
Abstract
Background:
Disruption of the medial patellofemoral ligament (MPFL) may lead to recurrent lateral patellar dislocation and patellofemoral chondral injury. Despite significant previous work investigating numerous performance parameters, the optimal graft choice for MPFL reconstruction for patellar instability remains unclear.
Purpose:
To compare functional outcomes scores, subjective recurrent instability, and revision rates between autograft and allograft in MPFL reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent MPFL reconstruction with autograft between 2013 and 2018 were identified. A 2:1 comparison group of patients who underwent MPFL reconstruction with allograft was matched by sex, age (±3 years), and body mass index (BMI) (±3 kg/m2). Patient characteristics, preoperative radiograph measurements, and intraoperative data were compared between the groups, as were patient-reported outcome measures, including International Knee Documentation Committee (IKDC) score, Lysholm score, Single Assessment Numerical Evaluation (SANE), and visual analog scale (VAS) for pain. Subjective recurrent instability and revision rate were also compared between groups.
Results:
The autograft group was composed of 30 patients (13 male, 17 female) with a mean age of 24.4 years and mean BMI of 25.0 kg/m2, and the allograft group was composed of 60 matched patients (25 male, 35 female) with a mean age of 24.1 years and mean BMI of 25.1 kg/m2. The autograft and allograft groups reported similar IKDC scores (73.0 vs 73.7; P = .678), Lysholm scores (77.5 vs 80.7; P = .514), SANE (72.0 vs 75.8; P = .236), and VAS pain (30.7 vs 26.6; P = .482), as well as similar rates of postoperative patellar subluxations (20.0% vs 19.3%; P = .867) and dislocations (10.0% vs 15.0%; P = .805).
Conclusion:
Both allograft and autograft were found to be viable options for MPFL reconstruction. There were no significant group differences in failure rates, patient-reported outcomes, pain, or complications between autograft and allograft MPFL reconstruction in this series.
The overall incidence of lateral patellar dislocations in the United States peaks during adolescence, with a rate of 29 per 100,000. 8 Based on anatomic studies, the medial patellofemoral ligament (MPFL) is the major medial stabilizer of the patella to lateral translation.6,10 In more than 90% of cases of recurrent patellar instability, there is disruption or incompetence of the MPFL. 16 The literature has demonstrated that, for patients with recurrent patellar instability without significant bony malalignment, an isolated MPFL reconstruction is an efficient and effective surgical solution. 17 There are several graft options available for MPFL reconstruction. Autografts can be harvested from the semitendinosus, gracilis, adductor magnus, quadriceps, or patellar tendon.3,5,7,15,19-21 In addition, allografts, typically semitendinosus or gracilis, can also be utilized with less donor site morbidity and the potential for faster recovery.2,14
Previous studies have shown both autograft and allograft to be comparable in terms of functional outcomes.4,9,13,18 However, many studies have been limited by small sample sizes or a heterogeneous population. In this study, we aimed to compare functional outcomes scores, subjective recurrent instability, and revision rates between patients with autograft and allograft MPFL reconstructions. We hypothesized that there would be no significant differences in clinical outcomes among patients who underwent MPFL reconstruction with autograft versus allograft.
Methods
We identified patients who underwent MPFL reconstruction (Current Procedural Terminology codes 27420, 27422, 27424, 27425, and 27427) utilizing autograft or allograft between January 1, 2013, and December 31, 2018, from the database of our institution. Exclusion criteria included patients with less than 2 years of postoperative follow-up and those who underwent MPFL repair rather than reconstruction. The electronic medical records of all patients were reviewed for date of first reported dislocation, number of dislocations before surgical intervention, previous ipsilateral surgeries, postoperative complications (including arthrofibrosis, deep venous thrombosis, and infection), and subsequent interventions after surgery, including revision surgery, joint arthroplasty, physical therapy beyond the standard rehabilitation protocol, and corticosteroid injections. Patient charts were further reviewed, and demographic and data including sex, age at the time of surgery, and body mass index (BMI) were recorded. A 2:1 ratio comparison group of patients who underwent MPFL reconstruction with allograft during the same time period was created by matching sex, age (±3 years), BMI (±3 kg/m2), time from injury to surgery, mechanism of injury, and preoperative anatomic radiographic measurements. This study was exempt from from review by our institutional review board.
