
Abstract
Background:
Clinical characteristics of uncomplicated bone bruises (ie, not associated with a ligament rupture, meniscal tear, or fracture of the knee) in young athletes have scarcely been reported.
Purpose:
To identify mechanisms of injury, characterize bone bruise patterns, and identify clinical factors relating to recovery in young patients suffering uncomplicated bone bruises about the knee.
Study Design:
Case series; Level of evidence, 4.
Methods:
A review of clinical records and magnetic resonance imaging (MRI) findings of patients seen at a single institution was completed.
Results:
We identified 62 children and teenagers (mean age, 13.9 years; range, 8-18 years) who had a total of 101 bone bruises on MRI. The injuries occurred during a variety of organized and recreational sporting activities, the most common being football, basketball, and soccer. The majority (61.4%) of bone bruises occurred as a result of noncontact mechanisms. Patients reported a mean pain scale score of 6.3 of 10 (range, 2-10) on presentation. Frequent clinical findings included non–joint-line tenderness (64.5%), limited range of motion (58.1%), joint-line tenderness (54.8%), and positive meniscal signs (50.0%). The majority of bone bruises (61.4%) were located medially, and the most common bone bruise type was subcortical (58.4%), followed by medullary/reticular (35.6%) and articular impaction (5.9%). The only factor related to time to recovery was mechanism of injury; patients reporting a noncontact mechanism required significantly more time to recover than those reporting a contact mechanism (mean, 99.7 ± 74.8 vs 65.7 ± 38.8 days, respectively; F = 3.753, P = .049).
Conclusion:
In this case series of 62 pediatric patients with non–anterior cruciate ligament (ACL) bone bruises, the majority occurred in the medial compartment, suggesting that these bone bruises result from a mechanism distinct from the pivot-shift mechanism, classically thought to cause ACL injuries.
The use of magnetic resonance imaging (MRI) in the evaluation of childhood knee trauma has created greater awareness of the appearance of bone bruises about the knee. Bone bruises represent fractures of trabecular bone after impact. They are most often seen on MRI of knees that have sustained traumatic ruptures of the anterior cruciate ligament (ACL) or posterior cruciate ligament. 2,5,8,10,11,17,28 –32 They appear as stellate or reticular hypodense lesions on T1-weighted images, or water density lesions on T2-weighted images, often adjacent to the articular surface of the femur and/or tibia. Occasionally, an adjacent cortical fracture is seen. These trabecular fractures are thought to occur at the instant after a ligament rupture when the knee is unstable and the femur and tibia impact each other. 28,29,32
Recently, it has been appreciated that bone bruises may occur as a result of knee injuries that do not cause ruptures of either cruciate ligament, as may occur in athletics during jumping, landing, or pivoting. 2,15,18,27 In a prospective study, Coursey et al 6 described 48 cases of MRI-proven bone bruises in children, with 25% (12/48) of these being uncomplicated, that is, traumatic in origin but not associated with meniscal tears or ligament ruptures. The authors hypothesized that children may be at a greater risk of these uncomplicated bone bruises than adults because of the greater inherent laxity of their ligaments 6 ; however, they presented little clinical data on these cases regarding mechanism, treatment, and healing time. Reports on adults with uncomplicated bone bruises suggest that healing time may vary from 6 weeks to 2 years. 22,35 Other reports suggest that bone bruises may be more common in younger adults than older adults after ACL injuries. 8
We have seen an increasing number of these uncomplicated bone bruises in the knee in young athletes over the past few years. The purpose of this study was to review cases of uncomplicated bone bruises encountered in a pediatric sports medicine practice and extract information regarding mechanisms, physical examination findings, treatment, and time to healing of these injuries.
Methods
This was a prospective review of charts of patients seen at a single clinic who underwent MRI for a knee injury. The study was approved by an institutional review board.
