
Abstract
Background:
Habitual patellar dislocation in flexion (HPD-F) is a rare condition in skeletally mature patients. Current literature reports that tibial tubercle proximalization has achieved favorable clinical outcomes for such patients. However, there are no studies to date reporting the clinical outcomes of revision surgery for skeletally mature HPD-F patients after failure of the initial procedure.
Purpose:
To evaluate the clinical and radiological outcomes of combined extensive lateral release, tibial tubercle proximalization, and medial patellofemoral ligament (MPFL) reconstruction for the revision treatment of HPD-F in skeletally mature patients who have failed initial surgery.
Study Design:
Case series; Level of evidence, 4.
Methods:
This retrospective study included 28 skeletally mature patients with habitual patellar dislocation in flexion who underwent revision surgery. The cohort had a mean age of 25.3 years and were followed up for a mean of 3.1 ± 1.3 years. All patients underwent the combined procedure. Preoperative and postoperative evaluations included patient-reported outcome measures (Kujala, Tegner, and Lysholm scores), radiological assessments, and isokinetic knee extension strength testing. Further analysis assessed the influence of postoperative iatrogenic patella alta on outcomes.
Results:
None of the patients experienced subsequent episodes of instability. The mean outcome scores were as follows: Kujala, 84; Tegner, 4; and Lysholm, 81. Following tibial tubercle proximalization by a mean of 17 mm, the mean Caton-Deschamps index increased from 0.7 ± 0.3 preoperatively to 1.2 ± 0.4 postoperatively. The mean isokinetic peak torque of the quadriceps muscles significantly improved from 31 N·m to 59 N·m after surgery, and no patient exhibited “extensor lag” postoperatively. Further analysis showed no significant differences in quadriceps strength or patient-reported outcomes between the patella alta group (n = 9) and normal group (n = 19).
Conclusion:
Combined extensive lateral release, tibial tubercle proximalization, and MPFL reconstruction demonstrated favorable short-term clinical outcomes with a low complication rate in skeletally mature patients with HPD-F who had failed previous surgery. In this case series, tibial tubercle proximalization led to postoperative patella alta in approximately one-third of patients; however, this did not appear to affect short-term functional outcomes or quadriceps strength.
Keywords
Habitual patellar dislocation in flexion (HPD-F) represents a severe form of patellar instability, characterized by the patella dislocating with every knee flexion. 1 The trochlea has a greater capacity for remodeling when patellar stabilization is performed at a younger age, 15 highlighting the importance of timely surgical intervention aimed at realigning and stabilizing the patella. Multiple etiological factors contribute to the pathogenesis of HPD-F, with key pathological influences including a shortened quadriceps mechanism and lateral soft tissue contractures.1,8,23 The literature describes various proximal and distal realignment procedures aimed at addressing this form of patellar instability in pediatric patients. 1 A central component of these interventions is a treatment algorithm that emphasizes quadriceps lengthening,8,23 which is essential for improving patellar tracking during knee flexion.
While most patients treated in childhood achieve satisfactory outcomes, a small subset may experience patellar redislocation due to various factors.3,6,16 The current literature offers limited guidance on managing these complex failed cases. For patients with HPD-F who undergo unsuccessful initial surgery in childhood, revision surgery may be considered once skeletal maturity is reached. Surgical approaches in these revision cases often involve bony procedures focused on realigning and stabilizing the patellofemoral joint, contrasting with the predominantly soft tissue surgery used in pediatric patients. 25 To our knowledge, no studies have reported the clinical outcomes of revision surgery for skeletally mature patients with HPD-F. Therefore, the aim of this study is to evaluate the short-term clinical and radiological outcomes of combined extensive lateral release, tibial tubercle proximalization, and medial patellofemoral ligament (MPFL) reconstruction in skeletally mature HPD-F patients who failed initial surgery.