Radiographic Review
The patient’s magnetic resonance imaging (MRI) reports were reviewed for concomitant pathology and the presence of patellar or trochlear chondral injury. Preoperative radiographs were also reviewed by 2 trained research assistants (J.P., D.F.), who measured the femorotibial angle, Insall-Salvati index, patellar tilt, and sulcus angle. The femorotibial angle was calculated as the angle between the diaphysis of the femur and the tibia on an anteroposterior knee radiograph.
Surgical Technique and Rehabilitation
Indications for MPFL reconstruction included patients with recurrent patellar instability who had failed nonoperative management. Patients first underwent a diagnostic arthroscopy to assess patellar tracking and diagnose and address concomitant pathologies. MPFL reconstruction was then performed using an open approach. A longitudinal medial parapatellar incision was made to expose the superomedial edge of the patella. An interval between fascial layers 2 and 3 was identified. MPFL reconstruction was performed using a single- or double-limbed configuration using either an autograft or allograft in accordance with surgeon preference. At the patella, graft limbs were either docked into predrilled bone tunnels and secured with suture on the contralateral side, fixed with a suture anchor, or docked and fixed in place using interference screws in accordance with number of graft limbs. Similarly, femoral fixation was achieved with either a single interference screw, a variable-tension suture button, or tied directly to the tendon insertion site on the adductor tubercle. All autografts were semitendinosus tendons, and allografts were semitendinosis or gracilis allografts with a minimum folded diameter of 6 mm.
Rehabilitation protocols between operating surgeons unanimously included 2 weeks of weightbearing in a hinged knee brace locked in full extension or until adequate quadriceps control to allow ambulation with an unlocked brace. In addition, patients were encouraged to achieve 90° of flexion within the first 2 weeks, progressing to full range of motion by 6 weeks. At 6 weeks, close chain strengthenining exercises were initiated. Return to light activities such as jogging was allowed at 3 months, and return to sports occured between 4 and 6 months postoperatively.
Patient-Reported Outcomes
Included patients were contacted via the REDCap email server (Vanderbilt University) or direct patient contact via phone call to fill out patient-reported outcome surveys. These included International Knee Documentation Committee (IKDC) score, Lysholm scores, Single Assessment Numeric Evaluation (SANE), and visual analog scale (VAS) for pain. In addition, a custom survey determining the number of subluxations/dislocations experienced since surgery, surgical complications, subsequent procedures, and other nonoperative treatment was administered.
Statistical Analysis
Descriptive statistics, including means, ranges, and standard deviations, were calculated. The Wilcoxon rank-sum test was used to compare continuous variables between the autograft and allograft groups with nonparametric data, while the Student t test was used to compare continuous variables between the groups with parametric data. The Fisher exact or chi-square test was used to compare categorical data. P < .05 was considered statistically significant. All statistical analyses were performed with R Studio (Version 3.6.3) (Posit Software).
Results
A total of 57 patients who underwent MPFL reconstruction with autograft met the inclusion criteria. Of these 57 patients, 6 declined participation and 21 did not respond or were unable to be reached due to expired or invalid contact information. Thus, 30 (52.6%) patients having undergone MPFL reconstruction with autograft completed the postoperative surveys and were included in the final analysis. A 2:1 matched control group of 60 patients who underwent MPFL reconstruction with allograft was created using anatomic parameters, time between injury and surgery, mechanism of injury, and preoperative radiographic measurements as described previously.
A comparison of demographic data is provided in Table 1, and preoperative radiographic data are provided in Table 2. Overall, there were no significant differences between the graft cohorts regarding patient characteristics. Similarly, there were no significant group differences in the preoperative femorotibial angle, Insall-Salvati index, patellar tilt, sulcus angle, or presence of a patellar chondral injury between the 2 cohorts, as listed in Table 2.
