
Abstract
Background:
Global acetabular retroversion is classically treated with open reverse periacetabular osteotomy. Given the low morbidity and recent success associated with the arthroscopic treatment of femoroacetabular impingement (FAI), there may also be a role for arthroscopic treatment of acetabular retroversion. However, the safety and outcomes after hip arthroscopic surgery for retroversion need further study, and the effect of impingement from the anterior inferior iliac spine (subspine) in patients with retroversion is currently unknown.
Hypothesis:
Arthroscopic treatment for global acetabular retroversion will be safe, and patients will have similar outcomes compared with a matched group undergoing arthroscopic treatment for focal pincer-type FAI.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Patients undergoing hip arthroscopic surgery for symptomatic global acetabular retroversion were prospectively enrolled and compared with a matched group of patients undergoing arthroscopic surgery for focal pincer-type FAI. Both groups underwent the same arthroscopic treatment protocol. All patients were administered patient-reported outcome (PRO) measures, including the 12-item Short-Form Health Survey (SF-12) Physical Component Summary (PCS) and a Mental Component Summary (MCS), modified Harris Hip Score (mHHS), Hip disability and Osteoarthritis Outcome Score (HOOS), and visual analog scale (VAS) for pain preoperatively and at 1 year postoperatively.
Results:
There were no differences in age, sex, or body mass index between 39 hips treated for global acetabular retroversion and 39 hips treated for focal pincer-type FAI. There were no major or minor complications in either group. Patients who underwent arthroscopic treatment for global acetabular retroversion demonstrated similar significant improvements in postoperative PRO scores (scores increased by 17 to 43 points) as patients who underwent arthroscopic treatment for focal pincer-type FAI. Patients treated for retroversion who also underwent subspine decompression had greater improvement than patients who did not undergo subspine decompression for the HOOS-Pain (33.7 ± 15.3 vs 22.5 ± 17.6, respectively; P = .046) and HOOS–Quality of Life (49.7 ± 18.8 vs 34.6 ± 22.0, respectively; P = .030) scores.
Conclusion:
Arthroscopic treatment for acetabular retroversion is safe and provides significant clinical improvement similar to arthroscopic treatment for pincer-type FAI. Patients with acetabular retroversion who also underwent arthroscopic subspine decompression demonstrated greater improvements in pain and quality of life outcomes than those who underwent arthroscopic treatment without subspine decompression.
Keywords
Global acetabular retroversion is a morphological variation involving posterior tilt of the acetabular opening, resulting in loss of the normal 17° ± 6° of anteversion of the acetabulum. 33 This creates a condition in which the hip is at risk for femoroacetabular impingement (FAI) due to anterolateral overcoverage and at an additional risk of instability due to posterior undercoverage. 5,39 Radiographic indicators of acetabular retroversion visible in the anteroposterior (AP) pelvis view include the crossover sign, posterior wall sign, and ischial spine sign. 34,38 All 3 radiographic findings are seen in cases of global acetabular retroversion, while a crossover sign in isolation may indicate a focal retroversion or pincer deformity with limited anterosuperior overcoverage or a prominence of the anterior inferior iliac spine (AIIS) (subspine impingement). 5,14,21,39 The role of subspine impingement in the symptoms of patients with FAI is ill-defined and often untreated. 13,35 In addition, although anatomically the position of the AIIS may be altered in the retroverted acetabulum, the relationship between subspine impingement and acetabular retroversion has not been investigated.
While open realignment with anteverting or “reverse” periacetabular osteotomy (PAO) to treat FAI in the setting of acetabular retroversion has demonstrated good long-term outcomes, the procedure is morbid with possible complications, including nonunion or neurovascular damage, and it may neglect associated intra-articular labrocartilaginous abnormalities more readily treated arthroscopically. 29,32 Recent studies have shown that both hip arthroscopic surgery and anteverting PAO for the treatment of symptomatic acetabular retroversion can lead to significant improvements in patient-reported outcomes (PROs), with a minimal progression of osteoarthritis. 12,21 Hartigan et al 12 found that in their case series, the arthroscopic treatment of global acetabular retroversion had a 99% survivorship rate at 2 years, with a minor complication rate of only 3.6%. However, there has been no previous analysis of PROs after the arthroscopic treatment of global acetabular retroversion as compared with outcomes after the arthroscopic treatment of focal pincer-type FAI. Patients with pincer-type FAI have well-established long-term satisfaction with arthroscopic management and are most comparable as a matched cohort for comparison. 2,19,28,31
The goal of this study was to compare outcomes in patients undergoing hip arthroscopic surgery for the treatment of global acetabular retroversion with a matched group undergoing hip arthroscopic surgery for focal pincer-type FAI. Additionally, we aimed to identify any differences in outcomes for patients with acetabular retroversion treated with additional subspine decompression in an effort to better delineate the role that this morphology plays in symptom generation in the retroverted pelvis. We hypothesized that there would be no significant difference in outcomes between the retroversion and focal pincer groups but that subspine decompression would lead to improved outcomes in cases of acetabular retroversion.
