
Abstract
Background:
Recurrent patellar dislocation (RPD) and habitual patellar dislocation (HPD) in flexion are frequently encountered in children and adolescents.
Purpose:
To compare the radiological features of RPD and HPD in children and adolescents.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Imaging data were collected from patients aged 9 to 15 years who received surgical treatment for HPD or RPD at a single institution between June 2015 and September 2020. The prevalence of trochlear dysplasia, tibial tubercle lateralization, and lower limb rotational deformity was assessed through hip/knee/ankle computed tomography (CT) using the following quantitative indicators: trochlear depth index, lateral trochlear inclination, sulcus angle, tibial tubercle–trochlear groove (TT-TG) distance, ratio of TT-TG distance to femoral width, TT-TG angle, femoral anteversion angle, and tibial external rotation angle. The morphology of trochlea and patella were graded on knee CT using the Dejour and Wiberg classification. The Insall-Salvati index and Caton-Deschamps index were used to evaluate the height of the patella on lateral view radiographs. To evaluate lower limbs malalignment, the mechanical lateral distal femoral angle and medial proximal tibial angle were measured on weightbearing full-length radiographs. The collected data were analyzed and compared between the HPD and RPD groups.
Results:
Enrolled were 15 patients (21 knees) diagnosed with HPD and 18 patients (22 knees) diagnosed with RPD. The age of first dislocation was significantly younger in the HPD group (7.6 ± 3.4 vs 11.2 ± 1.4 years; P = 0.003). Knees in the HPD group had a significantly higher proportion of Dejour type C dysplasia (57.1% vs 4.5%; P < .005) and Wiberg type 3 patella (66.7% vs 9.1%; P < .001). There were statistically significant differences between the groups in the trochlear depth index (HPD vs RPD: 1.1 ± 1.7 vs 2.2 ± 1.5 mm; P = .039), sulcus angle (170.3° ± 13.7° vs 157.3° ± 16.0°; P = .007), Insall-Salvati index (1.1 ± 0.2 vs 1.3 ± 0.2; P = .034), and tibial external rotation angle (31.3° ± 7.8° vs 38.4° ± 8.5°; P = .009).
Conclusion:
Patients in the HPD group presented with poorer trochlear and patellar development, lower patellar height, and less tibial external rotation compared with patients in the RPG group.
Keywords
Patellofemoral instability (PFI) is not uncommon in children and adolescents, with recurrent patellar dislocation (RPD) and habitual patellar dislocation (HPD) in flexion being the most frequently encountered in pediatric sport medicine departments, mostly requiring surgical treatments. 36
HPD in flexion is characterized by consistent dislocation of the patella each time the knee is flexed, and it usually appears in children between 5 and 8 years of age. While RPD is the most common type of patellofemoral instability, it usually occurs during preadolescence or adolescence, often triggered by a sprain or twisting. 7 In past studies, a variety of radiological features including hypoplastic trochlea/patella, patella alta/baja, excessive femoral anteversion, excessive tibial external rotation, genu valgum, increased Q angle, and increased tibial tubercle–trochlear groove (TT-TG) distance have been a reported characteristic in pediatric HPD and RPD patients. 10,16,28,34,35,45,47,52 Most of these studies, however, focused on only some of these parameters, and the comprehensive radiological appearance of the 2 groups is still missing.
Because of its relative rarity, HPD is usually discussed together with RPD in early research. The differences between the 2 groups were intentionally or unintentionally neglected despite their distinctive clinical features, not to mention the differences in their surgical management. 3 This formed the basis of the current study, the aim of which was to summarize the overall radiological characteristics of HPD and RPD and to determine whether there were differences between the 2 groups. For the purposes of this study, HPD in extension was not evaluated.
Methods
Medical records and imaging data were collected by reviewing all the patients who received surgical treatments for HPD and RPD in the Pediatric Orthopedics Department in Beijing Jishuitan Hospital between June 2015 and September 2020. Because of the different age predilection of the 2 diseases 7,36 and because of the limited accuracy of radiography and computed tomography (CT) in immature bone, the patients considered for this study were confined in age to between 9 and 15 years. The criteria for sample collection were as follows: (1) clinically confirmed HPD and RPD patients aged from 9 to 15 years old; (2) no previous knee surgery; (3) no previous history of other congenital or developmental musculoskeletal disorders; (4) a complete set of well-kept imaging data including lateral and axial radiographs, weightbearing full-length (WBFL) radiographs, and multislice hip/knee/ankle CT. Ethical approval was obtained from our institution for the study protocol, and written informed consent was provided by the included patients.
