
Abstract
Background:
Multiple risks predispose professional football players to adverse health outcomes and, in extreme cases, early death; however, our understanding of etiological risk factors related to early mortality is limited.
Purpose:
To identify etiological risk factors associated with all-cause and cause-specific mortality among National Football League (NFL) players.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
Articles examining all-cause and cause-specific mortality risk factors among previous NFL players were identified by systematically searching: PubMed, PsycINFO, Web of Science, and Google Scholar from 1990 to 2017. Study eligibility and quality were evaluated using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Results:
A total of 801 nonduplicated studies were identified through our search strategy. Of these, 9 studies examining 11 different risk factors were included in the systematic review. Overall, the risk of all-cause and cause-specific mortality was lower among NFL players than among the general male population in the United States. Nonwhite athletes, those in power positions, and those with a high playing-time body mass index (≥30 kg/m2) were associated with elevated all-cause and cardiovascular mortality risks.
Conclusion:
Methodological issues associated with the examined all-cause and cause-specific mortality risk factors preclude a definitive conclusion of etiological protective or risk effects. Comparison groups less prone to selection bias (“healthy worker effect”) and a life-course approach to the evaluation of suspected risk factors are warranted to identify etiological factors associated with early mortality among NFL players.
Multiple risks predispose professional football players to adverse health outcomes 15,24,35 and, in extreme cases, early death 1 –3,14,16 –19,36 ; however, our understanding of etiological risk factors associated with early mortality is limited. It is postulated that multiple pathways moderated by National Football League (NFL) player attributes and game-exposures are associated with longevity. 1 –3,14,16,17,19,24,36 Existing evidence, however, is limited by a number of methodological issues (eg, the “healthy worker effect,” misclassified latency periods, and suspected confounding effects). The delineation of etiological risk factors related to early mortality among NFL players is further complicated by competing outcomes such as cardiovascular mortality, catastrophic injuries, and mental health–related mortality.
Cardiovascular mortality is often a concern among certain playing positions, specifically linemen. Linemen tend to have a higher playing-time body mass index (BMI), which is a risk factor for cardiovascular mortality among the general population. 6 However, it is unclear if a higher playing-time BMI directly translates to an increased risk of cardiovascular mortality among NFL players. This is underlined by studies indicating that BMI overestimates adiposity 28 (a prognostic factor for cardiovascular disease risk) among athletes with a large muscle mass. Moreover, BMI after an athlete's NFL career changes differentially by player position. 27 In some regard, the recent decline in cardiovascular mortality among NFL players, 3 attributed to preventive efforts (health promotion) initiated in the late 1990s, 35 lends weight to the notion of temporal programming of risk during and after a player’s career. However, the influences of life-course BMI or adiposity trajectory changes on the cardiovascular risk and mortality are yet to be examined among NFL players.
Football is a contact sport with an elevated incidence of high-impact collisions that can result in catastrophic injuries. Some studies have suggested that physically elite people, through appropriate training-based fitness, can develop physical capacities that protect against injury risk. 13 On the other hand, repeated concussive and subconcussive blows to a player’s head and body are linked to chronic traumatic encephalopathy (CTE) and other neurodegenerative diseases. 16,17,22 Mediated by impaired decision making, 21,33 mental health disorders (eg, depression), 21 and substance and alcohol abuse, 9 football-related physical trauma is suspected to result in early death among NFL players. However, mediation analyses to confirm these relationships are lacking. Although there is a growing recognition of the link between mental health problems and CTE among athletes exposed to repeated traumatic injuries, the case selection in CTE studies is suspect to volunteer-related bias, and a relatively small percentage of deceased NFL player brains have been examined to date. 21,22
Overall, it is unclear whether NFL players are at an increased risk of early mortality from factors associated with football. Therefore, the objective of this study was to identify etiological risk factors associated with all-cause and cause-specific mortality among NFL players. We also discuss study findings in the context of epidemiological validity and provide recommendations for future research.
Methods
Data Sources and Searches
We conducted systematic searches of the existing literature to gather valid information on risk factors associated with mortality among NFL players. Specifically, we searched 3 electronic databases—PubMed, PsycINFO, and Web of Science—for articles published from January 1, 1990, to December 31, 2017. We also searched Google Scholar, previous systematic reviews, and selected study bibliographies for additional articles. The search strategy included the use of combinations of the following keywords for the (1) population of interest (NFL players): pro-football, athletes, elite, sports, players, football players; (2) outcome of interest (mortality): mortality, all-cause mortality, cause-specific mortality, longevity, death, life expectancy, fatal injuries; and (3) risk factors: exposures, risk, risk factors, mediators, moderators. The search results were limited to English-language text.