Methods
Patient Selection and Data Collection
Patients undergoing hip arthroscopic surgery for symptomatic FAI secondary to global acetabular retroversion or focal pincer-type FAI were prospectively enrolled in the study. All surgical procedures were performed by a sports medicine fellowship–trained surgeon with a focus on hip arthroscopic surgery (A.L.Z.). The study protocol was reviewed and approved by an institutional review board, and all patients provided consent before enrollment in the study. Inclusion criteria consisted of patients diagnosed with symptomatic focal pincer-type FAI or FAI secondary to acetabular retroversion, with failure of conservative management and physical therapy. Acetabular retroversion was diagnosed if the patient had all 3 radiographic findings, including a positive crossover sign, ischial spine sign, and posterior wall sign, on preoperative plain radiographs (Figure 1A). Focal pincer-type FAI was diagnosed for patients with an isolated crossover sign or lateral center-edge angle (LCEA) greater than 40° and no other radiographic abnormalities (Figure 1B). In addition, clinical examination findings consistent with FAI, such as a positive flexion, adduction, and internal rotation test result, were needed for inclusion. Intra-articular injections before arthroscopic surgery were used for diagnostic and therapeutic purposes but were not a strict inclusion criterion, as some patients refused injections and elected for surgical treatment after failing physical therapy. Exclusion criteria consisted of patients with osteoarthritis, hypermobility, and age older than 60 years.

Plain radiographs. (A) Global acetabular retroversion: the acetabular posterior wall (dashed blue line) crosses over the anterior wall (solid yellow line), creating a positive crossover sign. The posterior wall lies medial to the center of the femoral head (red dot), depicting a positive posterior wall sign. The arrow points to the ischial spine visible medial to the pelvic brim, a positive ischial spine sign. The presence of all 3 signs is indicative of global acetabular retroversion. (B) A focal pincer lesion with an isolated crossover sign: the acetabular posterior wall (dashed blue line) crosses over the anterior wall (solid yellow line), creating a positive crossover sign. The posterior wall is seen in its normal position lateral to the center of the femoral head (red dot). The ischial spine is not visible medial to the pelvic brim.
All postoperative outcome data were analyzed at 1-year follow-up. One-year follow-up was considered sufficient based on previous studies of arthroscopic FAI and subspine impingement surgery that demonstrated that the minimal clinically important difference (MCID) and substantial clinical benefit (SCB) were achieved within 1 year of surgery. 25 –27 Patient demographics such as sex, age, and body mass index (BMI) were recorded along with any major or minor complications or readmissions. All patients underwent a radiographic evaluation, which included preoperative and postoperative radiographs of the pelvis in the supine AP view and Dunn lateral 45° view, as well as preoperative magnetic resonance imaging of the affected hip. 30 Radiographic measurements, including the LCEA and Tönnis grade, were recorded preoperatively and postoperatively.
Surgical Treatment
All procedures were performed in the ambulatory surgery center of a tertiary referral academic medical center. The arthroscopic treatment of global acetabular retroversion was similar to the treatment of focal pincer-type FAI. Two arthroscopic portals (anterolateral and midanterior) were utilized. Acetabuloplasty was performed, followed by labral repair and femoroplasty in all patients. Limited anterior wall acetabuloplasty of 4 to 6 mm was performed in the retroversion group without significant superior acetabular rim removal to avoid iatrogenic dysplasia and instability. We also did not aim to remove the crossover sign completely in patients with global retroversion, as this would create iatrogenic anterior instability. Arthroscopic subspine decompression was performed if the AIIS was found to be prominent intraoperatively. This was performed similarly to previous reports 13 by exposing the AIIS on the anterior acetabular wall using a radiofrequency ablation device with fluoroscopic guidance, followed by using an arthroscopic burr to remove bone on the articular side of the spine and eliminate the abnormal prominent contour of the AIIS seen on fluoroscopy. Care was taken to not overresect the AIIS and cause iatrogenic rectus injuries by limiting the resection to less than 8 cm. A limited capsulotomy was performed in all patients, and capsular closure was performed in patients with greater joint laxity who may be at risk for postoperative instability. Any intraoperative and postoperative complications were recorded.