PFI patients who were treated surgically in our center routinely underwent lateral and axial view knee radiographs, knee magnetic resonance imaging (MRI), and WBFL radiographs. Multiple-slice CT of the hip, knee, and ankle (low dose in children) was also performed to assess the severity of torsion deformity of the lower limbs. Because of the lengthy waiting time, most patients had their knee MRI performed at local hospitals. The lack of original digital data and the varying image quality and film resolution made accurate quantitative measurement on MRI difficult to achieve; thus, MRI data were omitted in the present study.
Quantitative Measurements
All radiological data were collected from our picture archiving and communication system database (Carestream Health) and measured using the same system. All the distances and angles were measured by a fellowship-trained orthopaedic surgeon (L.H.) and a radiologist (Z.-H.Q.) in our center using the same workstation.
The morphology of the trochlea and patella were graded on knee CT using the Dejour and Le Coultre, 9 Nacey et al, 32 and Tavernier and Dejour 46 and Wiberg classifications. CT measurements and classification of the femoral trochlea as well as the calibration of the posterior femoral condylar line (PC line) were made utilizing the first craniocaudal slice of the femoral trochlea with complete cartilage coverage. The Dejour radiographic classification was not used in our study because the requirement of standard lateral view was not met in many cases.
The prevalence of trochlear dysplasia, tibial tubercle lateralization, and lower limb rotational deformity was assessed through hip/knee/ankle multislice CT. The following quantitative indicators were measured: trochlear depth index (TDI), lateral trochlear inclination (LTI) and sulcus angle (SA), TT-TG distance (TT-TG), TT-TG/femoral width (TT-TG/FW) ratio, TT-TG angle (TT-TGa), 31,44 femoral anteversion angle (FAA), and tibial external rotation angle (TERA). To diminish the effect of knee rotation, patients were positioned supine with legs fully extended and feet taped together at the level of the metatarsophalangeal joint during CT examination.
TDI was measured using the method described by Pfirrmann et al 38 in 2000. TDI was obtained as (a + b)/2, where a and b are the heights of the medial and lateral trochlear facets, respectively, as measured from the highest point of the medial and lateral trochlea vertically to a line parallel to the PC line and intersecting the lowest point of the trochlea. 45 SA and LTI were measured as the degree of the angle formed by the medial and lateral trochlear facet and the angle between the lateral trochlear facet and the PC line, respectively (Figure 1).

Measurements of trochlear depth index (TDI) and femoral width. The medial and lateral condylar trochlear offset are represented by a and b, respectively, and TDI was calculated as (a + b)/2. Femoral width was measured as the distance of 2 lines perpendicular to the posterior femoral condylar (PC) line and tangent to the medial and lateral margin of the distal femur. In severe cases, a line perpendicular to the PC line and tangent to the medial wall of the posterior notch was drawn, and the medial measurement point was where this line intersected the articular cartilage. LTI, lateral trochlear inclination; SA, sulcus angle.
TT-TG was measured on CT as described previously by Dejour et al. 10 To diminish the interference of knee size, the mediolateral width of the distal femur (Figure 1) was measured and TT-TG/FW ratio was obtained. 2,37 An angular parameter TT-TGa was also developed by modifying the tibial tubercle rotation angle introduced by Muneta et al 31 and Steensen et al 44 (Figure 2). FAA was measured using the angle formed by the long axis of the femoral neck and PC line, and TERA was measured using the angle formed by the PC line and the malleolar line (Figure 3).