Methods
This study was conducted in accordance with the approval of the hospital's ethics board and adhered to all patient consent requirements. At the hospital where the study was conducted, skeletally immature patients with patellar instability were treated by the pediatric orthopaedics department, while surgical management for skeletally mature patients was handled by the sports medicine department. From April 2017 to December 2019, a total of 84 consecutive skeletally mature patients diagnosed with HPD-F underwent surgical treatment. Of these, 31 patients who required revision surgery because of patellar redislocation after their initial procedure were assessed in this retrospective review. No patients were revised for isolated pain or functional limitation without documented redislocation. All included patients underwent combined procedures. This combined approach included 3 key components: extensive lateral release, tibial tubercle proximalization, and MPFL reconstruction, with the specific technique for each component adjusted according to intraoperative findings. Patients were excluded if they were missing preoperative or postoperative imaging data (n = 2) or had postoperative follow-up of <2 years (n = 1). Ultimately, 28 patients who underwent revision surgery were included in this study (Figure 1). The mean clinical follow-up period was 3.1 ± 1.3 years (range, 2.0-4.6 years). The group consisted of 10 male and 18 female patients, with a mean age of 25.3 years.
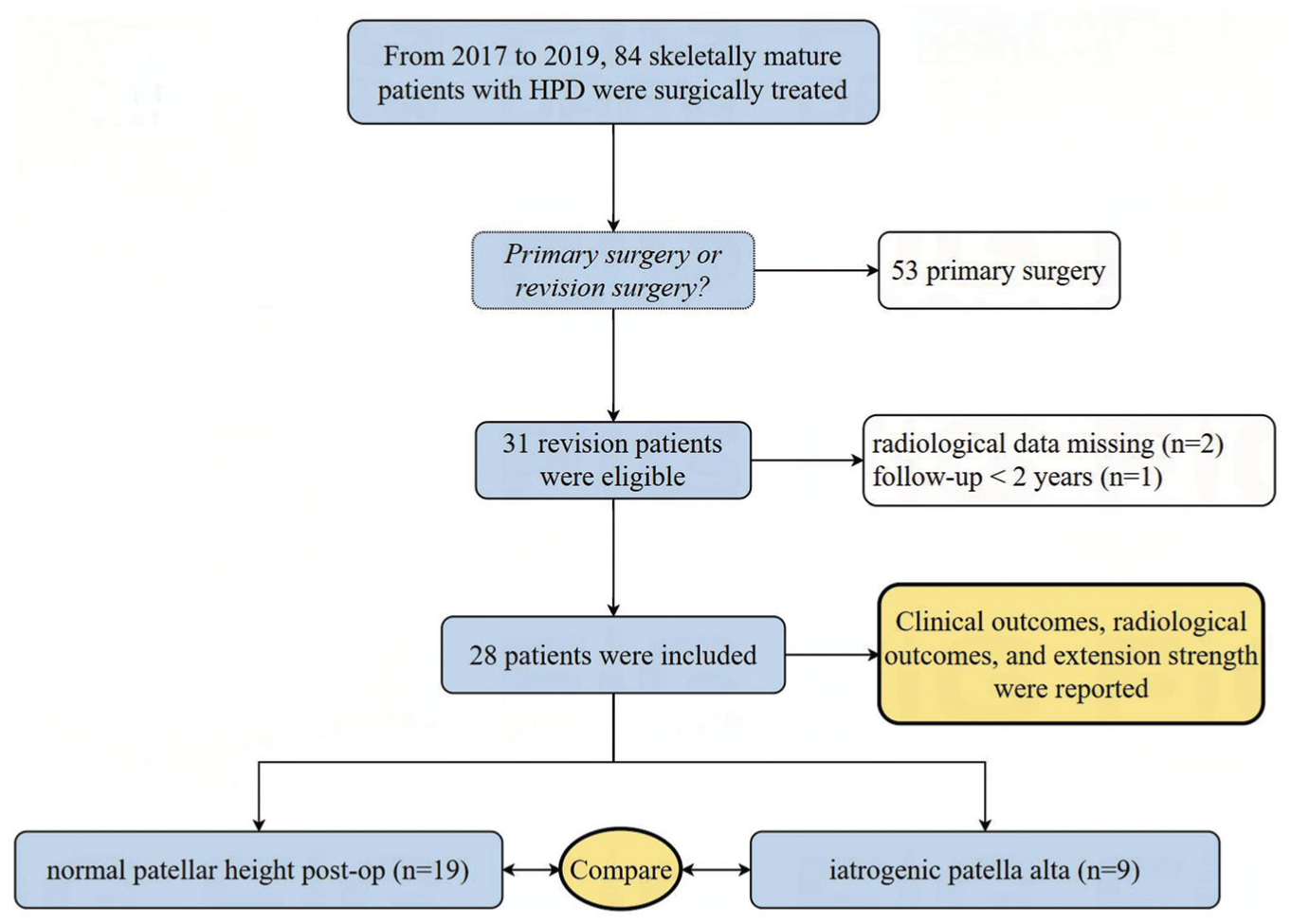
Flowchart of patient selection. HPD, habitual patellar dislocation.
