
Abstract
Background:
Bone–patellar tendon–bone (BPTB) autograft size may be one modifiable predictor of anterior cruciate ligament (ACL) reconstruction postoperative success, as smaller graft diameter has been associated with higher rates of rupture requiring revision. However, measuring the true intra-articular tendinous graft diameter of the soft tissue portion of a BPTB graft with standard intraoperative methods is difficult while keeping the graft intact.
Purpose/Hypothesis:
The purpose of the study was to use 3-dimensional magnetic resonance imaging (MRI) measurements to determine the cross-sectional area of the soft tissue, tendinous portion of a standard BPTB autograft with 10-mm diameter bone plugs, and, by calculation, the collagen graft size (ie, graft diameter), as would typically be reported in ACL reconstruction studies that consider soft tissue graft size. It was hypothesized that the calculated collagen graft diameter of 10-mm BPTB autografts would be significantly smaller than 10 mm.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 100 patients (10 girls and 10 boys at each age from 13 to 17 years) who underwent a knee MRI at a single academic orthopaedic center without documented extensor mechanism pathology were identified. The central 10-mm width of the patellar tendon that would be harvested for BPTB autograft was measured. The region of interest area tool was then used to measure the cross-sectional area of a 10-mm BPTB graft with subsequent soft tissue autograft diameter calculation.
Results:
The mean calculated tendinous graft diameter of a 10 mm–wide BPTB graft was 6.3 ± 0.5 mm and was significantly smaller than a 10-mm reference (P≤ .001). There was no significant association between age and cross-sectional area or graft diameter.
Conclusion:
Modern 3-dimensional imaging-based measurement techniques demonstrated that the true intra-articular tendinous soft tissue portion of 10-mm BPTB autografts shows substantial variation and is significantly smaller in diameter than the tunnels typically reamed to accommodate the bone plug portions of these grafts. Moreover, as graft size is a predictor of rupture rate, preoperative MRI-based evaluation may be an important tool when considering BPTB autograft for ACL reconstruction. Future comparative clinical research utilizing graft size as a study variable should consider quantifying and utilizing the diameter of the soft tissue component of BPTB autografts.
Anterior cruciate ligament (ACL) injuries are a devastating injury for pediatric and adolescent athletes and have been steadily increasing in incidence. 9 Graft choice for ACL reconstruction is dependent on a number of different factors in this demographic. However, in adolescents with minimal growth remaining around the knee, who have closing or closed distal femoral and proximal tibial physes, bone–patellar tendon–bone (BPTB) autograft has demonstrated higher rates of return to sport and lower rates of revision when compared with hamstring tendon autograft.11,18,21,24 Additionally, with the recent popularity of the use of quadriceps tendon autograft, 7 surgeons now have 3 viable graft options for these patients.
In part because of their high activity level, young athletes are at greater risk of ACL graft injury when compared with older patients.32,33 In addition to graft choice, ACL graft size may be one modifiable predictor of postoperative success, as smaller graft diameter has been associated with greater rates of rupture requiring revision, at least when hamstring tendon autograft is utilized.16,27,28 However, measuring the true intra-articular tendinous graft diameter of the soft tissue portion of a BPTB graft with standard intraoperative methods is difficult given that cylindrical sizing tubes must pass over bone plugs with eccentric collagen, which are consistently larger than the central soft tissue region in the anteroposterior direction (thickness) despite a width that is designed to approximate the width of the bone plug itself. While previous research has tried to circumvent this limitation by approximating collagen diameter by measuring circumferential suture around the harvested collagen 17 or use ultrasound or magnetic resonance imaging (MRI) to measure tendon thickness, # no study to the authors’ knowledge has measured the 3-dimensional collagen volume using MRI, nor has any study assessed the influence of age or sex on the graft diameter or volume. By accurately calculating collagen volume of the soft tissue portion of a standard 10-mm harvested BPTB graft, surgeons can better understand the true collagen graft diameter and place this into context with other graft choices.
Therefore, the primary purpose of this study was to use 3-dimensional MRI measurements to determine the cross-sectional area of the soft tissue portion of a standard 10 mm–wide BPTB autograft and, by calculation, determine the collagen graft size (ie, graft diameter), as would typically be reported in ACL reconstruction studies that consider graft size. Secondarily, the study sought to investigate potential associations between collagen graft size and age or sex. We hypothesized that the calculated collagen graft diameter of 10-mm BPTB autografts would be significantly smaller than 10 mm.
Methods
After institutional review board approval (Hospital for Special Surgery IRB No. 2022-1725), 100 patients (10 girls and 10 boys at each age from 13 to 17 years) who underwent a knee MRI at a single academic orthopaedic center between January 1, 2014, and January 31, 2022, without documented extensor mechanism pathology were identified. Patients were excluded for conditions that could affect the extensor mechanism, if there was a history of Osgood-Schlatter disease or Sinding-Larsen-Johansson syndrome, previous knee surgery, or if scans were not performed with the knee in the standard 30° of flexion (± 5°).
