
Abstract
Background:
Autologous chondrocyte implantation (ACI) is an established method for treating cartilage defects in the knee of adult patients. However, less is known about its effectiveness in adolescents.
Hypothesis:
Third-generation matrix-associated ACI (MACI) using spheroids (co.don chondrosphere/Spherox) is an effective and safe treatment for articular cartilage defects in adolescents aged 15 to 17 years, with outcomes comparable with those for young adults aged 18 to 34 years.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 71 patients (29 adolescents, 42 young adults) who had undergone ACI using spheroids were evaluated retrospectively in this multicenter study. For adolescents, the mean defect size was 4.6 ± 2.4 cm2, and the follow-up range was 3.5 to 8.0 years (mean, 63.3 months). For young adults, the mean defect size was 4.7 ± 1.2 cm2, and the follow-up range was 3.8 to 4.3 years (mean, 48.4 months). At the follow-up assessment, outcomes were assessed by using validated questionnaires (Knee injury and Osteoarthritis Outcome Score [KOOS], International Knee Documentation Committee [IKDC] subjective knee evaluation form and current health assessment form, and modified Lysholm score), the magnetic resonance observation of cartilage repair tissue (MOCART) score, and if relevant, time to treatment failure. Safety was assessed by the treatment failure rate.
Results:
No significant difference between the 2 study groups was found for KOOS, IKDC, or MOCART scores, with all patients achieving high functional values. A significant difference was found in the modified Lysholm score, favoring the young adult group over the adolescent group (22.3 ± 1.9 vs 21.0 ± 2.4, respectively; P = .0123). There were no differences between the rates of treatment failure, with 3% in the adolescent group and 5% in the young adult group.
Conclusion:
Third-generation MACI using spheroids is a safe and effective treatment for large cartilage defects of the knee in adolescents at midterm follow-up. Outcomes are comparable with those for young adults after ACI.
Articular chondral and osteochondral injuries of the knee are common in patients younger than 35 years who are active in sports. While the prevalence of cartilage defects in the knee has been reported to be about 60% in the adult population, 3,41 in children and adolescents, it has been stated as 34% in skeletally immature patients and 41% in skeletally mature patients younger than 18 years. 22 Traumatic injuries are the most common cause, while repetitive microtrauma and osteochondritis dissecans are further important causes, especially in the younger population. 32 Symptomatic defects may lead to chronic pain and functional disability. 8 Furthermore, untreated cartilage defects tend to increase and predispose to the premature onset of osteoarthritis. 36
Therefore, treatment options need to aim on restoring cartilage function as closely to physiological parameters as possible, especially in young and active patients. 31 In bone marrow–stimulating procedures (eg, microfracture or Pridie drilling), better results have been found in younger patients; however, the resulting fibrocartilage repair tissue is biomechanically inferior to hyaline cartilage and therefore yields poorer long-term results. 2,37 This applies especially to defects larger than 4 cm2. 2,37
Autologous chondrocyte implantation (ACI) has been shown to have favorable outcomes, especially in larger defects, with satisfactory long-term results. 6,11,18,24,26 Since its introduction in 1994, several modifications have been implemented; in the first generation, chondrocytes were implanted under a periosteal flap, which was sealed to the adjacent cartilage. In the second generation, this flap was replaced by a collagenous membrane, and in the third generation, the chondrocytes are seeded in a collagenous matrix.
Third-generation matrix-associated ACI (MACI) using spheroids is a fully autologous technique employing chondrocytes cultivated in vitro and condensed into 3-dimensional spheroids such as Spherox (originally named co.don chondrosphere [ACT3D-CS]; co.don). Because the spheroids adhere to the subchondral bone by surface tension, this eliminates the need for additional scaffolds, making arthroscopic implantation feasible. 33
The administration of co.don chondrosphere is currently indicated for adults and adolescents with closed epiphyseal growth plates. The European Medicines Agency granted marketing authorization for Spherox (spheroids) for the repair of symptomatic articular cartilage defects (International Cartilage Repair Society [ICRS] grades 3 and 4) up to 10 cm2 in the knee in adults. As its use for adolescents is restricted in Europe, it seems necessary to gain data on its efficacy and safety.
