLT:OLTP ratios have ranged from 14:1 to 20:1, with a series of 880 ankle arthroscopies noting a 2.6% rate of identified OLTPs. 5,15,27 It has been purported that OLTPs are rarer than are OLTs owing to differing cartilage biomechanics. 1,5,10,13,16,24 The distal tibial articular cartilage has a higher modulus of stiffness as compared with the talar articular cartilage, with the anteromedial tibia having the stiffest and the posterior talus having the weakest articular cartilage. 1 Furthermore, the convexity of the talus leads to different loading mechanics compared with those of the concave surface of the tibial plafond. 5,12,15,18 In the ankle, osteochondral lesions are most frequently the result of trauma. 13,24,27,36,37
OLTPs may occur in isolation or in conjunction with OLTs. Incidences of coexisting lesions range from 15.8% to 35%, although variances in study design and patient populations make evaluation of cited rates challenging. 15,21,34,41 Lesions are frequently described by location in equivalent surface area zones created using a 3 × 3 grid as described by Elias et al 15,16 in 2009 (tibia) and 2007 (talus), respectively. OLTs and OLTPs lesions are deemed “kissing” if they are located in the same zone on both the talus and tibia. 7,12,21,41 Posterior tibial tendon, lateral ankle ligament, and deltoid ligament abnormalities on magnetic resonance imaging (MRI) scans have also been shown to be more common in those with coexisting lesions as compared with those with isolated OLTs. 41
As the use of ankle arthroscopy has increased, recognition of OLTPs has increased, but there remain limited reports on clinical outcomes and what the long-term progression of disease may be. Even for the more common lesions on the talar side, the natural history is not well defined, and progression to arthritis may be less significant than previously thought, although risk of degeneration may be influenced by age. 14,22 It is important for ankle arthroscopic surgeons to understand the clinical outcomes after management of OLTPs to guide treatment decision making and counseling. The purpose of this review was to systematically evaluate the literature on lesion locations and treatment outcomes of OLTPs, whether in isolation or in combination with those of the talus. We hypothesized that data on OLTPs would be heterogeneous and of lower-level evidence but that outcomes of arthroscopic treatment would be overall favorable.
Methods
This systematic review was registered on the International Prospective Register of Systematic Reviews (PROSPERO CRD42020187348). A systematic database search of PubMed, Embase, and CINAHL was performed on May 19, 2020, for the following search terms: (tibia OR tibial) AND (osteochondral OR osteochondritis) AND (ankle OR distal). Studies were included if they discussed treatment or imaging outcomes of OLTPs. Studies describing the locations of lesions were also included, as were studies discussing outcomes after treatment of concomitant OLTPs and OLTs. Exclusion criteria were proximal tibial/knee osteochondral lesions, case reports or case series with <3 patients, and reports based on expert opinion. Epidemiologic studies without lesion locations or without imaging or clinical outcomes were excluded. Reports on global cartilage degeneration or arthritis if unrelated to osteochondral lesions were excluded. Studies of patients with OLTs and OLTPs with insufficient subgroup data on distal tibial lesions (whether isolated or coexisting/kissing), such as lesion locations on the plafond or outcomes on the group with OLTPs, were also excluded.
The review of titles and abstracts was performed independently by 4 authors for inclusion (A. Sachin, A. Sameer, R.A., K.G.). Any article identified by any reviewer as eligible underwent full-text review. In total, 23 articles were included for full-text review. During full-text review, 13 articles were excluded, as listed in Figure 1. Data collected from the remaining articles were publication characteristics, type of treatment, and outcome measures. Two authors (A. Sachin, B.C.L.) independently evaluated the level of evidence and the methodologic quality of the articles on surgical treatment using the Methodological Index for Non-randomized Studies criteria. 35

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart for study inclusion. Ten full-text articles were included.
Data were compiled for descriptive analyses and are reported as mean and SD with range when available. Lesion locations as described by Elias et al 15 were aggregated when described by zone in the study reviewed or classified into a zone by us when the study described lesions by location within the plafond. This zone classification divides the tibial plafond into a 3 × 3 grid for 9 equal-area anatomic zones, with zone 1, anteromedial; zone 3, anterolateral; zone 5, central; zone 7, posteromedial; and zone 9, posterolateral.