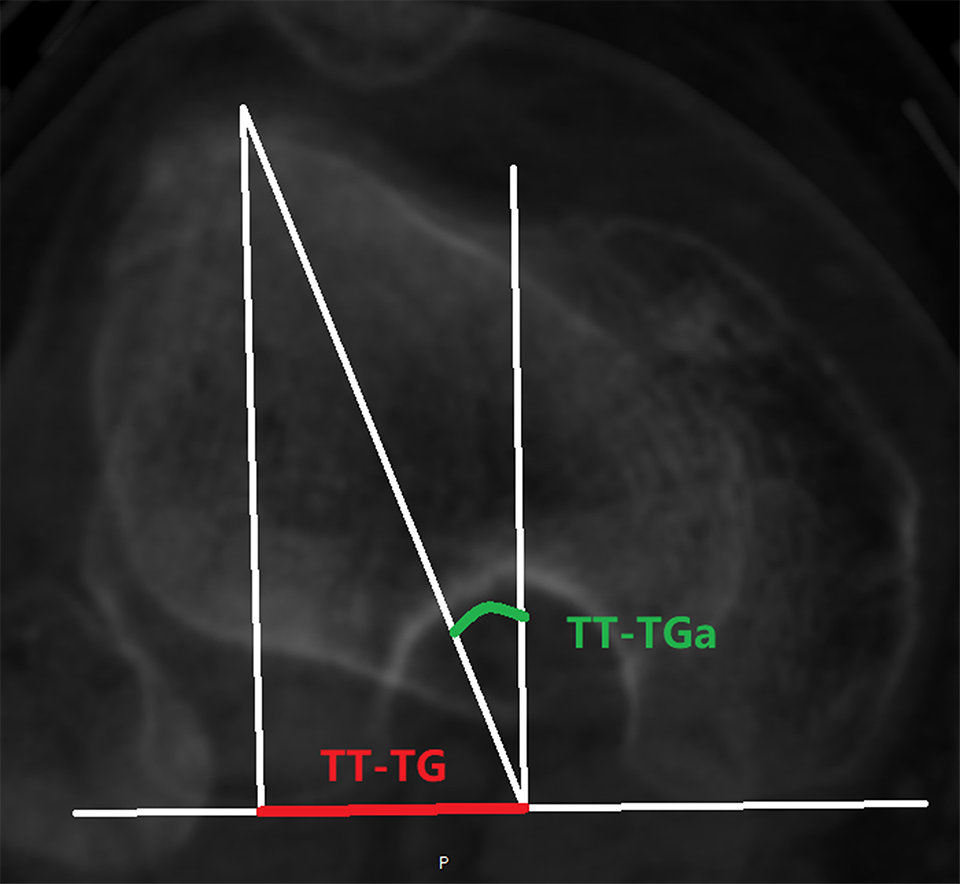
Tibial tubercle–trochlear groove angle (TT-TGa) was measured as the angle formed between a line from the deepest point of the trochlear groove perpendicular to the posterior femoral condylar line and another from the intersection point to the center of tibial tubercle. TT-TG, tibial tubercle–trochlear groove distance.

Tibial external rotation angle (TERA) was measured using the angle formed by the posterior femoral condylar line and malleolar line.
The Insall-Salvati index and Caton-Deschamps index 47 were utilized to evaluate the height of the patella on the lateral view of the knee joint at 30° of flexion. Mechanical lateral distal femoral angle (mLDFA) and medial proximal tibial angle (MPTA) were measured on WBFL radiography to evaluate lower limbs malalignment.
Data Analysis
The interrater reliability of the quantitative measurements was assessed with the intraclass correlation coefficient (ICC), in which ICC < 0.4 was considered poor agreement, 0.4 < ICC < 0.75 was fair to good agreement, and ICC > 0.75 was excellent agreement. Continuous data were reported as means and standard deviations, and categorical data were reported as absolute values and percentages. Qualitative assessment of the Dejour classification on CT was performed using the kappa statistic with linear weighting. For reference, the data from the quantitative measurements were compared with ranges of those indices as reported in previous literature. Statistical comparisons between the 2 groups were conducted using the independent-samples t test, paired-samples t test, or Fisher exact test, as applicable. Estimated effect size was analyzed using the Cohen d, in which a d value of 0.2 represents a small effect size, a value of 0.5 represents a medium effect size and a value of 0.8 represents a large effect size. In addition, for patients with bilateral dislocations, we compared the quantitative parameters between the left and right knee using the paired-samples tIBM test. All data analysis was performed using the Statistical Package for the Social Sciences Version 27.0 (IBM), and power analysis was conducted with G*Power 3.1 (HHU). All tests were considered statistically significant at P < .05.
Results
Demographic Characteristics
Between June 2015 and September 2020, 116 patients with 137 knees diagnosed with HPD and 158 patients with 170 knees diagnosed with RPD were surgically treated in our department. A total of 33 patients (43 knees) met the grouping criteria and served as the study group. There were 26 girls (78.8%) and 7 boys (21.2%), with their mean age being 11.5 years (range, 9.4-14.7 years).
Within the study cohort, 15 patients (21 knees) were diagnosed with HPD and 18 patients (22 knees) were diagnosed with RPD. There were 6 knees (28.6%) in the HPD group and 21 knees (95.5%) in the RPD group with a history of knee injury (P < .001). The mean age of onset was significantly younger in the HPD group (P = .003). No significant differences were observed in the other patient characteristics (Table 1).
Characteristics of the Study Groups a

a Data are reported as mean ± SD or n (%). Boldface P values indicate statistically significant differences between groups (P < .05). HPD, habitual patellar dislocation; NA, not applicable; RPD, recurrent patellar dislocation.
