
Abstract
Background:
Global acetabular retroversion has been associated with an increased risk of hip osteoarthritis, femoroacetabular impingement, and intra-articular soft tissue abnormalities. However, the role of global acetabular retroversion on total hip arthroplasty (THA)–free survivorship has not been explored.
Purpose:
To compare long-term THA-free survivorship after primary hip arthroscopic surgery between patients with global acetabular retroversion and a propensity score–matched control group without global acetabular retroversion.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective study examined patients aged ≥18 years with a minimum 8-year follow-up who underwent primary hip arthroscopic surgery by a single surgeon between May 2001 and September 2013 for the treatment of symptomatic labral tears secondary to femoroacetabular impingement. Patients with global acetabular retroversion, indicated by the combined presence of a crossover sign, ischial spine sign, and posterior wall sign on preoperative supine pelvic radiographs, were 1:1 propensity score matched by age, sex, body mass index, and labral treatment (repair vs debridement) to controls without global acetabular retroversion. Patient, radiographic, and intraoperative variables were compared between groups. Cox multivariate regression, controlling for global acetabular retroversion and Tönnis grade, was used to assess conversion to THA. Patient-reported outcome measure (PROM) scores were also compared between groups.
Results:
Overall, 49 patients (49 hips) with global acetabular retroversion were 1:1 matched to 49 controls, with a mean follow-up of 10.7 ± 2.1 and 11.1 ± 2.8 years, respectively (P = .524). There were no significant differences in patient characteristics and radiographic findings between groups. Patients with global acetabular retroversion had significantly greater rates of severe chondrolabral junction breakdown (P = .010). Unadjusted Kaplan-Meier survival curves analyzed by the log-rank test demonstrated significantly decreased survivorship among patients with global acetabular retroversion (68.6%) compared with matched controls (83.9%) at final follow-up (P = .036). Cox multivariate regression demonstrated that patients with global acetabular retroversion had a significantly greater risk of conversion to THA (hazard ratio, 3.94; P = .039). There were no statistically significant differences in any PROM scores at final follow-up.
Conclusion:
Patients with global acetabular retroversion had significantly inferior THA-free survivorship at a minimum 8-year follow-up after hip arthroscopic surgery relative to matched controls as well as greater rates of severe chondrolabral junction breakdown, despite no statistically significant differences in PROM scores at final follow-up among patients not converting to THA. These findings suggest that global acetabular retroversion on preoperative radiographic assessments may be a valuable predictor of long-term failure after hip arthroscopic surgery.
Keywords
Global acetabular retroversion, defined as a rotational-plane abnormality of the acetabulum with complete anterior overcoverage with corresponding posterior undercoverage,19,28 results in the acetabular opening facing more posterolaterally than normal. 43 This abnormality leads to relative overcoverage of the femoral head by the anterolateral acetabulum, which may result in pincer-type femoroacetabular impingement (FAI) with dynamic impingement between the anterolateral femoral head-neck junction and the retroverted acetabular rim. In addition, intrinsic to this abnormality is posterior undercoverage of the femoral head, which may increase the risk of posterior instability. 42 Apart from causing anterosuperior pincer-type FAI and posterior undercoverage, acetabular retroversion has been associated with early-onset hip osteoarthritis 36 in addition to labral and chondral injuries, 9 underscoring the frequent need for surgical management. While reverse (anteverting) periacetabular osteotomy has traditionally been the gold standard for surgical treatment in patients with acetabular retroversion with or without dysplasia, in recent years, hip arthroscopic surgery has emerged as a safe and effective method to treat patients with global acetabular retroversion, in conjunction with labral tears, in patients without severe dysplasia.14,20,41
Radiographically, in the anteroposterior (AP) pelvic view, the combined presence of the crossover sign, ischial spine sign, and posterior wall sign classically indicates global acetabular retroversion.18,19,42 This radiographic assessment has been employed in several studies to assess patient-reported outcome measure (PROM) scores in patients with versus without global acetabular retroversion, with studies consistently demonstrating that patients with global acetabular retroversion have favorable functional improvements after hip arthroscopic surgery, equivalent to those without global acetabular retroversion.12,20,31,35
However, to date, no studies have included a follow-up of sufficient duration to conduct a primary analysis of the effect of global acetabular retroversion on rates of conversion to total hip arthroplasty (THA). The association between global acetabular retroversion and early-onset hip osteoarthritis 36 raises a concern about the risk of THA in these patients, even after appropriate hip arthroscopic surgery. Furthermore, accurate assessments of this risk require a longer follow-up than what has been tracked to date, with studies featuring the longest follow-up reporting only 5 20 and 2 35 total cases of conversion to THA across both cohorts. Assessments of the effect of global acetabular retroversion on rates of conversion to THA will provide a crucial metric regarding the long-term prognosis for these patients. Thus, the purpose of the present study was to compare long-term THA-free survivorship after primary hip arthroscopic surgery between patients with global acetabular retroversion and a propensity score–matched control group without global acetabular retroversion. We hypothesized that patients with global acetabular retroversion would have inferior long-term THA-free survivorship after hip arthroscopic surgery.
