
Abstract
Background:
While it is believed that good results can be achieved by arthroscopic debridement of partial-thickness tears (PTTs) of <50% tendon thickness, few studies have directly compared the treatment of articular- versus bursal-sided PTTs of <50%.
Purpose:
To compare the postoperative outcomes of patients with articular- versus bursal-sided PTTs of <50% tendon thickness that were treated with arthroscopic debridement and selective acromioplasty (for type II or III acromions).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
An analysis was performed with data from 76 consecutive patients diagnosed with a PTT <50% tendon width (Ellman grade II) who had undergone arthroscopic debridement and selective acromioplasty (for type II or III acromions). Outcome measures included the short version of the Western Ontario Rotator Cuff index, the American Shoulder and Elbow Surgeons score, and the relative Constant-Murley score, as well as strength of the affected shoulder. A statistical paired t test (preoperative vs 2 years postoperative) and an independent t test were utilized to compare outcomes between patients with bursal- and articular-sided tears.
Results:
Between 2001 and 2010, there were 40 (53%) articular- and 36 (47%) bursal-sided tears treated with debridement and selective acromioplasty. The mean patient age was 55 years (range, 36-77 years) for the bursal group and 56 years (range, 33-81 years) for the articular group. The mean follow-up was 24 months (range, 22-26 months). Both groups showed significant improvement in the short version of the Western Ontario Rotator Cuff index, American Shoulder and Elbow Surgeons score, and relative Constant-Murley score 2 years after surgery (P < .0001) as well as in strength (P < .0001 for bursal tears, P = .006 for articular tears). There was no statistically significant difference between groups in any of the postoperative outcome measures at 2 years.
Conclusion:
The results of this study demonstrate that good outcomes can be achieved with arthroscopic debridement and selective acromioplasty among patients with articular- or bursal-sided PTT of <50% tendon thickness. No difference was observed between groups at 2-year follow-up.
Partial-thickness tears (PTTs) of the supraspinatus tendon, whether on the bursal or articular side, are typically managed according to their depth, or the thickness of the tear in relation to the tendon width. 17 Tears of <50% are usually treated with debridement with acromioplasty where indicated, especially in the setting of bursal-sided tears. Tears of >50% are repaired, 26 by transtendinous repairs for articular-sided tears, 15 by in situ repair for bursal-sided tears, 4,27 or by conversion to full-thickness tears followed by repair. 4,6,12,14,16,26
A systematic review by Strauss et al 26 in 2011 identified 7 studies on the treatment of PTTs with debridement without repair. All 7 studies treated tears that were <50% of the tendon’s thickness: 4 routinely used acromioplasty 3,13,17,20 ; 2 used acromioplasty selectively 1,25 ; and Reynolds et al 22 described debridement without acromioplasty when treating articular-sided tears in professional baseball pitchers.
While Strauss et al 26 concluded that good results could be achieved by arthroscopic debridement of PTTs of <50% of tendon thickness, a few studies directly compared the treatment of articular- versus bursal-sided PTTs of <50%, with conflicting results. Two studies suggested that bursal-sided tears treated with debridement may not do as well as articular-sided tears, 3,7 while another study identified superior outcomes for bursal-sided tears. 20
Articular-sided tears are much more common than bursal-sided tears. They occur more often in young people, and are thought to be related to trauma, 20 while bursal-sided tears appear to be related to aging rather than extrinsic impingement. 1,11 Debridement, thought to stimulate a degree of healing, does have some advantages over repair, as the rehabilitation period varies considerably between the treatments. Patients undergoing repair invariably require a period immobilized in a sling and an extended period away from sporting activities, while those patients treated with debridement alone can generally begin active and passive movement immediately. 20
The purpose of this study was to compare the postoperative outcomes of patients with articular- versus bursal-sided PTTs of <50% of the tendon thickness who were treated with arthroscopic debridement and selective acromioplasty (for type II or III acromions). The hypothesis was that there would be no difference in outcomes between patients with articular- and bursal-sided PTTs.
