
Abstract
Background:
Previous studies have acknowledged the medial patellofemoral ligament (MPFL) as the primary stabilizer of the patella, preventing lateral displacement. MPFL reconstruction (MPFL-R) restores stability and functionality to the patellofemoral joint and has emerged as a preferred treatment option for recurrent lateral patellar instability.
Purpose:
To objectively measure biomechanical characteristics of athletes cleared for return to sport after MPFL-R compared with healthy controls.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A prospective case-control study design was employed on 31 total athletes. Sixteen athletes (6 male, 10 female; mean age, 16.1 ± 2.74 years; 385 ± 189 days after surgery and 235 ± 157 days after return to sport) underwent MPFL-R and were medically cleared to return to sport. This group was matched by age, sex, and activity level to 15 healthy athletes with no history of lower extremity injuries. Athletes and controls completed validated questionnaires as well as hopping, jumping, and cutting tests with 3-dimensional motion analysis and underwent strength, flexibility, laxity, and balance assessments.
Results:
Participants in the MPFL-R group scored significantly lower (worse) on the International Knee Documentation Committee (IKDC) (89.2 ± 7.6 vs 98.1 ± 2.0, respectively; P = .0005) and significantly higher (worse) on the Tampa Scale for Kinesiophobia (TSK) (32.4 ± 5.0 vs 25.4 ± 6.5, respectively; P = .006) than those in the control group, but there was no difference in the Kujala score (95.6 ± 5.3 vs 98.8 ± 3.0, respectively; P = .06). Participants in the MPFL-R group demonstrated reduced hip and ankle flexion relative to those in the control group (P < .05). Participants in the MPFL-R group also took significantly longer to complete the 6-m timed hop test relative to those in the control group (P < .05). No statistically significant differences were found in anthropometrics, knee extension or flexion strength, hamstring flexibility, hip abduction strength, or joint laxity between the MPFL-R and control groups.
Conclusion:
The current data indicate that MPFL-R generally restores functional symmetry, while subtle deficits in global power may remain after being released to full activity. Clinicians should ensure that athletes are fully rehabilitated before returning to sport after MPFL-R by emphasizing functional multijoint exercises.
A lateral patellar dislocation (LPD) is a common acute knee disorder in the adolescent athletic population, occurring with an annual incidence of approximately 43 in 100,000. 9,25 This injury presents clinically with decreased range of motion in the knee, swelling, and single or recurrent “giving-way” events of the knee that prevent normal physical activity. 3 Unless there is evidence of articular cartilage damage or intra-articular loose bodies, the initial management plan for an LPD consists of a short period of immobilization, followed by nonsurgical restorative rehabilitation. 28 However, the risk of patellar instability or subsequent dislocations/subluxations has been reported to be as high as 70% in children aged 11 to 14 years. 28 Long-term comorbidities of an LPD include patellofemoral osteoarthritis in tandem with a decline in physical fitness and psychosocial coping levels. 3,33,37 Similar to anterior cruciate ligament (ACL) injuries, female athletes between the ages of 10 and 17 years are at a higher risk of sustaining LPDs. 5,16,38
The medial patellofemoral ligament (MPFL) gives the patella lateral stability and is the primary ligament involved in LPDs. 1,7,34,39 MPFL reconstruction (MPFL-R) is an option that is typically reserved for patients when an LPD recurs or if there is failure to regain functional abilities after nonsurgical rehabilitation. 26,27 Because MPFL-R effectively re-creates the MPFL and restores patellofemoral joint stability and functionality, it has become the preferred procedure for athletes hoping to return to sport. 6 In a recent prospective analysis of MPFL-R patient data, 84.1% of athletes returned to their previous level of sport participation, with only 1.2% reporting recurrent patellar instability. 31
Presently, there is a lack of agreement or available objective criteria by which clinicians can evaluate patients’ knee function after MPFL-R to dictate when the patient can safely return to competitive sport activity. 8 Conventionally, sports medicine physicians have utilized patients’ range of motion, flexibility, anatomic alignment, strength, and other subjective criteria to medically clear athletes for return to sport. 30 A recent systematic review found that for most studies, the rehabilitation guidelines for athletes undergoing MPFL-R included weight and range of motion restrictions, while only 18.9% of studies included objective or patient-centric criteria in determining return to sport. 40 However, some athletes return to sport at a lower level than before undergoing MPFL-R. 18 These poor outcomes between rehabilitation management and level of return to sport provide an opportunity to improve the treatment of athletes undergoing MPFL-R and enable them to return to their preinjury activity level. The purpose of this study was to characterize functional and biomechanical differences between athletes undergoing MPFL-R and healthy controls while initiating an effort to make clinical decision making for athletes returning to sport after MPFL-R more evidence based and objective.