Results
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the search is demonstrated in Figure 1.
Ten articles were included in the review (Figure 1, Table 1). 2,3,5,10,13,18,20,24,29,36 All studies were published in 2000 or later and were deemed level 4 evidence, except for Elias et al. 15 The mean Methodological Index for Non-randomized Studies score of the 5 surgical treatment studies 3,12,23,27,33 was 8.6 (range, 8-10); each of these was a noncomparative case series.
Descriptive Data of the Included Studies a
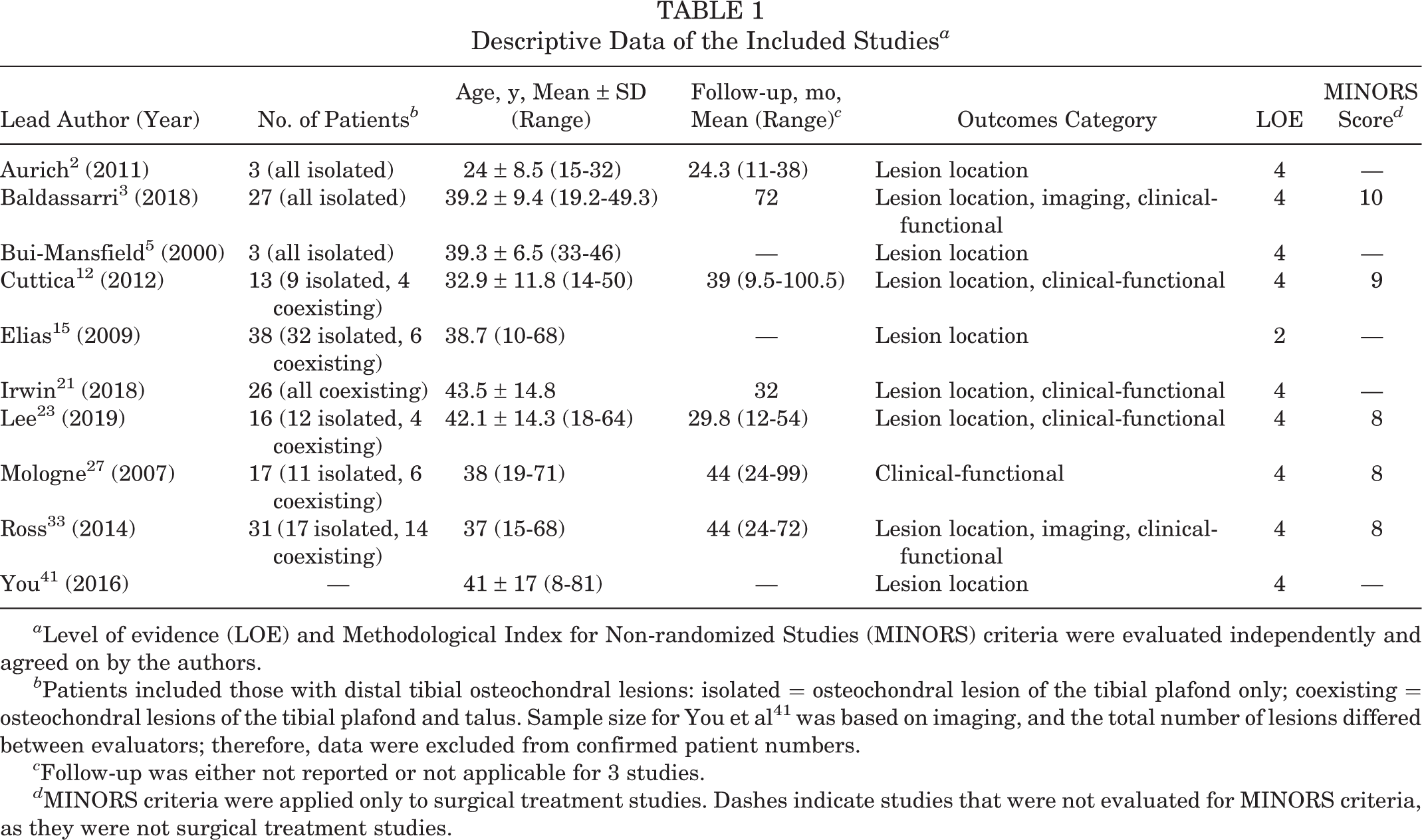
a Level of evidence (LOE) and Methodological Index for Non-randomized Studies (MINORS) criteria were evaluated independently and agreed on by the authors.