Data Collection Methods
This study utilized a prospectively maintained institutional database with data sourced from (1) electronic health records (surgical details/radiological reports), (2) picture archiving and communication systems (pre-/postoperative imaging), and (3) electronically collected/stored patient-reported outcome (PRO) measures via clinic tablets with automated completeness checks. Two patients were excluded solely due to missing preoperative computed tomography (CT) scans, while PRO measures achieved 100% completeness through real-time electronic validation.
Clinical Assessment
The following data were systematically collected from medical records: sex, age at the time of initial and revision surgery, affected side (left or right), and the surgical methods used for both initial and revision procedures. Before surgery, a dynamic evaluation of patellar tracking throughout the full range of motion was performed for patients diagnosed with habitual patellar dislocation in flexion. The Kujala score, Tegner activity score, and Lysholm score were assessed preoperatively and at a minimum of 2 years postoperatively.
Isokinetic Knee Muscle Strength
To quantify knee muscle strength, isokinetic measurements were performed using a Biodex isokinetic dynamometer both before surgery and at the 2-year follow-up. Testing followed a validated protocol preprogrammed into the Biodex system, with knee flexion and extension evaluated at speeds of 60 deg/s and 180 deg/s (Figure 2). Patients were verbally encouraged to perform 5 full flexion and extension movements of the leg in an alternating sequence, exerting maximal muscle strength throughout. Quadriceps peak torque was recorded during the test.

Isokinetic muscle test results. (A) Preoperative isokinetic peak torque: 72 N·m. (B) Same patient, isokinetic peak torque: 127 N·m at the 2-year postoperative follow-up.
Radiological Measurement
All patients included in the study underwent CT scans and radiographs preoperatively and at the 2-year follow-up, including routine anteroposterior views, true lateral views at 30° of knee flexion, and axial views of the patellofemoral joint at both 30° and maximal knee flexion (Figure 3). Patellar height was assessed on lateral knee radiographs using the Caton-Deschamps index (CDI). 17 The degree of trochlear dysplasia was classified according to the Dejour classification system. 7 The mechanical femoral-tibial angle (mFTA) was measured on whole-leg standing anteroposterior radiographs to detect the presence of severe valgus deformity (mFTA ≥8°). 25 Additionally, patellar shape was categorized using the Wiberg and Baumgartl classification system. 13 Axial views of the patellofemoral joint were used to evaluate the congruence angle and the lateral patellofemoral angle. 21 The tibial tubercle–trochlear groove (TT-TG) distance was measured on CT scans. 2

(A) Anteroposterior radiograph of the knee. (B) True lateral radiograph of the knee at 30° flexion, showing lateral patellar dislocation, making it impossible to measure patellar height. (C) Axial views of the patellofemoral joint at maximal knee flexion, revealing lateral patellar dislocation. (D) Three-dimensional computed tomographic reconstruction of the knee joint.
