
Abstract
Background:
Estimating skeletal maturity is crucial for treating pediatric knee conditions. Recently, a knee bone age atlas based on the magnetic resonance imaging (MRI) data of pediatric and adolescent population in Southern California (the San Diego atlas) was published. However, its accuracy in other populations has not been verified.
Purpose:
To (1) validate the San Diego atlas in a South Korean pediatric and adolescent population and (2) create and validate a shorthand knee MRI atlas for bone age estimation tailored to South Korean pediatric and adolescent population (the Korean shorthand atlas).
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
We retrospectively analyzed the data of 695 participants aged ≤18 years with normal knee MRI findings between 2000 and 2019. To create the Korean shorthand atlas, age-specific features based on the San Diego atlas that appeared on the evaluated MRI scans (n = 417) were modified to reduce the standard deviation of age. In a separate data set (n = 278), the accuracy of both the San Diego and the Korean shorthand atlases was validated by comparing the knee bone age with the chronological age and determining the correlation between bone age and chronological age.
Results:
In the overall study population, the mean bone age based on the San Diego atlas did not differ from the mean chronological age, and a very strong correlation was observed between them (rS = 0.95). However, the mean bone age based on the San Diego atlas significantly differed from the mean chronological age in female participants aged 7 to 12.9 years (0.6 years younger; P = .003) and in male participants aged 14.0 to 18.0 years (0.4 years older; P = .045). The mean bone age assessed based on the Korean shorthand atlas did not significantly differ from the mean chronological age in any age or sex subgroup and was also very strongly correlated with the mean chronological age (rS = 0.94) in the overall population.
Conclusion:
The San Diego atlas was accurate in estimating bone age in Korean pediatric and adolescent population except for certain age ranges. The Korean shorthand atlas was an accurate tool for estimating bone age in the Korean pediatric and adolescent population at any age range.
Estimating skeletal maturity or bone age is essential for determining the appropriate treatment method for pediatric knee conditions, including anterior cruciate ligament (ACL) tears.3,9 The most commonly used methods for bone age estimation are the Greulich and Pyle bone age atlas and the Tanner-Whitehouse staging system.11,29,30,33,34 However, these methods have some limitations, including a steep learning curve, 14 variable reliability,2,5 and reliance on the skeletal maturity of the left hand, 35 which may not accurately reflect that of the injured knee. 1 Furthermore, obtaining additional radiographs of the left hand heightens the radiation burden of pediatric patients and increases the cost and duration of treatment.
To overcome these drawbacks, Pennock et al20,21 recently developed a new bone age assessment method based on knee magnetic resonance imaging (MRI), which is usually performed for the diagnosis of ACL tears or osteochondritis dissecans. They created the San Diego atlas, an MRI-based knee atlas representing standard female participants aged 1 to 17 years and male participants aged 1 to 18 years based on the age-specific features of the femur, tibia, patella, and fibula. Using the features of the San Diego atlas, Politzer et al 23 and Meza et al 18 developed shorthand atlases for bone age estimation that allow for a faster assessment and require less extensive training.
The skeletal maturity of children can vary based on their ethnicity12,19,39 and socioeconomic status,6,25,26 even if they are of the same chronological age. The atlas created by Pennock et al20,21 was based on a cohort from Southern California. Hence, it is important to determine its accuracy for children with different ethnic backgrounds and regions of residence. To the best of our knowledge, no studies have validated this method in any population other than the cohort used to create the atlas.
The purpose of this study was to (1) confirm the accuracy of the San Diego atlas in a cohort of South Korean pediatric and adolescent population and (2) create and validate a shorthand knee MRI atlas tailored to South Korean pediatric and adolescent population (Korean shorthand atlas). We hypothesized that the San Diego atlas would provide an accurate assessment of the South Korean pediatric and adolescent population.