b Patients included those with distal tibial osteochondral lesions: isolated = osteochondral lesion of the tibial plafond only; coexisting = osteochondral lesions of the tibial plafond and talus. Sample size for You et al 41 was based on imaging, and the total number of lesions differed between evaluators; therefore, data were excluded from confirmed patient numbers.
c Follow-up was either not reported or not applicable for 3 studies.
d MINORS criteria were applied only to surgical treatment studies. Dashes indicate studies that were not evaluated for MINORS criteria, as they were not surgical treatment studies.
A total of 174 confirmed OLTPs were included. One study by You et al 41 was included in the review, but lesions and their locations were not reported as confirmed, owing to the lack of consensus among MRI evaluators. The mean patient age in those with confirmed OLTPs ranged from 24.0 to 43.5 years, with a calculated cohort mean of 38.8 years. A total of 157 lesions had confirmed locations on the distal tibial plafond, which were aggregated; Mologne and Ferkel 27 did not comment on lesion locations for the 17 patients evaluated in their study (Table 2). The most common zone reported for lesions was zone 4 (central-medial, 32/157; 20.4%), followed by zone 5 (central, 22/157; 14.0%) and zone 2 (central-anterior, 19/157; 12.1%) (Figure 2). The medial zones (zones 1, 4, and 7) accounted for 61 of 157 (38.9%) lesions; the lateral zones (zones 3, 6, and 9), for 37 of 157 (23.6%); and the central zones (zones 2, 5, and 8), for 59 of 157 (37.6%). In the anteroposterior plane, the anterior zones (1-3) accounted for 47 of 157 (29.9%) lesions; the middle zones (4-6), 66 of 157 (42.0%); and the posterior zones (7-9), 44 of 157 (28.0%). Because of inconsistency in the studies in distinguishing the locations between isolated and coexisting lesions, coexisting lesion locations on the plafond were not aggregated.
Distribution of OLTPs According to Zone Descriptions a

a Classified according to Elias et al, 15 in which the tibial plafond is divided into a 3 × 3 grid of 9 anatomic zones: zone 1 = anteromedial, zone 3 = anterolateral, zone 5 = central, zone 7 = posteromedial, and zone 9 = posterolateral (also see Figure 2). OLTP, osteochondral lesion of the tibial plafond.

Map of aggregated osteochondral lesions of the tibial plafond from the included studies based on the zone description by Elias et al. 15 Data from You et al 41 were excluded from the aggregated numbers in this figure, as there was a lack of consensus between reviewers on the number of lesions and lesion locations on magnetic resonance imaging evaluation without arthroscopic confirmation.
Two studies 3,33 evaluated imaging outcomes after treatment, utilizing the MOCART scoring system (magnetic resonance observation of cartilage repair tissue) (Table 3). Baldassarri et al 3 treated the tibial lesions using bone marrow–derived cell transplantation (BMDCT) and noted complete chondral defect filling in 68% on MRI evaluation and intact surface repair tissue in 71%. Ross et al 33 utilized arthroscopic microfracture/bone marrow stimulation techniques and found that increasing age and lesion size were correlated with poorer MOCART scores.
Imaging Outcomes of the 2 Studies Relating to Osteochondral Lesions of the Tibial Plafond a

a Both studies utilized the MOCART (magnetic resonance observation of cartilage repair tissue) scoring system to assess imaging outcomes and healing. FAOS, Foot and Ankle Outcome Score; SF-12, 12-Item Short Form Health Survey.