Patient-Reported Outcomes
Patients completed 3 PRO measures both preoperatively and postoperatively: the 12-item Short-Form Health Survey (SF-12), the modified Harris Hip Score (mHHS), and the Hip disability and Osteoarthritis Outcome Score (HOOS). These PRO measures have been validated in past studies of hip arthroscopic surgery outcomes to assess a patient’s pain, functional status, and quality of life. 17,36 The SF-12 contains a Physical Component Summary (PCS) and a Mental Component Summary (MCS) to assess general health–related quality of life. 7,15,16,37 The mHHS produces a single score assessing hip function. 1,11 The HOOS provides 5 subscores: Symptoms, Pain, Activities of Daily Living (ADL), Sports, and Quality of Life (QOL). 23,24 In addition, patients rated their pain preoperatively and postoperatively on a visual analog scale (VAS) from 0 to 10, with 0 referring to no pain and 10 referring to the most pain. All data were collected in REDCap (version 8.1.4).
Statistical Analysis
An a priori power analysis was performed based on results of a previous FAI hip arthroscopic surgery study that used similar PRO measures as the main outcomes of interest. When examining preoperative versus1-year postoperative mHHS and HOOS-QOL scores in patients older than 25 years, to adequately power the study to 1 – β = 0.80, it was found that 14 patients were needed in each group for the mHHS and 12 patients for the HOOS-QOL. 4 An unpaired Student t test was used to calculate statistical significance between preoperative and postoperative values, significance in the change in PRO scores (postoperative minus preoperative) between groups, and significance in demographic variables. Our study used the mean change in preoperative and postoperative scores to measure improvement, which differs from many studies that compared only postoperative PRO scores. 6,9,18 Evaluating the mean change in values may be a better way of illustrating improvement because if the patient started at a lower or higher preoperative score, this method captures his or her progress, regardless of the final postoperative score. The Pearson chi-square test was used to assess significance between categorical variables such as sex and affected hip side. A P value <.05 was considered statistically significant for all calculations. A post hoc power analysis conducted for the mHHS in the non–subspine decompression subgroup (n = 17) resulted in a power value of 98.5%. All statistical computations were conducted in StatPlus:mac (version v6; AnalystSoft). SF-12 scores were calculated, with permission, using the Veterans RAND 12-Item Health Survey (RAND VR-12) scoring program in R software (version 3.4.0; R Foundation for Statistical Computing).
Results
Demographic and Radiographic Findings
Thirty-nine hips met the inclusion and exclusion criteria for global acetabular retroversion. These patients were matched to 39 hips with focal pincer-type FAI without acetabular retroversion based on sex, age, and BMI. Of the 39 hips in the retroversion group, there were 22 patients who underwent subspine decompression and 17 patients who underwent arthroscopic treatment without subspine decompression. Demographic and radiographic findings for the retroversion and matched groups are provided in Table 1. All patients met a minimum 1-year follow-up, and a postoperative data analysis was performed at the 1-year follow-up time point. There was no significant difference between the retroversion and matched groups in sex (16 males and 23 females in each group; P > .999), age (31.2 vs 33.9 years, respectively; P = .226), BMI (23.8 vs 25.0 kg/m2, respectively; P = .120), or involved hip side (21 right and 18 left vs 23 right and 16 left, respectively; P = .647). All patients in the retroversion group had a positive crossover sign, ischial spine sign, and posterior wall sign. The mean LCEA was lower in the retroversion group compared with the matched group (33.4° vs 36.3°, respectively; P = .024).
Demographics and Intraoperative Findings for Retroversion and Matched Groups a

a Values are presented as No. of patients unless otherwise specified.
b Student unpaired-samples t test for mean values and chi-square test for categorical values.
Demographic and radiographic findings within the retroversion group for the 22 patients in the subspine decompression subgroup versus the 17 patients in the non–subspine decompression subgroup are provided in Table 2. There were no significant differences in age, BMI, sex, or involved hip side between the subspine decompression and non–subspine decompression subgroups. The mean LCEA did not differ significantly between the subspine decompression and non–subspine decompression subgroups (33.6° vs 33.0°, respectively; P = .730).