Methods
Research Design
A case-control study design was utilized to evaluate clinical outcomes and dynamic lower extremity function, strength, and neuromuscular control in athletes after the treatment of LPDs with MPFL-R compared with healthy controls. The research design and protocol were approved by an institutional review board, and signed informed consent/assent forms were obtained from all participants and their guardians before data collection.
Participants
A group of 16 adolescent athletes who underwent MPFL-R was recruited for the present study via referrals from local orthopaedic surgeons, physical therapists, and primary care physicians. Additionally, 15 healthy controls, matched on age, sex, and activity level, participated in this study. The controls were recruited in one of 2 ways: (1) by asking the surgical patient to bring a peer of the same age and activity level or (2) by contacting local schools. Football, soccer, basketball, and volleyball were the most common sports among participants in both the MPFL-R and control groups.
To be included in the study, athletes in the MPFL-R group must have (1) been within the ages of 10 to 25 years; (2) suffered an LPD with pivoting, cutting, or jumping activities; (3) completed presurgical and postsurgical rehabilitation before and after MPFL-R; and (4) been cleared to return to sport participation. Athletes were excluded from the study if they had (1) undergone prior lower extremity orthopaedic surgeries other than procedures for patellar instability, (2) lower extremity injuries within the past 3 months other than a patellar dislocation, (3) neurological disorders or medical conditions that affected neuromuscular performance, or (4) an LPD managed with nonsurgical rehabilitation. All exclusion criteria applied to the healthy controls, while the only criteria needed for inclusion were similar age, sex, and activity level to athletes in the MPFL-R group. Participants in the control group were chosen based on the type of sport/activity involvement that most closely aligned with those in the MPFL-R group who were included in the study.
Procedures
A 5-station screening system consisting of anthropometrics, patient-reported outcome measures (PROMs), motion analysis, strength testing, and hopping tests was used to assess the clinical outcomes of the MPFL-R athletes and the healthy controls. Participants in both the MPFL-R and control groups completed PROMs before arrival at the facility. The order of testing for the MPFL-R group was the following: (1) anthropometrics, (2) motion analysis (drop vertical jump [DVJ] and single-legged drop landing [SLD]), (3) hopping tests, and (4) strength testing. The order of testing for the control group was the following: (1) strength testing, (2) anthropometrics, (3) motion analysis (DVJ and SLD), and (4) hopping tests. This order was determined by the availability of the testing equipment and training staff. No participants in the MPFL-R and control groups complained of fatigue and/or pain after any of the tests.
Anthropometrics
Height and weight were recorded using a standard stadiometer and physician’s scale. The body mass index of the athlete was then calculated from these parameters. A tape measure was used to measure leg length from the athlete’s anterior superior iliac spine to the lateral malleolus. Anthropometric measurements were used to normalize strength and functional performance data.