Trochlear Dysplasia
The Dejour classification on CT of each group is listed in Table 2. The proportion of high-grade dysplasia (Dejour types B-D) was higher in the HPD group (90.5% vs 63.6%; P = .069). As for specific trochlear morphology, knees in the HPD group presented with a lower proportion of trochlear bump (Dejour types B and D, 33.3% vs 59.1%; P = .129) but a significantly higher proportion of type C trochlear dysplasia (57.1% vs 4.5%; P < .005) compared with RPD group. Exact interrater agreement was found in 79% (34/43) of knees between the 2 readers when classifying specific Dejour types [weighted κ = 0.77; 95% CI, 0.62-0.91].
Dejour Classification on Computed Tomography by Study Group a
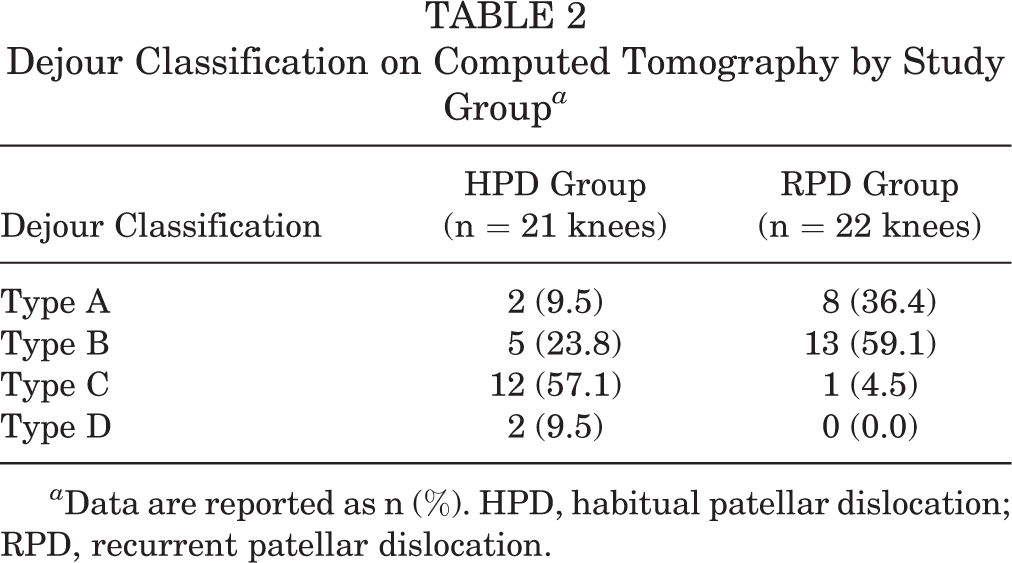
a Data are reported as n (%). HPD, habitual patellar dislocation; RPD, recurrent patellar dislocation.
Patellar Dysplasia
The Wiberg classifications of both groups are listed in Table 3. The morphology of the patella appeared more dysplastic in the HPD group, with up to 66.7% of the patella being the Wiberg type 3 (9.1% in RPD group; P < .001).
Wiberg Classification by Study Group a
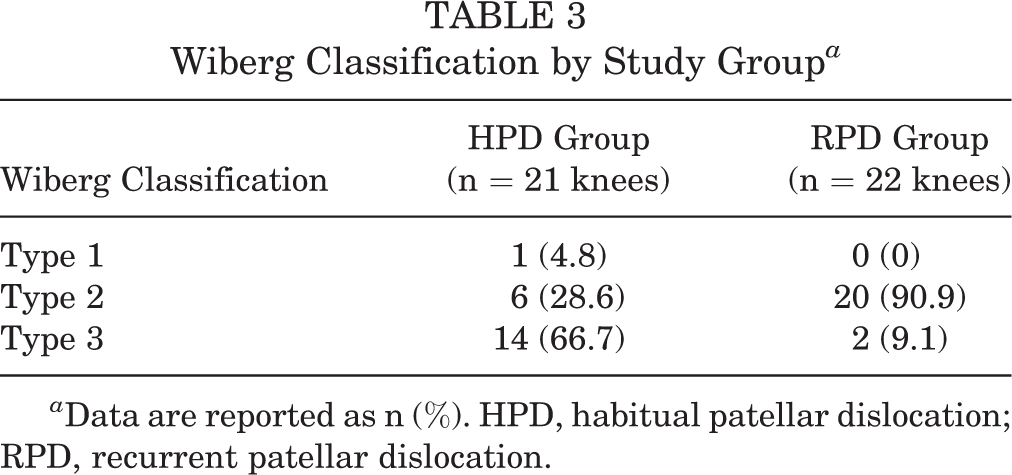
a Data are reported as n (%). HPD, habitual patellar dislocation; RPD, recurrent patellar dislocation.
