
Abstract
Background:
Patients are staying active longer and expect to return to sports or continue participating in recreational activities after total shoulder arthroplasty (TSA) for primary glenohumeral osteoarthritis.
Purpose/Hypothesis:
The purpose of this study was to assess the ability of patients to return to recreational sports following TSA. We hypothesized that TSA would allow a high rate of return to recreational sports.
Study Design:
Case series; Level of evidence, 4.
Methods:
All patients who underwent primary TSA by a single surgeon and were at least 2 years out from surgery were included and were studied for their ability to return to recreational activity following surgery between December 2005 and January 2015. Patient-reported outcomes were obtained, including the 12-Item Short Form Health Survey–Physical Component Summary (SF-12 PCS); Single Assessment Numeric Evaluation (SANE); Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) questionnaire; American Shoulder and Elbow Surgeons (ASES) score; and satisfaction scores (10-point scale), preoperatively and at a minimum of 2 years postoperatively. Return-to-sport rates were assessed using a standardized patient-reported outcome questionnaire.
Results:
A total of 165 patients (186 shoulders) that received TSA met the inclusion criteria for the study. Preoperatively, 139 patients (157 shoulders) were involved in recreational sports; 16 (8.6%) shoulders required additional surgical intervention after the index TSA procedure. A significant postoperative increase was noted in the mean ASES (from 48.3 to 87.0; P < .001), QuickDASH (from 41.0 to 15.8; P < .001), SANE (from 49.1 to 81.2; P < .001), and SF-12 PCS scores (from 38.6 to 48.9; P = .004). Of the 157 shoulders in the recreational sports cohort, responses to the survey examining recreational sporting activities after surgery were available for 112 shoulders. The overall rate of return to sport or recreational activity following TSA was 93.7% (105/112 shoulders). The rate of return to recreational sporting activity equal to or better than the preinjury level was 69.7% (78/112 shoulders), while 6.3% (7/112 shoulders) of our cohort reported that they were unable to compete in recreational sports following TSA. Of the patients who participated in predominantly upper extremity sporting activities after TSA, 49% had to modify their postoperative recreational sporting activity because of lifestyle change, pain, weakness, or decreased range of motion.
Conclusion:
Patients undergoing TSA showed excellent postoperative improvement in their outcome scores, satisfaction, and return to athletic activities. Despite the expected decrease in activity levels with the slow progression of osteoarthritis over time until TSA was performed, almost 94% of patients successfully returned to various recreational sporting activities postoperatively. This study showed that return to recreational sports can be achieved at participation levels that are comparable with preoperative levels, but athletes in some sports such as tennis or swimming, which require more intense levels of exercise, are less likely to return to the same participation levels.
The incidence of shoulder arthroplasty has increased over the past few years as the indications have been expanded toward younger and more active patients. 1,9 While joint-preserving approaches may be effective, the durability of nonarthroplasty, arthroscopic, joint-preserving options for glenohumeral primary osteoarthritis remains unknown. Millett and colleagues 15,16 demonstrated excellent clinical results using arthroscopic joint-preserving techniques to improve function and pain relief after a comprehensive arthroscopic management procedure as treatment for glenohumeral osteoarthritis in young and active patients. However, the authors reported progression to total shoulder arthroplasty (TSA) in 26% of the patients within the first 5 years after surgery. Therefore, arthroplasty remains the gold standard of treatment for glenohumeral osteoarthritis. Expanding indications and advancement of implant design parallel a trend and desire in the elderly population to remain active and return to recreational activities, even after TSA. 3
A patient’s desire to return to sports after TSA historically conflicted with the surgeon’s recommendation, which limited patients to low-demand activities to avoid catastrophic failure. Recent studies have surveyed shoulder surgeons about recreational activities they generally allow after arthroplasty 7,12 and have found that most surgeons counsel their patients to refrain from contact or overhead sports, while permitting activities such as running or golf. Reasons for these restrictions included concerns about glenoid loosening, rotator cuff tears after TSA, and general implant failure. 7,12 However, there is a paucity of evidence that critically evaluates return to sport following TSA.
