
Abstract
Background:
A habitual patellar dislocation (HPD) is a rare condition in skeletally mature patients, especially for those with severe quadriceps contracture. Until now, no study has reported the effectiveness of tibial tubercle proximalization to lengthen the extensor mechanism in treating severe HPDs in skeletally mature patients.
Purpose:
To describe a novel comprehensive procedure that includes tibial tubercle proximalization, extensive lateral release, tibial tubercle medialization, and medial patellofemoral ligament (MPFL) reconstruction in treating severe HPDs in skeletally mature patients and to report its early clinical outcomes.
Study Design:
Case series; Level of evidence, 4.
Methods:
From January 2014 to May 2016, a total of 43 consecutive patients (47 knees) with HPDs were surgically treated at a single institution and were retrospectively reviewed. Among them, 11 skeletally mature patients (11 knees) with severe primary HPDs underwent the index comprehensive procedure. Results of patellar tracking were recorded preoperatively and at the final follow-up. The radiological assessment included radiographs in standard anteroposterior, true lateral, and axial views and computed tomography scans at full knee extension before surgery and at the final follow-up. Subjective patellofemoral function was evaluated with the Kujala functional score before the index procedure and at the final follow-up visit.
Results:
The 11 included patients were evaluated for a mean period of 34.9 months (range, 25-46 months). The mean knee flexion angle when the patella dislocated laterally was 25° (range, 10°-30°) preoperatively. Radiologically, there was a statistically significant improvement in the congruence angle, from 73.4° ± 17.0° preoperatively to –7.1° ± 5.8° postoperatively (P < .01) and in the lateral patellofemoral angle, from –65.6° ± 9.4° preoperatively to 6.1° ± 2.7° postoperatively (P < .01). The mean preoperative Kujala functional score was 42.9, and the mean postoperative Kujala functional score was 95.2 (P < .05). No patients reported a recurrence of patellar dislocation at the final follow-up visit.
Conclusion:
The novel comprehensive procedure, including tibial tubercle proximalization, extensive lateral release, tibial tubercle medialization, and MPFL reconstruction, effectively treated lateral HPDs in skeletally mature patients with severe quadriceps contracture.
Keywords
A habitual patellar dislocation (HPD) is a rare condition. The cardinal physical sign in an HPD is that if the patella is forcibly held in the midline, it is impossible to flex the knee more than 90°. Further flexion is then possible only if the patella is allowed to dislocate, when a full range of motion (ROM) is readily obtainable. 1 –3
Various pathological factors have been described in the pathogenesis of HPDs, such as femoral trochlear dysplasia, increase in the Q angle, increase in the tibial tubercle–trochlear groove (TT-TG) distance, lateral soft tissue contracture, and medial soft tissue relaxation. 7 Jeffreys 8 in 1963 described an abnormal attachment of the iliotibial tract to the patella, producing HPDs in knee flexion. Later, Gunn 7 in 1964 described the association of quadriceps fibrosis with intramuscular injections to the thighs. He also put forward the idea that quadriceps contracture may sometimes give rise to dislocations of the patella. 7
A number of realignment procedures have been described in the literature for the management of HPDs in children. Among them, a treatment algorithm focusing on quadriceps lengthening is mandatory to reduce the patella in deep knee flexion. 9 Skeletally mature patients who have suffered from lateral HPDs often show a more severe degree of quadriceps contracture. Usually, the patella is forcibly held in the midline, and it is impossible to flex the knee more than 30° to 40°, indicating that the degree of quadriceps contracture is more severe than that in children. It is believed that HPDs in skeletally mature patients with severe quadriceps contracture require combined lengthening procedures. Until now, no study has reported the effectiveness of tibial tubercle proximalization to lengthen the extensor mechanism in addressing severe quadriceps contracture in the treatment of HPDs in skeletally mature patients.