Patient-Reported Outcome Measures
Participants in the MPFL-R and control groups completed 4 knee/activity questionnaires: International Knee Documentation Committee (IKDC), Kujala Anterior Knee Pain Scale, Tampa Scale for Kinesiophobia (TSK), and Marx Activity Rating Scale. These questionnaires have been evaluated for their reliability and validity in assessing an adolescent athletic population returning from ACL and other knee injuries. 10,12,24,29 The IKDC is a 10-item knee-specific measurement tool assessing symptoms, sport activity, and function; it is scored by summing the individual items and then transforming the score to a scale from 0 to 100. A score of 100 represents no limitations with activities of daily living or sport activities and the absence of symptoms. 11 The Kujala Anterior Knee Pain Scale is a self-administered, knee-specific scale with 13 items assessing the following: limp, mobility aid dependency, walking, stair climbing, squatting, running, jumping, prolonged sitting with the knee flexed, pain, swelling, instability, thigh atrophy, and flexion deficiency. The scale is scored from 0 to 100, with lower scores representing greater disability. 35 The TSK is a 17-item self-administered questionnaire aimed at quantifying the fear of reinjuries due to movement and physical activity. Each item is provided with a 4-point Likert scale. The sum of the items provides a score from 0 to 51, with a higher score indicating more fear. 15 The Marx Activity Rating Scale is composed of 4 questions regarding the frequency of running, cutting, decelerating, and pivoting in the past year. The maximum possible score for this scale is 16, and a higher score indicates a greater level of activity. 32
3-Dimensional Motion Analysis
Motion data were collected using a 44-camera, real-time, high-speed, 3-dimensional motion analysis system (Motion Analysis) sampling at 240 Hz. Before undertaking data collection, 1 investigator (K.K.) equipped each athlete with 43 retroreflective markers placed on the sacrum, thorax (posterior cluster of 3 noncollinear markers), sternum, and C7 and bilaterally on the shoulder, upper arm, elbow, wrist, anterior superior iliac spine, greater trochanter, midthigh, medial and lateral femoral condyles, tibial tubercle, midshank, distal shank, medial and lateral malleoli, and a standardized shoe (Supernova Glide 2; Adidas) with markers embedded at the heel, lateral foot (fifth metatarsal), posterior foot (between the heel and lateral foot), and toe (between the second and third metatarsals) (Figure 1). Ground-reaction force data were collected from 2 embedded force platforms (AMTI) sampling at 1200 Hz and were synchronized with video data.

Depiction of retroreflective marker placement on participants in the medial patellofemoral ligament reconstruction (MPFL-R) and control groups during 3-dimensional motion analysis. (A) Front and back views of marker placement. (B) A backpack with a cluster of 3 noncollinearly placed markers. (C) A standardized shoe with 4 embedded markers.
Before dynamic movement trials, a static trial was conducted in which the participant was instructed to stand in a neutral position with foot placement standardized to the laboratory’s global coordinate system. Motion and force data were then collected on each athlete performing a number of landing and jumping tasks as described below. Both the marker trajectories and force data were filtered using a low-pass, fourth-order Butterworth filter with a cutoff frequency of 12 Hz. Lower extremity Cardan angles and internal joint moments in the sagittal plane were then calculated from these data using inverse dynamics analysis in Visual3D (C-Motion).
Drop Vertical Jump
Athletes performed 3 DVJ trials from a 31-cm box (Figure 2). To perform the task, athletes were instructed to drop off the box with both feet at the same time, land on the force platforms in front of the box, and immediately perform a maximum-effort vertical jump while reaching up with both hands to grasp an overhead target. Trials were repeated if athletes did not leave the box with both feet at the same time (ie, led with one foot), did not perform a maximum vertical leap immediately upon landing, or did not land with one foot on each of the force plates (ie, if both feet landed on the same force plate or if they did not land fully on the force plates). There was no number of maximum trials for the DVJ task or any other task in which trials were repeated.

Depiction of the drop vertical jump task during 3-dimensional motion analysis.
Single-Legged Drop Landing
Athletes also performed 3 SLD trials for each side from the 31-cm box (Figure 3). The athletes were instructed to align their foot on a piece of tape affixed to either the left or right of the box, balance on that foot only, drop off the box, and land on the force platform in front of the box on the same leg. After landing from the box, the athletes were instructed to hold the landing for a minimum of 2 seconds. Trials were repeated if athletes were unable to hold the landing upon contact with the force platform. The athletes were given instructions and the opportunity to perform several practice trials before the commencement of this test.