Methods
Study Design
This was a retrospective cohort study of patients with a minimum 8-year follow-up who underwent hip arthroscopic surgery for the treatment of symptomatic acetabular labral tears. All patients were treated by a single fellowship-trained sports medicine surgeon (S.D.M.) between May 2001 and September 2013. During the study period, patients who presented to the senior author's (S.D.M.) clinic with hip pain underwent a standardized preoperative evaluation, consisting of hip and pelvic radiography (ie, supine AP pelvic, AP hip, and 45° Dunn lateral views) and a physical examination with provocative testing of the labrum and an assessment of impingement-related symptoms (eg, pain and/or limited range of motion with flexion, adduction, and internal rotation [FADIR] or flexion, abduction, and external rotation [FABER]). 13 Patients with positive clinical and radiographic findings underwent magnetic resonance arthrography to evaluate labral tears, coupled with a diagnostic and therapeutic intra-articular hip joint injection (ie, combined local anesthetic with a low-dose corticosteroid). 21 Finally, all patients underwent initial nonoperative management, including activity modification and formal physical therapy, for a minimum of 3 months. Patients who failed to achieve adequate symptom and functional improvements after nonoperative management and who underwent hip arthroscopic surgery were reviewed for inclusion in this study. 32 This study received institutional review board approval (No. 2011P000053).
Study Population
Inclusion criteria were (1) age ≥18 years at the time of surgery, (2) primary hip arthroscopic surgery for the treatment of symptomatic acetabular labral tears between May 2001 and September 2013, (3) available preoperative AP pelvic radiographs, and (4) completed PROMs at a minimum 8-year follow-up. Exclusion criteria were (1) previous surgery on the ipsilateral hip, (2) advanced hip osteoarthritis (Tönnis grade >1), (3) radiographic evidence of hip dysplasia (lateral center edge angle [LCEA] <20°), and/or (4) previous hip conditions (eg, fractures, inflammatory arthropathy, Legg-Calve-Perthes disease, slipped capital femoral epiphysis, or avascular necrosis).
Radiographic Evaluation
Preoperative supine hip and pelvic radiographs were assessed for all patients. Acetabular retroversion was assessed in the AP pelvic view using 3 radiographic signs, as shown in Figure 1: crossover sign (the anterior acetabular wall crosses lateral to the posterior wall at some point, overlying the silhouette of the femoral head), ischial spine sign (the ischial spine projects medial to the pelvic brim), and posterior wall sign (the posterior wall protrudes medial to the center of the femoral head). Global acetabular retroversion was defined by the presence of all 3 of these radiographic signs; this definition has been used in previous studies assessing acetabular retroversion in the context of hip arthroscopic surgery.12,20,35 All pelvic radiographs were assessed by 2 independent reviewers (S.M.G. and J.S.L.) for signs of global acetabular retroversion, with all disputes mediated by a separate musculoskeletal-trained radiologist (F.J.S.). Acetabular and femoral version angles could not be measured because the senior surgeon (S.D.M.) does not routinely perform preoperative computed tomography (CT) or magnetic resonance imaging of the bilateral pelvis (necessary for acetabular version measurements) or the lower extremity that includes axial slices of both the femoral neck and femoral condyles (necessary for femoral version measurements).

Anteroposterior pelvic radiograph of a patient with global acetabular retroversion of the right hip, indicated by the simultaneous presence of the crossover sign (where the contour of the anterior wall [red dotted line] crosses lateral to the posterior wall [blue dotted line]), ischial spine sign (yellow arrow), and posterior wall sign (where the posterior wall [blue dotted line] lies medial to the center of the femoral head [green dot]).
Other radiographic measurements collected using the AP pelvic view included the Tönnis grade, joint space width, Tönnis angle, and LCEA. To measure joint space width, a computer-assisted semiautomated method was employed, as has been previously described. 34 Finally, the alpha angle was measured in the Dunn lateral view.