Demographics and Intraoperative Findings for Subspine Decompression and Non–Subspine Decompression Subgroups a
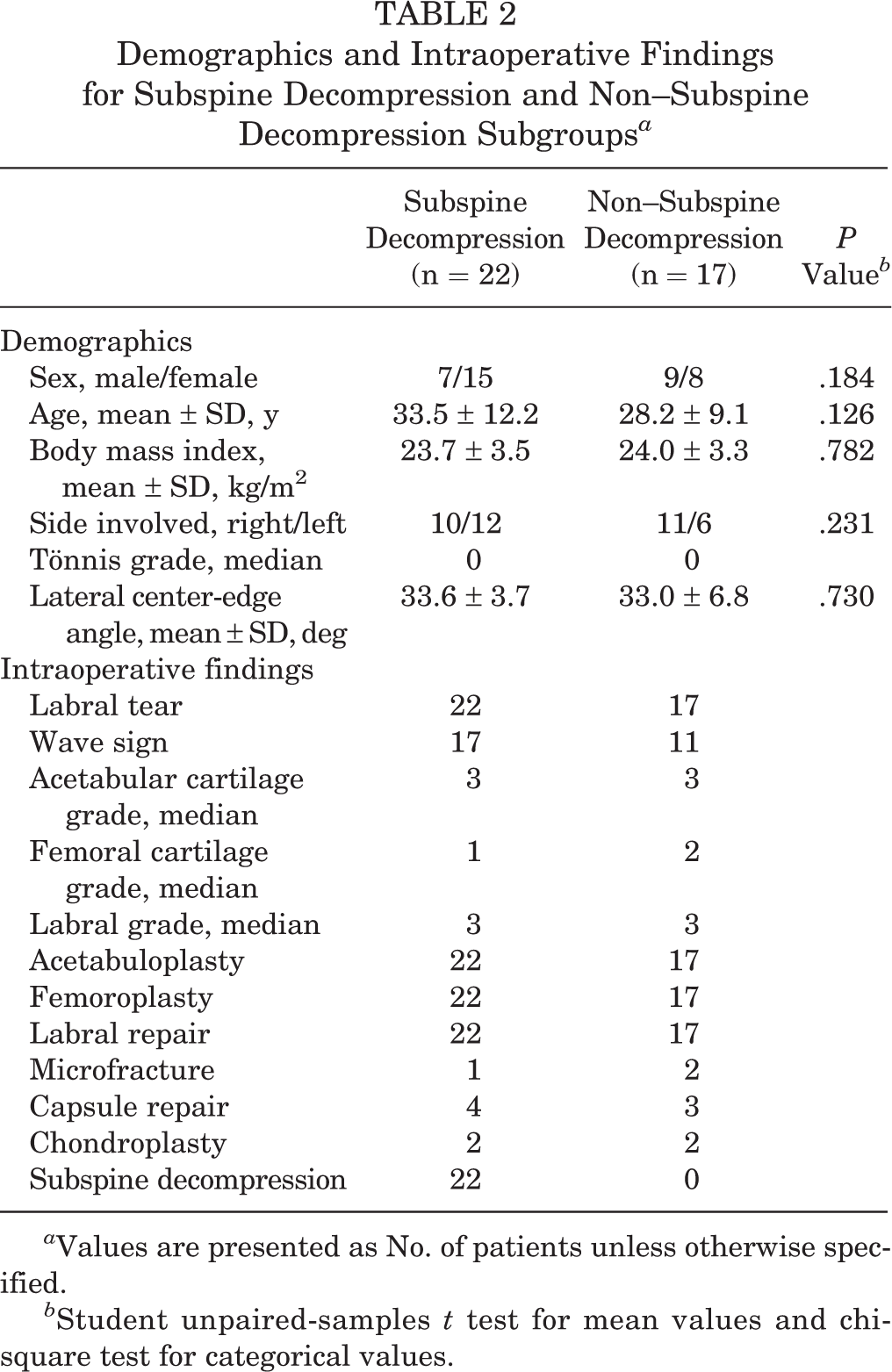
a Values are presented as No. of patients unless otherwise specified.
b Student unpaired-samples t test for mean values and chi-square test for categorical values.