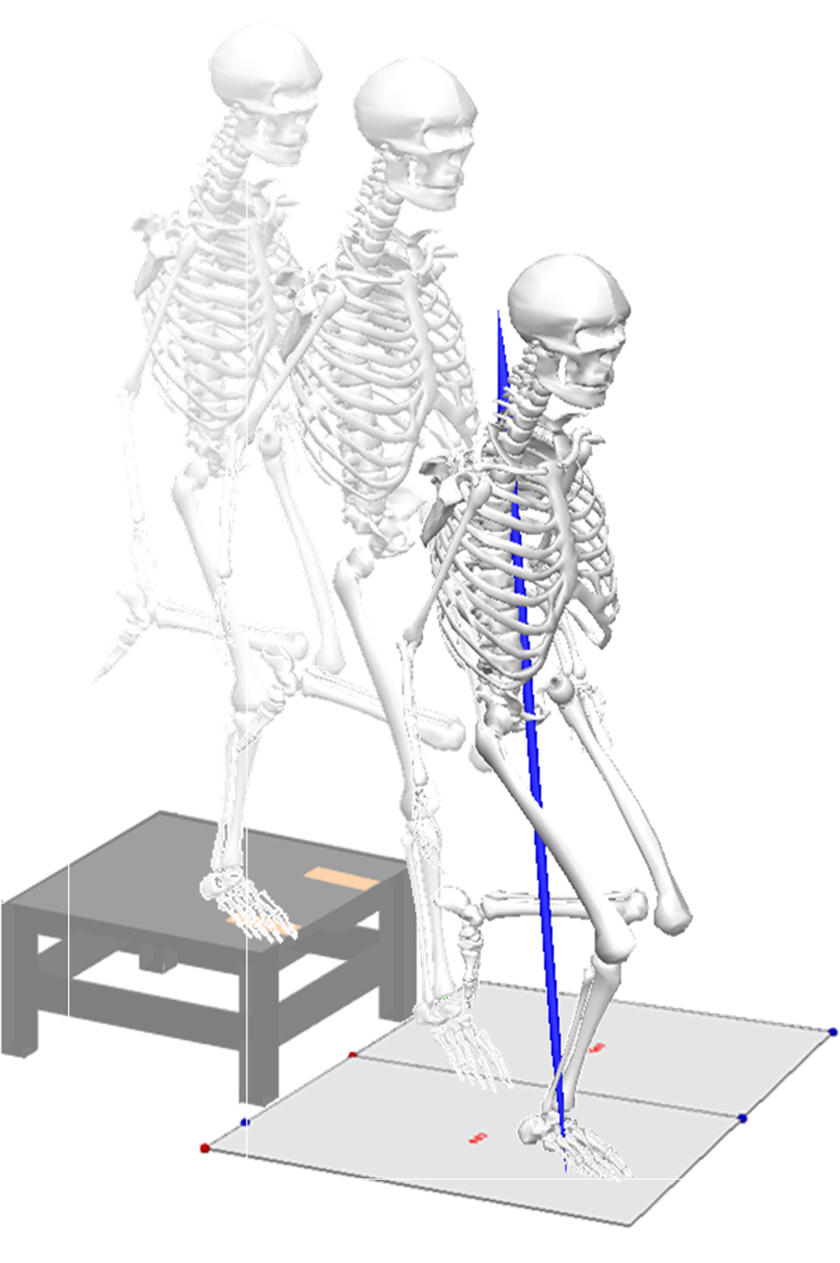
Depiction of the single-legged drop landing task during 3-dimensional motion analysis.
For all trials of both the DVJ and SLD tasks, sagittal-plane lower extremity angles and moments were calculated during the landing phase of the movement. The landing phase was defined as the time from initial contact with the force plate (subsequently defined as the time point at which the vertical ground-reaction force exceeded 20 N) to toe-off for the DVJ task and 500 milliseconds after initial contact for the SLD task. Data during the landing phase were normalized to 101 points and averaged across trials of the respective task for a given participant, and peak values for each of the lower extremity angles and moments were computed from the average time series and were aggregated across all participants.
Hopping Tests
To assess dynamic lower extremity function, each athlete performed 4 different single-legged hop tests: (1) a single-legged hop for distance, (2) a triple crossover hop for distance, (3) a triple hop for distance, and (4) a 6-m timed hop (Figure 4). These hop tests have demonstrated moderate to high reliability with low measurement errors in active children. 14 The single-legged hop for distance involved the athletes starting on one leg and hopping for maximal distance while being able to control the landing. If the landing was not controlled (ie, if athletes lost their balance, needed a second landing for stabilization, etc), the trial was repeated until the landing was controlled. The triple crossover hop involved the athletes performing the triple hop for distance while crossing over a line on the floor with each hop. The athletes started with a hop in the medial direction relative to their hopping foot. If the athletes were unable to control the final landing, the trial was repeated until the landing was controlled. The triple hop involved the athletes performing 3 single-legged hops in a row, each for maximal distance, and controlling the final landing. The 6-m timed hop involved the athletes hopping on one foot as fast as possible for a distance of 6 m. Time was recorded from the moment their starting movement was initiated through the point when they reached the 6-m distance. All athletes were given 2 practice trials and then performed 2 measured trials for each hop test on each leg, and the data from each of the measured hop tests were averaged for each leg. Time and distance for all of the trials were recorded using 3-dimensional motion analysis.