Surgical Technique
All patients underwent a standardized surgical technique that did not change during the study period. After the administration of general anesthesia, patients were positioned supine on a hip distraction table (Smith & Nephew) with a silicone-padded perineal post. Intra-articular access was first established with the anterolateral portal using intra-articular fluid distention under fluoroscopic guidance to avoid iatrogenic damage to the labrum. 2 Next, under direct arthroscopic visualization, the anterior, midanterior, and Dienst portals were placed to complete the puncture capsulotomy approach that avoids disruption of the iliofemoral ligament.7,11 Then, a thorough diagnostic examination was performed to assess the extent of damage to the labrum, chondrolabral junction (CLJ), acetabulum, and femoral head articular cartilage. The hip arthroscopic technique utilized includes the use of intermittent traction, the use of pulsed lavage to maintain ambient intra-articular temperatures, and an emphasis on CLJ preservation.26,27,37,38
As clinically indicated, capsular elevation and acetabuloplasty were performed to address underlying pincer deformities using a CLJ-preserving technique. 38 Labral repair was then performed for small, discrete linear tears that had adequate healthy tissue amenable to suture anchor fixation. If the labral tear was degenerative, hypoplastic, or isolated to a single plane involving <50% of the labrum, labral debridement was performed.17,24 After addressing any pincer impingement and labral lesions, traction was released to ensure restoration of the hip suction seal and confirm in-round labral repair. As indicated, cam deformities were resected via femoroplasty while the hip was flexed to 45°. Finally, a dynamic range of motion examination ensured restoration of the labral seal and adequacy of femoroacetabular decompression and was followed by the closure of all incisions. Capsular closure was not performed, given the minimally invasive nature of the puncture capsulotomy technique that does not significantly disrupt the hip capsule.
Postoperative Rehabilitation
Postoperatively, all patients followed the same 5-step, 6-month patient-guided rehabilitation protocol. First, patients were permitted immediate weightbearing as tolerated using a flat-foot gait with crutches for the first 6 weeks; for the first 3 of these weeks, they were prescribed daily deep vein thrombosis prophylaxis (aspirin 81 mg). At 6 weeks postoperatively, patients began to use a stationary bicycle with minimal resistance. At 10 weeks, patients could begin using an elliptical trainer on low resistance or swimming (± a pull buoy) while avoiding intense flutter kicks. At 4 months, patients resumed light strengthening exercises, including short arc leg presses and hamstring curls. Finally, at 6 months postoperatively, patients were permitted to resume impact-loading activities as tolerated. 25
Data Collection
Patient data were collected preoperatively, including age, sex, body mass index (BMI) at the time of surgery, and laterality. Intraoperative variables collected included traction time, Outerbridge grade of articular cartilage, labral tear size, Beck classification of labral damage and transition zone (ie, CLJ) cartilage injuries,3,4,22 type of osseous decompression performed for FAI, and labral management (debridement vs repair).
Group Matching
Patients satisfying all inclusion/exclusion criteria undergoing hip arthroscopic surgery with radiographic signs of global acetabular retroversion were 1:1 matched to patients undergoing hip arthroscopic surgery without global acetabular retroversion based on age, sex, BMI, and labral management using propensity score matching with the greedy nearest neighbor method. The adequacy of matching was assessed using balance diagnostics, including the percentage reduction in the standardized mean difference of the logit propensity score (closer to 100% indicates better matching) and the variance ratio (closer to 1 indicates better matching).
Outcome Measures
The primary outcome was conversion to THA at any point during the follow-up period after primary hip arthroscopic surgery. In addition, scores for the following 6 PROMs were obtained: modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), Lower Extremity Functional Scale (LEFS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports-Specific Subscale (HOS-SSS), and 33-item International Hip Outcome Tool (iHOT-33). For patients with a minimum 10-year follow-up, the rates of achieving the Patient Acceptable Symptom State (PASS) at 10-year follow-up were determined using previously published thresholds: mHHS (76.0), HOS-ADL (85.3), and HOS-SSS (60.2). 1
Secondary outcomes assessed included pain levels and patient satisfaction. Pain levels were assessed using the visual analog scale (VAS) for pain in which 0 indicated no pain and 10 indicated the worst pain imaginable. Finally, patient satisfaction was assessed with 3 questions, each via a binary “yes”/“no” response: satisfaction with overall treatment, satisfaction with the postoperative regimen, and whether the patient would elect to choose the same treatment again.
Statistical Analysis
An a priori power analysis was performed based on previous literature to identify the number of patients necessary to achieve 80% power for our primary outcome of conversion to THA. In line with previous literature reporting survivorship for patients with and without global acetabular retroversion undergoing acetabular repair, patients with global acetabular retroversion and controls were assigned an estimated long-term survivorship of 86.3% and 97.5%, respectively. 40 Based on a 1:1 enrollment ratio with an alpha value of .05, a total of 48 patients were needed in each group to achieve 80% power.