The purpose of this study was to assess patients’ ability to return to recreational activity after TSA. We hypothesized that the rate of return to sport is high regardless of the recreational sporting activity pursued by the patient and that failure rates are low.
Methods
Study Population
This was an institutional review board–approved retrospective outcomes study using prospectively collected data. All patients who underwent primary TSA by the senior surgeon (P.J.M.) between December 2005 and January 2015 and who were at least 2 years out from surgery were eligible for inclusion. No restrictions were placed on the patients’ activities after the rehabilitation period of 4 to 6 months. Some patients were excluded from analysis because they refused to participate or died during the follow-up. Clinical failure was defined as the need for revision TSA or conversion to reverse TSA (RTSA).
Preoperatively and at a minimum of 2 years postoperatively, patient-reported outcomes were obtained, including the American Shoulder and Elbow Surgeons (ASES) score; Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) score; Single Assessment Numeric Evaluation (SANE) score; and 12-Item Short Form Health Survey–Physical Component Summary (SF-12 PCS) score. Postoperative satisfaction scores were also collected (10-point scale, where 1 = highly unsatisfied and 10 = highly satisfied). Additional questions assessed patients’ postoperative ability to return to specific recreational activities. Specific questions asked were the following: How does your pain affect your ability to compete? Responses can be none, only after competing, mild during competing, moderate pain competing, and severe pain prevents competition. With regard to your shoulder, at what grade can you now participate in sports? Responses can be equal to or above my preoperative level, slightly below my preoperative level, moderately below my preoperative level, significantly below my preoperative level, I cannot compete in my usual sport, and I cannot compete in any sport. Painless use of arm for reasonably strong activities. Responses can be waist, chest, neck, head, and overhead. Tell us how difficult your usual recreational activities and your usual sporting activity are to perform for each shoulder. Responses can be normal, somewhat difficult, very difficult, and unable to perform. Have you modified you recreational sporting activity since your surgery? Responses can be yes or no. If yes, please indicate why (multiple choice responses, not mutually exclusive).
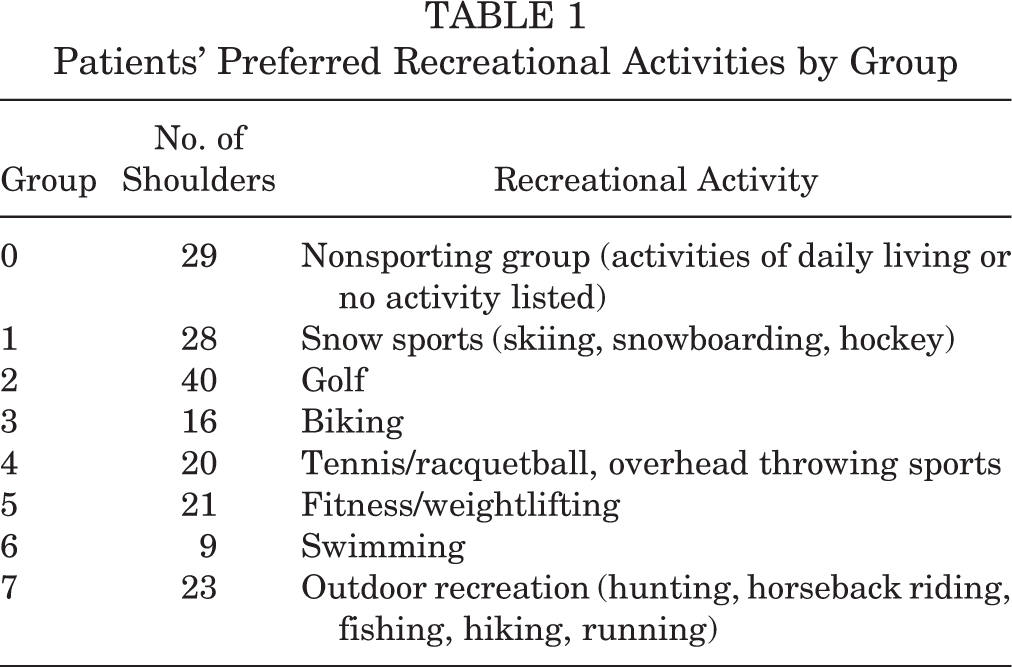
For analysis, nonsporting group, lower extremity sports, and upper extremity sports were grouped accordingly: Nonsporting group (group 0): activities of daily living (including playing with grandchildren, or no activities listed) Lower extremity sports (groups 1 and 7): skiing, snowboarding, horseback riding, hockey, soccer, walking, hiking, running Upper extremity sports (groups 2-6): golf, softball, baseball, mountain biking/cycling, handball, swimming, volleyball, tennis, triathlon, sailing, hunting, ice climbing, yoga, fitness or weight lifting, cross country ski, rancher, farmer, rodeo, kayaking, white water rafting, fishing
Surgical Technique