Methods
Study Design and Population
This study was approved by our institutional review board. The requirement for obtaining informed consent was waived due to the retrospective study design. We retrospectively reviewed the clinical and imaging data of male and female participants aged ≤18 years who underwent a knee MRI between January 2000 and December 2019 at a tertiary-care pediatric center (n = 1628). Excluded from the study were participants with imaging findings of tumor (n = 346), trauma (n = 274), infection (n = 109), or previous operation (n = 13). We additionally excluded participants with conditions or treatment history that may affect knee morphology or skeletal maturity (n = 155), such as congenital anomalies or endocrinopathies, and those with MRI scans of inadequate quality for bone age assessment (n = 12). As the number of children aged <2 years was too small to evaluate as a separate age group, they were also excluded (n = 24). Eventually, a total of 695 participants (371 male and 324 female) who met the eligibility criteria were included in the analysis. The mean age of the participants was 11.0 ± 4.2 years (range, 2.0-18.0 years). Each age and sex group included ≥10 participants.
The study participants were randomly divided into 2 groups in a 1:1.5 ratio: 1 for validation of the San Diego and Korean shorthand atlases (validation group; n = 278) and 1 for creation of the Korean shorthand atlas (creation group; n = 417). The mean age was 11.1 ± 4.1 years (range, 2.0-18.0 years) in the validation group and 11.0 ± 4.3 years (range, 2.0-18.0 years) in the creation group, with no significant difference in age between the 2 groups (P = .69). Participants in the validation group were further divided into 3 age groups: 2.0 to 7.9, 8.0 to 13.9, and 14.0 to 18.0 years for male participants, and 2.0 to 6.9, 7.0 to 12.9, and 13.0 to 18.0 years for female participants. The distribution by age and sex in each group is shown in Figure 1.

Distribution of the overall study population by age and sex. Within each age and sex group, participants were randomly allocated into validation and creation groups at a ratio of 1:1.5. M, male; F, female.
MRI Protocol
Knee MRI was performed using a 1.5-T MRI system (Avanto; Siemens Healthcare) and an 8-channel knee coil. Participants were placed in the supine position with their knees placed in full or near-full extension, based on their comfort level. The routine knee MRI protocol included sagittal and axial fat-suppressed proton-density turbo spin-echo (TSE), coronal proton-density TSE, sagittal and oblique coronal T2-weighted TSE, coronal fat-suppressed T2-weighted TSE, and sagittal T1-weighted TSE sequences. All images were obtained at a slice thickness of 3 mm without an interslice gap, and field-of-views were adjusted to the participant's size.
Creation of the Korean Shorthand Knee MRI Atlas
The Korean shorthand atlas for bone age estimation was developed by modifying the age-specific features described in the San Diego atlas.20,21 First, MRI scans in the creation group were analyzed for the presence of features based on the San Diego atlas. Then, the median age and standard deviation were calculated for each feature. For the femur, the features included presence of a secondary ossification center, incomplete epiphyseal ossification, complete epiphyseal ossification, presence of Oreo sign, disappearance of Oreo sign, physeal thinning (height <2 mm), central physeal closure, and complete physeal closure. In the tibia, the features included presence of a secondary ossification center, partial tibial spinal ossification appearing as a bump, complete tibial spinal ossification, anterodistal epiphyseal ossification extension toward the tubercle apophysis, tubercle apophyseal ossification, partially fused tubercle apophysis appearing as a crack, complete tibial tubercle ossification, physeal thinning (height <2 mm), central physeal closure, and complete physeal closure in the tibia. For the patella, the features were classified according to the percentage of ossification (0%, 1%-24%, 25%-49%, 50%-74%, 75%-99%, and 100% ossified). In the fibula, the features included the presence of a secondary ossification center, styloid not ossified, central physeal closure, and complete physeal closure in the fibula. The MRI slices used for bone age estimation were selected according to the instructions of the San Diego atlas.20,21
Next, to improve the accuracy and reduce the standard deviation in age when the features appeared on MRI, several features of the San Diego atlas were modified. Tibial tubercle epiphyseal extension was further categorized from no extension or extension to no extension, extension distal and below the level of physis <2 mm, or extension distal and below the level of physis ≥2 mm. The ossification of the patella was further classified from 6 into 7 stages (0%, 1%-19%, 20%-39%, 40%-59%, 60%-79%, 80%-99% and 100%). The features of Oreo sign in the femur, partially fused tubercle apophysis appearing as a crack in the tibia, and styloid not ossified in the fibula were excluded because their presence was uncertain and could only be identified in a small number of participants in our cohort. Tables 1 and 2 show the ages at which each feature appeared in male and female participants, respectively.