Quantitative Measurements
Excellent interrater reliabilities were found regarding all quantitative measurements. The comparisons of quantitative parameters between the study groups, combined with the reference ranges and interrater reliabilities, are listed in Table 4.
Quantitative Measurements Between the Study Groups, Reference Ranges, and Interrater Reliabilitiesa

a Values are presented as mean ± SD. Boldface P values indicate statistically significant difference between the study groups (P < .05). FAA, femoral anteversion angle; HPD, habitual patellar dislocation; ICC, intraclass correlation coefficient; LTI, lateral trochlear inclination; mLDFA, mechanical lateral distal femoral angle; MPTA, medial proximal tibial angle; NA, not applicable; RPD, recurrent patellar dislocation; SA, sulcus angle; TDI, trochlear depth index; TERA, tibial external rotation angle; TT-TG, tibial tubercle–trochlear groove distance; TT-TGa, tibial tubercle–trochlear groove angle; TT-TG/FW, tibial tubercle–trochlear groove distance/femoral width.
b n = 10 knees in the HPD group.
Tibial Tubercle Lateralization
No significant differences were observed regarding the parameters of tibial tubercle lateralization between the 2 groups.
Patellar Height
Attempts to obtain the Insall-Salvati index and Caton-Deschamps index failed in 11 HPD (52.4% ) knees because of the already dislocated patella in the lateral view of the 30°-flexed knee, which were excluded from analysis (Figure 4). For the remaining cases, the mean Insall-Salvati index in HPD and RPD group was significantly different (1.1 ± 0.2 vs 1.3 ± 0.2, respectively; P = .034).
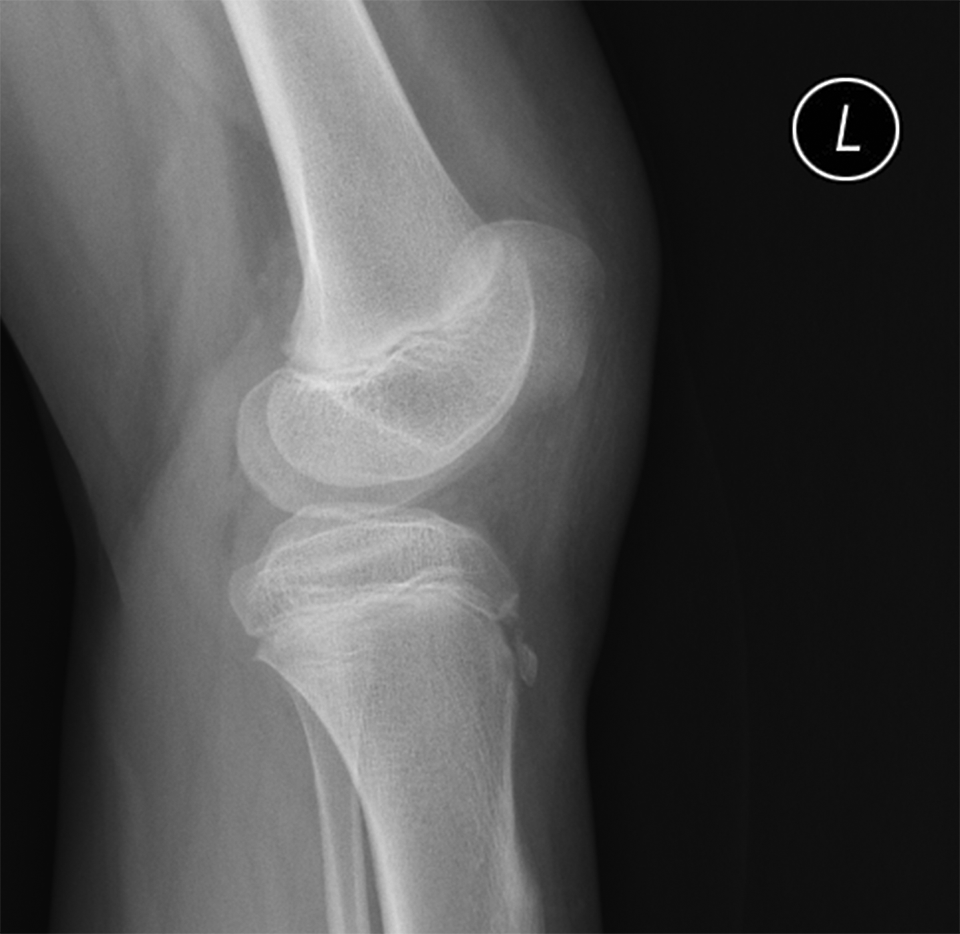
The already dislocated patella in a 30°-flexed knee.