The purpose of this study was to describe a novel comprehensive procedure in treating severe lateral HPDs in adults and to report its early clinical outcomes. The comprehensive procedure consisted of tibial tubercle proximalization, extensive release of the soft tissue lateral to the patella, tibial tubercle medialization, and medial patellofemoral ligament (MPFL) reconstruction. The key step of this comprehensive procedure is tibial tubercle proximalization, acting as a “bony release” of the extensor mechanism, which is easy to perform. The biggest advantage of tibial tubercle proximalization is rigid fixation, which ensures early postoperative rehabilitation and no risk of scar tissue formation from the quadriceps muscle. We hypothesized that skeletally mature patients with severe lateral HPDs would have satisfactory clinical outcomes after undergoing the index comprehensive procedure.
Methods
Study Design
This was a retrospective study. From January 2014 to May 2016, a total of 43 consecutive skeletally mature patients (47 affected knees) with HPDs were surgically treated in our department and were retrospectively reviewed. The inclusion criteria were as follows: (1) lateral HPDs with a severely contracted quadriceps muscle (knee flexion angle of patellar dislocations should be <30°); (2) the index comprehensive procedure should include tibial tubercle proximalization, extensive release of the soft tissue lateral to the patella, tibial tubercle medialization (surgical indication should be a TT-TG distance >15 mm), and MPFL reconstruction; and (3) the follow-up time should be more than 24 months after the index procedure. The exclusion criteria were as follows: (1) skeletal immaturity, (2) revision cases, (3) severe malalignment of the affected lower extremity (>10° of valgus) that required combined corrective osteotomy, (4) generalized joint laxity (>5/9 on the Beighton score 17 ), and (5) severe trochlear dysplasia after undergoing a combined trochleoplasty procedure. The application of the selection criteria ultimately left 11 patients (11 affected knees) (Figure 1). The patient group included 6 men and 5 women, with the right side involved in 7 patients and the left side involved in 4 patients. The mean age at the time of surgery was 29.5 years (range, 15-46 years). The mean follow-up period was 34.9 months (range, 25-46 months) (Table 1). This study was approved by our institutional review board, and patient consent was obtained.