Interrater reliability for the assessment of global acetabular retroversion between the 2 raters was quantified using the Gwet AC1 coefficient. The following values were used to classify measurement agreement based on the AC1 coefficient: 0.00-0.20, none; 0.21-0.39, minimal; 0.40-0.59, weak; 0.60-0.79, moderate; 0.80-0.90, strong; and >0.90, almost perfect agreement. 23
Categorical variables were analyzed with the chi-square test or Fisher exact test, as appropriate. Continuous variables were compared using a 2-tailed independent t test. Cox multivariate regression, controlling for global acetabular retroversion and Tönnis grade, was used to assess conversion to THA. A survivorship analysis was performed using unadjusted Kaplan-Meier survival curves analyzed by the log-rank test. Rates of achieving the PASS at 10 years for the mHHS, HOS-ADL, and HOS-SSS were compared between groups using multivariate logistic regression, controlling for global acetabular retroversion and Tönnis grade. Parameter estimates and descriptive statistics for continuous variables are presented with 95% confidence intervals.
Frequency statistics are reported for all noncontinuous variables. A P value <.05 was considered statistically significant. All statistical analyses were performed using R (Version 4.3.1; R Foundation for Statistical Computing).
Results
Patient Selection and Matching
In total, 513 patients underwent hip arthroscopic surgery during the study period, but 339 could not be assessed because of the lack of patient data. Of 174 patients screened for this study, a retrospective review identified 159 patients satisfying inclusion criteria (91.4%) who were assessed for radiographic signs of global acetabular retroversion; this included 49 with global acetabular retroversion and 110 without global acetabular retroversion. For interrater reliability, the coefficient for the reliability of global acetabular retroversion based on preoperative radiographs was 0.895, indicating strong agreement between raters. After 1:1 propensity score matching, 49 patients with global acetabular retroversion were matched to 49 patients without global acetabular retroversion (Figure 2). Patients with only 1 or 2 radiographic signs of global acetabular retroversion were included in the matched control group. Balance diagnostics showed a 95.4% reduction in the standardized mean difference of the logit propensity score and a variance ratio of 1.05, suggesting adequate matching on the selected covariates (age, sex, BMI, and labral treatment).

CONSORT (Consolidated Standards of Reporting Trials) flowchart detailing patient selection criteria. BMI, body mass index.
Patient Characteristics and Radiographic Findings
Patients with global acetabular retroversion and matched controls had a mean follow-up of 10.7 ± 2.1 and 11.1 ± 2.8 years, respectively (P = .524). There were no significant differences in patient and radiographic parameters between groups, including age, sex, BMI, laterality, Tönnis grade, joint space width, Tönnis angle, LCEA, alpha angle, or type of FAI (P > .05 for all) (Table 1).