Age of MRI Feature Appearance in Male Participants a

Boldface values indicate medians (50th percentile). Min, minimum; Max, maximum.
Age of MRI Feature Appearance in Female Participants a

Boldface values indicate medians (50th percentile). Min, minimum; Max, maximum; NA, not applicable.
Finally, we excluded the features in Tables 1 and 2 with a standard deviation in age of >1.7 years. The remaining 12 features were selected as the key features for creating the Korean shorthand atlas. Representative images that best demonstrated the corresponding features were selected and arranged in the atlas in the order of their median chronological age (Figure 2). The sequence of the images matches the median chronological ages at which the specific features in Tables 1 and 2 appeared on MRI. Bone age was determined based on the presence of a certain age-specific feature and the absence of a subsequent feature. For example, if an MRI of a boy showed tibial epiphyseal extension toward the tubercle >2 mm but not complete tibial spinal ossification, his bone age was considered 10.5 years.
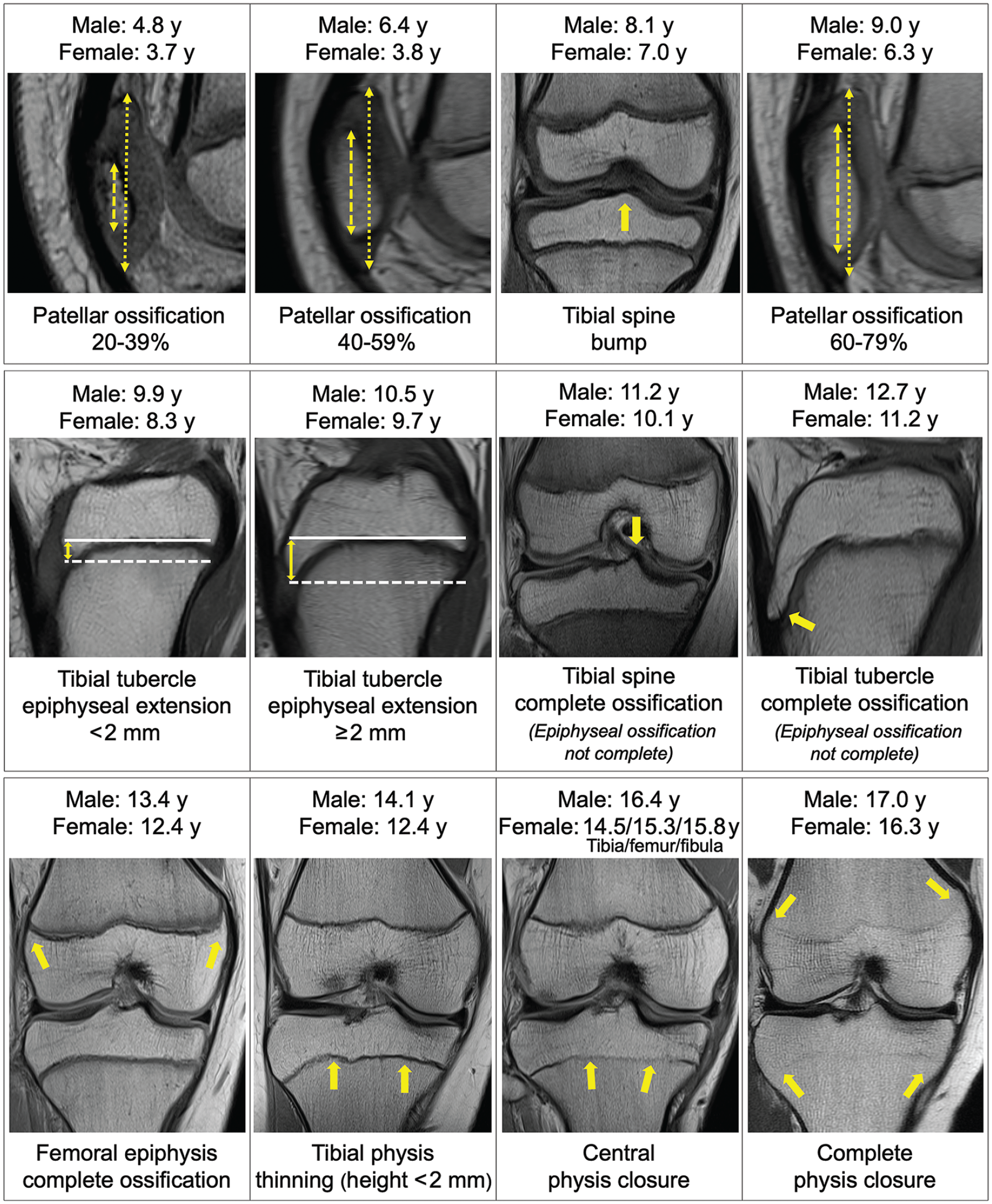
The Korean shorthand knee magnetic resonance imaging (MRI) atlas for bone age estimation. The bone age is determined according to the presence of a certain age-related feature and the absence of a subsequent feature. The percentage of patellar ossification is determined by dividing the length of the ossified portion (double-headed dashed yellow arrow) by the total length of the patella (double-headed dotted yellow arrow). Tibial spinal bump refers to partial ossification of the tibial spine that gives it a rounded, convex shape. The length of the tibial tubercle epiphyseal extension (double-headed solid