Only a few studies have reported on the functional outcomes of patients younger than 18 years with the use of MACI, and there have been no reports of outcomes with this third-generation MACI using spheroids. Hence, the objective of this study was to assess the midterm results of MACI using spheroids in patients from 15 to 17 years of age (inclusive) at the time of implantation and to compare them with the functional outcomes of patients aged 18 to 34 years.
Methods
A total of 29 patients aged between 15 and 17 years treated with co.don chondrosphere between December 2007 and December 2011 were retrospectively included in the study. The mean age at implantation was 16.0 ± 0.9 years (range, 15-17 years), and the mean and median overall follow-up times were 63.3 and 58.0 months, respectively, with a range of 3.5 to 8.0 years (Table 1). The epiphyseal status was open in 8 patients, closed in 12 patients, and not documented in 9 patients.
Patient and Injury Characteristics a

a Data are shown as mean ± SD unless otherwise indicated. ACI, autologous chondrocyte implantation; ICRS, International Cartilage Repair Society.
As a control group, 48-month follow-up data of patients aged between 18 and 34 years were included from a phase II dose-level comparison study (EudraCT No. 2009-016816-20) (n = 42 patients). Treatment was performed between January 2011 and September 2012. The mean age at implantation was 26.5 ± 4.9 years (range, 19-34 years) (Table 1). Both studies were sponsored by co.don AG.
An overview of the patients’ characteristics is depicted in Table 1. In the adolescent group, 14 patients (48%) had cartilage lesions caused by trauma, and an equal number had osteochondritis dissecans; for 1 patient (3%), the defect cause was unknown. In the young adult group, defects were caused by trauma in the majority of patients (n = 24, 57%), whereas osteochondritis dissecans was present in only 3 patients (7%); other defect types (not further specified) were common (n = 13, 31%). Two patients in the young adult group were classified as having osteoarthritis; however, preoperative standing radiographs only revealed Kellgren-Lawrence scores ≤1.
In the adolescent group, 3 patients (10%) had more than 1 ICRS grade 3 or 4 lesion (2 lesions in each case), while in the young adult group, all patients had only 1 clinically relevant ICRS grade 3 or 4 lesion, and 2 of these patients (5%) also had a clinically irrelevant grade 2 lesion.
More than two-thirds of the cartilage defects in the adolescent group were femoral condyle lesions (20/32 defects, 69%), whereas in the young adult group, most defects were patellar lesions (28 /44 defects, 66%). The mean defect sizes were similar between the adolescent and young adult groups: 4.6 ± 2.4 cm2 and 4.7 ± 1.2 cm2, respectively.
Of the 29 patients in the adolescent group, 13 had undergone at least 1 previous surgical procedure to the affected knee compared with 7 of 42 patients in the young adult group. In the adolescent group, most prior surgeries performed addressed the cartilage defect (10/13). Treatments included drilling (n = 4), shaving (n = 2), refixation of an osteochondral fragment (n = 3), osteochondral transplantation (n = 1), and microfracture (n = 2). Apart from these treatments, surgeries performed were partial meniscal resection (n = 1), meniscal repair (n = 1), and lateral release (n = 1).
Of the 7 patients with previous surgical procedures in the young adult group, only 1 procedure was for cartilage treatment (microfracture). The remaining were ligament reconstruction (anterior cruciate ligament [ACL]: n = 3; posterior cruciate ligament: n = 1), partial meniscal resection (n = 4), and medial patellofemoral ligament (MPFL) repair (n = 1).
Concomitant procedures either at biopsy or at ACI were performed in 21 patients in the adolescent group and 13 in the young adult group. At biopsy, they consisted of shaving (n = 5), chondral debridement (n = 1), lateral release (n = 1), and meniscal repair (n = 1) in the young adult group and removal of loose bodies (n = 2), MPFL reconstruction/repair (n = 2), bone grafting (n = 3), ACL reconstruction (n = 1), screw removal (n = 1), and synovial plica resection (n = 1) in the adolescent group.
Simultaneous procedures at ACI consisted of shaving/abrasion (n = 5) in the young adult group and bone grafting (n = 4), medial imbrication (n = 3), MPFL reconstruction (n = 2), tibial tubercle transfer (n = 1), synovectomy (n = 1), arthrolysis (n = 1), and synovial plica resection (n = 1) in the adolescent group.