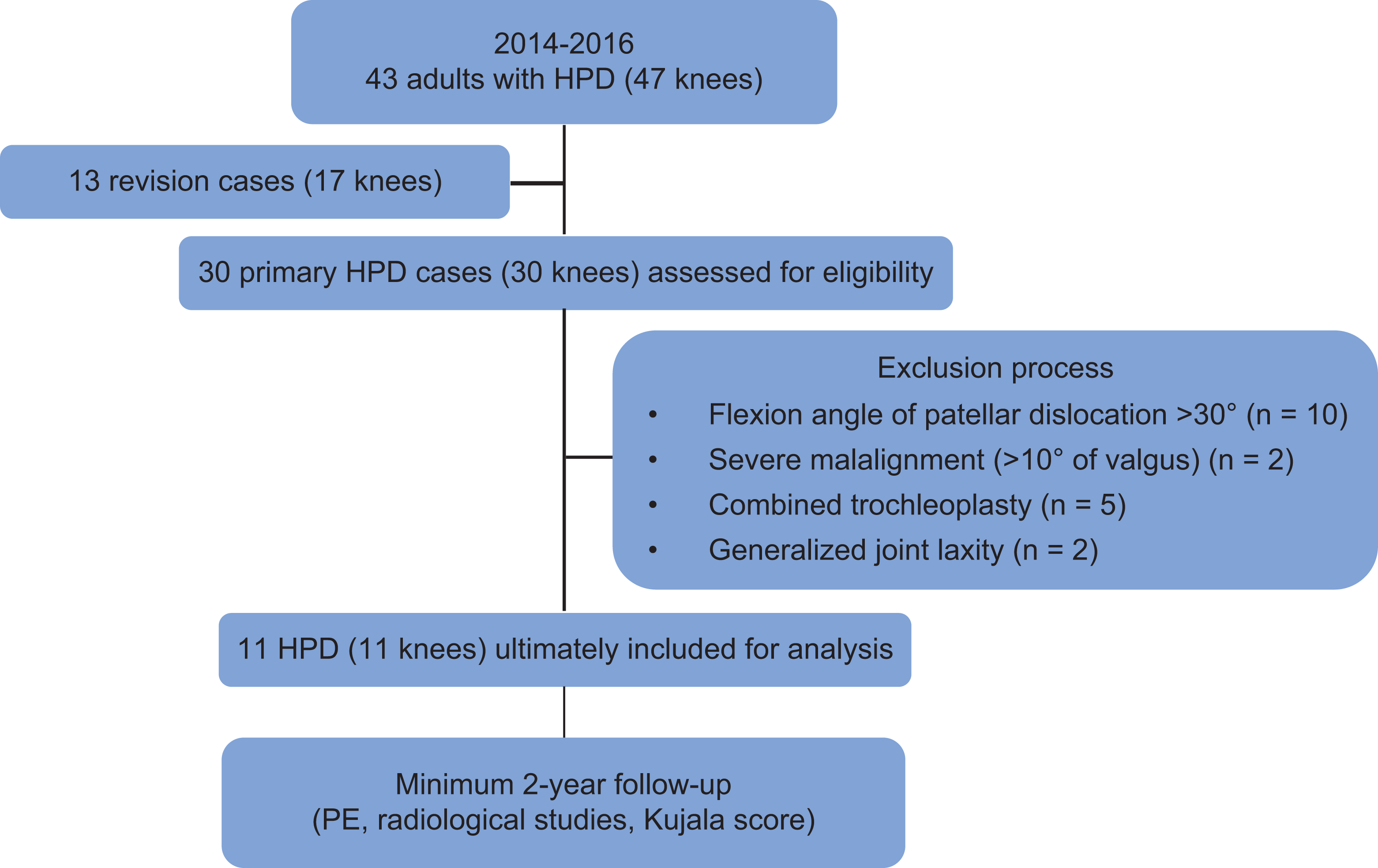
Flowchart of patient selection. HPD, habitual patellar dislocation; PE, physical examination.
Summary of Patient Data

Physical Examination
Preoperatively, dynamic patellar tracking throughout the full ROM was evaluated. The knee flexion angle when the patella dislocated laterally was then recorded. In addition, results of the apprehension tests and patellar tracking were evaluated at the final follow-up.
Radiological Imaging
The radiological diagnosis was based on radiographs, including routine anteroposterior views, true lateral views at 30° of knee flexion, and axial views of the patellofemoral joint at both 30° and maximum angle of knee flexion. Computed tomography (CT) scans of both knees were obtained with the knees at full extension. On the lateral knee radiographs, the Caton-Deschamps index 4 was used to measure patellar height. The Dejour classification system 13 was used to evaluate the degree of trochlear dysplasia. The shape of the patella according to the Wiberg and Baumgartl classification system, 18 the congruence angle, and the lateral patellofemoral angle were evaluated on axial views of the patellofemoral joint.
Surgical Techniques
Patellar dynamic tracking and lateral dislocations of the patella were evaluated routinely before surgery under anesthesia (Video Supplement 1) and intraoperatively after each step of the comprehensive procedure was performed. A midline incision was made from 5 cm above the patella to 10 cm below the patella to expose the quadriceps muscle and tibial tubercle (Figure 2). Intra-articular pathological findings were recorded, including the grade of chondromalacia in each facet of the patella and the lateral femoral condyle according to the Outerbridge classification system. 14
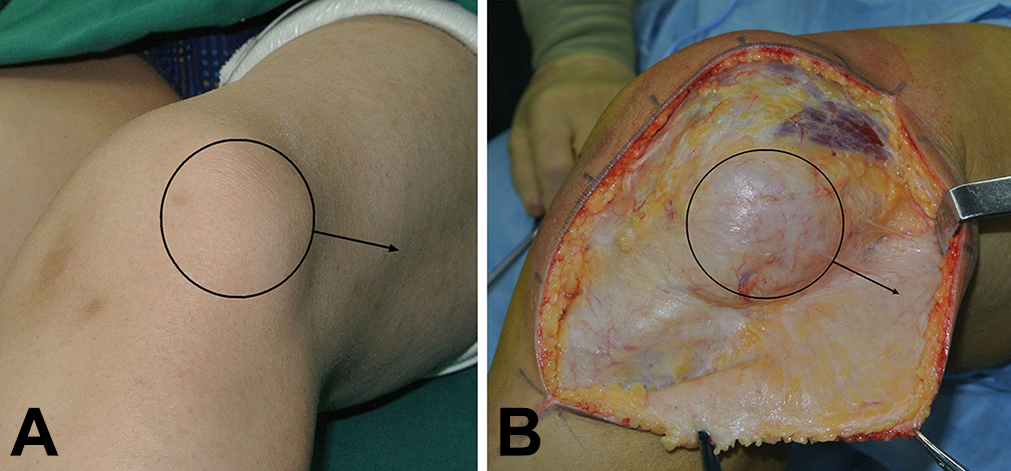
(A) Preoperatively, the patella (circle) dislocated laterally (arrow) at about 30° of knee flexion. (B) A midline incision was made to expose the laterally dislocated patella (circle and arrow).
