
Abstract
Background:
Hip and groin problems are just as common in ice hockey as they are in soccer. The 5-second squeeze test (5SST) is a valid indicator of hip- and groin-related sporting function (self-reported function) in soccer and is suggested to be interpreted according to a “traffic light” approach in guiding the early identification and management of affected players. It is currently unknown how the 5SST relates to self-reported function and muscle strength in ice hockey players.
Purpose:
To investigate correlations between the 5SST result, self-reported function, and hip muscle strength in ice hockey players. A further aim was to investigate the discriminative ability of the “traffic light” approach (numeric rating scale [NRS] score: 0-2 = green, 3-5 = yellow, 6-10 = red) regarding levels of self-reported function and strength.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Professional and semiprofessional male ice hockey players (N = 333) performed the 5SST and completed the Sport subscale of the Copenhagen Hip and Groin Outcome Score (HAGOS). Bilateral adduction and abduction strength was measured using handheld dynamometry. Associations were estimated using Spearman rank-order correlations, and groups were compared using the Kruskal-Wallis test or analysis of variance. Standardized effect sizes (ESs) for differences in strength (Hedges g) and self-reported function (r) were provided.
Results:
The 5SST result was significantly correlated with self-reported function (rho, –0.319; P < .01) and hip muscle strength (rho, –0.157 to –0.305; P < .01). The HAGOS Sport scores differed significantly between all 3 traffic light groups (ES, 0.23-0.33; P ≤ .005). Players with an NRS score >2 (yellow or red light) had lower adduction (ES ≥ 0.75; P < .001) and abduction strength (yellow: ES, 0.30; P = .031) (red: ES, 0.51; P = .058) than players with a green light.
Conclusion:
The 5SST result was significantly correlated with self-reported function as well as hip muscle strength and was able to discriminate between the traffic light levels in ice hockey players. Players with a yellow or red light had reduced adduction and abduction strength compared with players with a green light (NRS score ≤2). Routine 5SSTs may allow the early identification of affected ice hockey players and indicate yellow and red light situations, in which players may benefit from load management and appropriate hip muscle strengthening.
Hip and groin pain is common in ice hockey, leading to both time loss and non–time loss injuries. 2,20 The impact of hip and groin pain on the physical function of a player can be assessed by valid and reliable self-reported outcome measures such as the Copenhagen Hip and Groin Outcome Score (HAGOS). 19 However, in a fast-paced environment such as competitive ice hockey, medical professionals additionally require objective and easily performed field tests as rapid measures of objective hip function to guide the management of affected players.
One such measure is the 5-second squeeze test (5SST), which has recently been introduced as a valid indicator of hip and groin function in soccer players. 17 As opposed to the HAGOS, which measures hip and groin function over the previous week and requires time to administer and evaluate, the 5SST can provide valuable information about players’ hip and groin function as well as pain in just 5 seconds. The 5SST categorizes players’ experienced pain according to intensity (numeric rating scale [NRS] score groupings of 0-2, 3-5, or 6-10) and can be used to assist clinicians in identifying and managing affected players by interpreting results according to a “traffic light” approach (green = safe, yellow = acceptable, red = high risk). 17
Therefore, the 5SST may be a time-efficient and valuable tool with the potential ability to assist appropriate on-site decision making regarding whether athletes should be removed from aggravating activity, if they require medical attention, or if they should be allowed full sport participation. However, to date, the 5SST has only been tested in soccer players and has not been investigated in other sports such as ice hockey.
In addition to subjective experience, objective measures such as hip muscle strength have demonstrated relevance for athletes with groin pain. 18 According to a 2016 systematic review, decreased hip adductor strength during a 45° hip flexion squeeze has been reported to be strongly associated with groin pain in athletes, while there is limited evidence of such an association with the hip in the neutral position. 11 Interestingly, the only study included in the review that measured adductor strength with a neutral hip found larger impairments compared with the measurement in 45°. 13 Evidence regarding adductor strength as a risk factor for injuries in ice hockey is conflicting. Emery and Meeuwisse 3 found isometric adductor torque to not be predictive of groin injuries, while Tyler et al 22 identified hip adductor weakness and abduction-to-adduction ratios of less than 80% as risk factors for adductor muscle strains.