Participants
All patients reported herein presented to Texas Children’s Hospital with a complaint of knee pain after an injury and were examined by 1 of 3 fellowship-trained, board-certified primary care sports medicine physicians (J.E.G., D.D.M., S.D.R.). Patients were included in this study if they (1) were ≤24 years old (the upper age limit for adolescence as defined by the World Health Organization 34 ), (2) presented with a knee injury, and (3) underwent MRI to evaluate their knee injury. Patients were excluded from the study if (1) they were >24 years of age and (2) MRI showed evidence of a physeal fracture, ligament tear, high-grade ligament sprain, meniscal tear, patellar dislocation, or displaced osteochondral fracture. Treatment consisted of partial weightbearing on crutches if patients were limping on presentation; restriction from impact activities (running, jumping, skipping, hopping, dancing, etc) apart from walking; applications of ice; a home exercise program to maintain hip, quadriceps, and hamstring strength and flexibility, with or without dedicated physical therapy with a sports physical therapist; and in some cases, use of a knee sleeve. Patients were asked to return to the clinic at regular intervals until they reported no pain, had normal physical examination results, and were able to walk and jog without pain, at which time their injury was deemed to have resolved.
Data Extraction
The following clinical data were extracted from the charts: age, sex, side of injury (left or right knee), date of initial evaluation, date of injury, mechanism of injury (fall, collision, jump, hyperextension, noncontact), and sport or activity. Patients were asked to rate their level of pain from 0 to 10 using the Faces Pain Scale. 33 Data extracted regarding physical examination findings on initial presentation included height, weight, presence of ecchymosis, swelling or effusion, joint-line tenderness to palpation, other tenderness to palpation, limitation of active or passive motion of more than 10° compared to the uninjured side, positive pain or click in response to meniscal tests (McMurray, bounce home, Apley, Thessaly), and other prominent findings. Data extracted regarding treatment and outcomes included treatment with physical therapy or a knee brace and date of clinical resolution, defined as the follow-up visit at which the patient reported 0 of 10 on the Faces Pain Scale, had normal knee examination results, and demonstrated normal walking and running gait without pain.
MRI Evaluation
MRI of the knee was performed on a 1.5-T or 3-T platform (Philips) using a dedicated knee coil, both of which have been shown to delineate articular lesions in the knee equally well. 16 Multiplanar T1-, proton density–, and T2-weighted images were generated using a standard sports medicine protocol and reviewed by all authors. Findings were verified by a fellowship-trained pediatric musculoskeletal radiologist (J.H.K.). On MRI, bone contusions were defined as decreased signal intensity on T1-weighted images, with corresponding increased signal on fluid-sensitive sequences with or without associated incomplete trabecular disruption, indicative of a concomitant fracture, subchondral cortical depression, or chondral injury. Bone bruises were classified as follows: (1) medullary/reticular (Figure 1), describing abnormal signal primarily with the medullary space of the bone without an interruption of the cortex; (2) articular impaction (Figure 2), describing abnormal signal adjacent to the articular surface with interruption of the cortical line; or (3) subcortical, describing abnormal signal immediately adjacent to the articular surface but without cortical disruption (Figure 3). 14 The location was categorized as medial femoral condyle (MFC), lateral femoral condyle (LFC), medial tibial plateau, or lateral tibial plateau. 6,10,20

Proton density–weighted fat-saturated coronal image of a 15-year-old boy with a medial tibial plateau medullary/reticular bone contusion (arrow).

T2-weighted fat-saturated sagittal image of a 16-year-old girl with a posterolateral tibial plateau articular impaction bone contusion (arrow). There was no cortical undulation and an absence of normal overlying articular cartilage at the site of the bone contusion.

Proton density–weighted fat-saturated coronal image of a 12-year-old boy with a subcortical bone contusion involving the majority of the lateral femoral condyle. Note that the overlying articular surface is preserved, unlike the articular impaction injury pattern (Figure 2).
Statistical Analysis
Data reduction included computing patient age (date of initial evaluation minus date of birth), delay to presentation (date of initial evaluation minus date of injury), and time to resolution (date resolved minus date of initial evaluation) and identifying the mechanism or injury as either contact (fall, collision) or noncontact (jump, hyperextension, other). Patients whose delay to presentation was >2 months were excluded from the calculation of time to resolution. Descriptive statistics were generated for demographic variables, clinical variables, and MRI findings. Analysis of variance was used to determine relationships between time to resolution and clinical factors, including age, sex, mechanism, and treatment.