yellow arrow) is measured from the most proximal point of the tibial physis (solid white line) to the tip of the tibial tubercle epiphysis (dashed white line). Complete ossification of the tibial spine, tibial tubercle, or femoral epiphysis is identified by the absence of the cartilaginous portion of the epiphysis. The single-headed yellow arrows denote the regions of interest within the MRI scans.
Validation of the San Diego and Korean Shorthand Atlases
Pennock et al20,21 showed excellent intra- and interobserver reliability for the San Diego bone age atlas method, with intraclass correlation coefficients (ICCs) of >0.9. To determine intra- and interobserver reliability for the Korean shorthand atlas, 3 reviewers estimated the bone age of 100 participants who were randomly selected from the validation group twice, with an interval of 4 weeks. Reviewer 1 (W.L.) was a board-certified orthopaedic surgeon, reviewer 2 (Y.J.C.) was a pediatric orthopaedic fellowship-trained staff surgeon, and reviewer 3 (S.Y.Y.) was a research coordinator without a medical degree. A brief printed instruction was given to the reviewers to estimate the bone age. Reviewers were blinded to the participants’ chronological age but were provided with participant sex to select an appropriate atlas.
To confirm the accuracy of the San Diego and Korean shorthand atlases, one of the authors (W.L.) estimated the bone age of each participant in the validation group using the 2 atlases. The knee bone age, as estimated based on these atlases, was compared with the participant's chronological age, both in the overall validation group and in each age and sex subgroup. The correlation between bone age and chronological age was also evaluated for each atlas.