Risk factors for hip and groin injuries are usually assessed before the competitive season. 3,22 However, hip and groin problems appear to develop gradually, 6 and associated factors such as adduction strength change in response to increasing loads 25 that can be expected during a competitive ice hockey season. To account for within-season variability of strength and the gradual development of hip and groin problems, regular in-season monitoring of players may facilitate the early detection of at-risk individuals and therefore aid in appropriate management. A recent study evaluating youth soccer players proposed using such in-season monitoring of hip muscle strength and self-reported hip function (HAGOS) as an early detection and management strategy. 26 The 5SST thus bears potential for a rapid and practical tool that could be used for regular in-season monitoring of hip and groin function. However, it is currently unknown to what extent the subjective 5SST outcome is related to suggested risk factors such as hip adduction and abduction strength or to subjective hip and groin function among ice hockey players.
Therefore, the purpose of this study was to evaluate 5SST findings, alongside measurements of self-reported hip and groin function, adduction strength, and abduction strength, in male ice hockey players. The aim was to investigate correlations between 5SST results, self-reported sporting function (HAGOS Sport scores), and hip adduction and abduction muscle strength. Furthermore, the study aimed to investigate whether further categorization of 5SST results according to levels of groin pain intensity (the traffic light approach) was able to differentiate between levels of subjective sporting function and strength among ice hockey players. We hypothesized that 5SST results would be correlated with self-reported hip and groin function and hip muscle strength and that the traffic light approach discriminates between levels of subjective sporting function and hip muscle strength.
Methods
Design
In this cross-sectional study, subjective and objective hip and groin function was measured in a group of professional and semiprofessional ice hockey players either by the end of the season (spring) or the beginning of the season (autumn). The 5SST was administered as a measure of subjective pain experienced during a 5-second maximal squeeze. Self-reported hip- and groin-related sporting function was assessed by the HAGOS Sport subscale. Objective hip muscle strength was measured for bilateral adduction (“adduction strength”) and bilateral abduction (“abduction strength”). The study was approved by the ethics committee at Lund University, and all participants provided written informed consent.
Setting
Data collection was performed during either the end of the 2016/2017 season (February-March 2017) or the beginning of the 2017/2018 season (August-October 2017). Responsible sport managers for ice hockey clubs in the Stockholm area and Scania, Sweden, were first contacted by email with written information regarding the study. Subsequently, contact was established to provide verbal information regarding practicalities and to allow for questions regarding the study. Measurements were performed before regular training sessions and without interfering with training routines.
Participants
A total of 15 Swedish professional (Svenska hockeyligan, HockeyAllsvenskan) and semiprofessional/amateur (Division 1-3) ice hockey teams, located in the Stockholm area (n = 12) and in Scania (n = 3), were invited to participate in the study, and 13 teams agreed to participate. All players attending training sessions on the day of the measurements were invited to participate in the study. Players were included in the study if they were at least 18 years of age and did not have any current injury, unrelated to the hip and groin, which prevented participation in practice or match play.
Measurements
Data collection included a web-based survey (including questions regarding relevant demographic information and self-reported hip and groin function [HAGOS]), which participants completed before the 5SST and strength measures. Online survey responses, 5SST results, and adduction strength measurements were obtained for all study teams (n = 13). The bilateral abduction measure was added to the procedure only for the teams in the Stockholm area (n = 10).