Patient Characteristics a

Data reported as mean ± SD or n (%). BMI, body mass index.
Preoperative Radiographic Data a

Data reported as mean ± SD or n (%).
Intraoperatively, a significantly greater proportion of patients in the autograft group underwent MPFL reconstruction with a double-limbed graft configuration (93.3% for autograft vs 61.6% for allograft; P = .002). There were no significant differences in the use of suture anchors at the patella between the 2 cohorts (73.3% for autograft vs 85.0% for allograft; P = .080). Likewise, similar proportions of patients in each group underwent femoral fixation with interference screws (100% for autograft vs 93.3% for allograft; P = .699). Intraoperative data are given in Table 3.
Intraoperative Data a
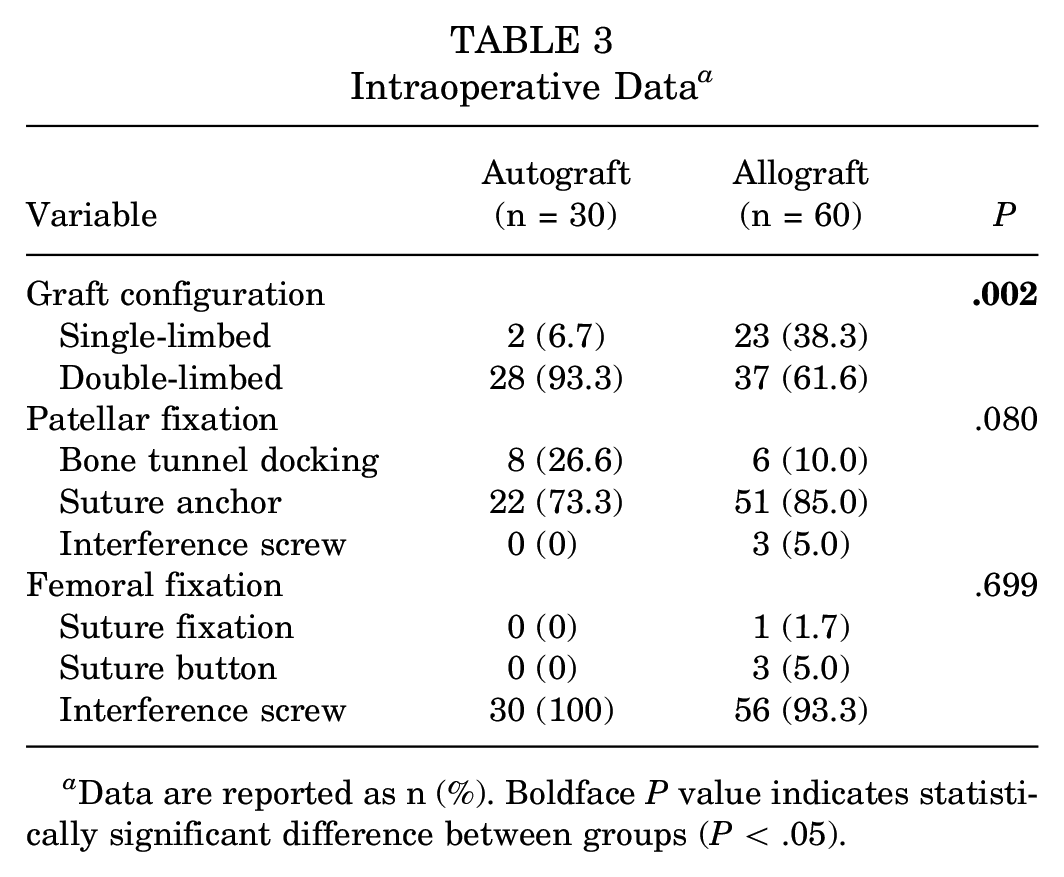
Data are reported as n (%). Boldface P value indicates statistically significant difference between groups (P < .05).