Representation of hopping test procedures utilized by participants in the medial patellofemoral ligament reconstruction and control groups to assess dynamic lower extremity function. 22 (Reprinted with permission from Myer GD, Schmitt LC, Brent JL, et al. Utilization of modified NFL Combine testing to identify functional deficits in athletes following ACL reconstruction. J Orthop Sports Phys Ther. 2011;41(6):377-387.)
Strength Testing
Knee flexion and extension strength were measured using an isokinetic dynamometer (Biodex Medical Systems), for which the setup procedures have been previously reported. 21 Participants performed a series of 5 maximum-effort isokinetic knee extension and knee flexion trials at a speed of 300 deg/s as practice. Once practice trials were completed and the participants were comfortable with the task, a 10-repetition trial was completed. Peak values of knee flexion and extension torque were recorded and normalized to each participant’s body weight. To evaluate hip muscle strength, participants were positioned in the dynamometer in a standing position with their trunk perpendicular to the floor and their hip aligned with the axis of rotation of the dynamometer. Using bilateral upper extremity support, the participants pushed outward into abduction for maximal effort against a padded buttress for 10 repetitions at 120 deg/s. The peak torque across the 10 repetitions was recorded and normalized to body weight. The participants worked in a full arc of motion from 0° to 45°.
Statistical Analysis
Independent t tests were conducted to evaluate differences in anthropometrics (age, height, weight) and PROMs between the MPFL-R and control groups. Two-way multivariate analyses of variance (group × leg) were used to assess differences in sagittal-plane kinematic and kinetic variables during the DVJ and SLD tasks; hip abduction, knee flexion, and knee extension isokinetic strength; and functional performance during the hop tasks (6-m timed hop, single-legged hop for distance, triple hop for distance, and triple crossover hop for distance) between the MPFL-R and control groups. The involved leg of athletes in the MPFL-R group was matched with the respective leg of the healthy controls while taking into account the dominant lower extremity in both the MPFL-R and control groups. Two-way analyses of variance were used to conduct post hoc comparisons between specific variables, and effect sizes were computed using Cohen d. An alpha level of .05 was selected a priori to indicate statistical significance.
Results
Anthropometrics
There were no statistically significant differences between the MPFL-R (6 male, 10 female; mean age, 16.1 ± 2.74 years; mean height, 1.73 ± 0.12 m; mean weight, 80.9 ± 23.3 kg) and control groups (5 male, 10 female; mean age, 17.1 ± 3.27 years; mean height, 1.73 ± 0.13 m; mean weight, 69.3 ± 18.1 kg) on age, height, or weight (all P > .05).
Testing Times and PROM Scores
Athletes in the MPFL-R group were tested at a mean of 385 ± 189 and 235 ± 157 days after surgery and return to sport, respectively. Athletes in the MPFL-R group had significantly lower (worse) scores on the IKDC and significantly higher (worse) scores on the TSK compared with those in the control group (P < .05); however, there were no significant differences between the MPFL-R and control groups on the Marx and Kujala questionnaires. Table 1 displays the results for the PROMs between the MPFL-R and control groups.
Patient-Reported Outcome Measure Scores a

a Data are presented as mean ± SD. IKDC, International Knee Documentation Committee; MPFL-R, medial patellofemoral ligament reconstruction; TSK, Tampa Scale for Kinesiophobia.
b Statistically significant difference between groups (P < .05).