5-Second Squeeze Test
The 5SST was performed with the assessor’s arm placed between the players’ ankles. Players were then asked to perform 5-second maximal isometric adduction. 17 A submaximal familiarization trial was performed before the actual test. Groin pain during the test was verbally rated on an 11-point NRS. Players were verbally instructed to rate their groin pain on a scale from 0 to 10, with 0 representing no groin pain and 10 representing maximal groin pain. According to their score on the NRS, players were then categorized into pain intensity groups, with a score of 0-2 being categorized as low (green light), 3-5 as medium (yellow light), and 6-10 as high (red light) pain intensity. 17
Strength Measures
Two trained assessors performed all strength measures using a handheld dynamometer (MicroFET2; Hoggan Health Industries), which was calibrated before testing. The specific method for adduction and abduction testing was developed by Kristian Thorborg in Copenhagen. Adduction strength was measured during the 5SST according to a standardized and reliable (intratester) procedure. 12 Abduction strength was measured with a fixation belt around the players’ lower legs in line with the point of application used for the 5SST and by placing the handheld dynamometer in between the leg and belt (see Figure 2). During both tests, players were asked to perform a 5-second maximal isometric contraction after a submaximal familiarization trial. Adduction and abduction torque, expressed in newton meters (force × lever arm [distance between the anterior superior iliac spine and point of force application]), was then normalized to body weight (in kilograms) to control for isolated effects of limb length and body weight on muscle strength.
Before strength testing in this setup, reliability was investigated in physically active healthy patients between 20 and 34 years of age, including 19 participants (10 female) for intratester reliability and 32 participants (17 female) for intertester reliability. Intraclass correlation coefficients, 2-way random model (2.1), for intratester reliability were 0.97 for adduction strength, 0.92 for hip abduction strength, and 0.80 for adduction-to-abduction ratio. Intraclass correlation coefficients, 2-way random model (2.1), for intertester reliability were 0.95 for adduction strength, 0.95 for hip abduction strength, and 0.75 for adduction-to-abduction ratio.
Self-Reports
All players replied to an online survey containing questions regarding relevant background information, which included playing level, playing position, and previous hip and groin problems leading to time loss and non–time loss injuries. Sports-related hip and groin function was assessed by the Sport subscale of the HAGOS. The HAGOS is a self-reported instrument consisting of 37 items relating to 6 dimensions (subscales): symptoms, pain, function in daily living, function in sport and recreation, participation in physical activities, and hip- and/or groin-related quality of life. 19 Raw sum scores for the items relating to the HAGOS Sport subscale were computed and then transformed to a 0-to-100 scale, with 0 representing extreme hip and/or groin problems and 100 representing no hip and/or groin problems.
Statistical Analysis
Associations between 5SST pain intensity results on one hand and HAGOS scores and strength measurements on the other were estimated by Spearman rank-order correlation. The significance level was set to P ≤ .05. The strength of correlations was categorized as large (≥0.5), moderate (≥0.3), or small (≥0.1). 1 Comparisons between the 3 pain intensity groups regarding the HAGOS Sport score were analyzed using the Kruskal-Wallis test, with pairwise post hoc comparisons. No apparent violation of normal distribution for strength data was detected by visual inspection of histograms. Hence, group comparisons regarding adduction and abduction strength measurements were analyzed using univariate analysis of variance, with pairwise post hoc comparisons (least significant difference). Standardized effect sizes (ESs) for strength measurements were computed as Hedges g: (M2 – M1) / SDpooled/weighted. Unlike Cohen d, Hedges g takes unequal variances and unequal group sizes into account by weighting the pooled SD and hence provides a more accurate estimation of ESs in this case. ESs of 0.1 were considered small, 0.3 medium, and 0.5 large. 1 For the HAGOS score, the standardized ES was computed from the pairwise Mann-Whitney U test as r = Z/√n. Data analysis was performed using SPSS Statistics 23 (IBM).