Results
A total of 62 patients (38 male and 24 female) met the study criteria, with ages ranging from 8 to 18 years (mean age ± SD, 13.9 ± 2.6 years). The age distribution of patients is shown in Figure 4. Approximately 50% of all bone bruises revealed on MRI were associated with a ligament rupture, meniscal tear, or patellar dislocation.

Age distribution of patients with bone bruises.
The right knee was involved in 28 patients (45.2%). Thirty-four patients (54.8%) reported a noncontact injury mechanism (jump, hyperextension, other), while 28 (45.2%) reported a contact mechanism (fall or collision). The mean self-reported pain level at the time of presentation was 6.3 ± 2.1 (range, 2-10). The sports or play activities that they were engaged in at the time of their injury are summarized in Table 1.
Sports Activities Resulting in Bone Bruise Injuries

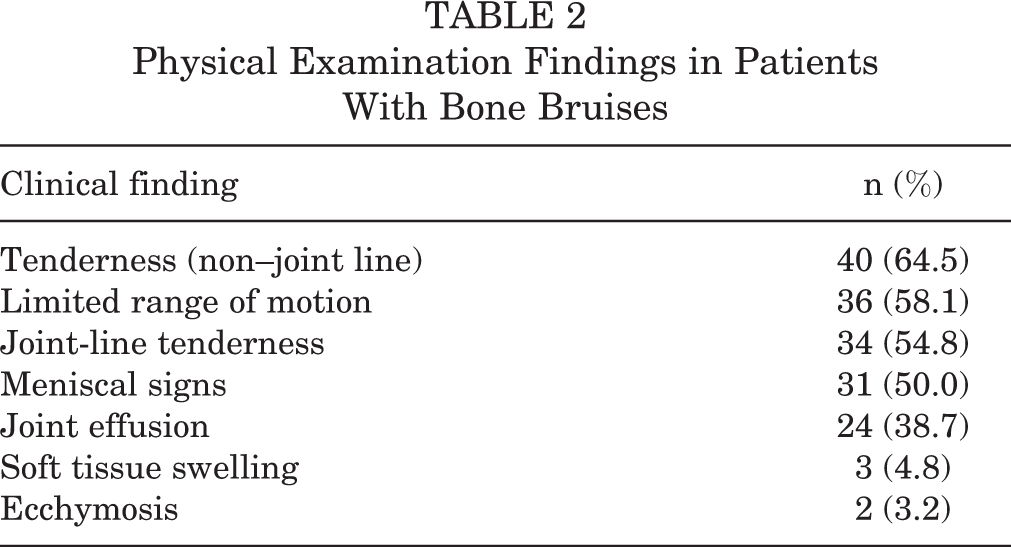
Table 2 summarizes the physical examination findings. Non–joint-line tenderness (eg, patella, condyles, tibial metaphysis) was the most common finding, followed by limited range of motion and joint-line tenderness.
Physical Examination Findings in Patients With Bone Bruises
Findings on MRI are shown in Table 3. The 62 patients had a total of 101 bone bruises identified on MRI. The majority of bone bruises identified occurred in the medial compartment (n = 62, 61.4%). Twenty-eight patients had multiple bone bruises; in 15 patients, the bone bruises occurred on the same side (10 medial, 5 lateral), and in 13 patients, they were found in both the medial and lateral compartments. The most common bone bruise type was subcortical (n = 59, 58.4%), followed by medullary/reticular (n = 36, 35.6%) and articular impaction (n = 6, 5.9%). No patellar bone bruises were encountered that were not associated with patellar dislocations.
Bone Bruises on Magnetic Resonance Imaging by Location

Associations between bone bruise location and mechanism of injury are shown in Table 4. The majority (61.4%) of bone bruises occurred as a result of noncontact mechanisms. The proportion of medial versus lateral bone bruises was not significantly different between contact and noncontact mechanisms (χ2 = 1.247, P = .536).