Intraoperative Findings
The intraoperative findings for the retroversion and matched groups are provided in Table 1. All patients underwent pincer resection (acetabuloplasty) and labral repair except for 1 patient with labral debridement. The intraoperative findings within the retroversion group for the subspine decompression and non–subspine decompression subgroups are provided in Table 2.
Outcomes
There were no major or minor complications in either the retroversion or matched groups, and no patient converted to total hip arthroplasty. All patients were safely discharged home on the same day of the outpatient procedures. Preoperative to postoperative PRO scores for the retroversion and matched groups are provided in Table 3 and shown in Figure 2. For both groups, there was a significant improvement in preoperative to postoperative scores for the VAS pain, SF-12 PCS, mHHS, HOOS-Symptoms, HOOS-Pain, HOOS-ADL, HOOS-Sports, and HOOS-QOL (all P < .001). There was no change in the SF-12 MCS score, nor was there a significant difference in the mean change in PRO scores between the retroversion and matched groups for all PRO measures (Table 4). One patient in the retroversion group did not complete the SF-12 PCS or MCS and was excluded from the analysis.
Preoperative and 1-Year Postoperative Patient-Reported Outcome Scores for Retroversion and Matched Groups a

a Values are presented as mean ± SD. ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCS, Mental Component Summary; mHHS, modified Harris Hip Score; PCS, Physical Component Summary; QOL, Quality of Life; SF-12, 12-item Short-Form Health Survey; VAS, visual analog scale.
b Student unpaired-samples t test.

Preoperative versus 1-year postoperative patient-reported outcome (PRO) scores after hip arthroscopic surgery for the retroversion and matched groups. The error bars indicate standard error. The mean postoperative PRO scores improved significantly from the preoperative scores in both groups for the modified Harris Hip Score (mHHS) and all Hip disability and Osteoarthritis Outcome Score (HOOS) subscales: HOOS-Symptoms, HOOS-Pain, HOOS–Activities of Daily Living (ADL), HOOS-Sports, and HOOS–Quality of Life (QOL).