Results
Within the 13 study teams, all players who attended training sessions on the day of measurements agreed to participate, aside from 3 players who declined participation for unspecified reasons. Four players were excluded (medial collateral ligament sprains: n = 3; age <18 years: n = 1). A total of 333 participating players (152 players during end of season 2016/2017; 181 players during beginning of season 2017/2018) were included in the analyses. Demographic information is provided in Table 1.
Player Demographics (N = 333) a

a Data are reported as n (%) unless otherwise indicated. IQR, interquartile range.
Correlations Between 5SST, Strength, and Self-Reported Sporting Function
Significant negative correlations were found between the 5SST result and all strength measurements as well as the HAGOS Sport score (P < .01), indicating that pain intensity during the squeeze was associated with lower strength values and worse self-reported function. Correlations between the 5SST result and adduction strength as well as sporting function were of moderate strength. Correlations between the 5SST result and abduction strength and adduction-to-abduction ratio were small (Table 2).
Correlations (Spearman Rho) Between 5SST, Strength, and Self-Reported Sporting Function a
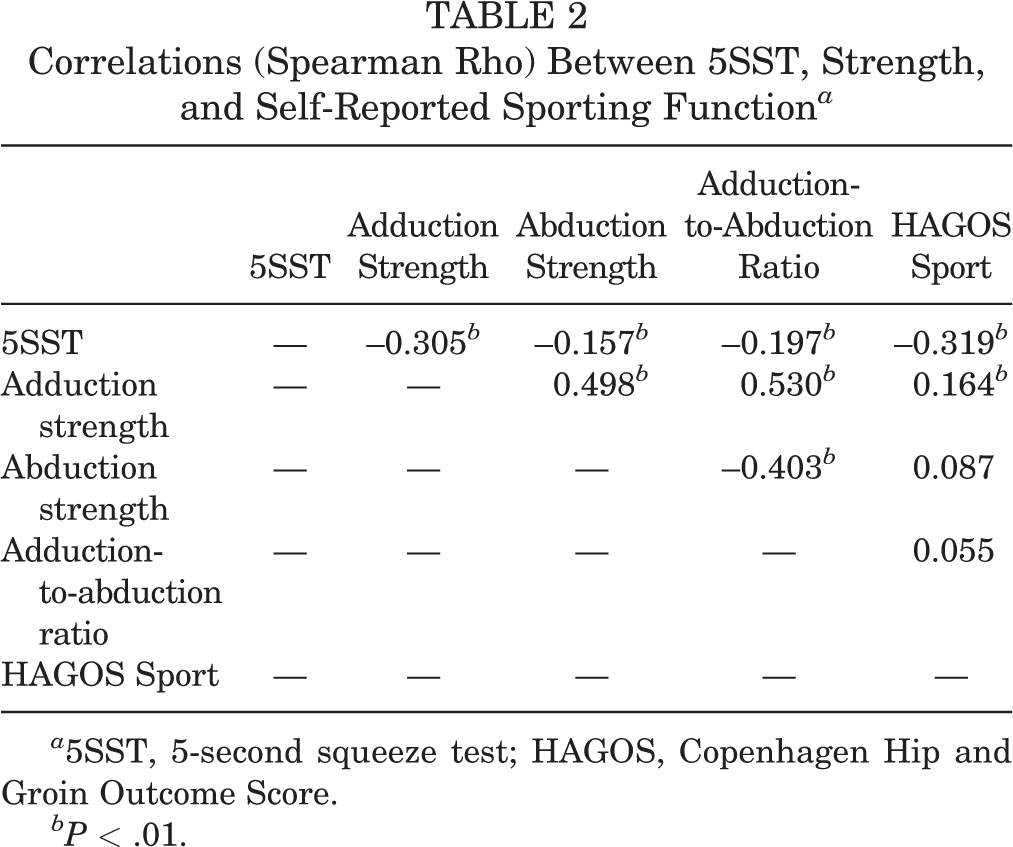
a 5SST, 5-second squeeze test; HAGOS, Copenhagen Hip and Groin Outcome Score.
bP < .01.