Six studies 3,12,21,23,27,33 evaluating clinical or functional measures after treatment were included (Table 4). Three studies 3,12,27 utilized the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot scale; 2 studies, 21,33 the Foot and Ankle Outcome Score (FAOS); and 2 studies, 23,33 the 12-Item Short Form Health Survey (SF-12). The treatments varied. Baldassarri et al 3 utilized BMDCT, noting significantly improved AOFAS scores (52.4 to 80.6 posttreatment; P < .05), with smaller lesions (<150 mm2) having a greater rate of improvement (P = .038) and shallower lesions (<4 mm2) having better overall AOFAS scores (P = .003). Cuttica et al 12 incorporated a variety of techniques, including debridement, marrow stimulation, and lateral ligament stabilization in 3 patients. The authors found that patients with coexisting lesions had a longer time before return to unrestricted activity (19.7 ± 9.2 weeks for isolated lesions vs 23.8 ± 11.7 weeks for coexisting lesions). Irwin et al 21 treated OLTs with bone marrow stimulation or autologous osteochondral transplantation and reported no difference in functional outcomes in those with coexisting tibial lesions. Lee et al 23 and Ross et al 33 primarily utilized arthroscopic microfracture/bone marrow stimulation techniques. Lee et al noted significantly improved visual analog scale for pain scores (from 8.3 ± 1.2 to 1.8 ± 1.2; P < .001) in addition to significantly improved Foot and Ankle Ability Measure and SF-12 scores; however, the effect of sports activity in this cohort decreased after treatment (P = .012). Ross et al found significantly improved FAOS (from 50.5 to 74.2; P < .01) and SF-12 (from 38.7 to 59.5; P < .01) scores and that age was negatively correlated with SF-12 scores (r = –0.50; P < .01). Notably, lesion location and area were not associated with outcome measures, and there were no differences in functional outcomes between those with isolated and coexisting lesions. Mologne and Ferkel 27 treated patients with debridement, curettage, abrasion arthroplasty, and in some cases bone marrow stimulation or grafting of cystic cavities, noting significantly improved AOFAS scores (median, 57 to 82; P < .001) and no differences based on lesion size or differences in pre- or postoperative scores in isolated versus coexisting lesions.
Clinical and Functional Outcome Measures of Studies Relating to OLTPs a

a AOFAS, American Orthopaedic Foot and Ankle Society (ankle-hindfoot score); BMI, body mass index; FAAM, Foot and Ankle Ability Measure; FAOS, Foot and Ankle Outcome Score; MCS, Mental Component Summary; OLT, osteochondral lesion of the talus; OLTP, osteochondral lesion of the tibial plafond; PCS, Physical Component Summary; postop, postoperative; preop, preoperative; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
b Outcomes are listed as mean pre- to postoperative scores unless otherwise noted.
c Data by Irwin et al 21 are on coexisting OLTP and OLT, comparing outcomes between patients with coexisting lesions and those with isolated OLTs.
d Mean lesion size was not reported or calculable from data ranges listed by Mologne and Ferkel. 27
Discussion
The present review highlighted the reported locations of OLTPs and outcomes of treatment. Lesion locations were aggregated for this rare but important-to-recognize entity to contribute to the literature summarizing OLTPs. Although studies were limited, with heterogeneous treatment strategies and outcome measures in current literature, treatment outcomes for OLTPs appeared favorable. Furthermore, studies included outcomes of isolated distal tibial and coexisting lesions.
The most common zone location in the aggregated group was zone 4, the central-medial tibia plafond, representing 20.4% of the group. In the original zone description by Elias et al, 15 zone 4 was also the most common zone, representing 21% of lesions. In other studies, zone 4 was frequently noted to be one of the most involved zones. 3, 21,29,41 Biomechanical data have shown that zone 8 has the lowest puncture strength on the plafond, significantly lower than that of zone 3 and zone 7, which are the strongest areas. 39 Differences in locations in clinical data from these laboratory data are likely due to clinical and traumatic forces on the plafond. Another area warranting further investigation with regard to location is correlating findings on MRI scans with findings of arthroscopy. In the review of MRI scans by You et al, 41 interobserver agreement kappa between the 2 reviewers for the presence of osteochondral lesion was 0.73 and 0.77 on the first and second reviews, respectively. Interobserver agreement kappa was 0.62 and 0.61 in terms of lesion location and stage. These interobserver agreements were similar to those found in an MRI study of lesions in the talus. 25 Ultimately, however, arthroscopic findings may be useful for confirmation of lesion location, size, and depth.