Patient Characteristics and Radiographic Findings a
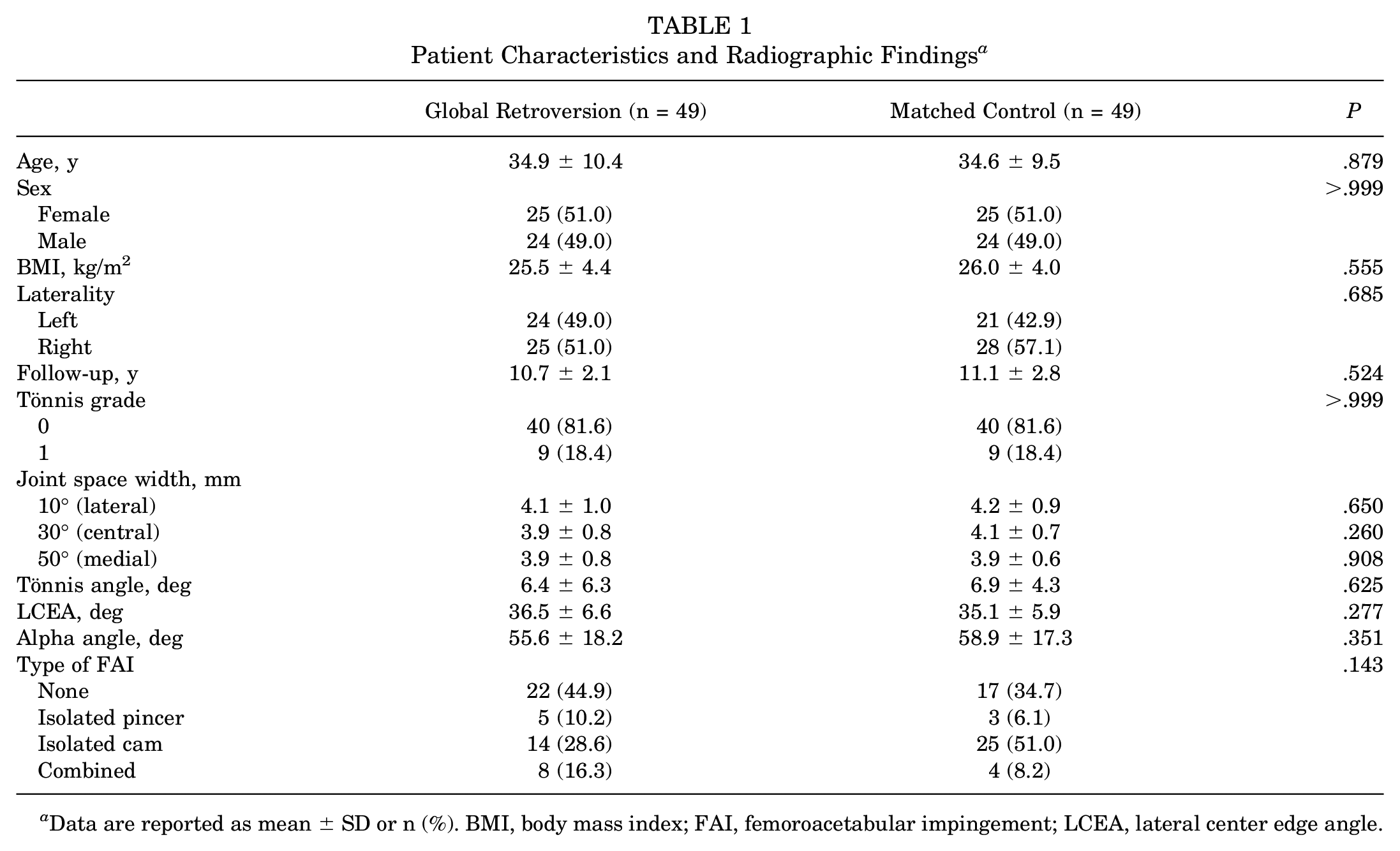
Data are reported as mean ± SD or n (%). BMI, body mass index; FAI, femoroacetabular impingement; LCEA, lateral center edge angle.
Intraoperative Findings and Procedures Performed
Comparing intraoperative findings, patients with global acetabular retroversion had significantly greater damage to the CLJ according to the Beck classification (P = .010), with 36.7% (n = 18) of the global retroversion group versus 14.3% (n = 7) of the matched control group having severe (grades 3-4) damage to the CLJ (P = .019). There were no significant differences in traction time, Outerbridge classification, labral tear size, Beck classification of labral damage, FAI treatment, and labral management between groups (P > .05 for all) (Table 2).
Intraoperative Findings and Procedures Performed a

Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). CLJ, chondrolabral junction; FAI, femoroacetabular impingement.
Long-term Survivorship
Unadjusted Kaplan-Meier survival curves analyzed by the log-rank test demonstrated significantly decreased survivorship among patients with global acetabular retroversion (68.6%) compared with controls (83.9%) at final follow-up (10.9 ± 2.5 years; P = .036) (Figure 3). There were 10 patients with global acetabular retroversion who converted to THA at a mean 7.5 ± 4.9 years compared with 3 matched controls who converted to THA at a mean 8.1 ± 2.8 years (time to conversion: P = .841) (Table 3). Age at conversion to THA (36.4 ± 11.8 vs 35.1 ± 10.2 years, respectively) was also not significantly different between patients with global acetabular retroversion and matched controls (P = .551). Cox multivariate regression, controlling for Tönnis grade, demonstrated that patients with global acetabular retroversion had a significantly greater risk of conversion to THA (hazard ratio, 3.94; P = .039). Tönnis grade (1 vs 0) was not a significant predictor of conversion to THA (hazard ratio, 3.36; P = .059).

Unadjusted Kaplan-Meier survival curves depicting total hip arthroplasty (THA)–free survivorship as a function of time between patients with global acetabular retroversion (“yes”) and matched controls (“no”). Data were analyzed by the log-rank test.
Conversion to THA a

Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). THA, total hip arthroplasty.
PROM and Pain Scores
Consistent with previous literature,6,20 PROM scores for patients who converted to THA were excluded from analysis. There were no differences in any of the PROM scores between patients with global acetabular retroversion and controls at final follow-up, including the mHHS (86.3 ± 14.8 vs 86.5 ± 12.6, respectively; P = .946), NAHS (85.8 ± 14.8 vs 85.1 ± 13.9, respectively; P = .842), LEFS (69.8 ± 12.6 vs 69.4 ± 10.9, respectively; P = .870), HOS-ADL (92.4 ± 10.8 vs 90.3 ± 10.0, respectively; P = .373), HOS-SSS (82.8 ± 18.9 vs 79.1 ± 21.1, respectively; P = .404), or iHOT-33 (76.7 ± 23.9 vs 72.0 ± 22.2, respectively; P = .362) (Table 4).