Methods
This study involved a retrospective analysis of prospectively collected data. All patients were ≥18 years of age and had failed identical nonoperative treatment of PTTs of at least 6 months. Nonoperative treatment involved a therapist-supervised protocol of passive and active range of motion exercises and capsular stretching, as well as strengthening of periscapular muscles and the rotator cuff. Approval for use of existing data was obtained from the local institutional research ethics board. Inclusion criteria were existence of an articular- or bursal-sided tear involving <50% of the tendon thickness—confirmed intraoperatively and treated with arthroscopic debridement with or without other decompression surgery (acromioplasty/distal clavicle resection)—and a minimum follow-up of 2 years. Tear depth was assessed with a probe and direct arthroscopic visualization. Exclusion criteria included (1) Ellman grade 1 PTT 5 (<3 mm deep), on the basis that this should be treated with debridement; (2) Ellman grade 3 PTT (>6 mm deep, >50% of the thickness), on the basis that this should be treated with repair; (3) patients with both bursal- and articular-sided tears; (4) patients with full-thickness rotator cuff tears requiring repair; (5) suspected internal impingement (throwing athletes with anterior instability/anterior labral tear and PTT); (6) hyperlaxity (Beighton score >4) and/or patients thought to have anterior instability attributed to capsular laxity; (7) other concomitant major surgery, such as superior labral anterior-posterior (SLAP) repair or biceps tenotomy/tenodesis; and (8) previous surgery on the operative shoulder.
Patient demographics were recorded, including age, sex, history of injury (eg, single traumatic incident inciting shoulder pain), and presence of a work-related claim. Physical examination was used to identify patients with a painful arc, positive impingement signs (Neer impingement sign, Hawkins-Kennedy impingement sign), and clinical evidence of rotator cuff weakness. 18,19 Radiographs were used to assess the degree of acromioclavicular joint osteoarthritis (Zanca view), grade the acromial morphology (supraspinatus outlet view), and exclude glenohumeral osteoarthritis. The diagnosis of PTT was confirmed on preoperative magnetic resonance imaging (MRI; 1.5 T), the majority of which was performed at a single institution. A meta-analysis of studies using 1.5-T MRI to detect PTTs identified 67% sensitivity, 94% specificity, a positive likelihood ratio of 11.2, and a negative likelihood ratio of 0.4. 24 A single senior surgeon (R.H.) evaluated each patient and made the decision to proceed with surgery.
Three outcome measures were completed prior to surgery and 2 years after surgery by a single physical therapist (H.R.) who was blinded to the location of the partial tear: the American Shoulder and Elbow Surgeons (ASES), 23 the relative Constant-Murley score (which adjusts the absolute scores of the Constant-Murley score for age or sex differences 2 ), and the short version of the Western Ontario Rotator Cuff index (Short WORC). 21 Strength was measured in pounds pre- and postoperatively in the scapular plane (arm at 90° elevation and 30° in front on the coronal plane) with a spring-scale dynamometer. 9
Operative Technique
The senior author (R.H.) performed all operations arthroscopically, with the patient in the lateral position and suspended with a traction system (3-Point Distraction System; Arthrex). All partial articular tears were debrided via an anterior rotator interval portal with a 3.5-mm full-radius shaver and then measured with the probe to apply an Ellman grade. The biceps was carefully inspected with a probe inserted from the anterior portal—patients with a SLAP tear were treated with a repair, while patients with tears >50% were treated with tenotomy—and any patient undergoing surgery to address the biceps tendon or its insertion was excluded from this study. The instruments were then introduced into the subacromial space. Acromioplasty was performed only in the presence of a type II or III acromion detected on the supraspinatus outlet radiograph view, and in cases where acromioplasty was performed, the coracoacromial ligament was also released. In the presence of acromioclavicular osteoarthritis diagnosed on radiograph (joint space narrowing, inferior osteophytes seen on the Zanca view) and confirmed intraoperatively, the distal clavicle was excised with an anterior portal. Bursal-sided tears were debrided with a 3.5-mm full-radius shaver and then graded (Figure 1).