Rotational deformities of the lower extremities were assessed according to a previously described method. 24 Femoral anteversion was defined as the angle between the axis of the femoral neck and the posterior condylar line of the distal femur. External tibial rotation was measured as the rotational angle between the distal and proximal tibia.
All radiographic measurements were performed independently by 2 orthopaedic surgeons using standardized protocols (Z.Z., D.W., blinded to patient identifiers and clinical outcomes). Measurement reliability was assessed by calculating inter- and intraobserver intraclass correlation coefficients (ICCs) using 20 randomly selected cases. The interobserver ICC values were: 0.92 for femoral anteversion, 0.91 for external tibial rotation angle, 0.93 for TT-TG distance, 0.90 for lateral patellofemoral angle, 0.87 for mFTA, 0.94 for the congruence angle, and 0.91 for CDI. Intraobserver ICCs showed similar excellent reliability (all >0.90).
Surgical Techniques
Extensive Lateral Release
A midline incision was made from 5 cm above the patella to 10 cm below it to expose the quadriceps muscle and tibial tubercle. During revision surgery, all cases exhibited tight distal/mid-lateral retinacula requiring release, but proximal retinacular integrity was not systematically evaluated. “Step-by-step” extensive lateral release was performed, following the technique described by Song et al. 21 The procedure began with a lateral retinacular release, followed by the release of the abnormal connection between the iliotibial band and the patella. The release was then extended proximally along the patella to partially resect the vastus lateralis tendon. Typically, this involved an “L-shaped” release: the process began with a “horizontal” release to detach the distal portion of the vastus lateralis tendon from its patellar insertion, followed by a “longitudinal” release along the interval between the vastus lateralis tendon and the rectus femoris tendon (Figure 4). Finally, the distal portion of the vastus lateralis tendon was reapproximated and sutured to the proximal part of the rectus femoris tendon without tension, with the knee held at 90° flexion.

Extensive lateral release and L-shaped lengthening of the vastus lateralis. (A) After performing an extensive lateral release, the vastus lateralis is incised along the junction between the vastus lateralis and the vastus internus. (B) The site of the vastus lateralis incision is shown (arrow). (C) At 90° of knee flexion, the vastus lateralis is sutured to the vastus internus without tension (arrow).
Patellar tracking was reassessed by gradually flexing the knee joint, and the flexion angle at which patellar dislocation occurred was recorded. After extensive lateral release, patellar tracking showed improvement compared with preoperative status. However, before tibial tubercle proximalization, all 28 cases still showed lateral patellar dislocation during deep flexion testing. This underscored the need for additional distal realignment procedures.
Tibial Tubercle Medialization and Proximalization
Meticulous dissection exposed the tibial tubercle and patellar tendon insertion. An osteotomy, approximately 5 cm in length, was performed at the tibial tubercle. The medial capsule around the lower patella was released to enable displacement of the tibial tubercle. In 5 patients with a preoperative TT-TG distance >20 mm, tibial tubercle medialization was initially performed, targeting a TT-TG distance of 10 mm. After medialization, the tibial tubercle was temporarily secured with Kirschner wires for provisional fixation, and patellar tracking was reassessed. However, no significant improvement in patellar tracking was observed. Subsequently, all patients underwent proximalization of the tibial tubercle (Figure 5). The bone block was initially displaced proximally by approximately 10 mm and temporarily fixed with guide pins. Patellar tracking was then reevaluated, and further proximal displacement was made as needed until the patella remained consistently reduced through the full range of motion. A trough was created in the tibia to accommodate the bone block, which was then secured with cortical screws.