Mean Difference in Patient-Reported Outcome Scores for Retroversion and Matched Groups a

a Values are presented as mean ± SD. ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCS, Mental Component Summary; mHHS, modified Harris Hip Score; PCS, Physical Component Summary; QOL, Quality of Life; SF-12, 12-item Short-Form Health Survey; VAS, visual analog scale.
b Student unpaired-samples t test.
Preoperative to postoperative PRO scores for the subspine decompression and non–subspine decompression subgroups are provided in Table 5 and shown in Figure 3. For both subgroups, there was a significant improvement in preoperative to postoperative scores for all measures except the SF-12 MCS. Patients who underwent subspine decompression for acetabular retroversion had greater improvement than patients with retroversion who did not undergo subspine decompression regarding the HOOS-Pain (33.7 vs 22.5, respectively; P = .046) and HOOS-QOL (49.7 vs 34.6, respectively; P = .030) (Table 6 and Figure 4).
Preoperative and 1-Year Postoperative Patient-Reported Outcome Scores for Subspine Decompression and Non–Subspine Decompression Subgroups a
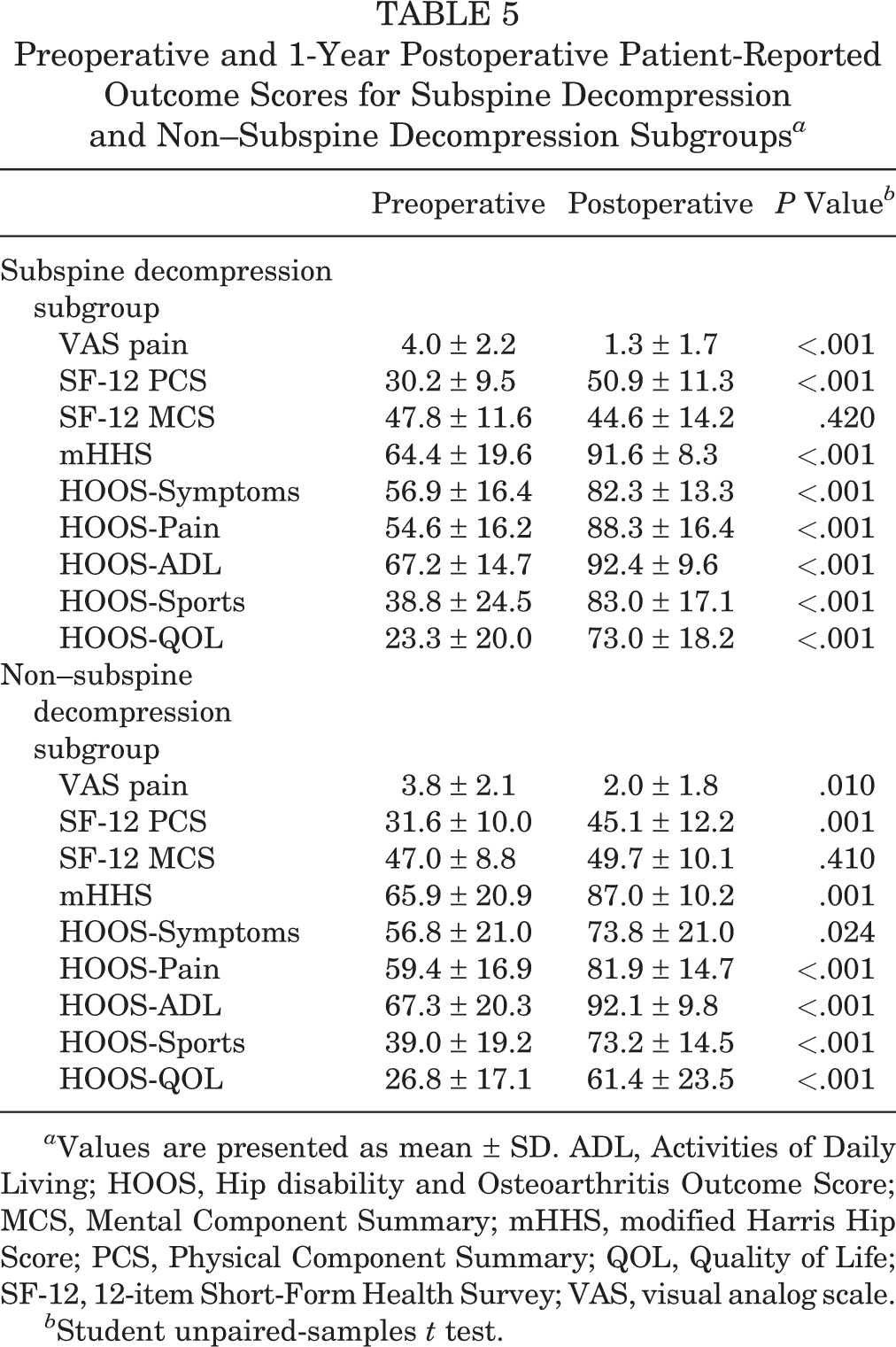
a Values are presented as mean ± SD. ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCS, Mental Component Summary; mHHS, modified Harris Hip Score; PCS, Physical Component Summary; QOL, Quality of Life; SF-12, 12-item Short-Form Health Survey; VAS, visual analog scale.
b Student unpaired-samples t test.

Preoperative versus 1-year postoperative patient-reported outcome (PRO) scores after hip arthroscopic surgery for the subspine decompression and non–subspine decompression subgroups. The error bars indicate standard error. The mean postoperative PRO scores improved significantly from the preoperative scores in both subgroups for the modified Harris Hip Score (mHHS) and all Hip disability and Osteoarthritis Outcome Score (HOOS) subscales: HOOS-Symptoms, HOOS-Pain, HOOS–Activities of Daily Living (ADL), HOOS-Sports, and HOOS–Quality of Life (QOL).