“Step-by-Step” Extensive Lateral Release
Release of the lateral retinaculum was performed first. Then, the abnormal connection between the iliotibial band and the patella was released (Figure 3). The release site was then extended proximally along the patella to resect the vastus lateralis tendon. Usually, an “L-shaped” release was achieved by a “horizontal” release first to resect the distal part of the vastus lateralis tendon from its patellar attachment site, followed by a “longitudinal” release along the interval between the vastus lateralis tendon and the rectus femoris tendon. Finally, the distal part of the vastus lateralis tendon was sutured back to the proximal part of the rectus femoris tendon without tension (Figure 4) at 90° of knee flexion. Patellar tracking was then checked by flexing the knee joint. Usually, the patella could be stabilized in the trochlear groove during early knee flexion; however, it would redislocate laterally when the knee was flexed beyond 90°. Further distal realignment procedures were needed.

(A) The lateral retinaculum was released first from the lateral edge of the patellar tendon, proximal along the lateral edge of the patella (purple dashed line). (B) By using a surgical scissor, lateral release was performed (black arrow). ITB, iliotibial band; P, patella; PT, patellar tendon; TT, tibial tubercle.

(A) “L-shaped” release was achieved by a “horizontal” release first to resect the distal part of the vastus lateralis tendon from its patellar attachment site, followed by a “longitudinal” release along the interval between the vastus lateralis tendon and the rectus femoris tendon (arrow). (B) Finally, the distal part of the vastus lateralis tendon was sutured back to the proximal part of the rectus femoris tendon (arrow).
Tibial Tubercle Proximalization and Medialization
Meticulous separation was first made to expose the tibial tubercle and the insertion of the patellar tendon. Further separation was then performed between the patellar tendon and the infrapatellar fat pad. Osteotomy of the tibial tubercle was performed with a saw and osteotome. The length of the osteotomy site created was about 8 cm. The fibrotic medial capsule around the inferior portion of the patella was then released so that the tibial tubercle could be displaced proximally to lengthen the extensor. Usually, the bone block was displaced superiorly about 10 mm initially and then temporarily fixed with 2 guide pins, after which patellar tracking was again checked with the same maneuver described above. Meanwhile, if the TT-TG distance was greater than 15 mm, the tibial tubercle was then displaced medially, aiming to correct the TT-TG distance to less than 10 mm. After both proximal and distal realignment procedures have been completed, the knee should be able to flex over 90° with no tendency to lateral dislocation or subluxation. If a lateral dislocation still existed in a deep flexion angle, further tibial tubercle proximalization was performed until the patella did not dislocate laterally throughout the full ROM of the knee joint. After confirmation of normal patellar tracking, the bone block was secured with 2 or 3 cortical screws (Figure 5).

(A) Osteotomy of the tibial tubercle was performed, and the tibial tubercle, A, was displaced proximally to lengthen the extensor, B. (B) After confirmation of normal patellar tracking, the bone block was secured with 2 cortical screws.