Lower Limb Rotational Deformity
Although the mean FAA was higher in the HPD group than the RPD group, this difference was not statistically significant (33.0° ± 12.7° vs 31.3° ± 11.1°, respectively; P = .649). The TERA was significantly lower in the HPD group compared with the RPD group (31.3° ± 7.8° vs 38.4° ± 8.5°, respectively; P = .009).
Lower Limb Malalignment
No significant difference was observed regarding mLDFA or MPTA between the 2 groups.
Comparison of Patients With Bilateral Knees Affected
Overall, 10 out of the 11 patients with bilateral knees were included in this analysis (6 HPD and 4 RPD patients). One patient in the HPD group was excluded because of previous surgery to the contralateral knee. No significant differences were found between the affected and contralateral sides for either study group (Table 5).
Comparison of the Bilaterally Affected Knees in the Study Groups a
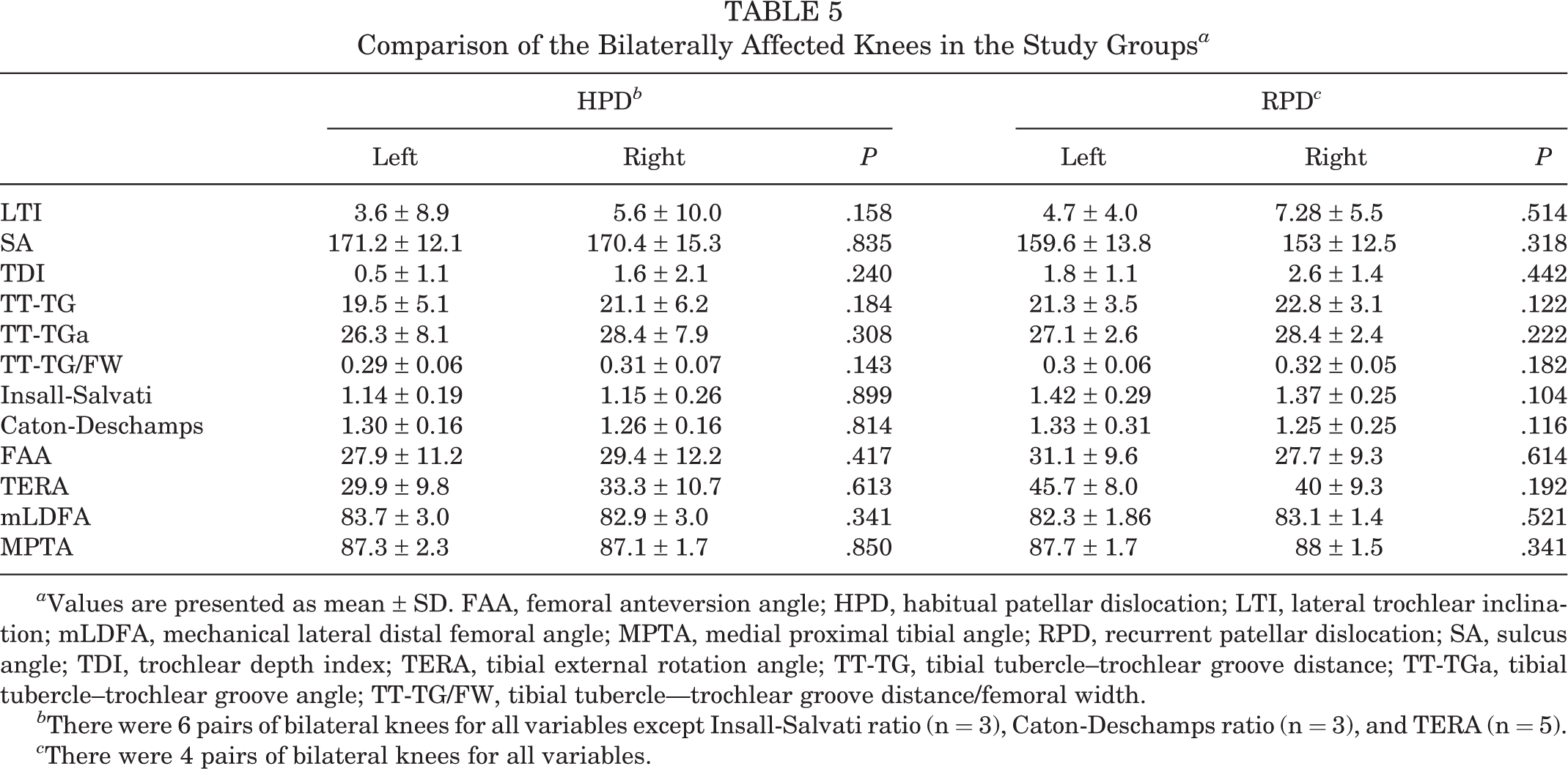
a Values are presented as mean ± SD. FAA, femoral anteversion angle; HPD, habitual patellar dislocation; LTI, lateral trochlear inclination; mLDFA, mechanical lateral distal femoral angle; MPTA, medial proximal tibial angle; RPD, recurrent patellar dislocation; SA, sulcus angle; TDI, trochlear depth index; TERA, tibial external rotation angle; TT-TG, tibial tubercle–trochlear groove distance; TT-TGa, tibial tubercle–trochlear groove angle; TT-TG/FW, tibial tubercle—trochlear groove distance/femoral width.