For the outcome assessment, the following validated scores were evaluated: Knee injury and Osteoarthritis Outcome Score (KOOS) and its 5 subscales (Pain, Symptoms, Activities of Daily Living, Sports and Recreation, and Quality of Life)
30
International Knee Documentation Committee (IKDC) subjective knee evaluation form
7
IKDC current health assessment form (Physical Functioning, Role Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role Emotional, and Mental Health) and associated summary scores: physical component summary (PCS) and mental component summary (MCS)
1
Magnetic resonance imaging (MRI) assessment including the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) score
15
The MRI assessment of repair tissue was performed with a minimum 1.5-T scanner using either a surface or knee coil, which has been proposed previously. 15,40 Sequences used were T1 axial and sagittal; T2 axial, sagittal, and coronal fast spin echo; proton density fast spin echo axial, sagittal (fat saturated), and coronal (fat saturated); and 3-dimensional gradient echo (fat saturated) with a slice thickness <5 mm.
The modified Lysholm score was administered by the investigator in an interview with young adults; KOOS and IKDC scores for young adults and adolescents, and the modified Lysholm score for adolescents, were collected by (electronic) self-reporting. For the Lysholm score, the modified version for cartilage defects recommended by Smith et al 35 was used (0-24 points). The MRI assessment for adolescents was performed by the responsible radiologist and for young adults by a blinded reader (radiologist). In the pediatric observation study and in the phase II study, patients with additional surgical treatment of cartilage after ACI were counted as treatment failure.
The 2 groups were compared by standard descriptive statistics, where appropriate, using the Wilcoxon 2-sample test at the exploratory level with significance defined as P < .05. A power analysis yielded a power of 0.090 to detect differences at an alpha of 0.05.
Results
Total KOOS and KOOS Subscales
The most important variable in both groups was the KOOS and its 5 subscales (Table 2). Total postoperative scores were not significantly different between the adolescent and young adult groups (82.6 ± 11.6 and 84.6 ± 11.7, respectively), with P values clearly above the defined significance threshold.
KOOS Total Score and Subscores a

a The number of completed questionnaires was 22 and 28 for adolescents and young adults, respectively. KOOS, Knee injury and Osteoarthritis Outcome Score.
IKDC Subjective Knee Evaluation Form