All surgeries were performed by the senior surgeon using a standard anatomic TSA implant (Apex or Univers II; Arthrex Inc). Surgery was performed with a combination of a peripheral nerve block and general anesthesia; patients were in the beach-chair position, and a pneumatic arm holder was used. Following a standard deltopectoral approach, the subscapularis tendon was released via a lesser tuberosity osteotomy. 19 The humeral head was then exposed, osteophytes were removed, capsular contractures were released, and the head was osteotomized to mimic native version. Next, the glenoid was prepared for component placement, and reaming was performed to achieve desired glenoid version. A pegged glenoid component was then inserted and fixed with cement. Afterward, the humerus was reamed to appropriate sizing, and the stemmed humeral implant was inserted. Finally, the humeral head component was sized and inserted. At this point, the shoulder was reduced and tested for stability. The subscapularis and lesser tuberosity were repaired by use of nonabsorbable sutures passed through the lesser tuberosity bone fragment and through the humeral shaft prior to final seating of the humeral implant. The wound was then thoroughly irrigated and closed in standard layered fashion. 18
Postoperative rehabilitation included immediate full passive range of motion with the exception of external rotation, which was generally limited to 30° for the first 3 weeks postoperatively. At 3 weeks, full active range of motion was permitted. 14 After full range of motion and strength were obtained, full activities were permitted. No restrictions were placed on patients’ recreational, work, or sporting activities after 4 to 6 months. 14
Statistical Analysis
All statistical analyses were performed with SPSS version 11.0. Because all available patients were included, a formal post hoc power analysis was not appropriate. In this data set, continuous variables were nonnormally distributed as confirmed with a Kolmogorov-Smirnov test. Therefore, the pre- and postoperative outcome scores were compared with a Wilcoxon signed-rank test. All results are presented as median and range unless otherwise indicated, and the level of significance was set at P < .05.
Results
Between December 2005 and January 2015, the senior surgeon performed primary TSA on 197 shoulders in 176 patients. After inclusion and exclusion criteria were applied (refusal to participate, affecting 8 shoulders; patient death, affecting 3 shoulders), the final study population consisted of 186 shoulders in 165 patients with a mean age of 64 years (range, 18-82 years) and a mean follow-up of 3.7 years (range, 2-10 years). Details on inclusion and exclusion criteria are outlined in Figure 1. Preoperatively, a total of 157 shoulders (136 patients) of the 186 shoulders (165 patients) were involved in recreational sports. Patient preoperative participation in recreational activities is detailed in Table 1.

Flow chart showing the patient population for this study after accounting for inclusions, exclusions, clinical failures, and those lost to follow-up. Patients progressing to another arthroplasty (reverse total shoulder arthroplasty [TSA] or revision TSA) were defined as clinical failures.