MPFL Reconstruction
The patellar glide test at 30° of knee flexion was then performed. If the result was positive, MPFL reconstruction was indicated. The MPFL was reconstructed using a semitendinosus tendon autograft. Two double-loaded suture anchors were inserted into the patella. One of the suture anchors was inserted into the near proximal margin of the patella, and the other was inserted into the center of the medial facet of the patella. The femoral tunnel was positioned under fluoroscopy using the method described by Schoettle et al. 15 The double-strand semitendinosus tendon was fixed by the sutures loaded on the suture anchors. Then, the free ends of the graft were transmitted between the second and third layers of the knee joint, which was fixed with an interference screw within the femoral bone tunnel. The graft was fixed at 20° to 30° of knee flexion. As a result of the comprehensive procedure, the patella was stabilized throughout the full ROM (Video Supplement 2).
Postoperative Rehabilitation
A protective knee brace without limitations of ROM was applied for the first 6 weeks after surgery to protect the patients from reinjury. A crutch provided partial weightbearing during this period. In addition, isometric quadriceps muscle training started immediately after surgery. The degree of knee flexion allowed was gradually increased with time, depending on the stability of the patella and the strength of the quadriceps muscle.
Follow-up Evaluation
Healing at the osteotomy site of the proximal tibia was evaluated by radiography at about 3 months after surgery. Postoperative CT of the affected knee joint was performed at the final follow-up. The patellofemoral function of the knee joint with severe HPDs was evaluated preoperatively and at the final follow-up visit using the Kujala functional score, 10 which includes a variety of symptoms of anterior knee pain related to daily activities and signs of patellar instability.
Statistical Analysis
Results of the physical examinations, radiological imaging, and functional evaluations of all the affected knee joints were collected. Preoperative and postoperative results were compared with the paired t test using the SPSS 18.0 software package (IBM). Statistical significance was set at P < .05.
Results
All patients experienced an insidious onset of the HPD, with no obvious history of multiple muscular injections in the involved thigh during childhood. No case was associated with significant trauma that had induced the HPD. During the follow-up, no patient reported the recurrence of patellar dislocation after the index comprehensive procedure. There was no instance of complications related to bony healing of the tibial tubercle osteotomy site. No complication involving skin necrosis or postoperative fractures of the tibia or patella was observed.