Study Eligibility, Selection, and Qualitative Assessment
We conducted the search strategy in 3 phases. In phase 1, we screened all documents retrieved based on title and abstract (A.H.O., B.L.K., B.W., and S.S.). Two exclusion criteria in phase 1 were (1) studies not related to American football and (2) no original data. The full text of articles moved to phase 2 were reviewed by A.H.O. and B.L.K. to determine their eligibility. Eligible articles were those that examined (1) NFL populations, (2) mortality outcomes, and (3) risk factor measures of association. We excluded case series and reports. We entered data from all articles moved to phase 3 into standardized electronic forms developed in Microsoft Access. The data included study characteristics (design, geographic location, period, and duration of the study), participant selection, and ascertainment of outcomes and exposures (risk factors). In phase 3, A.H.O. and B.L.K. independently evaluated articles for their epidemiological quality. The authors (A.H.O. and B.L.K.) assessed 8 signaling questions informed by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to summarize 5 quality domains relevant to observational studies: participant selection, prognostic/confounding factors, cointervening exposure, exposure assessment, and outcome assessment. We summarized each domain with a rating of low, moderate, or high risk of bias. We assigned studies with a low risk of bias across all 5 domains with a “good” overall quality rating. Studies with ≥1 moderate- and high-risk ratings were assigned a “fair” and “poor” overall quality rating, respectively. Disagreements or uncertainties were resolved through discussion with B.W. and S.S.
Operational Definitions of Mortality
In this study, all-cause and cause-specific mortality outcomes examined among reviewed studies were limited to those verified using the National Death Index (NDI) initiated in 1979. The NDI provides causes of death coded to the International Classification of Diseases (ICD) in effect at the time of death. In cases in which the NDI was not used, we considered studies and/or mortality outcomes that were verified using death certificates from state vital statistics offices and/or coded by a certified nosologist. Cardiovascular-related mortality was defined based on the ICD-10 classification codes 100 through 178. Catastrophic injury–related deaths were defined as those that occurred during or after a player’s NFL career that were linked to a severe injury to the spine, spinal cord, skull, or brain.
Summary Measures of Mortality Risk Factor Associations
The following mortality (or longevity) risk measures of association were examined in the selected studies: hazard ratio (HR) of death, life expectancy, standardized mortality ratio (SMR), standardized rate ratio (SRR), standardized proportional mortality ratio, mortality rate, mortality odds ratio (OR), and regression and correlation coefficients.
Results
Summary of Reviewed Studies
We identified 801 nonduplicated studies through the search strategy, of which 39 (5%) were eligible for review in phase 2. Of the 39 studies reviewed in phase 2, we excluded 25 studies because of a lack of mortality outcomes, 5 studies exclusively examined non-NFL players, 2 studies were review studies, 3 studies were case series/reports, and 1 study did not report any mortality risk measures of association (Figure 1). Table 1 summarizes the study characteristics of the 8 articles considered in phase 3 (data extraction and quality assessment). We also included results from a recent study by Venkataramani et al 36 that examined the association between NFL career participation and the mortality risk in retirement. Table 2 provides a summary of study-specific epidemiological quality ratings. Briefly, all the articles had a “poor” overall quality rating but were deemed acceptable for a quantitative evaluation.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart of the literature search and study selection process. *Some studies met more than 1 exclusion criterion. ∫A recently published study 36 was not identified through our study search strategy. NFL, National Football League; o/c, outcomes.
Summary Characteristics of Studies Reviewed That Examine Mortality Risk Factors Among NFL Players a

a BMI, body mass index; NFL, National Football League; NR, not reported; US, United States.
b Speed position: quarterback, running back, halfback, fullback, wide receiver, tight end, defensive back, safety, and linebacker. Nonspeed position: defensive and offensive linemen. Excluded: punters and kickers.
Risk of Bias Assessment for Selected Studies That Examine Mortality Risk Factors Among NFL Players a

a NFL, National Football League.
b Cardiovascular mortality.
c All-cause mortality.
d All-cause and cause-specific mortality.
e Neurodegenerative-related mortality.
f Suicide.