Mean Difference in Patient-Reported Outcome Scores for Subspine Decompression and Non–Subspine Decompression Subgroups a
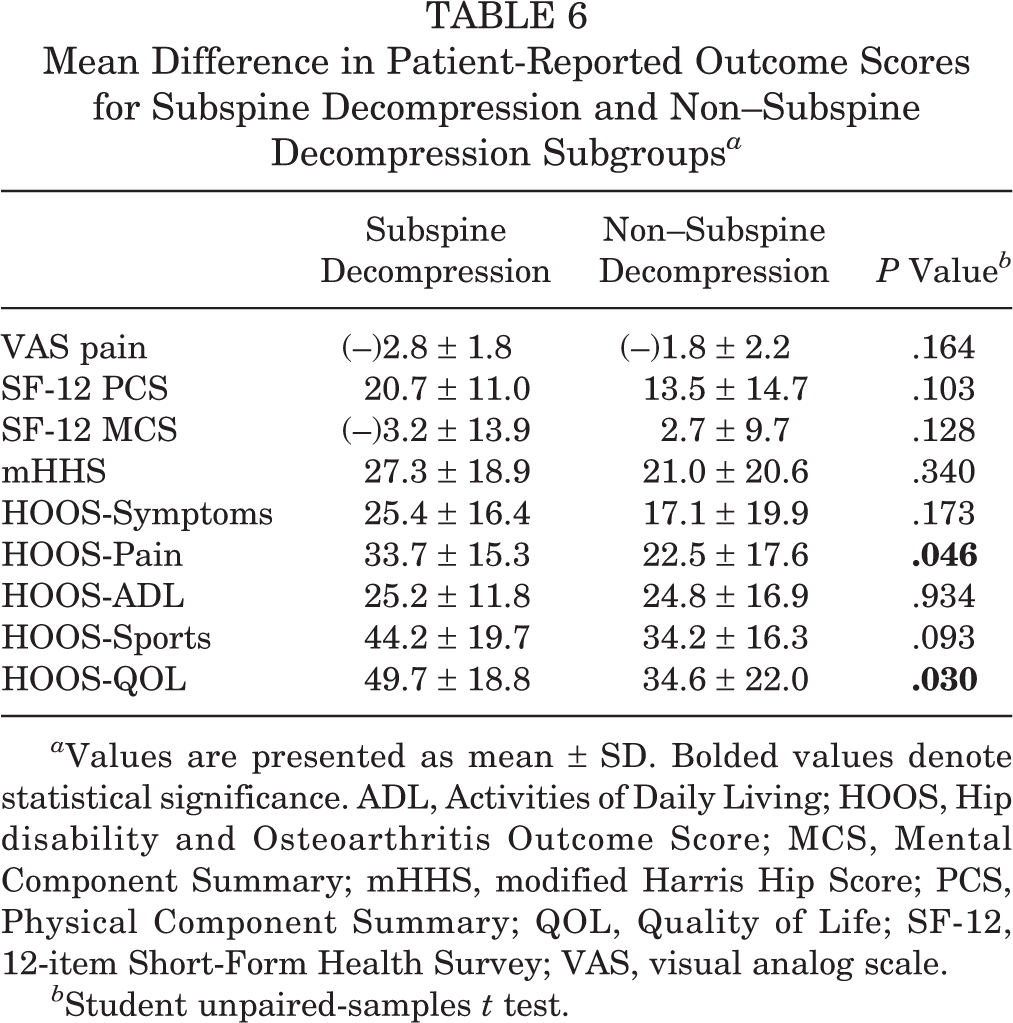
a Values are presented as mean ± SD. Bolded values denote statistical significance. ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCS, Mental Component Summary; mHHS, modified Harris Hip Score; PCS, Physical Component Summary; QOL, Quality of Life; SF-12, 12-item Short-Form Health Survey; VAS, visual analog scale.
b Student unpaired-samples t test.

Change in patient-reported outcome (PRO) scores after hip arthroscopic surgery: difference between 1-year postoperative and preoperative PRO scores for the subspine decompression and non–subspine decompression subgroups. The error bars indicate standard error. *The Hip disability and Osteoarthritis Outcome Score (HOOS)–Pain and HOOS–Quality of Life (QOL) showed statistically significant differences in the change in scores between the subspine decompression and non–subspine decompression subgroups. The change in scores was not statistically significantly different for the modified Harris Hip Score (mHHS), HOOS-Symptoms, HOOS–Activities of Daily Living (ADL), or HOOS-Sports.
Discussion
The purpose of this study was to evaluate outcomes after the arthroscopic treatment of acetabular retroversion in comparison with a matched group undergoing the arthroscopic treatment of focal pincer-type FAI. In doing so, we found that patients treated with hip arthroscopic surgery for acetabular retroversion improved greatly and equally compared with patients treated for focal pincer-type FAI and without major or minor complications, validating the utility of arthroscopic treatment for this condition. In addition, while patients with global acetabular retroversion treated either with or without subspine decompression improved preoperatively to postoperatively, those who underwent subspine decompression demonstrated greater improvement in pain and quality of life outcomes. These findings suggest that subspine decompression enhances patient outcomes with the arthroscopic treatment of acetabular retroversion and should be considered in these patients.