Differences in Sporting Function and Strength Between Players With Red, Yellow, and Green Light
Players with red, yellow, and green light pain intensity levels differed significantly (P < .01) from each other regarding self-reported sporting function, with worse HAGOS Sport scores in groups with higher pain intensity. Absolute values and differences between 5SST groups regarding sporting function and strength are illustrated and described in Figures 1 and 2 and Table 3. Players with low pain scores during the 5SST were significantly stronger in adduction (P < .001; Hedges g ≥ 0.75) than players who experienced medium or high levels of groin pain. Players with low levels of pain during the 5SST were also significantly stronger in abduction and had larger adduction-to-abduction ratios than players with medium pain levels. Higher abduction strength values were observed for players with low pain intensity compared with players with high pain intensity, but the difference was not statistically significant (P = .058), despite a large ES (Hedges g = 0.51). No significant differences in any strength measurements were found between players with medium and high pain intensity during the 5SST.
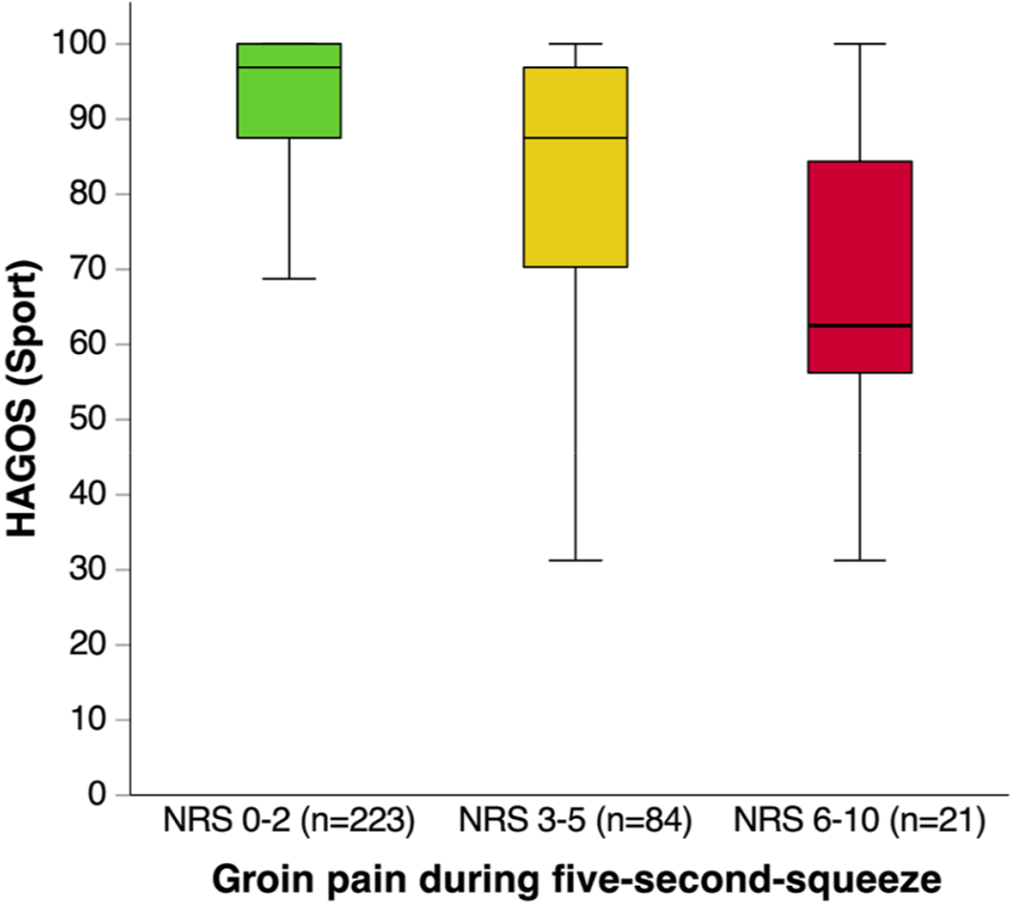
Copenhagen Hip and Groin Outcome Score (HAGOS) Sport scores (median [interquartile range]; range) according to the traffic light approach. NRS, numeric rating scale.