The mean knee flexion angle when the patella dislocated was 25° (range, 10°-30°) preoperatively. The major intraoperative finding was contracture of the lateral patellar retinaculum with fibrotic bands in the superolateral aspect of the patella. Chondromalacia of the patella was grade III in 5 knees and grade IV in 6 knees according to the Outerbridge classification system. The major location of involvement was the medial facet of the patella. Erosion of the corresponding lateral femoral condyle was noted in every knee. The amount of correction averaged 15.5 mm (range, 10-30 mm) for tibial tubercle proximalization and 12.9 mm (range, 10-15 mm) for tibial tubercle medialization (Table 2).
Details of Operative Procedures a
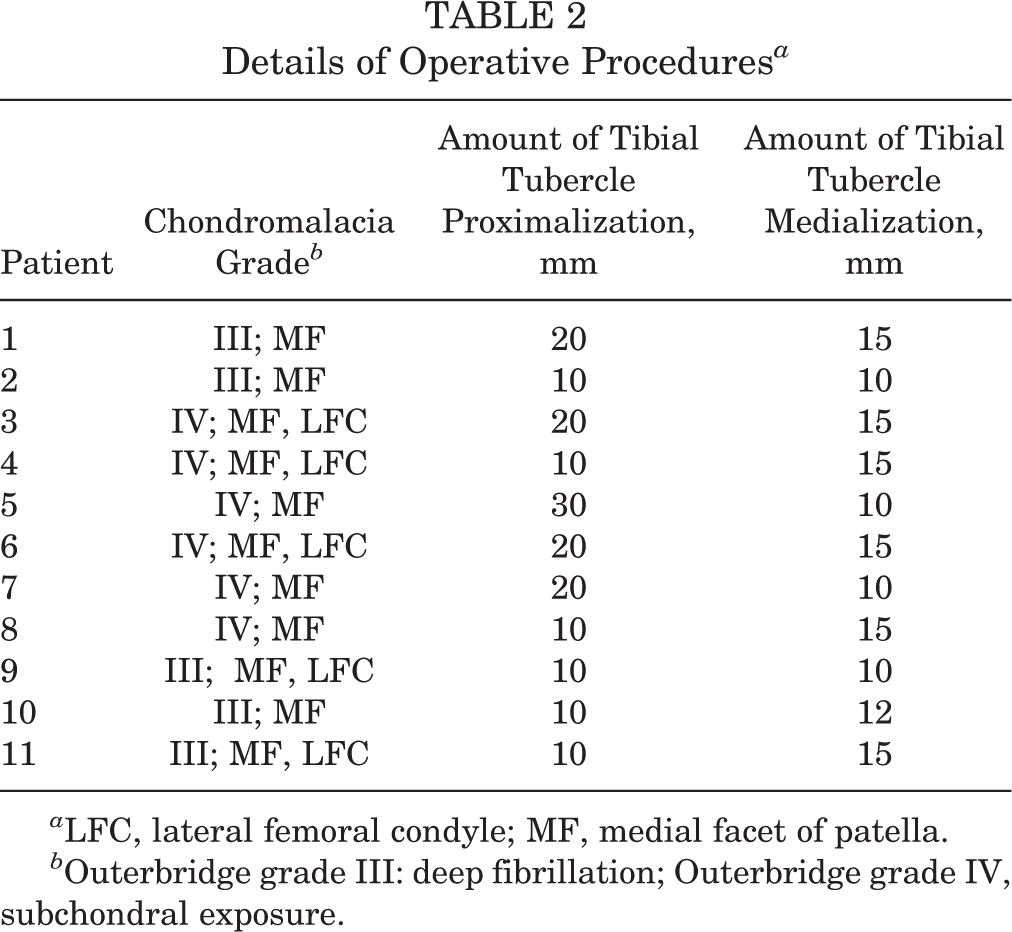
a LFC, lateral femoral condyle; MF, medial facet of patella.
b Outerbridge grade III: deep fibrillation; Outerbridge grade IV, subchondral exposure.
Radiologically, there was a statistically significant improvement in the congruence angle, from 73.4° ± 17.0° (range, 55° to 102°) preoperatively to –7.1° ± 5.8° (range, –20° to 3°) postoperatively (P < .01) and in the lateral patellofemoral angle, from –65.6° ± 9.4° (range, –83° to –54°) preoperatively to 6.1° ± 2.7° (range, 3° to 11°) postoperatively (P < .01). There was a significant change in the Caton-Deschamps index, with a mean of 0.94 ± 0.09 (range, 0.82-1.10) before surgery and 1.18 ± 0.12 (range, 1.04-1.35) after surgery (P < .05). The mean TT-TG distance decreased from 22.09 ± 1.97 mm (range, 19-25 mm) preoperatively to 9.18 ± 1.08 mm (range, 8-11 mm) postoperatively (Table 3).
Results of Radiological Measurements a

a Post, postoperative; pre, preoperative; TT-TG, tibial tubercle–trochlear groove.
b Negative values indicate a normal patellofemoral relationship.
c Negative values indicate abnormal lateral patellar tilt.
d According to the Wiberg and Baumgartl classification system. 18
e According to the Dejour classification system. 13
The Kujala functional score for the 11 knees improved from a mean value of 42.9 preoperatively to 95.2 postoperatively (P < .05). All patients returned to their daily walking activities without any trouble. Ten of the 11 patients were able to participate in running with no limitations. Only 1 patient had painful crepitus and constant pain during squatting and prolonged sitting with the knee flexed because of severe patellofemoral arthrosis. No further dislocation of the patella was noted after the index procedures (Table 4 and Video Supplement 3).
Summary of Kujala Score a

a Mean score of the 11 knees.