Patients’ Preferred Recreational Activities by Group
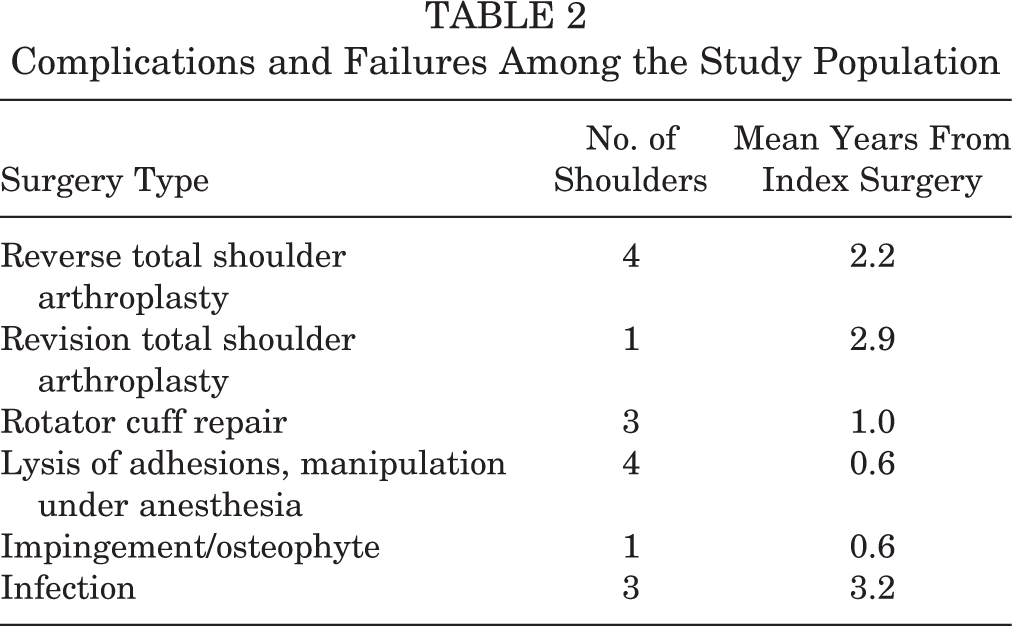
Sixteen patients (16 shoulders) experienced complications following the index surgery (Table 2). Among these, 4 patients advanced to RTSA and 1 patient required revision TSA due to glenoid loosening. Of the remaining 11 patients, 7 required revision surgery due to adhesions or rotator cuff tears, 1 had a revision subacromial decompression with osteophyte removal, and 3 experienced superficial postoperative infections and were treated with a series of surgical irrigation and debridements along with antibiotic treatments.
Complications and Failures Among the Study Population
Postoperative outcome scores (Table 3 and Figure 2) were collected from 169 patients (181 shoulders) (93.0%) with a mean follow-up of 3.7 years (range, 2-10 years). Significant preoperative to postoperative increases were noted in the mean ASES (from 48.3 to 87.0; P < .001), QuickDASH (from 41.0 to 15.8; P < .001), SANE (from 49.1 to 81.2; P < .001), and SF-12 PCS (from 38.6 to 48.9; P = .004). Median satisfaction after surgery was 10 out of 10 points. Furthermore, the type of recreational activity did not affect postoperative outcome scores (P > .05) (Table 3).
Pre- Versus Postoperative Outcome Scores of the Study Population a

a Continuous data presented as mean (range). ASES, American Shoulder and Elbow Surgeons; QuickDASH, Quick Disabilities of the Arm, Shoulder, and Hand; SANE, Single Assessment Numeric Evaluation; SF-12 PCS, 12-Item Short Form Health Survey Physical Component Summary.
b Statistically significant difference.

Graphic representation of pre- versus postoperative American Shoulder and Elbow Surgeons (ASES) and Single Assessment Numeric Value (SANE) scores among the different activity groups. See Table 1 for definitions of group numbers.