A similar proportion of patients underwent concomitant procedures at the time of surgery (23 [76.6%] for autograft vs 42 [70.0%] for allograft; P = .677). Of the patients undergoing a concomitant procedure, there were no significant differences in the number of patients experiencing greater than 1 simultaneous procedure (12 [52.1%] for autograft vs 18 [42.9%] for allograft; P = .645). Overall, among concomitant procedures, there were statistically significantly more loose body removal procedures for the allograft group versus the autograft group (0 for autograft, 8 for allograft; P = .049). A detailed breakdown of concomitant procedures is provided in Table 4.
Concomitant Procedures a

Data are reported as n (%). Boldface P value indicates statistically significant difference between groups (P < .05). MACI, matrix-induced autologous chondrocyte implantation; OAT, osteochondral allograft transplant.
The mean follow-up time was 5.03 years in the autograft group and 4.10 years in the allograft group. Patient-reported outcomes including IKDC (P = .678), Lysholm (P = .514), SANE (P = .236), and VAS pain (P = .482) did not significantly differ between groups. Detailed patient-reported outcome data are given in Table 5.
Patient-Reported Outcomes a

Data are reported as mean ± SD. IKDC, International Knee Documentation Committee subjective knee form; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Overall, there were no significant differences in rates of postoperative patellar subluxations (P = .867) and dislocations (P = .805), as listed in Table 6. In the autograft group, 24 patients (80%) reported no subsequent subluxations after surgery, 5 patients (16.6%) reported occasional subluxations in sports, 1 patient (3.3%) reported occasional subluxations in daily activities. Similarly, 27 (90%) of patients had no further dislocations, 1 patient (3.3%) reported at least 1 documented dislocation and 2 patients (6.7%) reported more than 2 dislocations. In the allograft group, 49 patients (81.7%) reported no subsequent subluxations after surgery, 8 (13.3%) reported occasional subluxations in sports, and 3 (5.0%) reported occasional subluxations in daily activities. In addition, 51 (85%) of patients had no postoperative dislocations, 3 patients (5.0%) reported at least 1 documented dislocation, and 6 patients (10.0%) reported more than 2 dislocations.
Patient-Reported Patellar Instability a

Data are reported as n (%).
Both groups experienced similar rates of complications with 3 (10%) complications reported in the autograft group and 3 (5%) complications reported in the allograft group (P = .396). In the allograft group, 1 patient experienced a deep venous thrombosis in the postoperative period that resolved with oral anticoagulation, 1 patient experienced arthrofibrosis, and 1 patient experienced a superficial wound infection that was treated with oral antibiotics. In the autograft group, 2 patients experienced arthrofibrosis after surgery and 1 patient required revision MPFL reconstruction 4 years after their index surgery.
Discussion
The results of this study supported our hypothesis that there would be no significant difference in outcomes including IKDC, Lysholm, SANE, VAS pain, self-reported recurrent instability, and revision rate between MPFL reconstruction utilizing autograft versus allograft. These results are also comparable with previous studies that showed no significant differences between autograft versus allograft MPFL reconstruction.
Calvo Rodriguez et al 4 studied 28 patients undergoing MPFL reconstruction with at least 12 months of follow-up. Hamstring tendon autograft was used in 13 patients, whereas allograft was used in 15 patients. There was no significant difference among postoperative Kujala subjective knee scores. No recurrent dislocations or graft-related complications were observed. 4 Flanigan et al 9 examined 57 patients who underwent MPFL reconstruction with allograft compared with 30 patients who underwent reconstruction with autograft. Both groups had a minimum of 1-year follow-up. There were no significant differences regarding recurrent dislocations or recurrent subjective instability. 9 Kumar et al 13 studied 59 patients (36 allografts, 23 autografts) with a mean follow-up of 4.1 years. They found no significant differences in return to activity, pain score changes, and incidence of failure between the use of autograft versus allograft for MPFL reconstruction. Although patients with surviving autografts reported statistically significant higher Kujala scores, this was not clinically significant. 13
The rate of recurrent instability reported in this study is consistent with previous studies. Previous studies have cited subluxation rates of 0% to 37% and 0% to 29%, whereas the present study reported a rate of 20% and 19% for autograft and allografts, respectively.5,9 Likewise, recurrent dislocations have been identified from 0% to 28% and 0% to 8.3% compared with this study’s rates of 10% and 15% for autograft and allograft, respectively.1,4,5,9,11-13 Proposed reasons for operative failure include variability in surgeon technique, small graft size, joint hyperlaxity, and differences in reported follow-up time.1,11,13 Within the scope of this study, factors possibly contributing to the increased rates of recurrence may include time of return to sport, type of sport, or surgical technique utilized.