Discussion
Habitual dislocations of the patella are uncommon and are usually detected in children. The typical clinical presentation of an HPD in young children is an odd-looking knee and, less often, pain and instability. 2 Contracture and fibrosis of the quadriceps muscle, mainly the vastus lateralis, 1 and iliotibial band contracture 11 may give rise to HPDs. In this study, all of the included patients developed HPDs as children, presenting many years after their initial instability event. It was also speculated that HPDs left untreated for many years resulted in quadriceps contracture. Therefore, various soft tissue procedures, targeted on lateral release and quadriceps lengthening, are mandatory in the treatment algorithm of HPDs. Bergman and Williams 3 reported good clinical results from a consecutive series of 35 cases of HPDs in children treated with extensive lateral release and lengthening of the rectus femoris. Later, Gao et al 6 reported satisfactory results in 87.8% of patients treated with similar procedures.
Until now, there have been only 2 clinical studies that described the surgical techniques for addressing HPDs in skeletally mature patients. Matsushita et al 12 reported the effectiveness of combined MPFL reconstruction and lateral soft tissue release on 2 skeletally mature patients with HPDs. Shen et al 16 performed both proximal and distal realignment procedures including lateral release, medial retinacular advancement, and anteromedial tibial tubercle transfer on 13 knees with HPDs in skeletally mature patients and reported satisfactory results. These 2 studies did not provide details about the degree of quadriceps muscle contracture. In addition, they did not perform quadriceps lengthening procedures. In the current study, the mean knee flexion angle when the patella dislocated laterally was 25° (range, 10°-30°) preoperatively. Moreover, with further knee flexion, the patella could not reduce to the midline, demonstrating severe quadriceps contracture. We believed that a combined quadriceps lengthening procedure was mandatory in treating these patients.
However, quadriceps lengthening may result in extensor lag during the postoperative rehabilitation period. In addition, a few complications related to quadriceps lengthening have been reported, including wound hematoma, wound dehiscence, or reformation of quadriceps contracture. 1 For skeletally mature patients with severe quadriceps contracture, the quadriceps lengthening procedure (Judet quadricepsplasty, proximal rectus femoris release, V-Y quadriceps tendon lengthening procedure), also called “soft tissue release,” may not be an ideal treatment option, as scar tissue formation in skeletally mature patients is much worse the situation in skeletally immature patients. Tibial tubercle proximalization, also called “bony release,” could be another option. The biggest advantage of tibial tubercle proximalization is rigid fixation, which ensures early postoperative rehabilitation and no risk of scar tissue formation from the quadriceps muscle.
One potential concern of tibial tubercle proximalization is patella alta postoperatively. Admittedly, tibial tubercle proximalization will increase the patellar height and sometimes even result in patella alta, as found from the results of this study (Figure 6). Patella alta is a known risk factor for patellar instability. The reason why it did not lead to the recurrence of patellar dislocation in this study might be the other associated procedures (tibial tubercle medialization and MPFL reconstruction). Additionally, with adequate physical therapy, there was no “extensor lag” phenomenon found in this study during postoperative rehabilitation. The postoperative Kujala functional score showed that the patients could perform daily activities without difficulty. Moreover, during surgery, the patellar height could be precisely adjusted under fluoroscopy before final fixation. Usually, the bone block was proximally displaced about 10 mm initially and then every 5 mm each time until patellar tracking was corrected to normal throughout the full ROM of the knee joint. To guarantee that the patella stayed in the trochlear groove in terminal knee flexion was another important step while performing this combined procedure.