Strength profiles (mean [95% CI]) of players with green, yellow, and red light pain intensity levels and testing position. (A) Adduction strength, (B) abduction strength, (C) testing position for adduction strength, and (D) testing position for abduction strength.
Differences in Strength and Sporting Function in 5SST Groups a

a 5SST, 5-second squeeze test; HAGOS, Copenhagen Hip and Groin Outcome Score; NRS, numeric rating scale.
br = Z/√n.
Discussion
This is the first study to investigate the 5SST in relation to self-reported sporting function in ice hockey players as well as the incorporated and quick screening measures for hip adduction and abduction strength. Principal findings of the study demonstrated that higher pain scores during the 5SST were associated with worse self-reported hip- and groin-related sporting function and decreased adduction and abduction strength in ice hockey players. By applying the traffic light approach, the 5SST can differentiate between levels of self-reported hip-related sporting function (green [NRS score 0-2] > yellow [NRS score 3-5] > red [NRS score 6-10]) as well as indicate decreased hip muscle strength, as players with a green light (NRS score ≤2) were stronger than players with a yellow or red light (NRS score >2).
We found a significant negative correlation between the 5SST result and HAGOS Sport score. Players with more pain during the 5SST presented with worse HAGOS scores. The Sport subscale of the HAGOS measures the severity of hip-related sporting function 19 and has previously been used as a comparator to establish construct validity of the 5SST among soccer players in the original study by Thorborg et al. 17 The correlation between the 5SST result and HAGOS Sport score found in the present study was of moderate strength and therefore appears to be weaker in ice hockey players than in soccer players. 17 Our data suggest that ice hockey players with pain during the 5SST are less affected in their perceived sporting function than soccer players when considering similar pain ratings. Groin pain is common in both soccer and ice hockey, 15 2 sports that include rapid acceleration, deceleration, and change in directions. Despite these similarities, the specific physical demands of the 2 sports may affect the extent to which hip and groin pain affects sporting ability. Furthermore, it is possible that ice hockey players evaluate pain differently than soccer players.
We found moderate correlations between the 5SST result and adduction strength, indicating that players with more pain during the 5SST were weaker than players with less or no pain during the test. This is in line with previous studies that have found impairments in adduction strength in athletes with groin pain compared with pain-free athletes. 14 Reduced adduction strength is also a suggested risk factor for groin injuries 24 but can be addressed by appropriate strengthening strategies. 9 In professional ice hockey, preseason strengthening of the adductors has been shown to reduce the risk for groin injuries. 21 It is therefore of clinical relevance to identify players with reduced adduction strength to address those deficits early. The 5SST is intended to be used as a tool to categorize players according to risk groups based on pain ratings through the application of a traffic light approach, 17 and our data suggest that this approach can also differentiate between different levels of strength in ice hockey players. Therefore, in addition to being an indicator of self-reported sporting function, the 5SST may be used as a quick indicator of impairments in adduction strength.
Players with low pain intensity were found to be significantly stronger for all measures compared with players with medium pain intensity. Abduction strength as well as adduction-to-abduction ratios did not differ significantly between players with low and high pain intensity, but ESs for the differences were larger than for the statistically significant differences between the low and medium pain intensity groups. The absence of a statistical significance could likely be explained by a lack of statistical power due to the relatively small number of players with a high pain rating. Hence, our results indicate that players with high pain intensity during the 5SST may also be weaker in abduction and have lower adduction-to-abduction ratios than players with low pain intensity. However, studies with larger sample sizes are needed to confirm these observed results. Only small and insignificant ESs were found between players with medium pain intensity and players with high pain intensity.