(A) Bursal-sided tear of <50% of tendon width, after debridement with shaver. The camera is in the posterior portal of a left shoulder, with a working portal placed laterally under the acromion. (B) Articular-sided tear of <50% before debridement. (C) Articular-sided tear after debridement.
All patients followed a standardized rehabilitation program. Active-assisted exercises started on postoperative day 1, progressing to active and resistive exercises within 3 weeks.
Statistical Analysis
Descriptive statistics (mean ± SD) were calculated. Independent t tests (for normally distributed data) and Wilcoxon 2-sample tests (for nonnormally distributed data) were used to examine group differences in ASES, Constant-Murley score, and strength. Changes between pre- and postoperative outcome measures were examined within groups with paired t tests. Chi-square or Fisher exact tests were used for categorical data as appropriate. Statistical analysis was performed with SAS (v 9.1.3; SAS Institute). Statistical results are reported with 2-tailed P values with significance set at P < .05.
Results
Patient demographics are detailed in Table 1, and a flowchart accounting for all excluded patients is presented in Figure 2. Between 2001 and 2010, 76 patients with PTT of <50% of the supraspinatus tendon width were treated; 36 (47%) patients had bursal-sided tears and 40 (53%) had articular-sided tears. No patient had a partial tear of the subscapularis. The collection period for each group was the same. The mean symptom duration prior to surgery was 47 ± 50 months (range, 6-204 months), while the mean follow-up was 24 months (range, 23-33 months). There was no difference in symptom duration or follow-up between the groups.
Group Differences in Demographic, Clinical, and Surgical Characteristics

a Chi-square or Fisher exact test.

Flowchart demonstrating the original number of patients with partial tears in the database, with details of the number of patients excluded and the reason for exclusion. SLAP, superior labral anterior-posterior.
There were no significant differences between the groups in terms of age, symptom duration, work-related claims, sex, precipitating trauma, or symptoms. A greater percentage of acromioplasties were performed in the bursal tear group (P = .003), with no difference between groups in the rates of distal clavicle resection.
The pre- and postoperative outcome scores for each group are presented in Table 2. Each group demonstrated a statistically significant improvement in ASES, relative Constant-Murley score, Short WORC (P < .0001), and strength (P < .0001 for bursal tears, P = .006 for articular tears). There were no statistically significant differences between the groups with respect to the 4 outcomes pre- or postoperatively.
Pre- and Postoperative Scores a

a ASES, American Shoulder and Elbow Surgeons; RCMS, relative Constant-Murley score; WORC, Western Ontario Rotator Cuff index.
bt tests were performed for normally distributed data, and Wilcoxon 2-sample tests were done for nonnormally distributed data.
c Change over time was statistically significant within each group at P < .0001.
d Change over time was statistically significant at P < .0001 for bursal tears and P = .006 for articular tears.
A power calculation was made with the known mean values for each group, the known standard deviation, and an alpha value of 0.5—the power was calculated at 0.99.
Discussion
The main finding of this study is that good results can be achieved with arthroscopic debridement and selective acromioplasty of articular- and bursal-sided PTTs that are <50% of the tendon width, with no difference in outcome between the groups at 2-year follow-up.