PROM and Pain Scores a
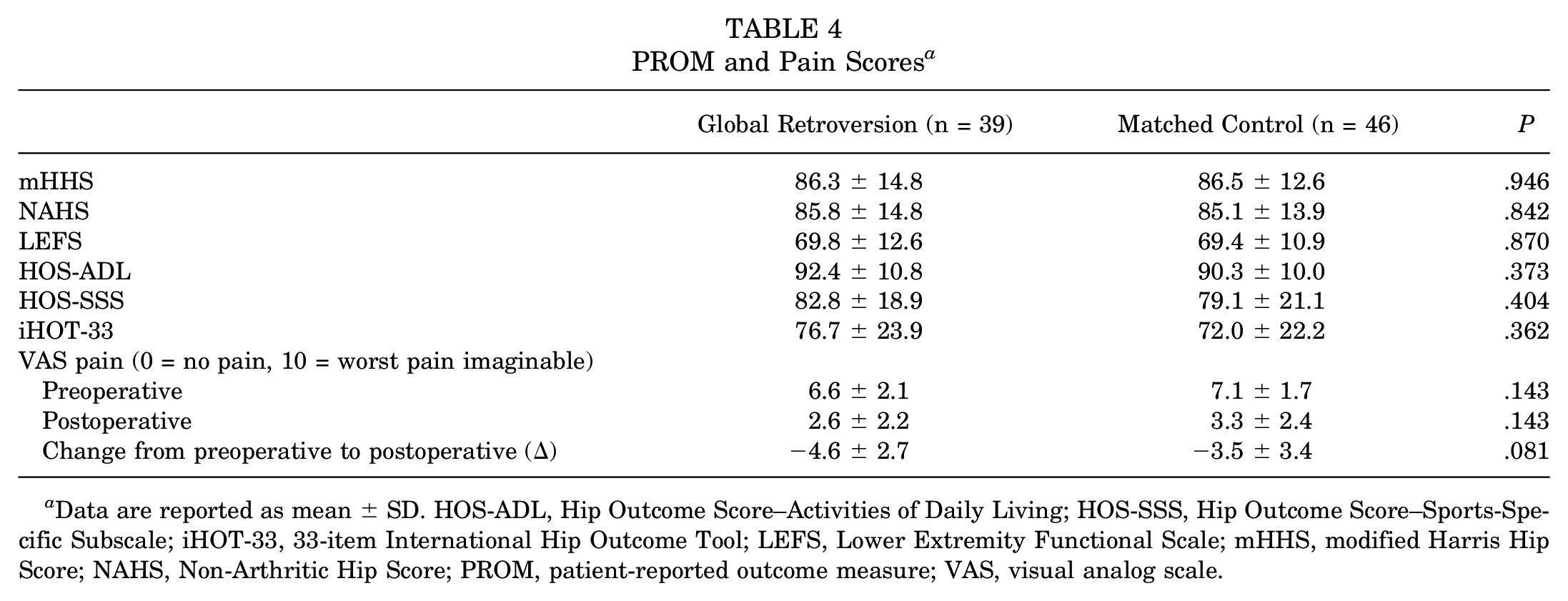
Data are reported as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-33, 33-item International Hip Outcome Tool; LEFS, Lower Extremity Functional Scale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; PROM, patient-reported outcome measure; VAS, visual analog scale.
On univariate analysis, patients with a minimum 10-year follow-up in the global retroversion group showed no significant differences in the rates of achieving the 10-year PASS: mHHS (65.2% vs 62.5%, respectively; P > .999), HOS-ADL (82.7% vs 91.3%, respectively; P = .665), and HOS-SSS (56.5% vs 65.2%, respectively; P = .763). Furthermore, multivariate logistic regression, controlling for global acetabular retroversion and Tönnis grade, identified that patients with global acetabular retroversion did not have significantly different rates of achieving the 10-year PASS for the mHHS (P = .827), HOS-ADL (P = .510), or HOS-SSS (P = .516).
VAS pain scores, both preoperatively (6.6 ± 2.1 vs 7.1 ± 1.7, respectively; P = .143) and postoperatively (2.6 ± 2.2 vs 3.3 ± 2.4, respectively; P = .143), did not differ significantly between the global retroversion and matched control groups. The global retroversion and matched control groups achieved similar improvements in the VAS pain score after surgery (−4.6 ± 2.7 vs −3.5 ± 3.4, respectively; P = .081) (Table 4).