In the validation group, 31 participants (13 male and 18 female) aged 7.5 to 15.4 years had available left-hand radiographs obtained within 3 months of the knee MRI. Accurately estimating bone age is crucial in this age range, particularly when deciding on a treatment strategy for pediatric knee conditions.16,22 In this population subset, the hand bone age was compared with the knee bone age as estimated based on the 2 atlases. We also assessed the correlation between the hand bone age and the estimated knee bone ages for each atlas. The Korean standard bone age chart, which is based on radiographs of the left hand and wrist and similar to the Greulich and Pyle bone age atlas, was used to determine the hand bone age. 38 This chart was derived from radiographs of 3407 South Korean children and showed a significant correlation with chronological age and bone ages estimated by the Greulich and Pyle and Tanner-Whitehouse 3 methods. 13
Statistical Analysis
To examine the intra- and interobserver reliability for the Korean shorthand atlas, the ICC for absolute agreement was calculated in a 2-way random-effects single-measures model, where <0.4 indicated poor agreement, 0.4 to 0.59 fair, 0.6 to 0.75 good, and >0.75 excellent agreement.8,17
The Student t test was used to compare the chronological age between the creation and validation groups. The Wilcoxon signed-rank test was used to compare knee bone age with chronological age and with hand bone age. Spearman correlation analysis was employed to assess the association between knee bone age and chronological age and between knee bone age and hand bone age, where a Spearman rho (rS) of <0.1 indicated negligible correlation, 0.1 to 0.4 weak, 0.4 to 0.7 moderate, 0.7 to 0.9 strong, and 0.9 to 1.0 very strong correlation. 32 Statistical significance was set at P < .05. Statistical analysis was performed using SPSS 27.0 (IBM Corp) and SciPy library 1.11.4 for Python 3.7. 36
The power analysis to detect an effect size of 0.278 for the Wilcoxon signed-rank test utilizing the sample size of our validation group was conducted using G*Power (Version 3.1.9.6). 10 The effect size was calculated based on a difference of 4 months between chronological age and knee bone age as estimated based on the San Diego atlas, 21 and the standard deviation of the difference between the 2 bone ages in our creation group, which was 1.2 years both in the overall creation group and in the male and female subgroups. The power was determined to be 99% in the overall validation group and 90% and 87% in the male and female subgroups, respectively.
Results
Validation of the San Diego Atlas
In the validation group, the mean bone age as estimated based on the San Diego atlas (11.1 ± 4.3 years) did not significantly differ from the mean chronological age (11.1 ± 4.1 years) (P = .90). However, in male participants, the mean bone age based on the San Diego atlas was slightly older than the mean chronological age (11.9 ± 4.3 vs 11.7 ± 4.1 years; P = .048), while in female participants, it was slightly younger (10.2 ± 4.2 vs 10.5 ± 4.0 years; P = .04) (Table 3). In the subgroup analysis by age and sex, the mean bone age based on the San Diego atlas was 0.6 ± 1.7 years younger than the mean chronological age in female participants aged 7.0 to 12.9 years (P = .003) and 0.4 ± 1.1 years older in male participants aged 14.0 to 18.0 years (P = .045). No significant differences were observed in any other subgroup.
Mean Differences and Correlations Between Chronological Age and Knee Bone Age Based on the San Diego Atlas a

Values are presented as mean ± SD. Boldface P values indicate statistically significant difference between chronological and bone age (P < .05).
Calculated as (knee bone age based on San Diego atlas)–(chronological age).
Spearman correlation coefficient between the knee bone age and chronological age (P < .001 for all).
In the correlation analysis, we observed a very strong correlation between bone age based on the San Diego atlas and chronological age in overall male (rS = 0.96; P < .001) and overall female (rS = 0.94; P < .001) participants (Table 3 and Figure 3). However, this correlation was moderate in male participants aged 14.0 to 18.0 years (rS = 0.53; P < .001) and girls aged 13.0 to 18.0 years (rS = 0.63; P < .001).

Scatterplot showing the relationship between chronological age and knee bone age in the validation group (n = 278). The blue line and dots indicate the knee bone age based on the San Diego atlas. The orange line and dots indicate the knee bone age based on the Korean shorthand atlas.
In the subset of 31 participants with available left-hand radiographs, the mean bone age based on the San Diego atlas did not significantly differ from the hand bone age in either male or female participants (Table 4), and the mean bone age was strongly correlated with hand bone age (rS = 0.78; P < .001) (Figure 4).
Mean Differences Among Chronological Age, Hand Bone Age, and Knee Bone Age Based on the San Diego Atlas a

Values are presented as mean ± SD (range) unless otherwise indicated. BA, bone age; CA, chronological age.
Positive values indicate that the knee bone age is older than the chronological age or hand bone age, while negative values indicate the opposite.

Scatterplot showing the relationship between knee bone age and hand bone age in 31 participants with available left-hand radiographs obtained within 3 months of the knee magnetic resonance imaging. The blue line and dots indicate the knee bone age based on the San Diego atlas. The orange line and dots indicate the knee bone age based on the Korean shorthand atlas.