All-Cause Mortality
Seven cohort studies (Appendix Table A1) examined 5 risk factors (being an NFL player, player position, length of career, race/ethnicity, and playing-time BMI) associated with all-cause mortality among previous NFL players in 6 cohorts: <1940, 1 1959-1988, 2,3,16,17 1970 and 1994, 14 1986-2012, 19 and 1982-1992. 36 Overall, the risk of all-cause mortality was lower among NFL players than among the general population of men in the United States (US), even after adjusting for differences in the length of players’ career in years (SMR range, 0.42-0.60), position (SMR range, 0.22-0.72), playing-time BMI (SMR range, 0.31-1.12), and race/ethnicity (SMR range, 0.39-0.63). 3,14,19
Among NFL players, Lincoln et al 19 showed that power positions (vs speed: SMR, 2.16 [95% CI, 1.62-2.86]), nonwhite race (vs white: SMR, 1.63 [95% CI, 1.21-2.21]), and higher playing-time BMI (vs <30 kg/m2: 30-34 kg/m2 : SMR, 1.51 [95% CI, 1.10-2.06] and ≥35 kg/m2: SMR, 3.84 [95% CI, 2.66-5.54]) were associated with a higher risk of early mortality. Similar results were reported by Koning et al 14 for race and player position among NFL players who played during the 1970 season (but not among those who played during the 1994 season). Conversely, for BMI, Abel and Kruger 1 showed a reversed relationship: a higher BMI was associated with a lower risk of mortality. In addition, Abel and Kruger 1 found that increased longevity was associated with longer playing careers, while Lincoln et al 19 did not. Koning et al 14 also reported no association (P = .60) between career length and mortality in a comparable reference period (1994 season) but found an elevated mortality risk (HR, 4.47; P = .01), with more games played at an earlier reference period (1970 season). Venkataramani et al 36 showed that the mortality risk was not different between NFL career and replacement players who participated in the NFL during a 3-game league-wide player strike in 1987, even after adjusting for differences in player position, playing-time BMI, and height (HR, 1.38 [95% CI, 0.95-1.99]).
Cardiovascular Mortality
Four cohort studies (Appendix Table A2) examined 6 cardiovascular mortality risk factors: being an NFL player, player position, length of career, race/ethnicity, playing-time BMI, and reference period. 2,3,16,19 Similar to overall mortality, irrespective of age, position, and race/ethnicity, the risk of cardiovascular mortality was lower among NFL players compared with US men (SMR range, 0.68-0.71). 2,3,16,19 An NFL player follow-up that occurred in 2000 or after was associated with a 72% lower risk of cardiovascular mortality (HR, 0.28 [95% CI, 0.12-0.71]) than an earlier follow-up that occurred before 1980. 3 Among NFL players, high (≥30 kg/m2) playing-time BMI (SRR range, 3.90-9.03), nonwhite race/ethnicity (HR, 1.57 [95% CI, 1.15-2.55]3 and OR, 1.70 [95% CI, 1.01-2.98]2), and power positions (SRR range, 2.12-2.99) were associated with an increased risk of cardiovascular mortality. 2,3,19
Catastrophic Injuries
For catastrophic injury–related mortality, 4 cohort studies (Appendix Tables A3–A5) examined 3 risk factors: being an NFL player, and player position. 16,17,19,23 Overall, NFL players had a lower risk (SMR range, 0.63-0.69) of injury-related death than the general population of US men, irrespective of position played or race/ethnicity. 16,19 However, neurodegenerative causes of death (eg, dementia/Alzheimer disease and amyotrophic lateral sclerosis), also linked to a player’s NFL career, were higher among speed position players (ie, fullback/halfback/defensive back/running back/quarterback, linebacker, tight end, and wide receiver positions: SRR, 4.74 [95% CI, 2.59-7.95]) than US men. 16
Conversely, Lehman et al 16 showed that the risk of brain- and nervous system–related deaths was not different among NFL players versus US men (SMR range, 2.83-3.26). A case-control study conducted by McKee et al 23 showed that career length (P < .01), years since retirement (P < .01), and age at death (P < .01) were positively correlated with a pathological stage of CTE. Their study did not find an association between family-reported numbers of concussions, years of education, lifetime steroid use, player position, APOE e4 allele gene, and stage of CTE (P > .05).