Bone Bruise Location by Mechanism of Injury a
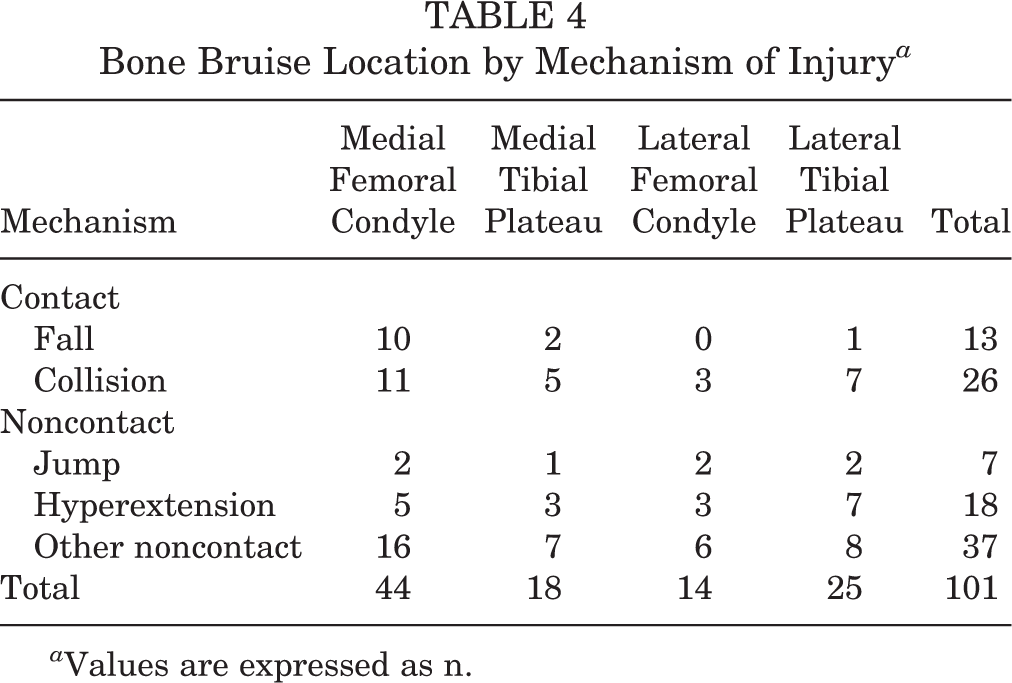
a Values are expressed as n.
The mean time to resolution was 83.7 ± 62.4 days. There were no significant relationships between time to resolution and the pain score at presentation (r = –0.19, P = .921), delay to presentation (r = 0.092, P = .529), body mass index (r = 0.198, P = .198), use of a brace (F = 3.329, P = .074), or formal physical therapy (F = 0.029, P = .865). However, the mean time to the resolution of symptoms was longer for patients with noncontact bone bruises (99.7 ± 74.8 days) than for patients with contact bone bruises (65.7 ± 38.8 days) (F = 3.753, P = .049). Post hoc analysis did not reveal any significant differences between the contact and noncontact groups in age (F = 2.525, P = .184), body mass index (F = 0.807, P = .530), or sex (χ2 = 2.212, P = .137).
Discussion
The majority of the investigations on bone bruises of the knee have concerned adult patients with ACL injuries. In this case series of 62 pediatric patients with non-ACL bone bruises, the majority of bone bruises occurred in the medial compartment, suggesting that these bone bruises result from a mechanism distinct from the pivot-shift mechanism, classically thought to cause ACL injuries.
Bone Bruises in Pediatric Patients
This is the largest case series of uncomplicated bone bruises in pediatric patients yet reported. Coursey et al 6 reviewed the cases of 48 pediatric patients aged 8 to 16 years (mean age, 13.6 years) who underwent MRI for various suspected knee injuries; 12 of these patients had uncomplicated bone bruises. Snearly et al 27 reported on 5 patients with uncomplicated bone bruises revealed by MRI among 53 adolescents (mean age, 15.6 years) referred for knee trauma, while Lee et al 13 reported on 21 pediatric patients with uncomplicated bone bruises among 43 patients (aged 5-16 years) who underwent both MRI and arthroscopic surgery for possible internal derangement.