A total of 157 shoulders (136 patients) of the 181 shoulders (160 patients) were involved in recreational sports preoperatively. In the recreational sports cohort, which consisted of 157 shoulders (136 patients), responses to the survey examining recreational sporting activities after surgery were available for 112 shoulders (95 patients) (Figure 1). The overall rate of return to sport or recreational activity (question 5) in the cohort following TSA was 93.7% (105/112 shoulders). The rate of return to recreational sporting activity at a level equal to or better than the preoperative level following TSA was 69.7% (78/112 shoulders), while 6.3% (7/112 shoulders) of the cohort reported they were unable to compete in recreational sports following TSA. No significant difference was found between the postoperative outcome scores among patients who did versus did not participate in sports (Table 4). Significant correlations with postoperative level of sports participation and satisfaction with surgical outcomes were found (rho = –0.562; P < .001), indicating that those who were able to compete at their presurgical level were more satisfied.
Postoperative Outcomes Comparing Patients Participating in Sports Versus Those Not Participating in Sports a

a Scores are presented as mean (range). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation.
All patients experienced significant improvement from preoperative to postoperative assessment regardless of whether the recreational sporting activity was predominantly lower or upper extremity dominant (P < .001) (Table 5). In the nonsporting group, 30% of patients indicated that they modified their recreational activity after TSA (Table 6). Of the patients participating in predominantly lower extremity sporting activities after TSA, 45% had to modify their activities following surgery (Table 6). Of the patients participating in predominantly upper extremity sporting activities after TSA, 49% had to modify their postoperative recreational sporting activity (Table 6). This indicates that more than 50% of patients in each group did not modify their recreational activity. However, patients who indicated that they had modified their recreational activity were significantly older than those who had not (67 ± 7.1 vs 61 ± 9.8 years, respectively; P < .000).
Sport-Specific Questions Related to Return to Upper Versus Lower Extremity Sports Activity Following Total Shoulder Arthroplasty a