There are few direct comparisons in the literature regarding the outcomes of debridement for articular- versus bursal-sided tears (Table 3). In 2003, Park et al 20 compared the results of arthroscopic decompression and debridement for 13 bursal and 24 articular PTTs of <50%. At 6 months postsurgery, the results were better for patients with bursal-sided tears; these patients also demonstrated faster pain relief and functional recovery as compared with the articular-sided group. At 2 years postsurgery, patients in the bursal group had higher satisfaction rates, but no difference was seen in ASES. Cordasco et al 3 compared articular-sided tears with bursal-sided tears of <50% that were treated with decompression and debridement. At 5-year follow-up, there was a higher rate of failure (L’Insalata score <70) in the bursal-sided group, although the number in this group (n = 14) was much smaller than that in the articular group (n = 63). The results of our study demonstrate that at 2-year follow-up, there was no difference in outcomes after debridement and selective acromioplasty for PTTs of <50% for both bursal- and articular-sided tears. It remains to be seen if there will be a deterioration in outcomes for the bursal-sided tears with further follow-up.
Summary of the Literature on the Treatment of Partial-Thickness Tears of the Supraspinatus Tendon a
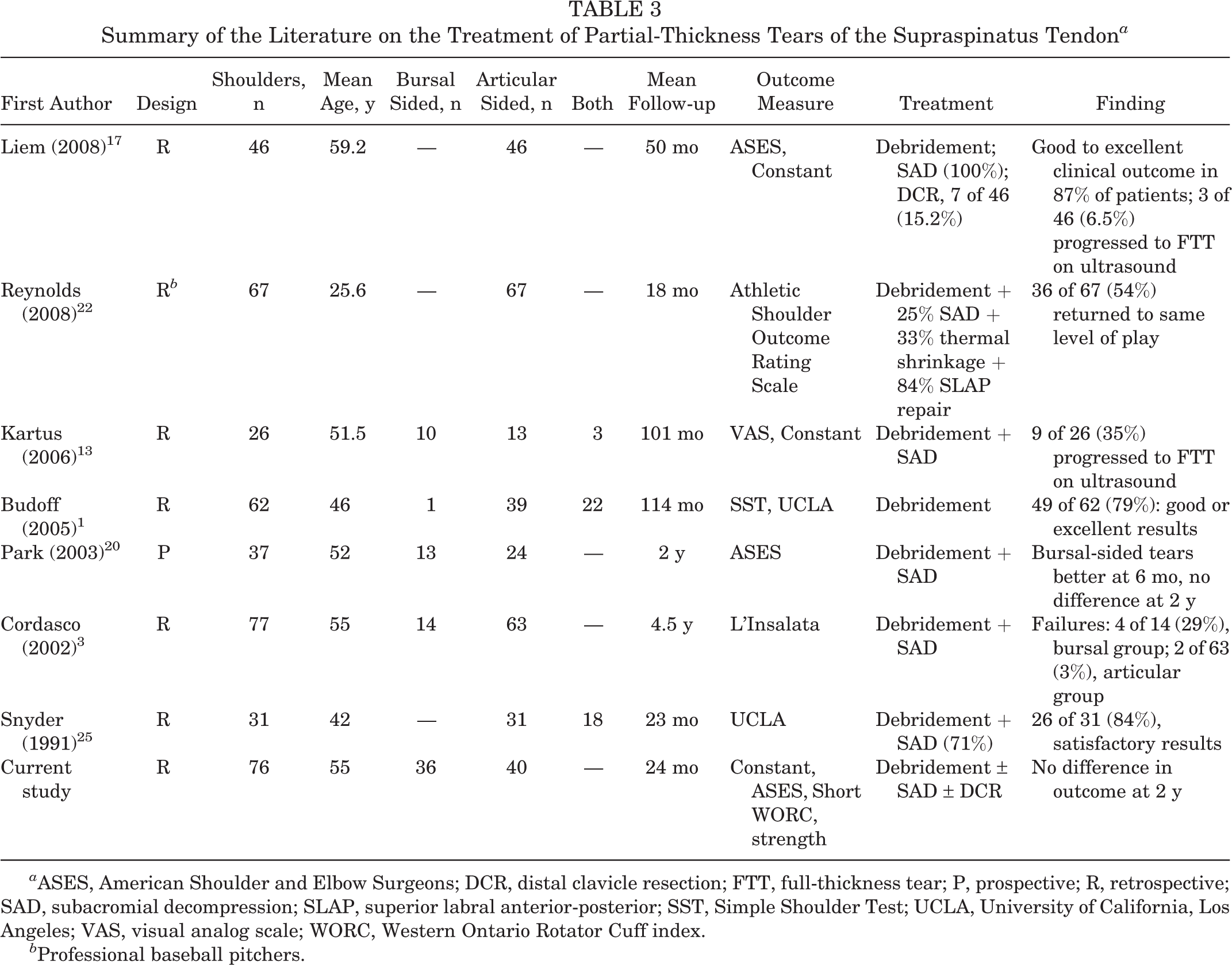
a ASES, American Shoulder and Elbow Surgeons; DCR, distal clavicle resection; FTT, full-thickness tear; P, prospective; R, retrospective; SAD, subacromial decompression; SLAP, superior labral anterior-posterior; SST, Simple Shoulder Test; UCLA, University of California, Los Angeles; VAS, visual analog scale; WORC, Western Ontario Rotator Cuff index.