DVJ and SLD Tasks
In the DVJ task, athletes in the MPFL-R group demonstrated statistically significant differences in biomechanics compared with those in the control group (F 6,47 = 2.42, P = .040). Post hoc analyses revealed that athletes in the MPFL-R group exhibited reduced knee flexion and ankle dorsiflexion, as well as decreased knee extensor moments, during landing in the DVJ task (all P < .05) relative to those in the control group. While there were group effects of deficits in the MPFL-R group, there was no significant difference between involved and uninvolved legs in the MPFL-R group or the matched legs in the control group (F 6,47 = 0.87, P = .521). Likewise, there was no significant interaction effect between group, either MPFL-R or control, and leg, either involved or uninvolved, on biomechanical outcomes (F 6,47 = 0.48, P = .819) during the DVJ task.
Similarly, in the SLD task, athletes in the MPFL-R group demonstrated statistically significant differences in biomechanics compared with those in the control group (F 6,45 = 3.38, P = .008). In the SLD task, athletes in the MPFL-R group exhibited reduced ankle dorsiflexion and decreased knee and ankle extensor moments (all P < .05) relative to those in the control group. Table 2 displays the results for the lower extremity variables in both the DVJ and SLD tasks. However, there was no statistically significant difference between involved and uninvolved legs in either group (F 6,45 = 0.38, P = .888). There was also no significant interaction effect between group, either MPFL-R or control, and leg, either involved or uninvolved, on biomechanical outcomes (F 6,45 = 0.72, P = .638) in the SLD task.
Peak Lower Extremity Results During the DVJ and SLD Tasks a

a Data are presented as mean ± SD. DVJ, drop vertical jump; MPFL-R, medial patellofemoral ligament reconstruction; SLD, single-legged drop landing.
b Main effect statistically significant between groups (P < .05).
Hopping Tests
There was a significant main effect for group (F 4,45 = 6.34, P < .001), but not for leg (F 4,45 = 0.16, P = .958) or group × leg (F 4,45 = 0.17, P = .953), in the hopping tests. Post hoc analyses revealed that athletes in the MPFL-R group took significantly longer to complete the 6-m timed hop test relative to those in the control group (P < .05). Table 3 displays the results for the hopping tests.
Hopping Test Results a
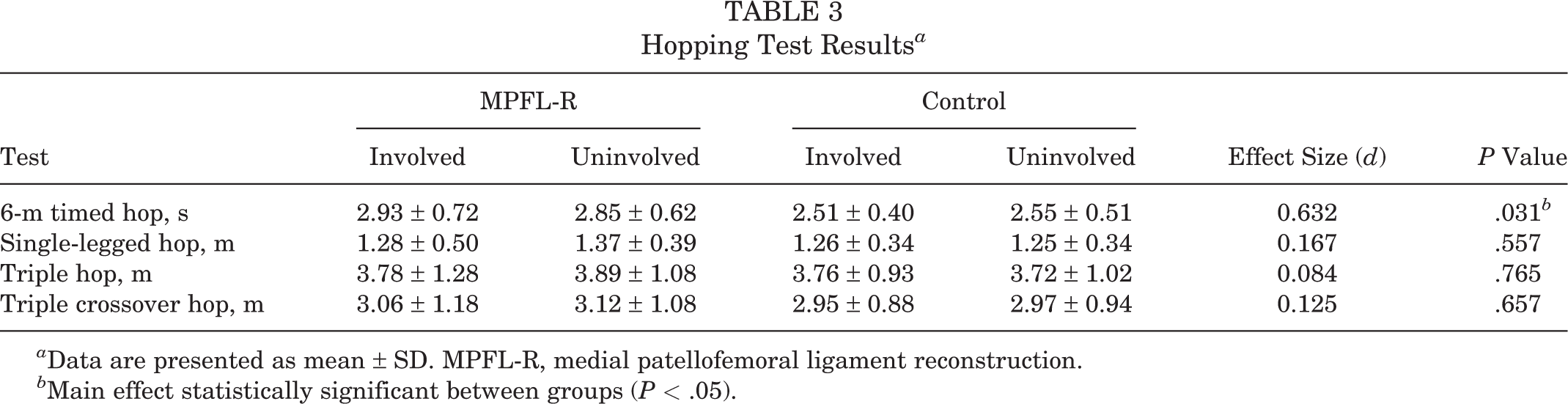
a Data are presented as mean ± SD. MPFL-R, medial patellofemoral ligament reconstruction.
b Main effect statistically significant between groups (P < .05).