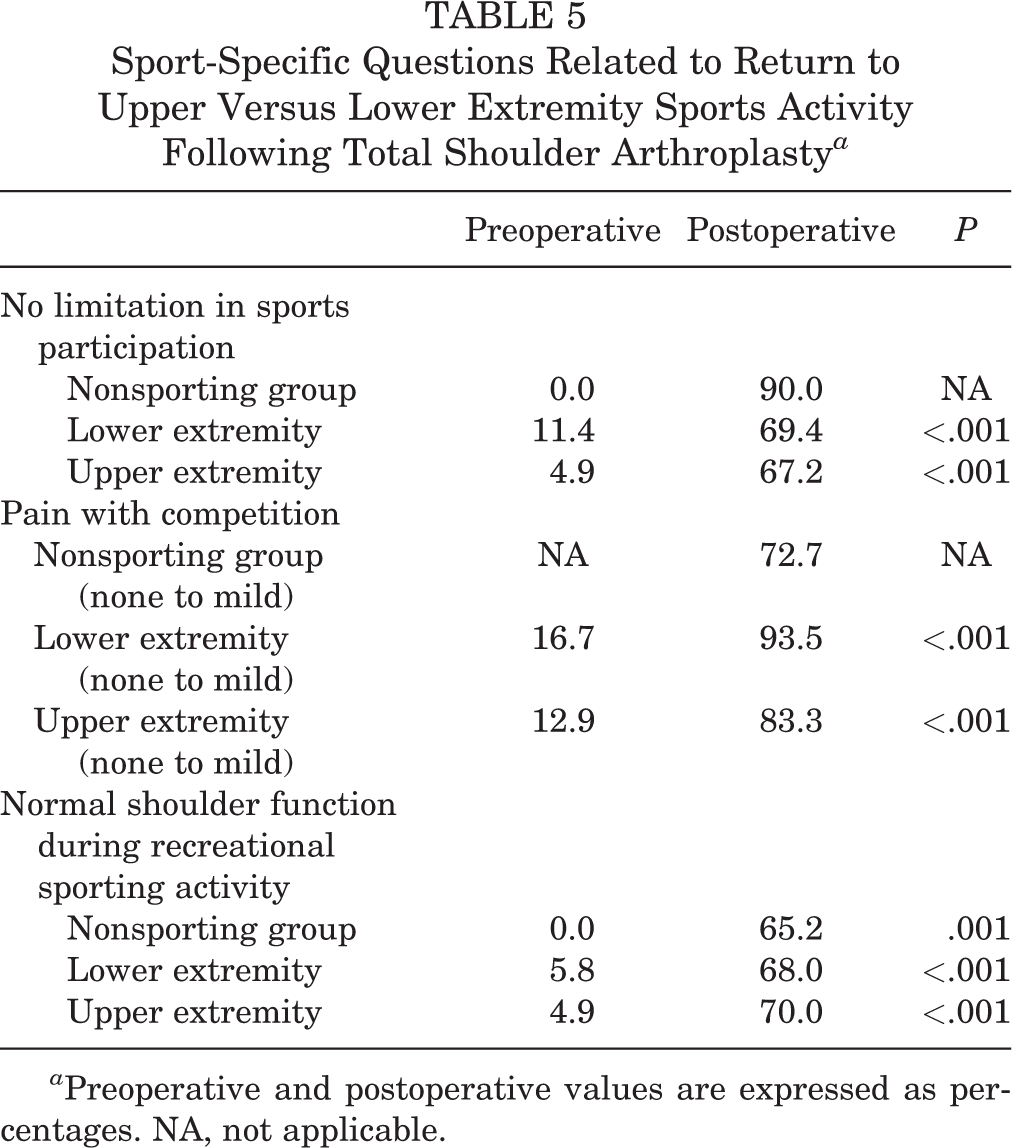
a Preoperative and postoperative values are expressed as percentages. NA, not applicable.
Modified Recreational Sporting Activity Since Total Shoulder Arthroplasty Surgery a

a Values are expressed as percentages.
Discussion
The important finding of our study was the high rate of return to activity after TSA. All patients experienced significant improvement from preoperative to postoperative assessment regardless of specific sporting activity performed. In our postoperative protocol for TSA, there is no activity restriction after a typical 4- to 6-month postoperative recovery and rehabilitation program. In our cohort, the lack of restriction on activity after an initial recovery period did not seem to relate to early loosening of the TSA prosthesis or rotator cuff tears in our short-term clinical experience, with only 1 (0.6%) patients revised for glenoid loosening. Further long-term follow-up is needed to determine whether our lack of postoperative restrictions affects TSA survivorship.
Patients undergoing total joint arthroplasty increasingly desire to participate in sports and recreational activities following surgery. 4,22,23 Comparing hemiarthroplasty and TSA, Garcia et al 5 demonstrated that TSA led to improved rates of return to sports. In our study, patients undergoing primary TSA generally had improvements in pain and function following surgical reconstruction based on their preoperative baseline (Tables 3-6; Figure 2). Regardless of the recreational sport, a certain percentage of the assessed patients undergoing TSA had to modify their activities (Table 7). However, at least 50% of each sports cohort stated they were able to return to their recreational activities at a level comparable with their preinjury level (Table 7). In only 3 of the cohorts (patients whose primary sports and recreational activities included tennis, racquetball, overhead throwing sports [21.4%]; fitness/weightlifting [9.1%]; or swimming [16.6%]) did athletes indicate that they were unable to participate in their primary sporting or recreational activities after surgery (Table 7). All other cohorts of patients in the subanalysis were able to participate in sporting and recreational activities after surgery, although some required modification or participation below preinjury level (Table 7).
