
Abstract
Background:
An arthroscopic technique for anatomic glenoid reconstruction has been proposed for the treatment of glenohumeral bone loss in patients with recurrent shoulder instability. This technique is proposed as an alternative to open techniques as well as to the technically challenging arthroscopic Latarjet procedure. In arthroscopic anatomic glenoid reconstruction, a distal tibial allograft is inserted through a novel far medial portal, superior to the subscapularis tendon and lateral to the conjoint tendon.
Purpose:
To evaluate the safety of the far medial arthroscopic portal for anatomic glenoid reconstruction in a cadaveric study.
Study Design:
Descriptive laboratory study.
Methods:
Ten cadaveric shoulder specimens were dissected after inside-out medial arthroscopic portal insertion in the lateral decubitus position for arthroscopic anatomic glenoid reconstruction. A single observer performed 3 measurements on each specimen with a digital caliper (to the nearest 0.1 mm) from the medial portal to neurovascular structures, and the mean (±SD) and the range were calculated. The anthropometric data of the cadaveric specimens were also collected.
Results:
The mean distances between the far medial arthroscopic portal and sensitive anatomic structures were as follows: 50.79 ± 13.69 mm from the musculocutaneous nerve, 46.28 ± 9.64 mm from the axillary nerve, 6.71 ± 8.52 mm from the cephalic vein, and 48.52 ± 7.22 mm from the subclavian artery and vein. The mean size of the medial arthroscopic portal was 25.60 mm. In all cases, the subscapularis muscle was intact.
Conclusion:
The far medial arthroscopic portal for anatomic glenoid reconstruction without a subscapularis split presents a minimal risk to most neurovascular structures during bony reconstruction of the glenoid surface in patients with anterior shoulder instability. The only anatomic structure at risk is the cephalic vein, while the axillary and musculocutaneous nerves are at a safe distance away from the portal, based on previous shoulder arthroscopic portal safety studies in the literature.
Clinical Relevance:
Arthroscopic anatomic glenoid reconstruction using a distal tibial allograft is increasing in popularity for the treatment of anterior shoulder instability with significant bone loss. Being a relatively new technique, the safety of it has yet to be established. This study aimed to demonstrate the safety of a new portal used for arthroscopic anatomic glenoid reconstruction.
Keywords
Several surgical techniques have been employed in the treatment of recurrent shoulder instability, including the open Latarjet procedure, 13 arthroscopic Latarjet procedure, 8 and open anatomic glenoid reconstruction. 11 The arthroscopic Latarjet technique, first introduced by Lafosse and Boyle, 8 uses 4 new portals and requires excision of the capsule and labrum. 9 Although this procedure has been found to have good clinical outcomes, it has not been widely adopted by North American surgeons because of its technical difficulty, high complication rates, and safety concerns related to nearby major neurovascular structures. Several studies have reported complication rates as high as 30%, 5 with neurological injuries in as many as 10% of cases for the arthroscopic Latarjet procedure. 6,14
Open anatomic glenoid reconstruction, first described in 2009, 11 uses a distal tibial allograft to re-create the bony surface of the anterior glenoid. This procedure is already known to yield low recurrence rates, high osseous incorporation, no graft resorption, and excellent clinical results based on a recent systematic review of allograft-based glenoid reconstruction. 12 The advantages of this technique include potential prevention of morbidity after coracoid transfer and nonanatomic placement of the conjoint tendon. Moreover, this procedure ensures restoration of the anatomy of the glenoid as well as a good fit of the graft for defects.
Recently, Wong and Urquhart 14 have developed an all-arthroscopic approach of anatomic glenoid reconstruction that is designed to overcome the technical challenges of the arthroscopic Latarjet procedure 2,8,9 as well as the longer time requirement for open anatomic glenoid reconstruction. 11 In contrast to the arthroscopic Latarjet procedure, arthroscopic anatomic glenoid reconstruction requires only 1 new portal, located medially, to pass the distal tibial allograft to the anterior glenoid. Moreover, arthroscopic anatomic glenoid reconstruction has shown an excellent safety profile with promising radiological outcomes in patients with shoulder instability. 1
The purpose of this investigation was to explore the safety profile of this new portal, with attention being paid to the portal’s proximity to neurovascular structures.