Our finding that the majority (61.4%) of these uncomplicated bone bruises occurred in the medial compartment is consistent with the report of Lee et al, 13 in which only 3 of 21 patients had uncomplicated bone bruises in the lateral compartment. In contrast, 44% of the bone bruises reported by Coursey et al 6 occurred in the medial compartment. All 5 patients with uncomplicated bone bruises reported by Snearly et al 27 had bone contusions classically seen with an ACL rupture (LFC, posterolateral tibial plateau). Those authors concluded that patients with bone bruises but with intact ACLs most likely, because of their young age, had sufficient ligamentous laxity to allow a pivot-shift event without causing ligament failure.
In contrast to previous reports that provided very little clinical data on uncomplicated bone bruises in pediatric patients, our study provides information regarding mechanisms of injury, the sport or activity that the patient was involved in when the injury occurred, and time to clinical recovery of uncomplicated bone bruises. Coursey et al 6 reported that 2 of their 48 patients suffered a “football injury”; they did not provide any other information regarding the mechanism of injury and no information regarding physical examination findings. Snearly et al 27 reported that all 5 of their patients with uncomplicated bone bruises suffered a twisting injury of the knee: 1 during rugby, 2 during basketball, 1 during football, and 1 patient whose activity at the time of injury was not mentioned. Two of these 5 patients were reported to have effusion and joint-line tenderness. The presence or absence of effusion or tenderness was not mentioned in 3 patients. None of the 5 patients had clinical instability. Lee et al 13 did not report any information regarding the injury mechanism, physical examination findings, or clinical course of their 21 patients with uncomplicated bone bruises. No data on the clinical course was reported by Coursey et al 6 or Lee et al 13 on their pediatric patients with uncomplicated bone bruises, whereas Snearly et al 27 reported that 4 of their 5 patients recovered uneventfully with conservative treatment.
We did not see any uncomplicated bone bruises in patients older than 18 years. We could conjecture that this reflects some maturational phenomenon in the development of knee stability. However, the more likely explanation is that in our pediatric sports medicine clinic, we see few patients older than 18 years, and most of those patients are not involved in organized sports.
Mechanism of Injury
In an ACL rupture, bone bruises are typically seen in the LFC and posterolateral tibial plateau as a result of the pivot-shift mechanism, a combination of knee valgus and either internal femoral rotation or external tibial rotation. § Medial bone bruises are thought to occur by mechanisms distinct from the classic pivot-shift mechanism and have been seen more commonly with injuries to the medial collateral ligament (MCL), medial meniscus, and posterolateral corner (PLC). 2,25
Sanders et al 24 and Quatman et al 21 described discrete mechanisms and the typical bone bruise patterns associated with these mechanisms: pivot shift and bone bruises of the LFC and lateral tibial plateau, hyperextension combined with valgus (lateral bone bruises) or varus (medial), dashboard injuries (anterior tibia), clip injuries involving pure valgus in the lateral compartment and sometimes the MFC when there is an avulsion injury of the MCL, and patellar dislocations (LFC and medial patellar bone bruises). Of these, only the mechanism combining hyperextension and varus adequately explains bone bruises in the medial compartment. Patients with ACL ruptures reported by Viskontas et al 32 were more likely to have medial compartment bone bruises if their injury occurred by a noncontact mechanism versus contact. The authors surmised, based on the more anterior position of bone bruises in the LFC compared to the MFC, that the noncontact mechanism involved combined anterior translation and internal rotation of the tibia. Miller et al 18 found that bone bruises associated with MCL injuries occurred predominantly in the lateral compartment, presumably as a result of direct impaction. In contrast, Atkinson et al 2 and Schweitzer et al 25 found that MCL injuries were associated predominantly with bone bruises of the MFC. Schweitzer et al 25 suggested that medial bone bruises may represent microavulsions associated with tugging of the MCL.