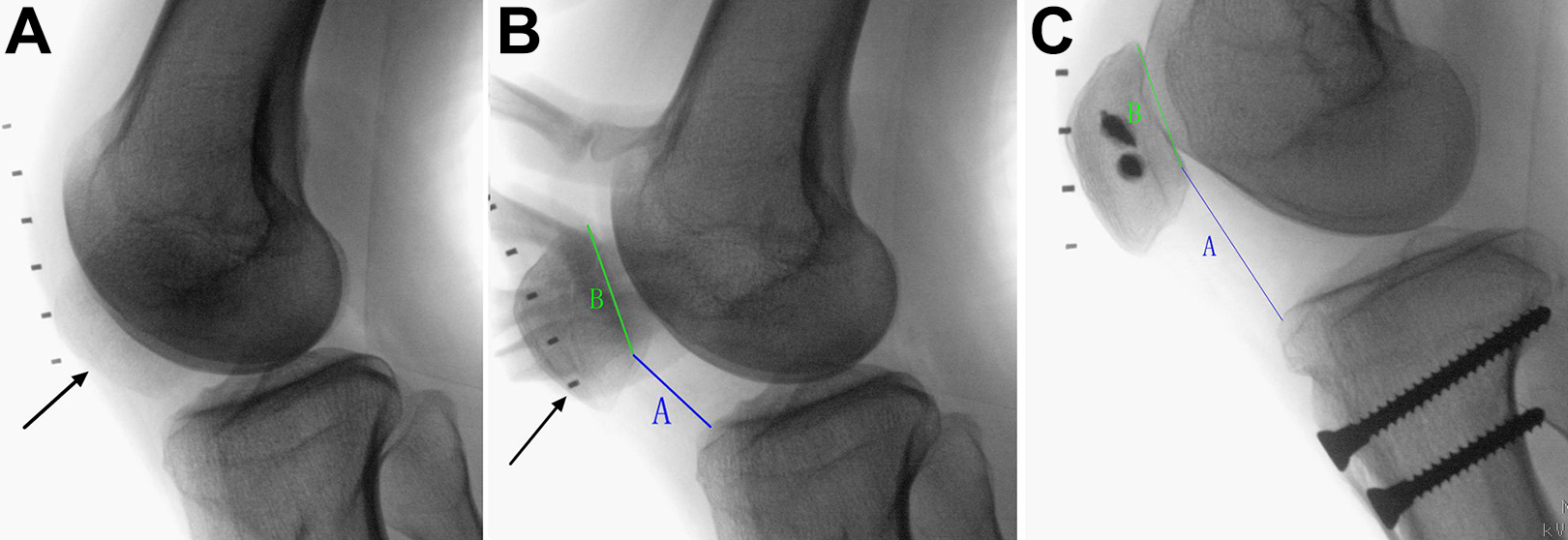
(A) Preoperative lateral radiography shows a laterally displaced patella (arrow) when the knee flexes. (B) When the patella (arrow) is forcibly pushed into the midline by the examiner’s finger, lateral radiography shows the Caton-Deschamps index: A/B = 0.85. (C) At the final follow-up, the osteotomy site healed completely, and the Caton-Deschamps index was A/B = 1.25.
The MPFL is the major medial ligamentous stabilizer in preventing the lateral patellar dislocation, which has been clarified by previous biomechanical studies. 5 Insufficiency of the MPFL results in lateral patellar instability with excessive lateral displacement of the patella, especially when the knee is in early flexion. It should be mentioned that the main purpose of MPFL reconstruction in our comprehensive procedure was to prevent the patella from dislocating when the knee was in early flexion.
There are some limitations to this study. First, this was a retrospective study. Second, the sample size was relatively small, as an HPD in skeletally mature patients is a very rare condition; however, all of the study patients completed the comprehensive follow-up evaluations. Third, the follow-up time was relatively short, especially for the evaluation of patellofemoral arthritis. Further studies with a larger sample size and longer follow-up time are needed. Fourth, the flexion angle of lateral HPDs was less than 30° in this study. According to our clinical experience, if the flexion angle of lateral HPDs is more than 30°, tibial tubercle proximalization might not be necessary, as the degree of quadriceps contracture is not as severe as seen in our study patients. Last, the method used to measure the patellar height preoperatively was inaccurate because the patella dislocated laterally when the knee was in 30° of flexion. Therefore, the patella was forcibly held in midline by the examiner to obtain a good lateral view of the knee joint.
Conclusion
Multiple procedures are necessary for addressing HPDs in skeletally mature patients with severe quadriceps contracture. The procedures we described include tibial tubercle proximalization, extensive lateral release, tibial tubercle medialization, and MPFL reconstruction. In this study, the novel comprehensive procedure effectively treated lateral HPDs in skeletally mature patients with severe quadriceps contracture.
A Video Supplement for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/2325967119831642.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from the Beijing Municipal Administration of Hospitals (XMLX201613 to H.F.). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.