Methods
Ten fresh-frozen cadaveric arms (scapula to fingers) (donated to the Department of Orthopedic Surgery at the Nova Scotia Health Authority for academic purposes) underwent placement of the far medial portal by residents, fellows, and attending surgeons. Shoulders were completely thawed before starting shoulder arthroscopic surgery for the creation of the portals. The mean age of the cadaveric specimens was 58.92 years. This was performed in the context of surgical skills training sessions. None of the participating surgeons had prior experience with this portal but were provided with specific directions as to its placement as well as supervision. Each cadaveric shoulder was secured in a lateral position using a bone clamp.
Technique
The technique for creating the Halifax portal consisted of putting a switching stick in the posterior portal, advancing it anteriorly to be sure that it was parallel to the glenoid face, and going through the rotator interval to be superior to the subscapular tendon. By staying parallel to the glenoid face, the switching stick was always found to be lateral to the conjoint tendon.
The switching stick was then pushed anteriorly through the deltoid muscle fibers until it tented the skin. Then, the skin was incised over the switching stick. 14 The portal was enlarged over the switching stick after it was pushed forward to tent the skin anteriorly. A scalpel was used to open the skin to a size of 2.5 cm to allow for passage of the graft. Two half-pipe cannulas were inserted superior and inferior to the switching stick into the glenohumeral joint, and a wide channel dilator (Latarjet set; DePuy Mitek) was used to bluntly open the portal between the 2 half-pipe cannulas. Further dilation of this portal was performed under the skin by using finger dissection. In all cases, a graft was passed through the portal and secured to the anterior rim of the glenoid, as we would do for anterior capsular reconstruction. A detailed description of the surgical procedure is described elsewhere. 14
Data Collection
After the surgical procedure was completed, each shoulder was dissected to perform measurements of the portal. The portal was identified with methylene blue dye and formed a cylinder-like path through the skin into the joint. The closest edge of this path was used to measure the distance to the neurovascular structure. Digital calipers were used to measure the shortest distance from the portal edge to important neurovascular structures in the arm: the musculocutaneous nerve, axillary nerve, cephalic vein, subclavian artery/vein, and suprascapular nerve. Three measurements were made for each of these structures by a single observer (I.M.), with mean ± SD distances being recorded.
Statistical Analysis
SPSS version 24 software (IBM) was used to perform descriptive statistical analysis (mean, SD, 95% CI).
Results
The mean length of the portal was 25.60 ± 2.88 mm. The mean distance from the portal to various neurovascular structures was as follows: musculocutaneous nerve, 50.79 ± 13.69 mm (Figure 1); axillary nerve, 46.28 ± 9.64 mm (Figure 2); cephalic vein, 6.71 ± 8.52 mm (this was the most at-risk structure, with there being effectively no distance between this structure and the portal [range, 0-23 mm]); and subclavian artery and vein, 48.52 ± 7.22 mm (Table 1). All other neurovascular structures were, on average, more than 40 mm away from the portal. In all cases, the subscapularis and supraspinatus muscles were intact. All the measurements had a normal distribution except the cephalic vein.