There was no significant difference in the IKDC score between the adolescent and young adult groups (81.1 ± 17.7 and 80.5 ± 15.2, respectively) (Table 3).
IKDC, Modified Lysholm, and MOCART Scores a
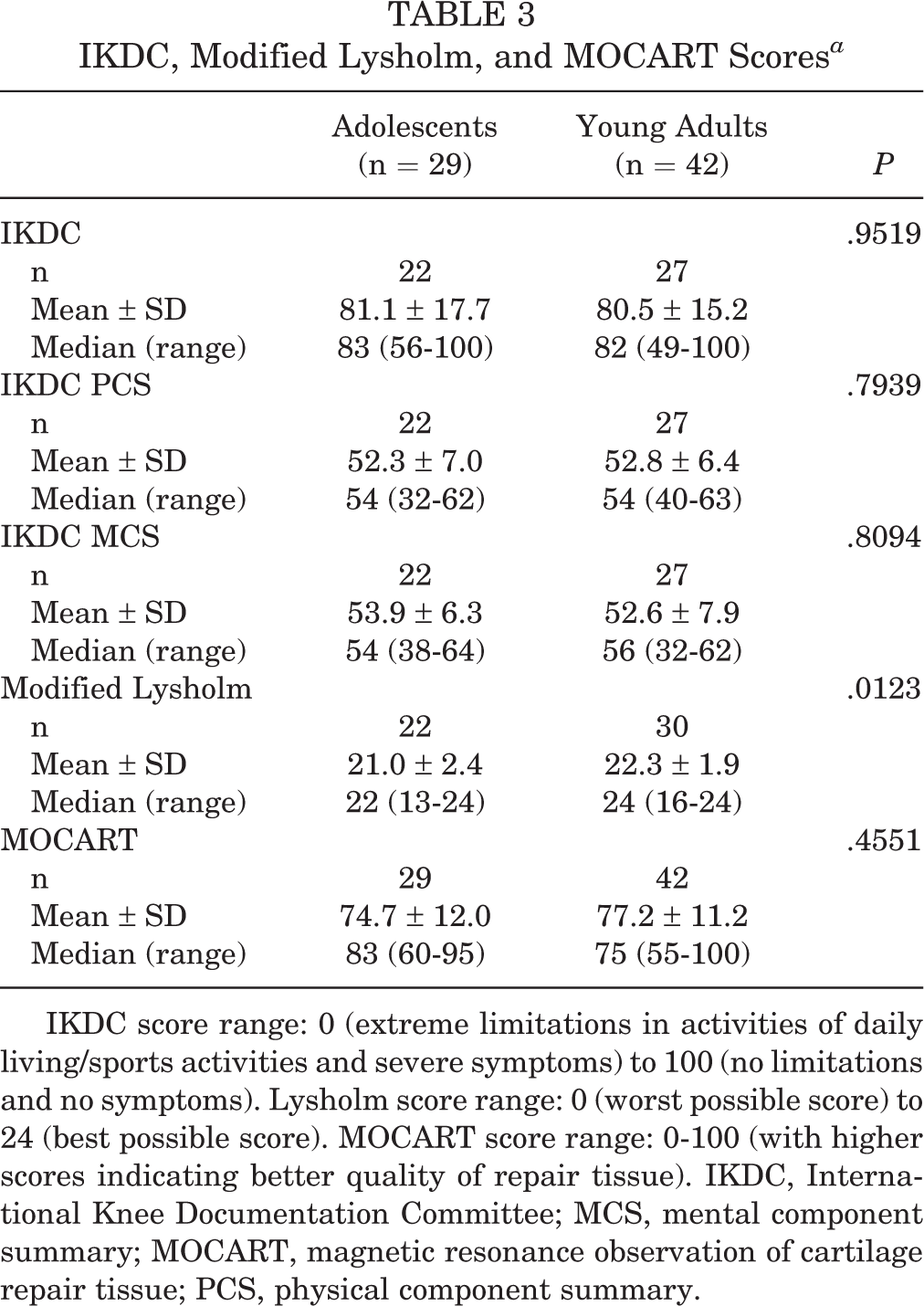
IKDC score range: 0 (extreme limitations in activities of daily living/sports activities and severe symptoms) to 100 (no limitations and no symptoms). Lysholm score range: 0 (worst possible score) to 24 (best possible score). MOCART score range: 0-100 (with higher scores indicating better quality of repair tissue). IKDC, International Knee Documentation Committee; MCS, mental component summary; MOCART, magnetic resonance observation of cartilage repair tissue; PCS, physical component summary.
IKDC Current Health Assessment Form and Summary Scores
The highest mean scores were achieved on the Role Emotional subscale in both the adolescent and the young adult groups: 93.9 ± 16.7 and 92.9 ± 16.6, respectively. The lowest mean scores were found on the Vitality subscale in both the adolescent and young adult groups: 70.7 ± 16.9 and 67.0 ± 21.1, respectively. There were no statistically significant differences between the groups on any of the 8 subscales: Physical Functioning (P = .7509), Role Physical (P = .6380), Bodily Pain (P = .4433), General Health (P = .3514), Vitality (P = .9062), Social Functioning (P = .4690), Role Emotional (P = .7127), and Mental Health (P = .7169). There were also no statistically significant differences in the IKDC PCS and MCS scores between the 2 groups, as Table 3 shows.
Modified Lysholm Knee Score
The mean modified Lysholm score was 21.0 ± 2.4 in the adolescent group and 22.3 ± 1.9 in the young adult group (Table 3). While the mean and median scores were likewise numerically similar between the 2 groups, a between-group comparison yielded a significant difference, with a P value of .0123.
MOCART Score
The MOCART scores were not significantly different between the adolescent and young adult groups (74.7 ± 12.0 and 77.2 ± 11.2, respectively) (Table 3).
Treatment Failure
One adolescent patient and 2 young adult patients, corresponding to 3% in the adolescent group and 5% in the young adult group, were identified as treatment failures. These small numbers did not allow a meaningful statistical comparison.
The adolescent patient was female, was 15 years old, and had a body mass index (BMI) of 21.6 kg/m2 at the time of ACI for the treatment of a traumatic cartilage defect on the femur (4 cm2) and patella (1 cm2) due to recurrent patellar dislocations and concomitant MPFL reconstruction. The duration of symptoms was 2 months, and treatment failure was experienced after approximately 34 months. She underwent another ACI procedure.