The measurement methodology was developed by a board-certified musculoskeletal radiologist (H.G.G.). As the central third of the patellar tendon is typically harvested in ACL reconstruction using BPTB autograft,2,14,23 the central 10 mm of the tendon was measured on the axial plane image at the midpoint of the length of the tendon between the tibial tubercle and apex of the patella using the multiplanar reformation mode. The region of interest area tool was then used to measure the cross-sectional area of a 10-mm BPTB graft (Figure 1). The autograft diameter (cylindrical in shape) was calculated by inputting the measured cross-sectional area into a derivation of the equation for the surface area of a circle 5 using the following formula:

where SA is the measured patellar tendon cross-sectional surface area and d is the calculated graft diameter.
The instructions for measurement of SA are as follows:
With a 1 × 2 image screen configuration, display sagittal proton density and axial proton density sequences.
Click on the axial proton density and turn on the multiplanar reformation mode.
3) Zoom into the patellar tendon on the axial plane image (Figure 1B). a) Measure the width of the patellar tendon. b) Divide the tendon width by 2 and subtract 5 for a measurement (x) that will be utilized to measure the distance from the tendon edges to begin measurement for the 10-mm strip of tissue that would be harvested as a 10-mm BPTB graft from the center of the patellar tendon. c) Measure distance x away from each end of the patellar tendon and mark those locations (y). d) Use the region of interest tool and calculate the cross-sectional area of the patellar tendon that is contained within the 10-mm region between 2 points y.

Measurement of patellar tendon cross-sectional area. (A) Sagittal MRI sequence of the knee with vertical (red) and axial oblique (yellow) plane lines drawn with respect to the patellar tendon. (B) Axial view of patellar tendon with measurement overlay.
Statistical Analysis
Statistical analyses were performed by members of the team with advanced formal training in biostatistics and epidemiology (S.A.B. and P.D.F.). After confirming acceptable interrater reliability between study personnel and the radiologist investigator (H.G.G.), 2 independent, blinded examiners (S.A.B. and R.H.J.) measured patellar tendon cross-sectional areas using MRI scans, and the means were then used for all analyses.
Intraclass correlation coefficient (ICC) values (via a 2-way random-effects model for single-measure absolute agreement) were calculated for all measured cross-sectional areas. A threshold coefficient of >0.70 was the threshold for sufficient interrater reliability. 6 Cross-sectional areas as well as calculated graft diameters were compared between sex and age strata using independent-samples t tests and analysis of variance, respectively. Calculated graft diameters were compared with a reference value of 10 mm using a 1-sample t test. A 2-tailed significance threshold of P≤ .05 was used for all comparative statistical tests. The coefficient of variation was calculated as the ratio of the standard deviation to the mean value and was used to compare the relative variance of the graft diameter measured in the current study with those of patellar tendon thickness measurements in the existing literature. SPSS Version 22.0 (IBM Corp) was used for all statistical analyses.
Results
A total of 100 adolescent patients were included in this study, 50 boys and 50 girls (mean age, 15 years) (Table 1). A total of 50 right and 50 left knees were included. The mean height was 169 ± 10 cm, the mean weight was 65 ± 14 kg, and the mean body mass index was 23 ± 4.3 kg/m2. Through use of the Kolmogorov-Smirnov test of normality, sex (P≤ .001), age (P≤ .001), laterality (P≤ .001), weight (P≤ .001), and body mass index (P≤ .001) were found to be not normally distributed; however, height was normally distributed. All patients’ MRI scans showed evidence of closing or closed distal femoral and/or proximal tibial physes (as would be the requirement for a BPTB autograft). The ICC for cross-sectional areas between the 2 examiners was 0.80 (95% CI, 0.71-0.86). The mean measured cross-sectional area was 32 ± 4.9 mm2 (coefficient of variation, 0.15), resulting in a mean calculated graft diameter of 6.3 ± 0.5 mm (coefficient of variation, 0.08) (Figure 2, Table 1). This calculated graft diameter was significantly smaller than a 10-mm reference (P≤ .001). The mean cross-sectional area was significantly greater in boys (34 ± 5.0 mm) than in girls (30 ± 3.7 mm) (P≤ .001). Accordingly, the mean calculated graft diameter was also significantly greater in boys (6.5 ± 0.5 mm) than in girls (6.1 ± 0.4 mm) (P≤ .001). There was no significant association between age and cross-sectional area or graft diameter.