The majority of medullary/reticular lesions in the current study were not adjacent to collateral ligament attachments, with the exception of several seen in the medial tibia. However, this is the less common location for avulsions of the MCL. Furthermore, this series did not include cases involving significant ligament injuries. Geeslin and LaPrade 9 found that bone bruises of the anteromedial femoral condyle were found most commonly with PLC injuries, and posteromedial femoral condyle and posteromedial tibial plateau bone bruises with combined PLC and ACL injuries, injuries that presumably involve a combination of hyperextension and varus angulation.
As none of the patients in this series experienced ligament ruptures, and only a subset reported a hyperextension injury, some of the medial compartment noncontact bone bruises likely resulted from some other mechanism, possibly involving valgus angulation and tibial-femoral rotation. Joint laxity may result in “opening” of the joint, that is, distraction of the femur and tibia, without a ligament rupture. These distraction episodes may include a combination of both torsion and translation and may result in bone bruising by 1 of 2 mechanisms. In 1 mechanism, the joint opens on 1 side, causing impact on the opposite side. In the other mechanism, after joint opening, the articular surfaces on the side of the opening approximate rapidly, with the resulting impact causing bruising. In addition, axial loads on the minimally flexed knee could result in a bone bruise because of a lack of muscular support in the developing adolescent. Which mechanism results in bruising may depend on the pattern of muscle recruitment responding to the joint distraction or the location of the center of mass in relation to the joint. While we have no data to establish either of these mechanisms in the patients reported here, the mechanisms seem plausible based on observations from previous studies. 21,24
Contact Versus Noncontact
Viskontas et al 32 found that bone bruises in adults undergoing ACL reconstruction tended to be more frequent, deeper, and more intense in patients reporting noncontact versus contact mechanisms, suggesting that noncontact knee injuries, on average, may involve greater mechanical energy than contact mechanisms. They also found that noncontact mechanisms were associated more often with medial compartment bruising, consistent with our findings. A noncontact ACL injury mechanism was shown by Kim et al 12 to involve a smaller knee flexion angle and greater internal tibial rotation than contact injuries, theoretically increasing the axial load on the tibia and femoral condyles at the moment of injury. Thus, a noncontact mechanism might result in more extensive bone bruising, resulting in longer recovery times. On the other hand, studies have shown poor correlation between the extent of bone bruising and the presence of associated ligament injuries, contradicting the idea that more extensive bruising is associated with higher kinetic energy. 7,17 The significance of longer healing times in our patients who reported noncontact bone bruises is not clear. As suggested by previous studies, the noncontact injuries could result in more extensive bruising. Another possibility is that the lack of functional stability, which may have led to a noncontact injury, may also have allowed abnormal forces across the knee joint during recovery, impeding the healing process.
Pain
The supposition that bone bruises can be a cause for pain in the patient with an acute knee injury has been previously investigated in adults but not in children or teenagers. The assumption that bone bruises associated with acute knee trauma significantly contribute to a patient’s pain is controversial. Boks et al 3 determined that bone bruising was not a significant contributor to pain in adult patients with knee trauma. However, the average age of patients with bone bruises in that study was 43 years, and many participants had associated injuries as well (meniscal tears, ligament damage, etc). Dunn et al 8 found that the presence of bone bruises did not significantly increase pain scores in patients at the time of ACL reconstruction. In contrast, Johnson et al 11 found that, compared with patients without bone bruising, those who had bone bruises with a concomitant ACL tear tended to take longer to achieve better range of motion, pain control, and neuromuscular control before their reconstructive surgery. Speer et al 28 felt that the posterolateral joint pain experienced by the majority of 54 patients with either an ACL rupture alone or also a sprain of the posterolateral ligament complex was caused by associated bone bruising of the LFC. Five of 36 patients with acute knee hemarthrosis reported by Ariyoshi et al 1 had bone contusions but no other intra-articular abnormalities, and all had medial compartment bone bruises. Within 13 weeks, all 5 of these patients had normal MRI results corresponding with the resolution of their knee pain. Quelard et al 22 also showed that patients with bone bruises along with an ACL tear had a more difficult time achieving normal range of motion postoperatively than those without bone bruises. Davies et al 7 evaluated 30 patients with acute knee trauma who underwent re-imaging after 12 to 14 weeks and found that all but one continued to report pain at follow-up, the exception being a patient with an uncomplicated bone bruise. The patients in our case series did not have other significant abnormalities to account for their pain. We assumed, and have concluded, that their pain and disability were directly related to the presence of bone bruising.