b There were 6 pairs of bilateral knees for all variables except Insall-Salvati ratio (n = 3), Caton-Deschamps ratio (n = 3), and TERA (n = 5).
c There were 4 pairs of bilateral knees for all variables.
Discussion
According to the results, the HPD group presented with significantly poorer trochlear development (TDI: 1.1 ± 1.7 vs 2.2 ± 1.5 mm [P = .039]; SA: 170.3° ± 13.7° vs 157.3° ± 16.0° [P = .007]) and patellar development (Wiberg type 3: 66.7% vs 9.1% [P < .001]), lower patellar height (Insall-Salvati index: 1.1 ± 0.2 vs 1.3 ± 0.2 [P = .034]), and less tibial external rotation (31.3° ± 7.8° vs 38.4° ± 8.5° [P = .009]) compared with the RPD group.
The qualitative assessment of trochlear dysplasia showed the proportion of high-grade dysplasia was higher in HPD group, although this difference was not statistically significant. Dejour classification on CT used in this study has been proven to be effective in distinguishing low-grade (type A) from high-grade (types B-D) dysplasia with high inter- and intraobserver agreement. 27,32 However, its validity in differentiating among different types of high-grade dysplasia has been controversial. 27,32,45 A study by Lippacher et al 28 found that qualitative interobserver agreement ranged from 28% to 68% when classifying specific Dejour types, whereas Nacey et al 32 reported substantial agreement (77%) in the same scenario, which was consistent with the result of the current study.
There are also different opinions regarding the validity of the 2-grade classification (separating type A from types B-D) in terms of predicting prognosis and instructing treatment. It is suggested that Dejour type B and D trochlear dysplastic morphologies are most amenable to a sulcus-deepening procedure secondary to the large supratrochlear bump, whereas a facet-elevating trochleoplasty may be of more value in correcting Dejour type C dysplasia. 32,49 The result of this study showed 59.1% knees of the RPD group presenting with a bump (Dejour type B and D), whereas 57.1% knees in HPD group presented with type C trochlear dysplasia, hinting that different surgical techniques may be considered when trochleoplasty is indicated in each group.
For more precise differentiation between the 2 groups, quantitative evaluation of trochlear dysplasia using SA, LTI, and TDI was performed. The data for these 3 parameters in this study were far from normal in both groups, but the value of SA and TDI were significantly worse in the HPD group (Table 4).
As reported in a previous study by Huri et al, 19 developing trochlear groove with inadequate patellar alignment becomes more flattened and predisposed toward patellar instability. In the current study, the mean age of onset of HPD was significantly younger than that of RPD. The long-term inadequate patellar alignment may have contributed to the poorer trochlear development in HPD knees. Correspondingly, the morphology of the patella was significantly worse in the HPD group. To determine the underlying congenital and developmental reasons for this difference, further anatomical study in younger age groups is required.
As for tibial tubercle lateralization, no significant difference was identified between the 2 groups. TT-TG of both groups were far beyond the normal range, 11 indicating surgical correction may be required. One of the key problems in studying patellofemoral instability is that patients of different ages have different knee sizes. As described previously by Hernigou et al, 17 there was a linear correlation between knee size and TT-TG. To diminish the possible effect of femoral condylar width, TT-TG/FW was also adopted in this study, and no significant differences were identified between the 2 groups. We also used the parameter TT-TGa to evaluate the degree of tibial tubercle lateralization in differently sized knees. 31 Although the angle seemingly avoided the effect of knee size, the reliability of this parameter is yet to be determined in further research because whether it varies with age is unknown. Because of the lack of MRI data, TT-TG index, a new knee size–adjusted parameter to determine the TT-TG distance described by Hingelbaum et al 18 was not used in the current study.