Strength Testing
No differences were found in hip and knee isokinetic strength between groups (F 3,56 = 2.43, P = .074), legs (F 3,56 = 0.75, P = .523), or group × leg (F 3,56 = 0.69, P = .564). Table 4 displays the results for the isokinetic strength tests.
Isokinetic Strength Results a

a Data are presented as mean ± SD. MPFL-R, medial patellofemoral ligament reconstruction.
Discussion
The purpose of the present study was to obtain objectively quantified information that can be used to inform clinical decision making regarding return to sport in athletes undergoing MPFL-R by characterizing the functional and biomechanical performance of a group of these athletes relative to healthy controls. Athletes in the MPFL-R group were found to exhibit significant biomechanical deficits compared with those in the control group—namely, reduced sagittal-plane angles and internal joint moments (reflective of relative quadriceps recruitment) of the knee during both a bilateral (ie, DVJ) and unilateral (ie, SLD) landing. Athletes in the MPFL-R group also exhibited functional deficits, taking significantly longer than healthy controls to complete the 6-m timed hop test. The use of functional and biomechanical testing may elicit deficits resulting from MPFL-R that may not be evident in other clinically established tests, such as isokinetic strength testing; in the present study, no differences were found in either the hip or knee between the MPFL-R and control groups. The current findings are an important first step in establishing objective evidence-based criteria to improve rehabilitation management in the treatment of athletes undergoing MPFL-R that will enable them to return to their preinjury activity level.
DVJ and SLD Tasks
Few studies have recorded lower extremity kinematics and kinetics in athletes after MPFL-R compared with healthy controls. Asaeda et al 2 investigated gait in patients with recurrent patellar dislocations who had lower knee extensor moments than healthy controls and found that MPFL-R restores normal knee kinematics and kinetics 1 year after the procedure. In contrast, we found that athletes in the MPFL-R group continued to exhibit reduced knee flexor and extensor moments compared with healthy controls in both the DVJ and the SLD tasks, on average, approximately 11 months after surgery. Premature release to sport, differences in the surgical technique, or a lack of proper rehabilitative therapy may explain these biomechanical differences.
Deficits in knee flexor and extensor moments can result in compensatory strategies that increase the load at other lower extremity joints. For example, while not statistically significant, we found moderate effect sizes in sagittal-plane moments between legs. This indicates that athletes in the MPFL-R group tended to demonstrate a preference (ie, asymmetry) for the uninjured leg in the DVJ task. Moreover, the decrease in knee flexor and extensor moments on both tasks may increase the demand at the hip. This motion puts the patella in a precarious position during dynamic loading and has been associated with other MPFL injury risk factors. Thus, MPFL-R may have limitations in facilitating the restoration of function-landing strategies to the injured leg in athletes undergoing MPFL-R with recurrent lateral patellar instability. Interestingly, the decreased knee flexor and extensor moments in landing mechanics were not associated with concomitant strength or anthropometric outcomes.
Strength Testing
An understudied area identified in a recent meta-analysis acknowledged an opportunity to evaluate hip abduction and hip external rotation as a function of patellar stability because almost 70% of LPDs involve this mechanism of injury. 9,31 Athletes with other patellofemoral conditions, such as patellofemoral pain syndrome, demonstrate significant deficiencies in hip strength testing. Increasing hip abduction strength may prevent these lower extremity injuries. 17,36 Therefore, the hip strength capabilities of athletes undergoing MPFL-R should be evaluated before return to sport to ensure that they return at preinjury activity levels. We found no significant differences in hip isokinetic strength between the MPFL-R and control groups. However, this finding may be a result of rehabilitation emphasizing nonfunctional strength over functional strength. Functional multijoint exercises during rehabilitation with appropriate sport-specific progressions may reduce hip strength deficits in athletes before returning to sport.