Time to Resolution
Most case series in adults discuss time to resolution in relation to normalization of knee imaging. ∥ In various studies, the resolution of bone bruises ranged from 2 months to 2 years, with the majority of these studies predominated by patients with acute ACL tears. Risk factors for prolonged resolution may include the presence an ACL tear and the presence of an osteochondral fracture. 18,30 All of the studies cited herein that report the progress to resolution at follow-up utilized repeat MRI for re-evaluations. We did not perform re-imaging on any of our patients, believing the bone bruises to be self-limited, and chose to follow progress toward healing clinically. Time to resolution of the bone bruises in our patients (mean, 83.7 days) was based on clinical findings and was calculated as the time from initial presentation (initiation of treatment) to the resolution of symptoms and return to normal knee function. The mean time to clinical resolution for these pediatric patients was similar to that reported by Wright et al 35 in 23 adults (average age, 25.6 years) with uncomplicated bone bruises, whose return to previous levels of activity occurred in an average of 3.0 to 3.4 months depending on the type of bone bruising. These are long healing times compared to other self-limited injuries.
Treatment
Treatment for uncomplicated bone bruises in other studies has consisted of rest, immobilization, partial or nonweightbearing, and physical therapy. 6,7,18,35 Miller et al 18 suggested that prolonged nonweightbearing be prescribed for patients with bone bruises associated with MCL injuries. Davies et al 7 had their patients with acute knee injuries begin physical therapy immediately and allowed them to participate in activity as long as they had no pain. We believe our treatment approach for these uncomplicated bone bruises based on level of pain and functionality to be straightforward and reasonable.
Limitations
While this is the largest series of uncomplicated knee bone bruises in young patients yet reported, the relatively small sample size limited our ability to perform subgroup analyses with sufficient power to detect meaningful results. Another shortcoming of this study is the lack of a standardized knee assessment. Furthermore, we did not perform any assessments, such as arthrometry or an assessment of general joint hypermobility, which may have distinguished patients with increased knee laxity. We did not perform an assessment of knee dynamic stability or strength; lack of dynamic stability may predispose to noncontact injuries. This case series is limited because of all the patients being from a single institution, and therefore, the results may not be generalizable to other populations. Because of the nature of our study, we were not able to determine any causality regarding the noncontact mechanisms and the longer recovery of noncontact bone bruises. We also did not account for any differences in physical therapy treatment or factors that might have influenced the decision on the part of the family to undergo physical therapy, and therefore we are unable to conclude more definitively that undergoing physical therapy had no effect on outcomes.
Future research should utilize a standardized patient assessment, such as the pediatric version of the International Knee Documentation Committee (IKDC) form, as well as evaluations such as arthrometry, kinematic analysis, and strength testing that may implicate knee laxity or lack of dynamic knee stability or strength in the injury mechanisms. Research is also warranted on various treatment options, such as early versus delayed weightbearing, bracing, and physical therapy to try to shorten otherwise long healing times.
Conclusion
Bone bruising about the knee may occur in child and adolescent patients without significant ligament injuries. The majority of uncomplicated bone bruises in this series occurred in the medial compartment. These uncomplicated bone bruises may occur as a result of contact and noncontact mechanisms and may result in weeks to months of disability, with bone bruises resulting from noncontact mechanisms in this case series requiring significantly longer healing times.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Institutional Review Board for Baylor College of Medicine and Affiliated Hospitals.