Ability to Return to Sport and Level of Participation Among the Different Activity Groups a
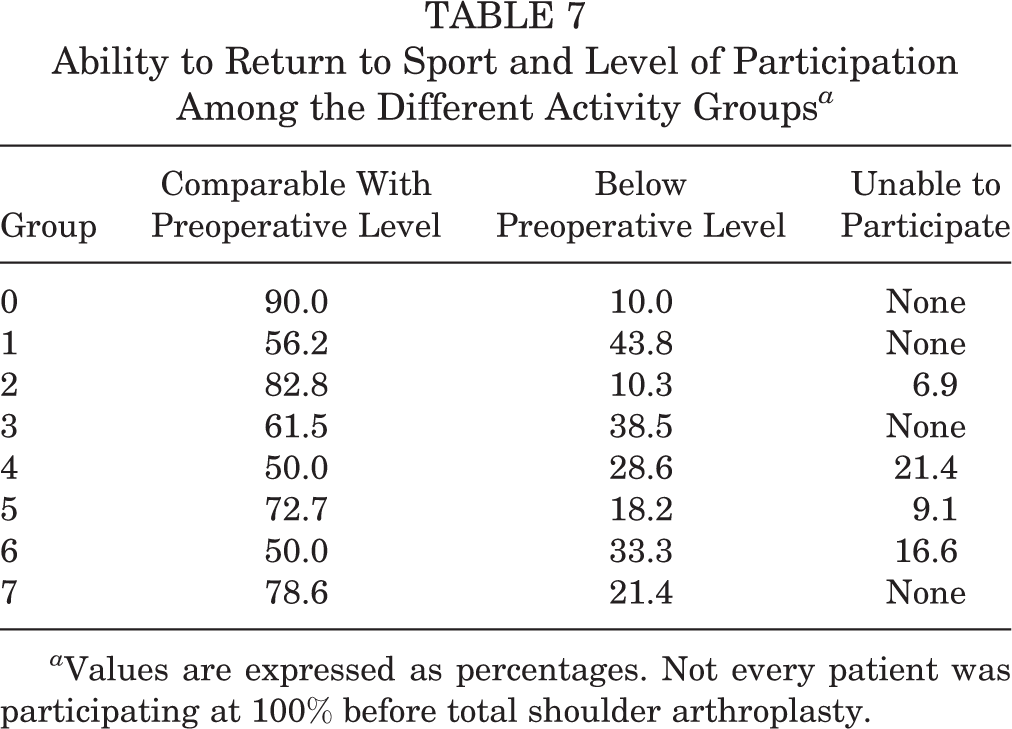
a Values are expressed as percentages. Not every patient was participating at 100% before total shoulder arthroplasty.
In general, certain sporting activities may lend themselves to successful return after arthroplasty. In a systematic review performed by Papaliodis et al, 17 the authors found that, based on sport-specific assessment, golfers were able to return to sport following total joint arthroplasty of the knee, shoulder, or hip with improvement in participation. Our current study supports this previously published report, as not all patients returned to preparticipation levels of recreational and sporting participation at equally successful rates (Table 7).
Garcia et al 6 found that in patients younger than 55 years who underwent TSA, 96.4% were able to return to previous sporting activity, and no patients required revision of the glenoid component with an average of 61 months of follow-up. Interestingly, Liu et al 10 studied return to sport following hemiarthroplasty or RTSA. They found that both the hemiarthroplasty and RTSA cohorts were able to return to recreational sporting activities, but the RTSA groups significantly outperformed the hemiarthroplasty group in patient-oriented pain outcomes and rates of return to sport. 10 In a comparison of return to sport following TSA, RTSA, and hemiarthroplasty, Johnson et al 8 found that the TSA group (75%-100%) returned to sports at a higher rate than the RTSA (75%-85%) and hemiarthroplasty (67%-76%) groups. Similar rates of return to sport following shoulder arthroplasty and conclusions were found by a separate systematic review and meta-analysis performed by Liu et al. 11
In the present study, sports participation significantly improved from preoperative baseline following TSA when patients were asked whether their sports participation was comparable with their preinjury level (P < .001) (Table 5). The rates of return to lower extremity sports and upper extremity sports following TSA in the present study were 69.4% and 67.2%, respectively (Table 5). These rates are similar to those identified in a systematic review of the most recent literature, which stated that 85.1% of patients were able to return to play and 72.3% were able to return at an equivalent or improved level of play. 11 However, 83.3% of TSA patients who participated in upper extremity–dominant sports and 93.5% of TSA patients who participated in lower extremity–dominant sports had no pain to mild pain postoperatively (Table 5). The most important finding of our study was that 70% of patients were able to return to sporting activity with no limitations by the treating physician. While the demands of various sports differ for each group, most were able to return to their desired sport. Tennis players and swimmers, with the highest demand on their shoulders, had the highest number who were unable to participate in their sport postoperatively. Golfers fared better, with almost 83% able to return to preoperative levels. Surprisingly, 25% of patients involved in lower extremity sports modified their sport because of weakness or decreased range of motion, although shoulder function was not expected to play a big role. As none of the patients in this study participated in contact sports, questions remain regarding whether return to contact sports is advisable. However, patients who continued participation in recreational activity without modification were about 6 years younger than those who did not (61 ± 9.8 vs 67 ± 7.1 years; P < .000).