Hopping Tests
The 6-m timed hop test has been utilized in the decision-making process and is regarded as the most predictive of the hop tests to assess athletes’ readiness to return to sport after ACL reconstruction. 4,23 Approximately 85% of athletes undergoing ACL reconstruction who completed the 6-m timed hop test at a speed equivalent to a healthy control returned to sport at preinjury levels 12 to 24 months after surgery compared with 44% of those who were slower than controls. 23 We found that athletes in the MPFL-R group took significantly longer than healthy controls on the 6-m timed hop test. This result suggests that athletes undergoing MPFL-R who possess functional deficits, such as a significantly slower 6-m timed hop, may return to sport below their preinjury levels, and it emphasizes the need for proper rehabilitation, including protocols, and injury-specific return-to-sport guidelines.
Neuromuscular Training and Rehabilitation
Limited evidence exists regarding the effect of strength and neuromuscular performance on clinical outcomes, such as time to return to sport after patellar dislocations or MPFL-R. 13,19 Because there were significant biomechanical differences between the MPFL-R and control groups, neuromuscular training and rehabilitation may play a pivotal role in reducing the risk of reinjuries when athletes return to sport. Future trials need to closely monitor the biomechanical and neuromuscular deficits of athletes undergoing MPFL-R and track long-term clinical outcomes, including secondary injuries, activity level maintenance, and other functional measures. Myer et al 20 identified a targeted trunk and hip neuromuscular training protocol to reduce the incidence of ACL injuries in adolescent athletes. A similar program could be initiated for athletes undergoing MPFL-R to increase lower extremity strength and ensure that there are no hip and trunk musculature deficits before returning to sport. These strategies could potentially lead to reduced reinjury rates in athletes undergoing MPFL-R and yield improved objective criteria so that athletes can return to sport at preinjury levels.
Limitations
One important limitation of the study included variability in the testing schedule for athletes in the MPFL-R group who were medically cleared to return to sport. For example, one athlete may have been medically cleared to return to sport and subsequently tested within the next week; however, another athlete may have been medically cleared to return to sport and involved in sport participation for over 3 months before being tested. This latter athlete may have utilized compensatory biomechanical responses, which could have potentially skewed the results of the study. Also, isokinetic strength testing is neither functional nor sport specific, which likely explains why there were no significant differences found between the MPFL-R and control groups. Potential differences in grafts and surgical techniques could also account for some of the persistent deficits in athletes in the MPFL-R group. The lack of statistically significant differences in anthropometrics, isokinetic strength, and Marx and Kujala questionnaires between the MPFL-R and control groups may be because of the relatively small sample size of the study.
While not statistically significant, there was a 16% weight increase in athletes in the MPFL-R group as compared with those in the control group, which may have influenced the kinematic and kinetic measurements in the DVJ and SLD tasks. Also, the insufficient power of the study may account for the lack of statistically significant differences in knee biomechanics between the involved and uninvolved legs of athletes in the MPFL-R group. This MPFL-R group of young, active athletes is also considered to be one of the highest risk groups for this injury; therefore, the results may not apply to an older, less active population with MPFL injuries. There were also minor variations in the type of sports played between participants in the MPFL-R and control groups. Other potential sources of variability in the investigation included leg length measurements and the cluster of 3 posterior, noncollinearly placed markers. The heterogeneity of surgical techniques and rehabilitation protocols is another variable of the study that may have affected the outcomes. Because the purpose of this study was to identify biomechanical and neuromuscular differences in athletes undergoing MPFL-R who have been released to return to sport compared with healthy controls, future trials are necessary to track the long-term implications of the deficits acknowledged in this study.
Conclusion
Currently, there are limited objective data on evidence that compares dynamic and functional outcomes after MPFL-R. The data collected in this pilot study suggest that athletes undergoing MPFL-R return to sport with generally restored functional symmetry but worse subjective ratings of knee function and objective functional deficits in global power compared with healthy controls. These deficits need to be investigated further to determine the implications for long-term outcomes, risk of reinjuries, and successful return to sport at preinjury levels.
Footnotes
Acknowledgment
The authors thank all study participants for their time.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported in part by the National Institutes of Health (grant T35DK060444) and University of Cincinnati’s Department of Orthopaedic Surgery. B.M.G. has received educational support from Arthrex and Smith & Nephew. S.N.P. has received educational support from CDC Medical and is a paid speaker/presenter for Synthes. M.G. has received educational support from CDC Medical. G.D.M. receives publishing royalties from Human Kinetics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Cincinnati Children’s Hospital Medical Center.