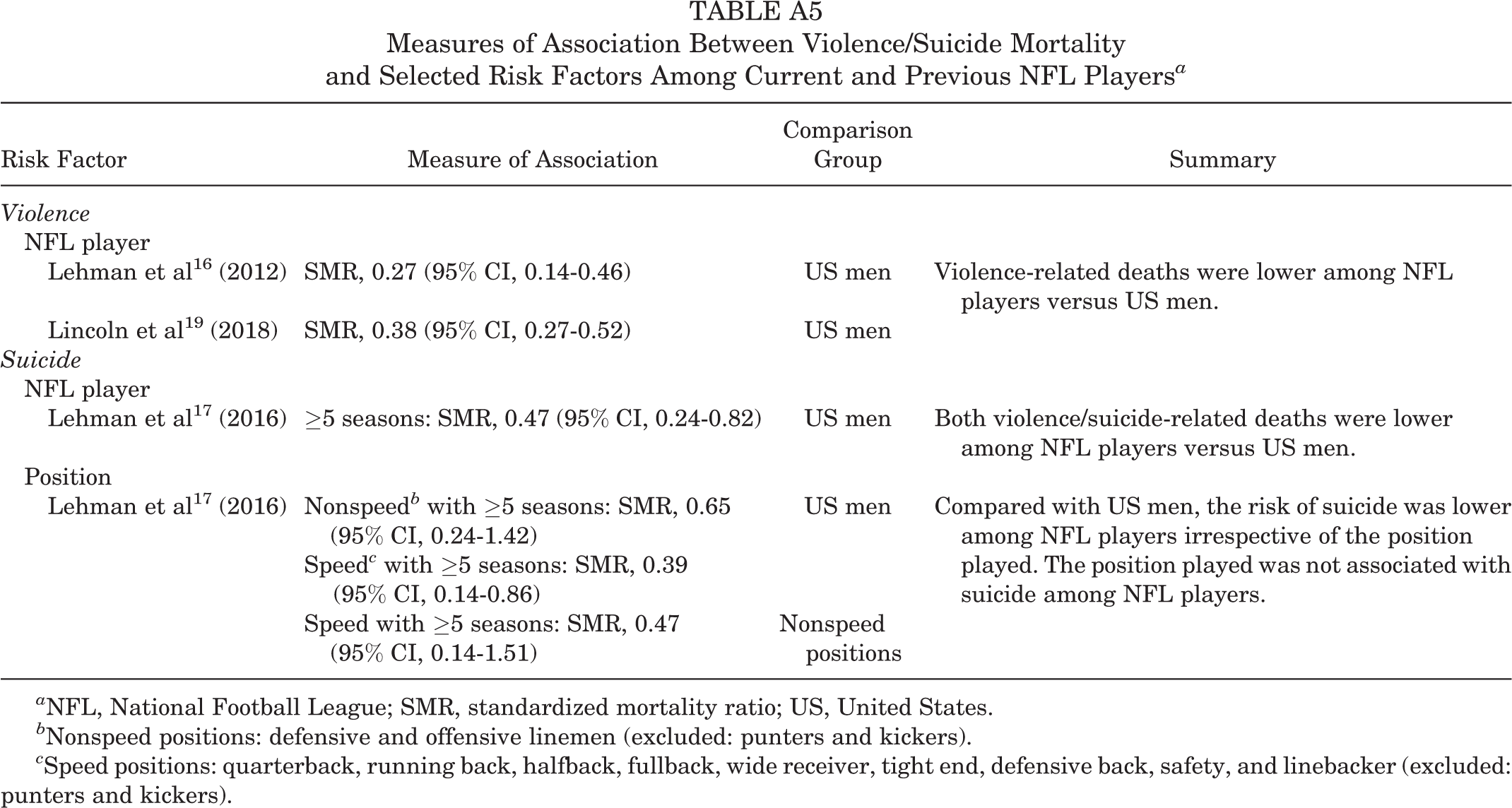
Although not proximately related to football injuries, the mortality risk associated with violence (SMR, 0.27 [95% CI, 0.14-0.46]) 16 and suicide (SMR, 0.47 [95% CI, 0.24-0.82]) 17 was lower among NFL players than US men. Among NFL players, there was no difference in the mortality risk between speed and nonspeed position players (SMR, 0.47 [95% CI, 0.14-1.51]). 17
Discussion
The reviewed studies suggest that the risk of all-cause and cause-specific mortality is lower among NFL players than among the general population of US men. 2,3,14,16,17,19 Among NFL players, nonwhite race/ethnicity, 14,19 power positions, 14,19 and high playing-time BMI (≥30 kg/m2) 2,19 were associated with elevated all-cause and cardiovascular mortality risks. NFL speed position players (vs US men) had an elevated risk of neurodegenerative-related death. 16 Overall, however, a number of methodological issues associated with all-cause and cause-specific mortality risk factors among NFL players in the existing literature 6 –11 preclude a definitive conclusion of etiological protective or risk effects.