Other studies of return to sport following TSA have similarly reported high rates of patients returning to recreational activity postoperatively. 5,6,13,17,21 The data from the present study support high patient satisfaction following TSA, with a relatively high rate of return to sporting and recreational activity regardless of whether the preferred sporting activity is lower extremity or upper extremity dominant.
Limitations
Despite the addition of our large cohort to the literature on return to sport and recreational activity after TSA, our study has limitations. First, this study was performed retrospectively on a prospectively collected database, but there may be some bias because not every patient answered every question, leading to a greater than 20% nonresponse rate. 2,20 Further, this study consists of a single surgeon’s experience at a referral practice center with highly motivated and active patients, and the results may not be generalizable to other surgical practices or patient populations. Another bias of this study is that high-demand patients meeting the clinical indications for a TSA may have been offered an alternative procedure pioneered by the senior author that addresses the pain generators in an osteoarthritic shoulder. 16 Additionally, there was no control group aside from historical controls and the preoperative baseline that was collected on each of the patients. A strength of this study is the large number of patients in the study cohort with excellent follow-up. Some of the subanalyses of specific sports activities were small compared with the larger cohorts in the study; however, analysis based on predominantly upper versus lower extremity sporting or recreational activity participation enabled larger cohort subanalysis. The mean follow-up of 3.7 years (range, 2-10 years) may not be sufficient to detect postoperative complications such as glenoid loosening or rotator cuff tear in the TSA population, who were not given any restrictions in their activities after their initial postoperative rehabilitation period.
Conclusion
Patients undergoing TSA showed excellent postoperative improvement in their outcome scores, satisfaction, and return to athletic activities. Despite the expected decrease in activity levels with the slow progression of osteoarthritis over time until a TSA is performed, almost 94% of patients successfully returned to various recreational sporting activities postoperatively. This study showed that patients can return to recreational sports at participation levels comparable with preoperative levels, but participants in some sports such as tennis or swimming, which require more intense levels of exercise, are less likely to return to the same participation levels.
Footnotes
Presented at the American Orthopaedic Society for Sports Medicine Annual Meeting, Toronto, Ontario, Canada, July 2017.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by the Steadman Philippon Research Institute, which is a 501(c)(3) nonprofit institution supported financially by private donations and corporate support from the following entities: Smith & Nephew Endoscopy, Arthrex, Siemens Medical, Ossur Americas, and Vail Valley Medical Center. S.M. has received educational support from Smith & Nephew and has grants/grants pending from DJO. S.J.F. has received educational support from Smith & Nephew and has grants/grants pending from DJO. J.A.G. has received educational support from Arthrex and Smith & Nephew and has grants/grants pending from DJO. J.P. has received educational support from Arthrex. P.J.M. is a consultant for Arthrex, receives royalties from Arthrex and MedBridge, has received hospitality payments from Arthrex, and has stock/stock options in VuMedi and Game Ready.
Ethical approval for this study was obtained from Vail Valley Medical Center (2002-03).