Cohort Characteristics and Graft Diameter a

Data are presented as mean ± SD unless otherwise indicated.
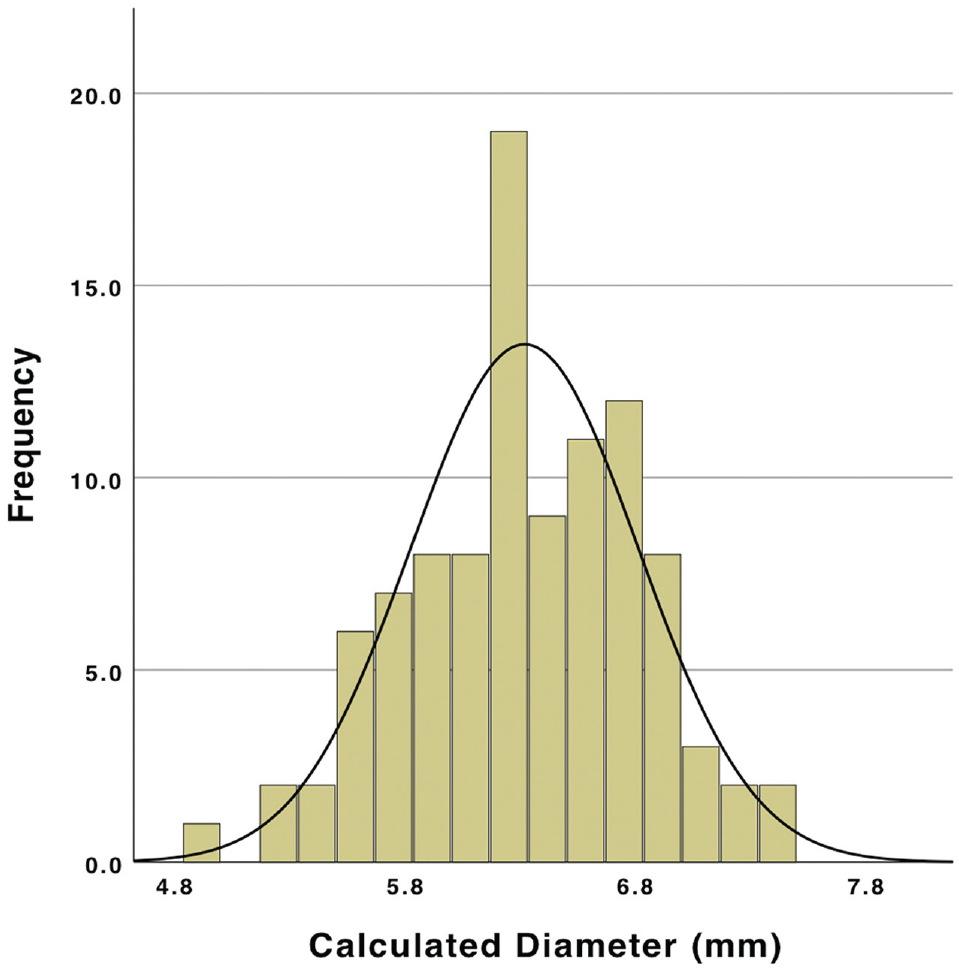
Calculated soft tissue equivalent graft diameter (N = 100). Mean diameter, 6.3 ± 0.5 mm.
Discussion
In the present study, the mean diameter of the soft tissue tendinous component of a 10 mm–wide BPTB autograft was calculated to be 6.3 mm. The collagen graft size values were significantly smaller than the width of the bone block, ranging from 5.0 to 7.4 mm with a standard deviation of 0.5 mm. Variation in the graft diameters indicates that not all size 10 BPTB autografts contain similar amounts of collagen to serve as replacement intra-articular ligament tissue. Previous studies have demonstrated strong associations between graft size and the rate of postsurgical ACL graft rupture, with each 0.5-mm increment decrease associated with a significantly greater likelihood of revision surgery.27,28 Notably, however, these studies involve hamstring tendon grafts, which have different biomechanical properties than patellar tendon grafts. As the results reported in the current study demonstrate a measured standard deviation of 0.5 mm in diameter, this suggests that, although a numerically low variation, there may be a clinically significant variation in the risk of postoperative graft injury among seemingly similar 10 mm–wide BPTB autografts. Furthermore, based on a reliable novel method of MRI-based diameter measurement, the large majority of measured autografts were found to be <7 mm in diameter and therefore approximately 37% smaller than other 10-mm all-collagen grafts, such as quadriceps tendon and most hamstring tendon autografts (typically 7.7-8.5 mm) utilized in ACL reconstruction surgery today.16,27,29 The soft tissue portions of BPTB autografts are, however, similar in size to the native pediatric ACL, which ranges from 4 to 6 mm. 3 Despite excellent reported clinical outcomes and low rates of graft rupture compared with other autografts,11,21 biomechanical analyses of adult and pediatric tissue suggest that the patellar tendon demonstrates weaker mechanical properties than hamstring tendons as measured by ultimate stress, ultimate strain, and the Young modulus.25,26 Therefore, in light of favorable overall retear rates relative to other graft options, these data suggest the advantages of the BPTB construct may stem from graft features such as postoperative graft maturation or variations in the resistance to rupture of a flat versus cylindrical graft or features other than the actual collagenous intra-articular segment, such as minimal creep, immediate relative rigidity, and preservation of the critical dynamic knee flexors/stabilizers.