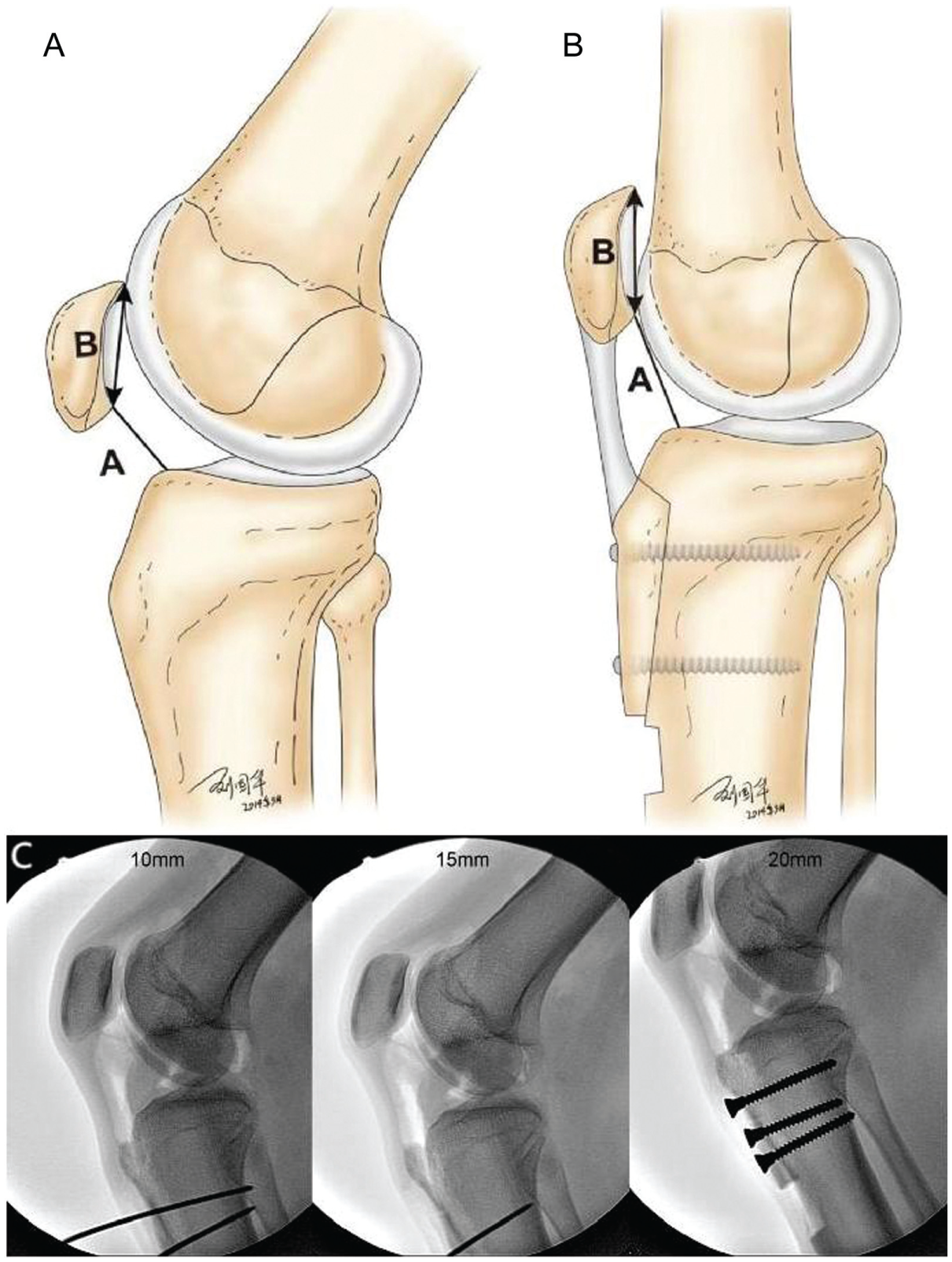
Proximalization of the tibial tubercle. (A) Schematic diagram of patella baja; A (straight line): the distance between the distal point of the patellar articular surface and the anterosuperior edge of the tibia; B (double-headed arrow): the length of the patellar articular surface. (B) Schematic diagram of tibial tubercle proximalization. (C) The initial proximalization distance was set to 10 mm. If patellar dislocation persisted throughout the full range of knee motion, the proximalization was incrementally increased by 5 mm until the patella remained reduced even at maximal knee flexion, then the bone block was finally secured with cortical screws.