b Professional baseball pitchers.
Potential causes of PTT include impingement, instability, trauma, and age-related degenerative changes. 8 Articular-sided tears are more common than bursal-sided tears 3,8 and are thought to be more responsive to nonoperative treatment. 7,17 It has been proposed that bursal-sided tears are associated with the aging process, while articular-sided tears are more likely to be encountered in young people after trauma. 10 In our study, no significant difference in mean age was seen between the groups (55 years for bursal sided, 56 years for articular sided), suggesting that articular-sided tears are not only encountered in young people. Certainly, the mean age of patients with articular-sided tears in the literature varies (Table 3). For example, Liem et al 17 studied patients with a mean age of 59.2 years, in contrast with patients in the studies of articular-sided tears by Snyder et al 25 (mean age, 42 years) and Budoff et al 1 (mean age, 46 years). Different again is the study by Reynolds et al 22 (mean age, 25.6 years), although this study examined professional baseball pitchers. The most likely conclusion is that articular-sided tears can be encountered in both younger and older populations.
There is some concern that PTTs will progress over time to full-thickness tears, with possible deterioration in patient outcomes. Liem et al 17 identified good results among patients with articular PPTs of <50% treated with decompression and debridement. In their study, ultrasound follow-up at a mean 50 months demonstrated that only 3 of 46 (6.5%) tears progressed to full thickness. However, Kartus et al, 13 following 26 PTTs of <50% for a minimum of 5 years, identified that 9 of 26 (35%) had a full-thickness tear on ultrasound at final follow-up. This suggests that patients should be counseled that there is a chance of deterioration of good results over time.
Limitations
This study is limited by its retrospective nature, albeit of prospectively collected data. There is also a mix of patients with work-related injuries and a significant difference between the groups with regard to the performance of acromioplasty. The number of patients with PTTs treated successfully with nonoperative treatment was not recorded. Furthermore, we have only 2 years of follow-up—it is possible that some patient outcomes will deteriorate with time, so continued follow-up of this patient group is required. This study did not include MRI or ultrasound findings, so we are unable to comment on the correlation between MRI and intraoperative findings or on the rate of progression to full-thickness tears. Additionally, we did not have a comparison group of patients who had a repair performed of PTTs <50%. Finally, some degree of estimation occurs when the degree of tendon involvement in a PTT is measured, whether it be on the articular side or on the bursal side of the rotator cuff, and while we believe that all tears were Ellman grade II, it is not possible to exclude that a small number may have been grade I or III.
Conclusion
The results of this study demonstrate that good outcomes can be achieved with arthroscopic debridement and selective acromioplasty among patients with articular- or bursal-sided PTTs of <50% of the tendon thickness. No difference was observed between groups at 2-year follow-up.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Sunnybrook Health Sciences Centre Research Ethics Office.