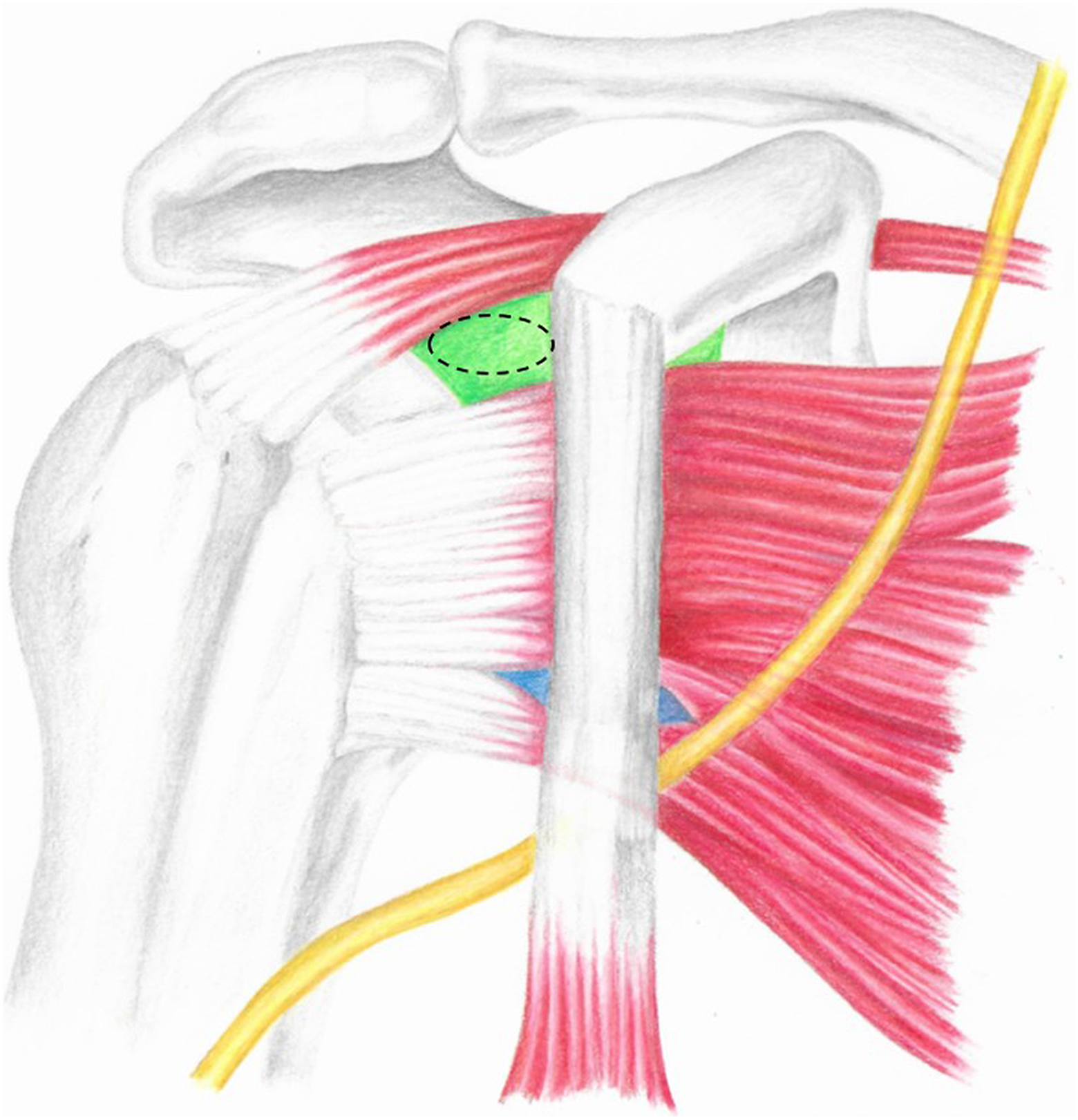
The musculocutaneous nerve (yellow) in relation to conjoint tendon, subscapularis split (blue), and Halifax portal (dotted circular green).

The axillary nerve (yellow) in relation to conjoint tendon, subscapularis split (blue), and Halifax portal (dotted circular green).
Distance Between Neurovascular Structures and the Far Medial Portal a

a The most vulnerable neurovascular structures were the cephalic vein and axillary nerve.
Discussion
The recently described arthroscopic anatomic glenoid reconstruction uses a far medial arthroscopic portal, which avoids most major local neurovascular structures. The cephalic vein was the only neurovascular structure at risk, with a mean distance to the portal of 6.71 ± 8.52 mm (range, 0-23 mm).