Patellar height has been investigated thoroughly in previous studies. It is believed that patella alta increases the risk of RPD, 5,20,44 and tibial tubercle distalization is an effective surgical technique for this condition. 29 In contrast, quadriceps fibrosis is a major risk factor for HPD, 6,16,21 and tibial tubercle proximalization is required to correct the shortening of extensor mechanism. 4,43 In this study, we adopted both the Insall-Salvati index and the Caton-Deschamps index to assess the height of patella. The measurement failed in 11 out of 21 (52.4%) HPD knees because of the patellofemoral dislocation already present in a 30°-flexed knee. The presence of patellar dislocation or patellar tilting hindered the accurate measurement of patellar height or, furthermore, the length of the extensor mechanism. For the obtained data, remarkable patella alta was observed in the RPD group. However, because of the limited sample size and the high failure rate, it remains premature to draw conclusions about the patellar height of the HPD group. A more precise index independent of these interventions is needed in further research.
In the aspect of rotational parameters of the lower extremity, the HPD group in the current study had greater femoral anteversion and significantly lower tibial external rotation. According to previous studies, increased femoral anteversion is associated with a flatter, more dysplastic trochlea, 22,26 which might explain the difference in trochlear development between the 2 groups. Meanwhile, the relation between the tibial external rotation and patellofemoral instability was scarcely studied. In an anatomical study by Wang et al, 50 the development of the trochlear groove could effectively compensate for the tibial malrotation. Another study by Prakash et al 39 suggested that increased tibial external rotation might be related to increased TT-TG distance. The correlation and causation between TERA and PFI are yet to be determined by further research.
Despite the rotational malformations, genu valgum was also observed in both groups, mainly occurring at the distal femur. The influence of genu valgum on the patellofemoral dysbalance has been reported in many publications, 13 –15,35,40,51 and this study appeared to justify this view. No significant difference was observed between the 2 groups.
The proportion of bilateral instability in HPD was higher than the RPD group (53.3% vs 16.7%), although no significant difference was observed. For the 10 patients with bilateral knees evaluated in this study, similar results were seen between the 2 knees on all quantitative indices except TDI and TERA. Significant difference in paired-samples t test was only found in TT-TG and TT-TG/FW, indicating that the pathological alternation of lower limbs was largely symmetrical except tibial tubercle lateralization. Compared with the RPD group, the indices of bilateral HPD knees correlated better with each other. However, because the sample size was small, it is way too early to conclude that the knees of HPD patients are more symmetrical than those of the RPD group. Further research with larger sample sizes is needed to uncover the difference in bilateral instability between the 2 groups, which may even provide some clue to the pathogenesis of the 2 diseases.
Limitations
Owing to the limited sample size, correlation between the parameters in each group was not analyzed. The lack of MRI data was also a limitation of this study. Although the reliability and reproducibility of CT scan was validated in previous studies, 1,28,42,48 the radiation exposure and the interference of cartilage is inevitable. The lack of comparison of radiological features between the surgical patients and other PFI patients who were not treated surgically is another limitation of the current study, which is significant in illustrating the factors affecting surgical decision making. Because hip/knee/ankle CT in our center was only performed in patients scheduled for surgery to determine the necessity of derotational osteotomy, the radiological data of the PFI patients who were treated nonoperatively were not comprehensive enough to match the surgical group.
Another major defect of the current study is the missing of soft tissue factors such as arthrochalasis, 33 MPFL laxity, 24,53 and quadriceps contracture, 6,16,25,43 which are important in surgical planning. Limiting the age for inclusion for habitual dislocation patients also introduced bias in this study, presenting an incomplete picture of the disease. To uncover a more comprehensive profile of pediatric PFI, a larger sample size with more detailed clinical information and MRI data is required in further studies.
It should also be noted that the proportion of HPD patients in this study was significantly higher than normally reported in previous studies. Because of the department division in our center, PFI patients >14 years of age were usually treated by our colleagues in the sports medicine department. The age limit of patient admission and the different age predilection of the 2 diseases might be the main reasons for this high proportion of HPD.
Conclusion
HPD and RPD in this study represented 2 distinct groups based on their radiographic and biomechanical factors, including trochlear dysplasia, patellar height, and tibial external rotation angle, which may have an influence on the choice of operative protocol during surgical planning.
Footnotes
Final revision submitted January 20, 2023; accepted March 9, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received by the Beijing Health Technologies Promotion Program (grant BHTPP2022016) Beijing Jishuitan Hospital Nova Program (grant XKXX202202) and Beijing JST Research Funding (code: LH-202208). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital (No. 202201-26).