Similar to previous findings in soccer players, 17 we found the traffic light approach differentiated between all pain intensity groups (green, yellow, red) regarding self-reported hip-related sporting function in ice hockey players. Furthermore, it showed capability to clearly differentiate levels of strength between players with low pain intensity (green) and more pain (medium [yellow] or high [red]). Hence, while a green light during the 5SST can be interpreted as acceptable function, a yellow or red light (NRS score >2) indicates that a player may have strength deficits requiring further investigation and treatment. With its ability to reflect both strength and self-reported hip-related sporting function through a 5-second test of groin pain severity, the 5SST could be a powerful tool for rapid measurements used to monitor hip and groin health in ice hockey players. Therefore, the 5SST may be used to identify players in subclinical or clinical phases of hip and groin injuries that may benefit from secondary or tertiary prevention strategies. 10 The 5SST, which requires minimal time to perform, could be used for in-season monitoring, as proposed by Wollin et al 26 in their study on youth soccer players.
Based on our results, it appears that ice hockey players with a yellow light during the 5SST may benefit not only from appropriate load management and a reduction of provoking activities but may also need to add strength work, with a focus on both adductors and abductors, with the adductors seemingly needing the most attention. This may in turn prevent the deterioration of symptoms (secondary prevention). Players with a red light during the 5SST presented with significantly reduced self-reported hip function in comparison with players with a green or yellow light. They may need to be completely removed from actual play for a while, as their hip and groin sporting function is more severely affected, and they may therefore benefit from tertiary prevention in the form of active rehabilitation. 8
It has to be acknowledged that this study is cross-sectional. Hence, no inference of results regarding the causal relationship between muscle weakness and subjective pain experience during the 5SST can be made. Even though studies using experimentally induced musculoskeletal pain models have suggested that higher subjective pain ratings indicate reduced muscle strength, 5,7,23 no studies have shown this in patients with long-standing hip and groin pain. While we cannot exclude the presence of pain inhibition during our strength measures, similar testing methods have shown to not be significantly correlated with subjective pain ratings. 16 Furthermore, athletes with long-standing hip and groin pain have been found to have strength deficits that cannot be explained by their subjective pain ratings. 4,18 In line with these findings, we consider the strength results presented in this study to be a valid representation of strength impairments in players with a red or yellow light.
Our study investigated the relation between the 5SST result and self-reported hip and groin function as well as hip muscle strength. We emphasize that the 5SST is not intended as a diagnostic test or as a single measure replacing further specific strength tests or clinical assessments. Based on our results, we recommend that clinicians use the 5SST as an indicator of hip and groin function. As such, the 5SST may initiate further assessments and specific strength testing to identify targets for early intervention or rehabilitation. However, the extent to which the 5SST can be used to guide the management of affected players needs to be investigated using prospective study designs.
Conclusion
In this study, the 5SST results correlated significantly with self-reported sporting function as well as hip muscle strength; higher pain levels experienced during the 5SST were associated with worse self-reported sporting function and decreased hip muscle strength. The categorization of 5SST results according to levels of groin pain (traffic light approach) was able to differentiate between levels of self-reported sporting function in ice hockey players. Categorization according to the traffic light approach also showed that players with a yellow or red light (NRS score >2) during the 5SST were significantly weaker than players with a green light (NRS score ≤2). Regular 5SST-testing is quick and easy and may allow clinicians to early identify and manage ice hockey players with yellow and red light ratings.
Footnotes
Acknowledgment
The authors thank Victor Anderberg and Albert Olsson for their contribution during data collection as well as Laura Krohn and Lasse Ishøi for the reliability of strength testing used in the present study. Furthermore, they thank all club officials and especially thank all participating players for their contribution to this study.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Lund University (Dnr 2017/128).