Although lesion location may ultimately be variable, examining patterns of injury may help guide understanding of the cause of the lesions as well as the treatment. Zones 2, 4, and 5 may be more commonly affected in the case of coexisting or kissing lesions. 21,41 As zone 4 is central-medial and zone 5 is central on the tibial plafond, the association with kissing lesions may be explained by the medial talar location being the most common site for OLTs. 36 Interestingly, medial talar dome lesions tend to have a more idiopathic cause, whereas laterally based OLTs have a more traumatic cause. 36 While there does appear to be a traumatic contribution to many OLTPs, it is unclear if trauma is significantly associated with the specific lesion locations on the tibia. The association of trauma and instability in general with OLTPs was supported by You et al 41 who found a significant association between those with coexisting lesions of the tibia or fibula (“zone 10”) and MRI abnormalities in the lateral and medial ankle ligaments and posterior tibialis tendon. Ross et al 33 additionally repaired the lateral ankle ligaments in 4 patients, 2 of whom had kissing lesions. Similarly, Cuttica et al 12 performed lateral ankle ligament stabilization in 3 of 13 patients (2 isolated, 1 coexisting). Furthermore, Baldassarri et al, 3 in evaluating BMDCT for isolated OLTPs, found inversion ankle sprain as a traumatic cause in 20 of 27 patients and noted that those with impingement findings had a worse rate of improvement in AOFAS scores at 12-month follow-up (P = .029). The findings from these studies suggest that additional ankle pathologies such as instability and trauma may affect the incidence, natural history, or outcomes of treatment of OLTPs. However, Baldassarri et al also noted that the presence of arthrosis did not affect the rate of improvement of AOFAS scores, although it did decrease the absolute value. Therefore, differential effects may be seen depending on the associated pathology, and there may be influences based on the type of treatment performed. While no current data suggest that different lesion locations affect functional outcomes, understanding lesion location may improve reliability of OLTP identification on diagnostic ankle arthroscopy, which can then guide treatment. However, data on the epidemiology of asymptomatic OLTPs and the natural history of these lesions are lacking, making an understanding of when to treat arthroscopically identified lesions challenging.
Thus far, imaging and functional outcomes do not appear to vary by lesion location. 15,27,33 Moreover, the data presented suggest that those with coexisting OLTs and OLTPs do not have differences in functional outcomes when compared with those with isolated OLTs or isolated OLTPs. 12,21,27,33 Irwin et al 21 did not find any difference in pre- or postoperative FAOS scores between patients undergoing bone marrow stimulation or osteochondral transfer procedures for OLTs in isolation and those coexisting with OLTPs. However, the authors did find that patients with coexisting lesions were more likely to have an International Cartilage Regeneration Society grade 4 OLT as compared with the isolated OLT group (P = .034) and that talar dome zone 6 was the most common location for those with kissing lesions (P = .043). 21 Most studies did not provide significant subgroup analyses comparing coexisting lesions with isolated lesions, likely limited by the small numbers of patients.
Age should be considered in the assessment of OLTPs. The mean age of those with confirmed lesions in the present study was 38.8 years. Irwin et al 21 found that patients with coexisting OLTPs and OLTs were significantly older than those with isolated OLTs (43.5 ± 14.8 vs 36.1 ± 13.8 years; P = .038). Baldassarri et al, 3 however, did not find that age affected AOFAS scores in patients with isolated OLTPs undergoing BMDCT. However, Ross et al 33 found a negative correlation between age and change in SF-12 (r = –0.50; P < .01) for patients undergoing bone marrow stimulation for isolated and coexisting lesions. It is difficult with current data to determine the true effect of age on OLTPs, as its influence may vary with type of treatment and the resultant cartilage architecture, presence of OLTs, and/or confounders. It is possible that degenerative osteoarthritic changes in the tibiotalar joint, whether age dependent or independent, may limit the benefits of regenerative treatments, but further information is needed to clarify ideal candidates and risks for treatment failure.