Patient Satisfaction
The global retroversion group reported similar rates of overall treatment satisfaction (95.6% vs 83.3%, respectively; P = .091), postoperative regimen satisfaction (87.0% vs 72.9%, respectively; P = .194), and answering “yes” when asked “Would you receive the same treatment again?” (86.7% vs 79.2%, respectively; P = .291) relative to the matched control group (Table 5).
Patient Satisfaction a

Data are reported as n (%).
Discussion
The principal finding of the present study was that patients with global acetabular retroversion had significantly decreased THA-free survivorship at a minimum 8 years after primary hip arthroscopic surgery relative to matched controls (68.6% vs 83.9%, respectively; P = .036). Intraoperatively, patients with global acetabular retroversion had significantly higher rates of severe CLJ breakdown relative to matched controls. Finally, among patients with THA-free survivorship at final follow-up, there were no differences in postoperative PROM scores, VAS pain scores, or patient satisfaction between groups. While previous studies have found that patients with global acetabular retroversion have similar improvements on PROMs after hip arthroscopic surgery to controls,20,35 this is the first study with a long-term follow-up to quantify the risk of conversion to THA in patients with global acetabular retroversion relative to matched controls.
The approach for assessing global acetabular retroversion in the present study should be highlighted. The present study defined global acetabular retroversion as the simultaneous presence of 3 radiographic signs: the crossover sign, the ischial spine sign, and the posterior wall sign. While this definition has been widely applied using preoperative pelvic radiographs in previous studies assessing global acetabular retroversion,12,19,20,28,35 it should be acknowledged that CT remains the gold standard for assessing acetabular retroversion. However, limitations with this approach include increased cost, less universal availability, and higher radiation exposure with standard CT protocols. Furthermore, pelvic radiographs are routinely obtained as part of the preoperative work-up before hip arthroscopic surgery to serve many purposes (eg, to assess advanced degenerative changes and the degree of cam- and/or pincer-type FAI), whereas CT of the bilateral pelvis is less commonly employed and has a reduced role in surgical indications and preoperative planning, highlighting the advantage of using radiographs for the assessment of acetabular retroversion. Additionally, the use of radiographs to characterize global acetabular retroversion based on the presence of all 3 radiographic signs (avoiding overestimation found with the use of only 1 or 2 signs) has gained increasing adoption and has been validated in the literature.16,18
The most notable finding of the present study was that patients with global acetabular retroversion had significantly inferior THA-free survivorship (68.6%) at a minimum 8-year follow-up relative to matched controls (83.9%). Cox multivariate regression further revealed that global acetabular retroversion was a significant predictor of conversion to THA (hazard ratio, 3.94). To date, Maldonado et al 20 and Savage-Elliott et al 35 are the sole studies to assess outcomes after hip arthroscopic surgery for patients with global acetabular retroversion at a longer follow-up. In an assessment of 205 patients with global acetabular retroversion and 205 without global acetabular retroversion, Maldonado et al 20 reported a total of 5 cases of conversion to THA, 3 (1.5%) in the retroversion group and 2 (1.0%) in the control group, with no difference in conversion rates, at a follow-up of 65.24 ± 20.31 and 65.61 ± 17.83 months, respectively. The present study captured more cases of conversion to THA by achieving nearly double the length of follow-up (128.4 ± 25.2 months for global retroversion group and 133.2 ± 33.6 months for matched control group). More recently, Savage-Elliott et al 35 assessed 38 patients with global acetabular retroversion at a mean follow-up of 81.1 ± 9.7 months and 38 matched controls at a mean follow-up of 80.9 ± 8.8 months, finding only 1 patient in each group who converted to THA; this sample size, coupled with the follow-up time, limited the authors’ ability to detect a difference in the rate of conversion to THA. A long-term follow-up enabled the present study to be the first investigation to conduct a primary analysis of THA conversion rates for patients with versus without global acetabular retroversion. The present study's findings, along with past literature, indicate that even though PROM scores may be favorable for patients with global acetabular retroversion, reduced long-term survivorship is an important consideration for patients with this abnormality.