One strength of the current study was the use of 3-dimensional MRI modalities to model collagen graft diameter equivalent of BPTB without attempting measurement techniques that might risk damaging tissue harvested for ACL grafts. The current literature is limited by measuring only patellar tendon thickness using ultrasound or MRI, typically for comparison between controls and those with pathology (eg, patellar tendinopathy). While these studies have validated methods for measuring patellar tendon thickness, variance in patellar tendon graft size, including the influence of age and sex, has not been well studied. ** Only 1 of these studies measured cross-sectional dimensions of the patellar tendon along 2 axes. 31 It is critical to ascertain from these studies the degree of variation in tendon size presented. As the measurement protocol of this study differed from that of the existing literature, focusing on diameter rather than thickness, by comparing coefficients of variation, an individual may compare the degree of relative variation rather than absolute standard deviation values. Nishida et al 20 validated an objective measure of MRI-based patellar tendon thickness with results demonstrating a coefficient of variation of 0.17. Strada et al 29 also demonstrated an MRI-based measurement technique of patellar tendon thickness and width at the midsubstance, along with the posterior cruciate ligament, and correlated these measurements with those of the ACL to determine which elements are predictive of ACL size. They demonstrated a coefficient of variation of 0.13 for patellar tendon thickness as well as a positive correlation between patellar tendon thickness and ACL thickness at the midsubstance. 29 Importantly, neither study measured cross-sectional area or collagen graft diameter, which would make it comparable to all soft tissue grafts. Nonetheless, the results presented in this study demonstrate a similar degree of variance of measured cross-sectional area with a reported coefficient of variation of 0.16. Furthermore, the results align with those of other researchers reporting a greater thickness of patellar tendon in males than females. 4 This difference, however, is <0.5 mm and therefore unlikely to be clinically relevant or measurable intraoperatively.
Limitations
Some important limitations of the study must be noted. First, the methodology used for measuring the patellar tendon cross-sectional area has not undergone rigorous validation. Rather, the measurement technique was developed through collaborative statistical and anatomic analysis with a fellowship-trained musculoskeletal radiologist, with its validity further supported using interrater reliability. Further validation could be considered to improve the reliability of the results of this study, although the purpose of the current study was not to create a clinical measurement to be applied to patient decision-making but rather to quantify the collagen graft size to allow for comparisons between BPTB autograft tendon and other soft tissue graft options. Additionally, the patients comprising the study group did not have ACL tears and therefore may not be exactly representative of a cohort of patients with an ACL injury. However, the patient population was purposefully curated to better represent patients who would be candidates for BPTB autografts, namely, boys and girls with closing and/or closed distal femoral and proximal tibial growth plates. Last, the BPTB autograft diameter is unable to be directly measured, unlike all soft tissue grafts, which are measured intraoperatively for each patient. Nonetheless, important conclusions can be drawn from this study.
Conclusion
Modern imaging-based measurement techniques demonstrated that the true intra-articular tendinous soft tissue portion of 10-mm BPTB autografts shows substantial variation. Accounting for this is critical in both clinical and research settings. Clinically, as graft size is a strong predictor of rupture rate, the predictability and quantification of graft size are imperative. Thus, preoperative MRI-based evaluation may be an important tool when considering BPTB autograft for ACL reconstruction. Moreover, future comparative clinical research using graft size as a study variable should consider quantifying and utilizing the diameter of the soft tissue component of BPTB autografts, as a 10-mm BPTB cannot be considered equal to a 10-mm all-collagen autograft, nor to another 10-mm BPTB autograft.
Footnotes
Final revision submitted January 16, 2024; accepted February 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.W.G. has received royalties from Arthrex and OrthoPediatrics Canada ULC; nonconsulting fees from Synthes GmbH and Arthrex; consulting fees from OrthoPediatrics; and education payments from Terumo BCT. B.E.H. has received education payments from Kairos Surgical, Pylant Medical, and Arthrex and nonconsulting fees from Arthrex. P.D.F. has received consulting fees from WishBone Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital for Special Surgery (ref No. 2022-1725).