MPFL Reconstruction
After completing the above steps, patellar tracking was normalized in all patients, with the patella remaining within the trochlear groove throughout the full range of knee motion. However, due to the deficiency of medial patellar stabilizing structures, lateral patellar dislocation still occurred when applying a lateral stress at 30° of knee flexion. Therefore, MPFL reconstruction was performed in all patients to restore patellar stability. The MPFL was reconstructed using a semitendinosus tendon autograft, under intraoperative fluoroscopy, following the method described by Schöttle et al. 19
Postoperative Rehabilitation
A protective knee brace without range of motion restrictions was applied for the first 4 weeks postoperatively. During this period, patients used crutches with partial weightbearing (<10 kg) for 4 weeks, followed by full weightbearing. The knee flexion angle was gradually increased each week as tolerated. Isometric quadriceps muscle training began immediately after surgery.
Statistical Analysis
Statistical analysis was performed using the SPSS 27 software package (IBM SPSS). Continuous variables were summarized as means and standard deviations, while discrete variables were described using counts and percentages. Categorical variables were presented with frequency distributions or as medians and interquartile ranges. Categorical data were compared using Pearson chi-square test or Fisher exact test, depending on the expected cell counts. Continuous variables were compared using either Student t test or the Mann-Whitney U test, based on the normality of the data distribution.
To evaluate the statistical power of the study, a post hoc power analysis was conducted using G*Power 3.1.9.7 software (Heinrich Heine University Düsseldorf). The effect size for the power analysis was determined to be 1.95, based on the Kujala score. With this effect size, a significance level (α) of .05 and a calculated power of 1.00 were achieved.
Results
PROs and Complications
None of the patients experienced subsequent episodes of instability. The median Tegner activity score significantly improved from 2 (IQR, 2-3) preoperatively to 4 (IQR, 3-5) postoperatively (P < .001). Similarly, both the Kujala and the Lysholm scores showed significant postoperative improvements (Table 1).
Clinical Outcomes and Quadriceps Strength Results a

Data are presented as mean ± SD or median (IQR) unless otherwise indicated. Bolded values indicate statistical significance at P < .05.
Comprehensive evaluation revealed the following complications: (1) knee stiffness requiring extended rehabilitation (3/28; 10.7%); (2) hardware irritation (3/28; 10.7%); (3) mild wound erythema without infection (2/28; 7.1%); (4) clinically insignificant intermuscular vein thrombosis detected on routine ultrasound (5/28; 17.9%). Notably, no cases developed nonunion, deep infection, compartment syndrome, or neurovascular injuries.
Radiological Measurement Results
The demographic information of the included cohort is summarized in Table 2. In 3 patients, the patella was already dislocated at 30° of knee flexion, and the preoperative CDI could not be measured. The mean preoperative CDI for the remaining 25 patients was 0.7 ± 0.3 (Table 3). Of these, 13 patients had patella baja, and none had patella alta preoperatively. At the final follow-up, the mean CDI was 1.2 ± 0.4, with 9 patients showing a CDI >1.2. All included patients exhibited trochlear dysplasia preoperatively, with type C trochlear dysplasia being the most common, accounting for 50% of cases.
Demographic Information of the Included Cohort (N = 28) a

Data are presented as mean ± SD or n (%) unless otherwise indicated. MPFL, medial patellofemoral ligament.
Pre- and Postoperative Radiological Information (N = 28) a

Data are presented as mean ± SD or n (%). Bolded values indicate statistical significance at P < .05. Dashes indicate that the data are not suitable for comparative analysis. CDI, Caton-Deschamps index; TT-TG, tibial tuberosity–trochlear groove.
Severe valgus was defined as a mechanical femoral-tibial angle ≥8°.