Because of the known increased incidence of osteoarthritis in hips with retroverted acetabula, this morphological variant is worthy of attention. 8 Hartigan et al 12 previously reported on the 2-year outcomes of 78 retroverted acetabula treated with hip arthroscopic surgery, describing an improvement in preoperative versus postoperative VAS (5.9 to 2.5), mHHS (65 to 81), HOOS-ADL (69 to 88), and HOOS-Sports (47 to 76) scores. Our results (VAS score decreased from 3.9 to 1.6, HOOS-ADL score increased from 67.3 to 92.3, and HOOS-Sports score increased from 38.9 to 78.7) are comparable with this previous series, with the additional finding that the improvements in PRO scores align with those observed in nonretroverted patients with pincer-type FAI treated in a similar fashion. This comparison group is useful because hip arthroscopic surgery has a good track record in cases of pincer-type FAI, with significant improvements in PRO scores and minimal conversion to arthroplasty. 3 In their large cohort of patients with pincer-type FAI treated arthroscopically with acetabuloplasty and labral refixation, Redmond et al 31 reported improvements in VAS (6.3 to 2.8), mHHS (61.2 to 84.4), HOOS-ADL (40.1 to 74.1), and HOOS-Sports (40.1 to 74.1) scores, again comparable with those seen in both groups of this study. The theoretical risk of posterior undercoverage in global acetabular retroversion has been a cause for some to hesitate in adopting arthroscopic acetabular decompression for the problem. However, our surgical technique of performing limited anterior acetabuloplasty while preserving the superior acetabulum demonstrated no major or minor complications, including postoperative subluxations or dislocations, in this cohort. The findings of equivalence in PRO scores between retroverted hips and hips with pincer-type FAI further support the use of arthroscopic treatment in these patients.
Extension of the AIIS to or below the level of the acetabulum can create a dynamic point of contact against the femoral neck (subspine impingement), which if unrecognized or untreated at the time of hip arthroscopic surgery can ultimately require revision surgery. 19 We hypothesize that retroversion of the acetabulum can produce concomitant anterolateralization and distalization of the AIIS, which can cause patients with retroversion to be susceptible to subspine impingement. One other previous case report proposed that atraumatic (congenital) subspine impingement can be seen in association with acetabular retroversion because of rotation of the AIIS more anteriorly and distally. 20 However, there has been no previous analysis of the role of subspine impingement and decompression in patients with symptomatic global acetabular retroversion. The current study’s findings of clinically meaningful 15- and 11-point improvements in HOOS-QOL and HOOS-Pain scores, respectively, in patients with acetabular retroversion treated with additional arthroscopic subspine decompression suggest that an associated AIIS morphological variant may contribute to symptoms in the retroverted pelvis, warranting concurrent surgical intervention. As arthroscopic subspine decompression yields excellent clinical results in isolation or combined with femoroacetabular osteoplasty and labral procedures, the treatment of subspine abnormalities during acetabular retroversion treatment may provide further clinical benefit to patients. 10,22,26
Limitations
Although this is a novel analysis, this study is limited as a single-surgeon sample. The smaller number of patients in the subspine decompression (n = 22) and non–subspine decompression (n = 17) subgroups is another limitation, but the study was adequately powered for the mHHS and HOOS completed based on a priori and post hoc analyses. Additional studies, including possible cadaveric examinations, are necessary to continue investigating the role of subspine impingement in acetabular retroversion to determine if our results are unique. This relationship is a goal of future research at our institution.
Another limitation includes the study’s 1-year minimum follow-up time, which prevented us from examining long-term outcomes after hip arthroscopic surgery. However, based on prior studies, patients treated arthroscopically for FAI and isolated subspine decompression achieved the MCID and SCB at 1-year follow-up. 25 –27 Future longitudinal studies on acetabular retroversion and subspine decompression are needed to investigate the risk for revision surgery or conversion to total hip arthroplasty.
Conclusion
Arthroscopic treatment for acetabular retroversion is safe and provides significant clinical improvement similar to arthroscopic treatment for pincer-type FAI. Patients with acetabular retroversion who also underwent arthroscopic subspine decompression demonstrated greater improvements in pain and quality of life outcomes than patients with retroversion who underwent arthroscopic treatment without subspine decompression.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.L.Z. is a consultant for Stryker, has received research support from Zimmer Biomet, and has received educational support from Arthrex.
Ethical approval for this study was obtained from the University of California, San Francisco (approval No. 14-14742).