The mean distance of the portal to the musculocutaneous nerve, 50.79 ± 13.69 mm, placed the nerve at a safe distance; this is important, as one of the concerns about the safety profile of the arthroscopic Latarjet procedure stems from reports of injuries to this nerve. 2,6 Delaney et al 4 showed through intraoperative neuromonitoring that the musculocutaneous nerve was endangered during the Latarjet procedure, with changes in somatosensory evoked responses or transcranial motor evoked potentials identified during the procedure. Hawi et al 7 performed a cadaveric study in 50 shoulder specimens using a subscapularis muscle split to describe the safety profile of the arthroscopic Latarjet procedure. In all cases, the musculocutaneous nerve was within the edges of the subscapularis split, placing the nerve at risk. In a cadaveric study of the anterior-inferior (5 o’clock) shoulder portal, which is used routinely in arthroscopic suergery, Davidson and Tibone 3 measured the distance between the portal and major neurovascular structures in 14 specimens. They found the average distance of the anterior-inferior portal to the musculocutaneous nerve to be 22.9 ± 4.9 mm. By comparison, the far medial portal reduces the risk to the musculocutaneous nerve.
Axillary nerve injuries are likewise a concern for the Latarjet procedure. The axillary nerve was the most common nerve to have neuromonitoring changes in a study by Delaney et al, 4 with 7 of 34 patients also having clinical deficits postoperatively. In our study, the axillary nerve was the closest nerve to the far medial portal, with a mean distance of 46.28 ± 9.64 mm. By comparison, the anterior-inferior portal was 24.4 ± 5.7 mm from the axillary nerve in the study by Davidson and Tibone. 3 In a 2007 study on 12 shoulder portals, Meyer et al 10 postulated that a mean distance of greater than 20 mm between the portal and nerve minimizes the risk of injuries. Thus, the far medial portal is even safer for the axillary nerve than other portals used in shoulder arthroscopic surgery. However, the current study focused solely on portal placement; there are also potential neurovascular risks associated with graft passage and fixation.
The nearest structure to the portal in this study was the cephalic vein, with a mean distance of 6.71 mm. Similar findings were observed in the study by Davidson and Tibone, 3 which placed the cephalic vein less than 10 mm away from the anterior-inferior portal. Meyer et al 10 found that the cephalic vein was 14 mm and 17 mm away from the anterior-inferior and anterior-central portals, respectively, with 2 direct injuries reported. The senior author (I.W.) of the current study has performed more than 100 surgical procedures using this technique but has never experienced any injury to the cephalic vein. The type of knife used for the skin (No. 11 blade), along with blunt dissection only, will negate the risks of being close to the cephalic vein. The switching stick is blunt as well, so it is unlikely to cause tearing of the vein. Hypothetically however, if there is continuous venous bleeding after the creation of the portal, one could consider that the vein was damaged, which may require pressure to stop it or theoretically the need to ligate it.
Our study used the portal with an inside-out technique, which is reproducible. The switching stick was placed from the posterior cannula, parallel to the glenoid, superior to the subscapularis, and lateral to the conjoint tendon. This allowed us to avoid the neurovascular structures while passing the switching stick through the rotator interval.
The main limitation of this study is the fact that it was performed in cadaveric specimens rather than in vivo. Consequently, our measurements may have been affected by postmortem changes such as rigor mortis and loss of fluid in tissues. Moreover, differences in muscle mass between preserved cadaveric specimens and actual patients may limit the applicability of cadaveric studies to human surgery. Furthermore, measurements were performed by a single observer, without calculating for intrarater reliability.
Conclusion
The far medial arthroscopic portal is safe and minimizes the risk to the most important neurovascular structures in the extremity. The only at-risk structure was the cephalic vein, lying very close to the portal. The tract of this portal represents a technical improvement over previous techniques as it avoids a subscapularis split and possible neurovascular complications. The far medial portal safely allows for minimally invasive bony reconstruction of glenoid deficiencies in patients with recurrent shoulder instability. Further studies are required to examine the adoptability of this technique into routine orthopaedic surgery practice.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
Acknowledgment
The authors acknowledge the help of Swagata Ghosh for conducting statistical analyses, summarizing results, and effecting overall formatting; Ryland Murphy for collecting and managing data; and Jalisa den Hartog for coordinating research and work with the research ethics board.