One young adult patient was male, was 23 years old, and had a BMI of 21.4 kg/m2 at ACI for the treatment of a 7-cm2 nontraumatic defect of the medial femoral condyle. He had a history of revision ACL reconstruction with ipsilateral patellar tendon and hamstring grafts and partial medial meniscectomy and experienced treatment failure after 27 months, with osseous formation in the ACI area. He underwent a reoperation including removal of the implant.
The other young adult patient was also male, was 34 years old, and had a BMI of 22.6 kg/m2 at ACI for the treatment of a 6-cm2 patellar defect associated with swelling and anterior knee pain. He had no prior surgical procedures and experienced treatment failure after 43 months, with hypertrophy of the trochlear cartilage. The patient underwent surgical removal of hypertrophic tissue.
Discussion
The most important finding of this study is that there was no difference in functional outcomes between patients aged 15 to 17 years and those aged 18 to 34 years. All patients attained high functional scores on the IKDC, KOOS, Lysholm, and MOCART measures, indicating a high rate of clinical success with third-generation MACI using spheroids.
Several studies have reported good or excellent functional outcomes for adolescent patients undergoing ACI for cartilage defects. 5,14,16,17,39 However, those studies used different outcome parameters and different generations of ACI. Macmull et al 14 published a case series of 31 patients undergoing ACI at a mean age of 16.3 years with a mean follow-up period of 66.3 months. In their study, all generations of ACI were included, but they did not differentiate between the ACI generations. Ogura et al 23 described the long-term results for 29 adolescent patients undergoing ACI with either a periosteal or collagen membrane cover. They reported an 89% survival rate after 10 years with excellent results in terms of outcome measures, and they concluded that ACI might even prevent the progression of osteoarthritis. 23 However, this hypothesis remains unproven, as there was no control group, which indeed would have been ethically unjustifiable, as it would have required symptomatic cartilage lesions to remain untreated.
A direct comparison of results between studies is difficult owing to the variety of outcome measures used. The ICRS recommended the IKDC and KOOS for providing validated outcomes in patients undergoing cartilage repair procedures. 29 Cvetanovich et al 4 reported a significant increase in KOOS and IKDC scores in adolescent patients after a mean follow-up period of 4.6 years, with IKDC scores considerably lower than those found in the present study (64.4 vs 81.1, respectively). However, they used first- or second-generation ACI, and concomitant procedures (such as patellar realignment or meniscal allograft transplantation) were performed in 22 of the 37 study patients, which might account for differences in outcome scores. IKDC scores were also provided in the study of Niethammer et al, 21 who described a matched-pair analysis of adolescent and adult patients undergoing ACI. They reported an IKDC score of 80.2 after 2 years and 77.5 after 3 years in the adolescent group, while the IKDC score in the adult group did not exceed 57.5, which was reached at the 2-year assessment. The score for the adolescent group was consistent with that for this study of 81.1 after 4 years, while the values for the adult group clearly differed from our results of IKDC score of 80.5 after 4 years. This might account for the fact that in our study, no significant differences between adolescent and adult patients were observed, in contrast to the results of Niethammer et al. 21 While the mean defect size was comparable with that in the current study, the reasons for the differing results are unclear. The differences in the mean age might be an explanation, as the mean age in the adult group was 10 years lower in the current study (26.5 ± 4.9 years) than in that of Niethammer et al 21 (36.7 ± 8.2 years).
The influence of age on functional outcomes after ACI is still a matter of debate. While some studies have shown better results for younger patients, 13,16 others have failed to show a correlation with age. 28,34 However, different cut-off values in age were applied, making a direct comparison difficult. In the study by Niethammer et al, 21 better results for the adolescent group were reported compared with adult patients, with adolescent patients defined as those younger than 20 years. Schmal et al 32 also suggested the age of 20 years as a cutoff in cartilage maturity between adolescents and adults. However, this is not consistent with the closure of epiphyseal growth plates. 32
Epiphyseal status is a commonly used method to determine bone maturity, and open epiphyseal growth plates are commonly used as a justification for restricting ACI. From a medical perspective, however, this seems to be of minor importance for cartilage regeneration therapy. Skeletal maturity is defined by the closure of the growth epiphyses, which normally occurs around the age of 15 years. Epiphyseal status is of major importance concerning fracture healing or limb correction, as bone has an increased potential for self-correction before closure of the epiphyses has occurred. 25 However, it does not allow a conclusion about cartilage maturity and cartilage regeneration potential. Furthermore, as the epiphyses are located metaphyseally, affecting during cartilage therapy is unlikely to occur. It has been shown that outcomes after ACI are correlated with the expression of cartilage markers. 20 Hence, cartilage markers seem to be a more valid measure of regeneration potential than epiphyseal status. Some studies have found no differences in outcome parameters between open and closed epiphyses after ACI, further supporting this view. 4,21,23 This is also in accordance with the findings of the present study, in which no differences in outcome parameters were noted between patients with open and closed epiphyses. However, only 8 patients in this study had open physes, so further investigations are warranted.