Validation of the Korean Shorthand Atlas
The intraobserver reliability for the Korean shorthand atlas was excellent, with ICCs >0.95 for all 3 reviewers (Table 5). The mean interobserver reliability was also excellent, with an ICC of 0.957 (95% CI, 0.941-0.970). The interobserver reliability between reviewers 1 and 2, reviewers 1 and 3, and reviewers 2 and 3 were all excellent, with ICCs >0.94 (Table 5). Therefore, for every analysis, the bone age estimated by reviewer 1 was used.
Intra- and Interobserver Reliability of the Korean Shorthand Atlas a

ICC, intraclass correlation coefficient.
The mean bone age based on the Korean shorthand atlas (11.1 ± 4.1 years) did not significantly differ from the chronological age, both in the overall validation group (11.1 ± 4.1 years; P = .74) and in any of the age and sex subgroups (Table 6). In the correlation analysis, a very strong correlation was observed between bone age based on the Korean shorthand atlas and chronological age in overall male (rS = 0.94; P < .001) and overall female (rS = 0.95; P < .001) participants (Table 6 and Figure 3). However, the correlation was weaker in older age groups, as seen in the San Diego atlas method.
Mean Differences and Correlations Between Chronological Age and Knee Bone Age Based on the Korean Shorthand Atlas a

Values are presented as mean ± SD.
Calculated as knee bone age – chronological age.
Spearman correlation coefficient between knee bone age and chronological age (P < .001 for all).
The mean bone age based on the Korean shorthand atlas did not significantly differ from the hand bone age for both male and female participants (Table 7). We also observed a strong correlation between bone age based on the Korean shorthand atlas and hand bone age (rS = 0.74; P < .001) (Figure 4).
Mean Differences Among Chronological Age, Hand Bone Age, and Knee Bone Age Based on the Korean Shorthand Atlas a

Values are presented as mean ± SD (range) unless otherwise indicated. BA, bone age; CA, chronological age.
Positive values indicate that the knee bone age is older than the chronological age or hand bone age, while negative values indicate the opposite.
Discussion
In the present study, we confirmed that the San Diego atlas can be used to accurately assess bone age in all Korean pediatric and adolescent population except female participants aged 7 to 13 years and male participants aged 14 to 18 years, which form the groups of greatest interest for bone age assessment in cases of ACL reconstruction. Furthermore, we developed a Korean shorthand atlas and validated its accuracy in all evaluated age and sex subgroups.
Skeletal maturity is a crucial aspect to consider when dealing with pediatric knee conditions, such as ACL tears, as it helps determine whether to perform a physeal-sparing or transphyseal reconstruction.9,15 However, bone age estimation methods based on knee radiographs have limitations similar to those for left-hand radiographs.1,35 The Pyle and Hoerr knee bone age atlas method has a reliability issue 31 similar to the Greulich and Pyle atlas method. 5 Moreover, it is not suitable for preadolescents and adolescents due to the lack of data points in these age groups.21,24 The Roche-Wainer-Thissen method is also impractical for daily use due to its complexity,27,28 similar to the Tanner-Whitehouse staging system.33,34 Recently, the modified Fels knee skeletal maturity system was developed, which consists of 7 radiographic parameters simplified from the Pyle and Hoerr and Roche-Wainer-Thissen methods. 4 However, it is still challenging to use in a busy clinical setting. In addition, it requires an additional knee radiograph for bone age estimation in patients who have already undergone knee MRI for the diagnosis of an ACL tear. Therefore, bone age estimation based on knee MRI, which has more information on skeletal maturity than knee radiographs, may be a better method for pediatric knee conditions.