This systematic review identified 6 studies evaluating outcomes for distal tibial lesions. 3,10,18,20,24,29 This is in contrast to a systematic review on treatment of OLTs published a decade ago identifying >50 studies. 42 The limited data on OLTPs likely reflect the relatively low incidence of OLTPs relative to OLTs. All of the data presented demonstrated generally favorable outcomes in terms of functional measures with low complication rates. However, given that all the treatment outcome data had level 4 evidence, there is a need for comparative studies. Furthermore, even within several of the studies, there was heterogeneity in treatment; for example, Cuttica et al 12 treated 3 patients using additional lateral ligament stabilization, and Mologne and Ferkel 27 used bone marrow stimulation in some cases and bone-grafted cystic cavities in others. The variation and addition of other procedures in a nonstandardized fashion make interpreting the benefit of treatment of the OLTPs alone challenging.
Three studies commented on outcomes in terms of return to activity or sports. 12,23,33 Cuttica et al 12 noted a return to unrestricted activity 20.9 ± 9.7 weeks after microfracture, with those with isolated lesions returning 4.1 weeks earlier compared with those with coexisting lesions (19.7 ± 9.2 vs 23.8 ± 11.7 weeks). This time frame was shorter than the mean 6.3 months (range, 2-22 months) for return to activity reported by Ross et al. 33 Lee et al 23 found significant improvements in the Foot and Ankle Ability Measure–Sports subscale (from 34.5 ± 26.0 to 65.2 ± 30.2; P < .001) and reported 100% return to sports; however, they also noted a significant decrease in level of sports activity as defined by impact, with a larger proportion of patients performing lower-impact activity postoperatively (from 12.5% preoperatively to 62.5% postoperatively; P = .012). Future studies evaluating return-to-sports outcomes after OLTPs should incorporate details on the type of sports, the level of activity, patient satisfaction with activity level or performance, and timing.
When lesions of the talus are treated, bone marrow stimulation techniques such as microfracture are generally used for smaller lesions (typically ≤150 mm2). 9,10,32 Bone marrow stimulation is the most common technique studied in managing OLTPs, with overall optimistic results. One retrospective evaluation of 31 ankles with a mean lesion size 38 mm2 demonstrated significant improvements in FAOS and SF-12 scores, 29 while another demonstrated significant improvements in AOFAS ankle-hindfoot scores. 10 It is not clear if a critical size exists or what that critical size is for microfracture of OLTPs. However, in 1 study assessing healing via the MOCART scores after microfracture, increasing age and lesion size were significantly associated with lower scores. 33 These outcomes suggest that the healing potential to the subchondral plate may be better in younger patients, with likely better microvascular networks, and in those with smaller lesions where microvascular flow may be less disrupted. Even if microfracture is clinically successful, the repair tissue may be considered inferior with poorer mechanics as compared with native cartilage. 33 In the case of OLTPs, because of the increased normal cartilage thickness of the distal tibia relative to the talus, 1 regenerating strong repair tissue may be even more important to match the surrounding mechanical environment. Additional treatments, such as augmentation with acellular micronized cartilage matrix and platelet-rich plasma, may be considered.
One treatment presented by Baldassarri et al 3 designed to address the weaker repair tissue of bone marrow stimulation techniques is BMDCT. This 1-step technique serves as a scaffold upon which bone marrow cells from bone marrow aspirate concentrate are stimulated with factors from platelet-rich fibrin to support osteochondral growth more similar to native hyaline cartilage. In the series of 27 patients with isolated OLTPs, there were significant improvements in rates in AOFAS scores up to 36 months, which remained stable at 72-month follow-up. Of note, there were no complications, and MRI scans demonstrated complete chondral defect filling in 68% of patients, with isointense signal intensity of the repair tissue in 89%. Further evaluations of this technique as a 1-step low-morbidity treatment are warranted. However, BMDCT may be limited by similar restrictions to those for microfracture, with patients with shallower and smaller lesions demonstrating improved outcomes. A comparative study is needed.