Radiologically, there was a statistically significant improvement in the congruence angle, from 73.4°± 17.0° preoperatively to −7.1°± 5.8° postoperatively, and in the lateral patellofemoral angle, from −65.6°± 9.4° preoperatively to 6.1°± 2.7° at the final follow-up (Table 3).
Quadriceps Strength Measurement Results
The isokinetic peak torque (N·m) during knee extension at 60 deg/s is summarized in Table 1. Although the postoperative isokinetic peak torque of the affected side remains significantly lower than that of the unaffected side, it shows a marked improvement compared with preoperative values.
Effect of Iatrogenic Patella Alta on Outcomes
Further analysis assessed the effect of postoperative iatrogenic patella alta on clinical outcomes. The results indicated no statistically significant differences in quadriceps muscle strength or PROs between the patella alta group (n = 9) and the normal group (n = 19) (Table 4).
Comparison Between Patients With and Without Iatrogenic Patella Alta a

Data are presented as mean ± SD or median (IQR) unless otherwise indicated.
Discussion
The most significant finding of this study is that the combined procedure produced favorable short-term clinical outcomes in skeletally mature HPD-F patients who had failed initial surgery. While some patients developed postoperative patella alta, this had minimal effect on knee extensor strength and functional outcomes.
Various techniques have been published to guide treatment; however, due to the severe nature of habitual patellar dislocation, MPFL reconstruction alone is insufficient to neutralize the deforming forces acting on the patella. 6 This necessitates the use of concomitant procedures, such as extensive lateral release, patellar ligament transfer, or quadriceps tendon lengthening, to restore normal patellar tracking as much as possible and reduce the risk of surgical failure.9,10,14,20 Among the various surgical techniques, quadriceps lengthening has become one of the most commonly used procedures, as it directly addresses the shortening of the knee extensor mechanism. 23 Although there are relatively few described quadriceps lengthening techniques for pediatric patellar instability, recent studies have shown promising results. Danino et al 3 performed a “4-in-1” procedure on 46 knees, combining the Roux-Goldthwait procedure, vastus medialis obliquus advancement, lateral release, and Galeazzi procedure, with 18% of knees experiencing recurrent instability. Similarly, Hidalgo Perea et al 6 performed quadriceps lengthening and concomitant MPFL reconstruction in 20 patients with obligatory patellar dislocation. Postoperative subjective functional scores were excellent, but 25% of patients experienced redislocation, with recent studies reporting a range of recurrent instability from 0% to 33%.11,12
Surgical strategies may vary for patients with HPD-F who are not treated until skeletal maturity. 22 In these cases, surgical approaches may include bony procedures aimed at realigning and stabilizing the patellofemoral joint, which differs from the predominantly soft tissue surgery performed in children. 25 Song et al 21 described a comprehensive procedure that included tibial tubercle proximalization, extensive lateral release, tibial tubercle medialization, and MPFL reconstruction for treating severe HPD-F in 11 skeletally mature patients. During a mean follow-up of 35 months, no patient experienced recurrent patellar dislocation or “extensor lag.” The quadriceps lengthening procedure commonly used in clinical practice, also referred to as “soft tissue release,” is an effective option. Another approach, tibial tubercle proximalization, termed “bony release,” offers the advantage of rigid fixation, which facilitates early postoperative rehabilitation and minimizes the risk of scar tissue formation in the quadriceps muscle.4,5,18 Similar to the risk of knee extension delay after quadriceps lengthening surgery, proximalization of the tibial tubercle may alter the resting length of the muscle-tendon unit, potentially weakening effective muscle contraction and strength despite an improved range of motion. This can lead to reduced functional strength in the quadriceps postoperatively. However, with adequate physical therapy, no extensor lag was observed in this study during postoperative rehabilitation.