Comparing intraoperative findings, the present study found that patients with global acetabular retroversion had significantly higher rates of severe CLJ breakdown (36.7% vs 14.3%, respectively) than matched controls. Defined as transition zone cartilage on the acetabulum within 5 mm of the labral attachment, 15 the CLJ provides a seamless transition between the fibrocartilaginous labrum and hyaline articular cartilage and exhibits unique histological features 33 that facilitate force transmission and structural continuity under high shear stresses. Cadaveric studies have suggested that the CLJ is essential to maintaining the hip suction seal and that disruption compromises this seal.5,10,30,39 Furthermore, an ovine study by Philippon et al 29 demonstrated that the CLJ did not completely heal within 12 weeks after iatrogenic labral tearing; furthermore, limited healing only occurred via scar extension from the vascularized capsular aspect of the labrum (not from the CLJ itself). Potentially, increased rates of pincer-type FAI (both isolated and mixed-type) in patients with global acetabular retroversion may have damaged the CLJ over time, helping to explain these findings. CLJ breakdown has been demonstrated to portend decreased long-term survivorship, with a recent study of 174 patients undergoing hip arthroscopic surgery finding that 10-year survivorship was significantly inferior for patients exhibiting severe versus mild CLJ breakdown (severe damage: 43.6% vs mild damage: 97.9%; P < .001). 8 This is one potential explanation for inferior long-term survivorship among patients with global acetabular retroversion versus matched controls. Regardless of the mechanism, this finding merits further study to determine how to best treat these patients. Potentially, hip arthroscopic surgery with reverse periacetabular osteotomy may yield optimal outcomes with respect to long-term joint preservation for these patients, but this strategy requires further investigation. Regardless, patients with global acetabular retroversion in the current study converted to THA at 7.5 ± 4.9 years, demonstrating acceptable longevity after hip arthroscopic surgery. These patients should, however, be counseled on the relatively increased risk of subsequent conversion to THA after isolated hip arthroscopic surgery.
Finally, the present study identified no differences in any PROM scores, rates of achieving the 10-year PASS for PROMs (among patients who did not convert to THA), VAS pain scores, or patient satisfaction between the global retroversion and matched control groups. Multiple previous studies have found similar PROM scores at short-term and midterm follow-up for patients with global acetabular retroversion versus controls.12,20,35 The present study confirms this finding at long-term follow-up (mean, 10.9 ± 2.5 years), with no significant difference in any PROM scores or pain levels at final follow-up as well as no differences in the rates of achieving the 10-year PASS for multiple PROMs. PROM scores at final follow-up of patients who converted to THA were excluded from this analysis, which could help to explain this lack of difference. However, similar methodology was employed by Maldonado et al, 20 who also found no difference in scores for 6 PROMs, VAS pain scores, and patient satisfaction between patients with global acetabular retroversion and controls. Despite higher rates of conversion to THA among a subset of patients with global acetabular retroversion, the results of the present study add to previous literature, demonstrating that patients with global acetabular retroversion achieved similar improvements on PROMs to matched controls.
Limitations
Certain limitations of the present study should be noted. First, assessments of global acetabular retroversion in this study were performed using supine pelvic radiographs, which could overestimate or underestimate the rates of retroversion relative to CT. 42 However, as noted, the use of pelvic radiographs has been validated in previous literature assessing the effect of retroversion on hip arthroscopic surgery outcomes.12,19,20,28,35 Similarly, the present study focused on acetabular retroversion; the consideration of femoral version in addition (eg, through the McKibbin index) could provide additional insights. Second, there may have existed significant radiographic variability in the matched control group, as these patients, while lacking all 3 signs indicating “global” retroversion, could have had 0, 1, or 2 of the corresponding radiographic signs. Relatedly, there were some differences (albeit not statistically significant) in radiographic metrics, such as the alpha angle, that were not explicitly controlled for between groups. Third, all patients in the present study underwent hip arthroscopic surgery by the senior surgeon. While this methodology increased internal validity by avoiding intersurgeon variability, it could also reduce the generalizability of our findings. Fourth, the fact that some patients with sufficient time since surgery did not complete the study's surveys may have introduced the potential for selection bias. Finally, because of the retrospective nature and early start date (May 2001) of the study, preoperative PROM scores were not available, limiting our ability to track changes in PROM scores from preoperatively to postoperatively. However, as long-term survivorship was the primary outcome of this study, this limitation did not affect our ability to collect patient characteristics, review intraoperative findings, or assess the association between global acetabular retroversion and rates of conversion to THA.
Conclusion
Patients with global acetabular retroversion had significantly inferior THA-free survivorship at a minimum 8-year follow-up relative to matched controls as well as greater rates of severe CLJ breakdown, despite no statistically significant differences in PROM scores at final follow-up among patients not converting to THA. These findings suggest that global acetabular retroversion on preoperative radiographic assessments may be a valuable predictor of long-term failure after hip arthroscopic surgery.
Footnotes
Acknowledgements
The authors thank the Conine Family Fund for Joint Preservation for its continued research support.
Final revision submitted February 7, 2025; accepted February 27, 2025.
Presented at the interim meeting of the AOSSM, San Diego, California, March 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.D.M. has received research support from the Conine Family Fund for Joint Preservation, education payments from Kairos Surgical, and honoraria from Allergan. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Brigham and Women's Hospital Institutional Review Board (No. 2011P000053).