When defect sizes are large in other joints such as the knee, osteochondral auto- or allograft transfers have demonstrated good outcomes and return to activities and sports. 6,11,20,29,40 However, for OLTPs, only case reports thus far have described grafting. 8,38 Ueblacker et al 38 utilized retrograde autografts from the femoral trochlea for the osteochondral transfer plug in 2 patients with distal tibial lesions. At >2-year follow-up postoperatively, MRI scans demonstrated integrated cylindrical plugs with congruent joint surfaces. One limitation of this technique is its potential for donor-site morbidity. However, donor-site morbidity may be less of a clinical concern based on evidence on talar lesions. Fraser et al 17 examined outcomes of donor sites for autograft osteochondral transplantation for OLTs and found no correlation between MOCART scores and Lysholm outcome scores.
Other techniques for larger defects, such as autologous chondrocyte transplantation, 28 autologous matrix-induced chondrogenesis, 26 autologous bone, 19 and synthetic osteochondral plugs, 31 have been described thus far only in case reports. The patient who underwent autologous chondrocyte transplantation had a tibial plafond cartilage defect of ∼75% of the joint surface and was able to return to recreational sports by 24 months postoperatively, with no pain in daily activities at final follow-up of 8 years. 28 Autologous matrix-induced chondrogenesis was used in conjunction with microfracture in a 29-year-old patient, who returned to activities 1 year postoperatively and had MRI evidence of an intact cartilage layer more consistent with that of native hyaline. 26 In contrast, the patient who had surgery using a synthetic osteochondral plug for an unstable distal tibial cartilage lesion with a cyst, despite subjective clinical improvement, had MRI findings more consistent with fibrous cartilage healing. 31 Higher-volume studies are needed before assessments of these treatments in managing OLTPs, including imaging outcomes to evaluate cartilage repair quality and clinical/functional outcome measures, can be made. In addition to lesion size, another factor warranting evaluation is lesion depth. Baldassarri et al 3 found that lesions that were deeper than 4 mm had worse AOFAS scores at 36 months (P = .005) and 72 months (P = .003) as compared with those that were shallower.
This systematic review was primarily limited in the paucity of data; the variety of treatments; and the current evidence, which is largely level 4 without comparison groups. Therefore, we were unable to aggregate the majority of the data or perform any meaningful meta-analyses, and conclusions of the studies should be interpreted with caution. The number of studies on OLTPs were also limited, with even fewer reporting on outcomes of treatment. Those that did report outcomes were heterogeneous in the measures utilized and the treatment techniques. More studies are needed on OLTPs and coexisting OLTPs and OLTs to understand algorithms in and outcomes of management. Future studies should evaluate factors such as the effects of age and lesion area and depth on outcomes. Furthermore, determining the association of imaging findings with arthroscopic findings and each of these with functional outcomes would be beneficial to understand the utility of the pre- and intraoperative evaluation. More data are needed to understand if there are differential outcomes with kissing or coexisting lesions as compared with isolated lesions, in addition to direct comparisons of treatment such as microfracture, BMDCT, and osteochondral auto- and allografts.
Conclusion
Osteochondral lesions of the distal tibia most commonly occurred at the central-medial tibial plafond. Microfracture of small lesions, <150 mm2, was the most common treatment utilized, and clinical and MRI results were favorable, although data were heterogeneous. Areas of future research may include the following: effects of patient factors and additional pathologies on outcomes; larger or deeper lesion treatment; more direct comparisons of outcomes between kissing or coexisting lesions and isolated lesions; and head-to-head comparisons of treatments such as microfracture, BMDCT, and osteochondral auto- and allografts.
Footnotes
Final revision submitted November 1, 2020; accepted December 11, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.K.P. has received consulting fees from OrthoPediatrics and educational support from Evolution Surgical. B.C.L. has received research support from Arthrex and Wright Medical and educational support from Smith & Nephew and SouthTech Orthopedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.