Hendawi et al 11 found significantly improved outcomes in their allograft group compared with autograft. A total of 21 patients had gracilis tendon autograft, and 35 had allograft gracilis tendon. The autograft group had significantly longer operative times, higher rates of graft failure, and lower Kujala scores. 11 These authors also addressed an underinvestigated aspect of the autograft versus allograft discussion, being the resource burden associated with each graft type. According to their analysis, the longer operative times for autograft harvest and an associated higher incidence of reoperation were associated with an increase in cost of (US) $445 and $34,740, respectively. 11 It is important to note that the driving force behind the associated financial burden of the autograft is undergoing a reoperation for graft failure. In addition, allograft still poses a significant financial burden cost of approximately $1058 per graft. 11 Thus, consideration of patient and practice resources is imperative before final graph choice.
Strengths and Limitations
There are several unique strengths of this study compared with other investigations currently in the literature. Notably, this study analyzes the largest patient population in the literature to date, utilizes a 2:1 matched cohort of 60 patients, and has a longer follow-up time with a mean = of 5.03 years in the autograft and 4.10 years in the allograft group, respectively.
Despite the strengths this study offers, it is not without limitations. Notably, the significant variability in surgical technique utilized for both femoral and patellar graft fixation between the autograft and allograft cohorts. We speculate that advances in graft fixation techniques as well as the availability of novel technology for patellar fixation may have contributed to the disproportionate utilization of certain fixation modalities, such as double-limbed graft technique in the autograft cohort, for example. In addition, given the retrospective nature of this study, recall bias, as well as selection bias, could have impacted reported outcomes, as there were a number of identified patients who chose to not participate in the study, thus limiting questionnaire follow-up. In addition, a lack of randomization of patient groups, graft types, and/or surgical technique utilized could have introduced bias into the study. Similarly, attempts to directly compare this study with previously published works may be limited by differences in outcome assessments utilized such as some studies’ utilization of the Kujula score or assessment with metrics such as the Dejour classification. Another limitation is the absence of recording both patient’s sport of choice, as well as return to sports metrics such as quadriceps or hamstrings strength after autograft harvest. Lastly, this study investigated MPFL reconstruction and included concomitant procedures that were performed. The addition of concomitant procedures may have affected outcomes; however, with only 1 statistically significant difference in number of concomitant procedures, it is our opinion that this effect is negligible.
Conclusion
Both allograft and autograft remain viable options for MPFL reconstruction. There were no significant differences in failure rates, patient-reported outcomes, pain, or complications between autograft and allograft MPFL reconstruction in this series. Based on the available data, we believe MPFL allograft has the potential for decreased donor morbidity, decreased operative time, and functional outcomes similar to those of autograft. We therefore recommend allograft be considered as the graft of choice in MPFL reconstruction. However, we recognize that, depending on practice type, allograft availability, and potential financial considerations, MPFL autograft is still a viable option with similar outcomes.
Footnotes
Final revision submitted November 4, 2023; accepted December 10, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.H. has received education payments form Liberty Surgical. P.P. has received grant support from Arthrex, education payments from Arthrex, and hospitality payments from Axogen and Stryker. K.B.F. has received grant support from Vericel; education payments from Liberty Surgical; consulting fees from Vericel, Innocoll, and Medical Device Business Services; nonconsulting fees from Vericel; and honoraria from Vericel. S.B.C. has received education payments from Liberty Surgical and consulting fees from Zimmer Biomet Holdings. S.H. has received education payments from Paladin Technology Solutions and Liberty Surgical, nonconsulting fees from Arthrex, and hospitality payments from Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Thomas Jefferson University (ref No. 20E.1063).