Previous studies have suggested that children's race and region of residence can affect their skeletal maturity.25,26 However, the San Diego atlas for bone age estimation, which was created based on findings in children living in Southern California, was generally accurate in the relatively racially homogeneous population of South Korea (96% in 2015). 7 In the current study, bone age based on the San Diego atlas was similar to both chronological age and hand bone age. Although bone age was more advanced than chronological age in male participants aged 14.0 to 18.0 years, the mean difference between these 2 ages was relatively small (0.4 years). In all other age and sex subgroups, bone age based on the San Diego atlas was comparable with the chronological age, except in girls aged 7.0 to 12.9 years, in whom chronological age was more advanced than bone age by >6 months. This discrepancy was partially due to the late appearance of tibial epiphyseal extension toward the tubercle in our cohort; the median age for the appearance of this feature in female participants was 7.3 years in the study of Pennock et al,20,21 while it was 8.3 years in the current study. The delayed ossification of the tibial tubercle in our cohort might be attributed to the lesser participation in sports of Asian girls.6,37
The original San Diego atlas method, although generally accurate in the Korean population, is complex and time-consuming. Furthermore, it showed discrepancies between bone age and chronological age in certain subgroups. To address these shortcomings, we created a simple and accurate shorthand atlas for the Korean population. Our new atlas was devised by further dividing the features of tibial tubercle ossification and patellar ossification compared with the San Diego atlas. In addition, unlike the shorthand knee MRI atlas methods of Politzer et al 23 and Meza et al, 18 our method has an advantage in that we selected age-specific features based on both the median age and the standard deviation, whereas the other methods relied solely on the opinion of a senior author or the median age alone.
In the present study, the Korean shorthand atlas method showed excellent intra- and interobserver reliability for all reviewers, who were provided with brief instructions. This finding implies that anyone can utilize this atlas method without extensive training, regardless of their level of knowledge and experience in pediatric orthopaedics. Not only the original San Diego atlas method but also the subsequent 2 shorthand atlas methods based on the original San Diego atlas also demonstrated excellent intra- and interobserver reliability.18,21,23 These results suggest that the original San Diego atlas consisted of distinct age-specific features that make it a reliable method for estimating bone age.
The choice of which knee MRI atlas to use for estimating bone age can be a subject of debate. In South Korea, the Korean shorthand atlas method can be a better option in busy clinical settings due to its high accuracy, reliability, and time efficiency. In the United States, the shorthand atlases made from the features of the San Diego atlas can be a good choice in a clinic.18,21,23 However, compared with the original San Diego atlas, the shorthand atlases have relatively larger age gaps between sequential images due to the smaller number of age categories. Therefore, if there is enough time to evaluate MRI, the original San Diego atlas could be a better option for more precise bone age determination, particularly when bone age based on a shorthand atlas is ambiguous. Nevertheless, we believe that the Korean shorthand atlas is more applicable in South Korea, particularly for girls aged 7 to 13 years.
Limitations
The present study has some limitations. First, the Korean shorthand atlas was not externally validated. Further study is required to validate the atlas in other centers in South Korea or for other ethnicities, particularly the population of other Asian countries sharing similar culture to South Korea. Second, the current study only included participants with normal knee morphology, which may limit the applicability of the atlas to patients with conditions affecting knee anatomy. Third, we could not exclude participants with very high or low percentile of height (for example, height >5% or <95%) due to lack of height information. They might have skeletal maturity beyond the mean within the same chronological age cohort. Fourth, although South Korea has a predominantly homogeneous race, with 96% of the population being of Korean descent, 7 we cannot exclude the possibility that some participants may have belonged to other ethnicities. Fifth, there might have been a selection bias because participants with accelerated or delayed skeletal maturation or pathologic bone conditions may have been more likely to have hand radiographs, even though we excluded those with conditions that could affect their bone age or bone morphology. Finally, although we validated the original San Diego atlas in the Korean population, the shorthand atlases based on the original San Diego atlas were not validated in the current study.
Conclusion
The San Diego knee MRI–based bone age atlas method was found to be accurate for estimating bone age in the South Korean pediatric and adolescent population except in female participants aged 7.0 to 12.9 years and male participants aged 14.0 to 18.0 years. The Korean knee MRI–based shorthand bone age atlas was reliable and accurate for estimating bone age in South Korean pediatric and adolescent population of both sexes and all age ranges. This atlas may help surgeons avoid the need for additional left-hand or knee radiographs in pediatric patients with knee conditions.
Footnotes
Acknowledgements
The authors thank Myoung-jin Jang from the Medical Research Collaborating Center at Seoul National University Hospital for providing a statistical review.
Final revision submitted August 21, 2024; accepted September 5, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University Hospital (reference No. H-2004-006-1114).