It is acknowledged that tibial tubercle proximalization increases patellar height and may even result in patella alta, as noted in the study's findings. Nevertheless, this iatrogenic patella alta did not have a significant effect on short-term clinical outcomes. During the combined surgery, patellar height could be precisely adjusted under fluoroscopy before final fixation. Typically, the bone block was initially displaced proximally by about 10 mm, with subsequent 5-mm adjustments made until patellar tracking was normalized throughout the full range of motion. Ensuring that the patella remained within the trochlear groove during terminal knee flexion was also a critical step in performing this combined procedure.
While our study demonstrates that iatrogenic patella alta did not significantly affect short-term outcomes, several important considerations remain regarding its potential long-term effects. The elevated patellar position may theoretically (1) reduce trochlear engagement in early flexion, increasing instability risk; (2) alter quadriceps lever arm mechanics, potentially leading to extensor weakness; and (3) accelerate patellofemoral joint degeneration due to altered contact pressures. These concerns suggest our procedure may be particularly advantageous for patients with preexisting patella baja, where proximalization serves to normalize patellar height rather than create pathological alta. For patients with normal preoperative patellar height, we recommend cautious incremental proximalization (2- to 3-mm steps) under direct fluoroscopic visualization to avoid excessive elevation. Future studies should evaluate long-term outcomes to assess whether patella alta affects late instability or arthritic progression.
To our knowledge, this is the first study to report the clinical outcomes of revision surgery for HPD-F in skeletally mature patients. This study underscores the clinical relevance of combined extensive lateral release, tibial tubercle proximalization, and MPFL reconstruction in treating skeletally mature patients with habitual patellar dislocation who failed initial surgery. The procedure demonstrated favorable short-term outcomes and a low complication rate, with improvements in functional scores and quadriceps strength, despite some cases of postoperative patella alta. This comprehensive surgical approach effectively addresses the complexities of HPD-F in adults and fills a significant gap in the literature regarding revision surgery for this condition, offering valuable insights for future clinical practice.
Limitations
This study has several limitations. First, it is a retrospective study with a relatively small sample size, which may limit the generalizability of the findings. Second, although all cases involved failed initial surgery, the surgical methods used in the initial interventions were neither uniform nor standardized, complicating the objective analysis of the reasons for these failures. While our combined revision procedure demonstrated favorable outcomes, its application must be individualized based on patient-specific factors including (1) the type of previous failed procedure, (2) residual anatomic deficiencies (patella baja, trochlear dysplasia grade), and (3) dynamic patellar tracking patterns. This underscores that surgical planning for revision HPD-F requires comprehensive preoperative evaluation—including advanced imaging and functional assessment—rather than the adopting of a single approach. Third, the absence of a control group prevents a direct comparison of the advantages and disadvantages of tibial tubercle proximalization versus quadriceps femoris lengthening. Fourth, this study did not quantitatively assess the relationship between specific trochlear dysplasia patterns (eg, Dejour classification) and lateral condylar hypoplasia, as our primary endpoint was functional improvement after revision surgery. Future dedicated anatomic studies with larger samples are needed to evaluate how these structural variations influence surgical decision-making. Last, the follow-up period was relatively short, leaving unclear the long-term effects of tibial tubercle proximalization. Future studies with larger sample sizes, standardized initial surgical methods, control groups, and longer follow-up periods are needed to validate and expand upon these findings.
Conclusion
Combined extensive lateral release, tibial tubercle proximalization, and MPFL reconstruction demonstrated favorable short-term clinical outcomes with a low complication rate in skeletally mature patients with HPD-F who had failed previous surgery. In this case series, tibial tubercle proximalization led to postoperative patella alta in approximately one-third of patients; however, this did not appear to affect short-term functional outcomes or quadriceps strength.
Footnotes
Final revision submitted July 18, 2025; accepted August 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the National Natural Science Foundation of China (No. 82202777, No. 82472527), Beijing Municipal Health Commission (No. BJRITO-RDP-2024), and Beijing Jishuitan Research Funding (No. XKXX202211). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital, Capital Medical University (approval No. 2023065).
Data Accessibility Statement
The data sets used or analyzed during the current study are available from the corresponding author on reasonable request.