The current marketing authorizations granted for chondrocyte medicinal products (co.don chondrosphere) approve ACI for the treatment of patients younger than 18 years and with closed epiphyses. However, regulations and/or legislations are adopted according to the legal consensus, that is, the age in a legal rather than a medical or biological sense. This might restrict future treatment of patients aged below 18 years owing to governmental regulations. Therefore, there is a need for studies evaluating patients younger than 18 years to gather further information on the applicability and safety of ACI in these patients.
The rate of revision surgery or treatment failure after ACI has been reported as between 10% and 69% in earlier studies. 4,21,23 Revision surgery has most commonly been performed for chondral debridement owing to graft hypertrophy. Graft hypertrophy is the most common complication in periosteum-covered ACI, with incidence rates reported between 9% and 40%. 10,12,19,42 In this study, treatment failure rates were considerably lower, with 3% in the adolescent group and 5% in the young adult group identified as failures, and with only 1 revision for graft hypertrophy (in the young adult group). These results might be attributable to the third-generation MACI procedure used in this study, as other studies commonly reported on the results of periosteum-covered ACI, which has been linked with the emergence of graft hypertrophy. 9,27
This study has certain limitations that are caused by the restricted number of patients and its retrospective design, which is also responsible for the longer follow-up time in adolescents. Furthermore, no baseline data for the adolescent population could be obtained because of the retrospective design. Therefore, changes from baseline between groups could not be evaluated. However, outcome scores were within the range of cartilage-restoring procedures and showed satisfactory results. Also, the number of concomitant surgical procedures differed between the groups, but as most of the procedures had been undertaken in the adolescent population, one would assume even worse results because of these procedures. Furthermore, this study could only show midterm effects, and no different surgical treatment was evaluated as a control group. However, it contributes to the very limited knowledge of third-generation ACI in children and adolescents, which is still a rarely used therapy.
Conclusion
Based on the results of this study, third-generation MACI using spheroids appears to be an effective treatment for large cartilage defects of the knee at midterm follow-up. Furthermore, results for adolescents seem to be comparable with those for young adults. This technique appeared to be safe and effective in adolescents with open physes. We recommend that this therapy be allowed in children and adolescents so that prospective randomized trials can be performed to better clarify the long-term results of this treatment in young patients with cartilage defects.
Footnotes
Acknowledgment
The authors thank F.-J. Bartilla, MD (St Marien-Hospital Buer), S. Hartmann, MD (MedArtes Orthopaeden und Chirurgen im Raum Woerth), S. Roessing, MD (Orthopaedie an den Planken Mannheim), C. Sobau, MD (ARCUS Sportklinik Pforzheim), W. Zinser, MD (St Vinzenz-Hospital Dinslaken), O.J. Braunsperger, MD (Orthozentrum Rosenheim), H.-G. Fieseler, MD (Zentrum fuer Orthopaedische Chirurgie Hannoversch Muenden), J. Hennings, MD (Park-Klinik Manhagen), T. Kolombe, MD (DRK Krankenhaus Luckenwalde), N. Langen, MD (Sonneberger Orthopaediezentrum Bremen), V. Laute, MD (Gelenk- und Wirbelsaeulen-Zentrum Steglitz), D. Mann, MD (St Elisabeth-Hospital Guetersloh), and M. Sasse, MD (KOMMEDICO Traunstein) for recruiting patients and actively participating in the study.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was sponsored by co.don. A.H. is an employee of co.don. P.N. receives royalties for limited educational purposes from the European Union, AO Foundation, DePuy Synthes, TiGenix, and DKG and receives consulting fees from Arthrex and Stryker. S.F. is affiliated with Arthrex and Bauerfeind. K.R. has received royalties for medical leadership of this study. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Paul Ehrlich Institute (PEI.11507.01.1).