One issue is that the all-cause and cause-specific SMR measure of association is prone to considerable bias because the case fatality rate and associated duration of illness vary widely between NFL players and the general population of US men. The case fatality rates of underlying causes of death such as cardiovascular disease are likely lower among NFL players than the general population of US men. Even when adjusted for potential confounders (playing-time BMI, age, race/ethnicity, and career length), the life span advantage conferred by health care access and quality (ie, early diagnosis, more effective treatment, and care that leads to better health outcomes) received by NFL players probably outweighs that of the general population. This is true even if an underlying cause of death (eg, CTE and related neurodegenerative diseases) is more prevalent among NFL players. 26 On the other hand, differences in health care between NFL players and the general population of US men may lead to the differential misclassification of underlying and contributory causes of death, resulting in an overestimate of certain causes (eg, neurodegenerative disease) among NFL players because of diagnostic suspicion. This bias is likely lower in NFL research studies conducted after the initiation of the NDI in 1979, which required rigorous fidelity checks for consistency in cause of death definitions at the state and national levels.
A second issue is that the underlying causes of death related to chronic diseases (specifically, cardiovascular disease) are set in train long before a clinical diagnosis is possible 20,32 ; therefore, measuring risk factors earlier in life among NFL players may provide more relevant etiological measures of risk than relying on time-dependent risk factors during and after a player’s NFL career. Indeed, the differentially long latency associated with chronic diseases may explain the differential effects of playing-time BMI observed on all-cause and cardiovascular-related mortality between reference periods examined in the existing literature. 1 –3,14,16,19 Moreover, existing evidence shows that the net effects of adulthood exposures on chronic disease and mortality risk are low to moderate at best. 4,5,12 Therefore, early-life exposures examined via a life-course approach are critical to the valid identification of etiological risk factors related to early mortality among NFL players.
A third issue is that estimating SMR entails determining the number of expected deaths in a standard population (ie, standard NFL and US male population) via a statistical model and then computing the observed/expected ratio. For comparisons made in the studies that we reviewed, 1 –3,14,16,17,19 what constitutes a “standard population” is clearly different between the 2 groups being compared, and therefore, the use of direct “observed” deaths likely overestimates the risk in the smaller NFL population. To the extent that football can differentially influence health and hence mortality between NFL players and US men, SMR comparisons are a useful measure of association; however, they may overestimate the attributable risk or “cause-specific mortality.”
All-cause and cardiovascular mortality risk differences by player position and playing-time BMI for within-NFL cohort comparisons provide some insights into the comparability issue of “healthy worker effect.” Specifically, our findings showed that obesity was associated with a higher risk of all-cause mortality in the general US male population than in the NFL population (irrespective of NFL career length). This suggests that at a comparable BMI, a person in the general population is at a higher risk of mortality than an NFL player is. Here, the “healthy worker effect” bias is a function of the fact that only healthy and physically fit men self-select or choose to draft for the NFL; moreover, healthier players are less likely to have short NFL careers. The impact of this bias is exacerbated in the studies by Baron et al, 3 Lehman et al, 16 and Lincoln et al 19 in which player inclusion is based on the number of seasons played. To address this issue, future studies should consider the use of dynamic cohort designs (including the collection of time-varying variables or risk factors) in which players enter the study sample when drafted into the NFL and are evaluated after their NFL careers. This should be augmented with pre-NFL exposure information (eg, high school and college participation in football) for a more complete view of relevant football-related etiological risk factors. Consideration of these critical exposure windows will ensure a valid inference about suspected etiological risk factors.
The health benefits associated with higher levels of physical activity and fitness among NFL players versus the general population of US men are irrefutable. 18 However, there are mixed findings for the relationships between training loads, injury risk, fitness, and performance in athlete populations. 13 Studies among rugby players suggest that training and competition stress result in muscle damage, 34 reduced neuromuscular function, 23 impaired immune systems, 10 and anabolic-catabolic homeostasis. 25 Given the similarities in physical activity requirements between rugby and football, these findings lend credence to the hypothesis of premature or accelerated aging due to traumatic body injuries. On the other hand, it is plausible that the injury risk is not increased by training per se but rather excessive and rapid increases in training loads in contact sports. 11 These relationships warrant further examination in football populations in which severe injuries such as concussions and resulting CTE are prevalent. 26
With more valid “control” comparisons (eg, other professional sport players), an elevated underlying and contributory cause-specific (eg, neurodegenerative, cerebrovascular, or musculoskeletal diseases) mortality risk among NFL players is not improbable. A recent examination of repeated head impacts through tackle football before the age of 12 years in 42 players demonstrated that children and adolescents are susceptible to prolonged later-life neurological impairment. 33 These negative effects remain, even after adjusting for differences in NFL career length and highest level of education attained. In fact, despite having shorter NFL careers, players exposed to body and brain trauma at younger ages (<12 years) had significantly lower executive function. 33 NFL exposure probably accelerates the pathophysiological mechanisms toward neurological deficits (observed among NFL players with short careers) as a result of the accumulation of traumatic injury incidents. 8
These early-life exposures may also be correlated with other causes of death such as suicide. This is supported by findings of an elevated suicide risk among National Collegiate Athletic Association (NCAA) football players compared with age- and race/ethnicity-matched male athletes. 30 Rao et al 30 showed that the risk of suicide (linked to mental health problems) was more than 2-fold (relative risk, 2.21 [95% CI, 1.05-4.61]) higher among football players than other athletes. Demonstrably, this finding underlines questions about the validity of evidence based on comparing the mortality risk among NFL players to that of the general population of US men. However, alternative explanations related to the differences between NFL and NCAA football players (eg, age of players and how they respond to stress) should not be ignored.
Additionally, potential confounding by the higher prevalence of known chronic disease risk factors such as tobacco smoking 29 and family history 7,31 in the general population of US men (vs NFL player population) likely functions to underestimate (bias) the mortality risk among NFL players. Future studies need to control for these confounders. NFL reference period/season-related factors, particularly those linked to body and head trauma (eg, number of games played, number of concussions), and their relation to neurodegenerative disease mortality also require more research.
Conclusion
This systematic review represents a comprehensive epidemiological evaluation of the etiological risk factors associated with early mortality among NFL players. Overall, the mortality risk among NFL players appeared to be lower than that in the general population of US men. However, methodological issues associated with all-cause and cause-specific mortality risk factors examined in the existing literature preclude a definitive conclusion of etiological protective or risk effects. Comparison groups less prone to selection bias (“healthy worker effect”) and a life-course evaluation of suspected risk factors are warranted.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported, in part, by funds provided by the David B. Falk College of Sport and Human Dynamics, Syracuse University. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Measures of Association Between Violence/Suicide Mortality and Selected Risk Factors Among Current and Previous NFL Players a
| Risk Factor | Measure of Association | Comparison Group | Summary |
|---|---|---|---|
| Violence | |||
| NFL player | |||
| Lehman et al 16 (2012) | SMR, 0.27 (95% CI, 0.14-0.46) | US men | Violence-related deaths were lower among NFL players versus US men. |
| Lincoln et al 19 (2018) | SMR, 0.38 (95% CI, 0.27-0.52) | US men | |
| Suicide | |||
| NFL player | |||
| Lehman et al 17 (2016) | ≥5 seasons: SMR, 0.47 (95% CI, 0.24-0.82) | US men | Both violence/suicide-related deaths were lower among NFL players versus US men. |
| Position | |||
| Lehman et al 17 (2016) | Nonspeed
b
with ≥5 seasons: SMR, 0.65 (95% CI, 0.24-1.42) |
US men | Compared with US men, the risk of suicide was lower among NFL players irrespective of the position played. The position played was not associated with suicide among NFL players. |
| Speed with ≥5 seasons: SMR, 0.47 (95% CI, 0.14-1.51) | Nonspeed positions | ||
a NFL, National Football League; SMR, standardized mortality ratio; US, United States.
b Nonspeed positions: defensive and offensive linemen (excluded: punters and kickers).
c Speed positions: quarterback, running back, halfback, fullback, wide receiver, tight end, defensive back, safety, and linebacker (excluded: punters and kickers).