
Abstract
Background:
The combination of a glenoid defect and a Hill-Sachs lesion in a shoulder with anterior instability has recently been termed “bipolar bone loss,” but the prevalence and influence of this condition on postoperative recurrence after arthroscopic Bankart repair are still unclear.
Purpose:
To investigate bipolar bone loss in male athletes using a new scoring system and to evaluate its efficacy by comparing it with the glenoid track concept.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
The sizes of both lesions were evaluated retrospectively in 80 male athletes (85 shoulders) using computed tomography. The glenoid defects and the length, width, and depth of the Hill-Sachs lesions were classified into 5 size categories and were allocated scores from “0” for no defect to “4” for the largest defect. Patients were then classified into 5 classes according to the total score for both lesions: class 1, 0-1 point; class 2, 2 points; class 3, 3 points; class 4, 4 points; and class 5, ≥5 points. The prevalence of bipolar bone loss and postoperative recurrence rates for patients with at least 2 years of follow-up were compared among the classes. The recurrence rate for each class was also compared between shoulders with an off-track lesion and shoulders with an on-track lesion as well as among 3 sporting categories: rugby, American football, and other sports.
Results:
Based on the combination of glenoid defect size and Hill-Sachs lesion length, the postoperative recurrence rate was 0% for shoulders in class 1, 12.5% for class 2, 33.3% for class 3, 28.6% for class 4, and 31.3% for class 5, while the recurrence rates were 0%, 16.7%, 28.6%, 27.3%, and 31.6%, respectively, for the combination of glenoid defect size and Hill-Sachs lesion width and 0%, 8.3%, 26.7%, 28.6%, and 35.3%, respectively, for the combination of glenoid defect size and Hill-Sachs lesion depth. Postoperative recurrence was frequently recognized regardless of the presence of off-track Hill-Sachs lesions. No recurrence was recognized in class 1 shoulders among rugby players, in classes 1 and 2 among American football players, and in classes 1 through 3 among other athletes based on the combination of glenoid defect size and Hill-Sachs lesion size.
Conclusion:
Our scoring system for bipolar bone loss was useful to evaluate the influence on postoperative recurrence in male athletes. The postoperative recurrence rate was influenced by the extent of bipolar bone loss and the sporting category regardless of the presence of off-track lesions.
Glenoid defects and Hill-Sachs lesions have long been recognized at the time of treating anterior shoulder instability. They have recently been categorized as bipolar bone loss, which is one of the significant risk factors for postoperative recurrence after stabilization surgery, especially after arthroscopic Bankart repair. Burkhart and De Beer 2 reported that patients with large bone defects, such as an inverted-pear glenoid and an engaging Hill-Sachs lesion, were not candidates for arthroscopic Bankart repair because of frequent postoperative recurrence of instability. Yamamoto et al 19 defined the zone of contact between the glenoid and the head of the humerus as the glenoid track (GT) and assessed the risk of a Hill-Sachs lesion engaging the glenoid rim with or without a glenoid defect based on this concept. The width of the GT is reduced in patients with a glenoid defect, so this concept enables clinicians to consider both lesions when assessing shoulders with anterior instability. Di Giacomo et al 3 proposed the concept of bipolar bone loss to describe varying degrees of bone loss affecting both the glenoid and the proximal humerus. They emphasized the importance of geometric interplay between these 2 sites of bone loss when developing logical criteria for surgical treatment based on the GT concept and stated that conversion of an off-track Hill-Sachs lesion to an on-track lesion is essential for stabilizing a shoulder with anterior instability. Recently, it has come to be considered that an assessment of bipolar bone loss is essential when planning surgery for traumatic anterior shoulder instability. 3,19
Finite element analysis and cadaveric studies by Walia et al 16 –18 and Arciero et al 1 reported that combined glenoid and humeral head defects have an additive negative effect on glenohumeral stability. However, there have been few clinical studies on the critical extent of bipolar bone loss for postoperative recurrence of instability. There has been no simple method to evaluate various combinations of bipolar bone loss other than the GT concept. Nakagawa et al 14 investigated the relationship between glenoid defects and Hill-Sachs lesions in shoulders with traumatic anterior instability. They reported that while the presence of both lesions significantly influenced postoperative recurrence of instability after arthroscopic Bankart repair, the size of the combined lesions did not have a significant influence. In their study, as glenoid defects and Hill-Sachs lesions were each divided into 5 size categories, the extent of bipolar bone loss was divided into a total of 25 size categories, so it was difficult to analyze their results because of the small numbers in each category.
In the present study, we developed a method that allowed the influence of various combinations of bipolar bone loss on postoperative recurrence to be compared simply and easily using an original scoring system for the extent of bipolar bone loss and a categorization into 5 classes based on the total score. We hypothesized that this scoring system could clearly show that the combination of larger lesions was associated with a higher risk of postoperative recurrence. Furthermore, we hypothesized that the evaluation of bipolar bone loss using our scoring system would significantly correlate with an evaluation using the GT concept. Thus, the first purpose of the present study was to evaluate the efficacy of our scoring system for bipolar bone loss by comparison with the GT concept.
Another possible explanation for the lack of correlation between combined lesion size and recurrent instability in the report by Nakagawa et al 14 is that most of their patients were young athletes and many were involved in collision sports such as rugby and American football, which may have increased the risk of recurrence after arthroscopic Bankart repair. Therefore, we also hypothesized that the influence of bipolar bone loss on postoperative recurrence in male athletes after arthroscopic Bankart repair may be different among several sporting categories. Accordingly, the second purpose of the present study was to assess the influence of sporting category on postoperative recurrence in each class of bipolar bone loss according to our scoring system.
Methods
This was a retrospective investigation of prospectively collected clinical data, and institutional review board approval was obtained. The participants were 80 consecutive male athletes (85 shoulders) who underwent arthroscopic Bankart repair for traumatic anterior shoulder instability at our hospital between January 2010 and December 2013 and who had been evaluated for glenoid defects and Hill-Sachs lesions by preoperative computed tomography (CT). During the study period, arthroscopic Bankart repair was performed without additional reinforcement procedures for all patients, including patients with a large glenoid defect. All patients were male athletes playing at a competitive level. Female patients, those not playing sports or playing at the recreational level, and those with recurrent instability after previous anterior stabilization surgery were excluded.
The mean age at the time of primary trauma was 17.4 years (range, 14-26 years), the mean age at surgery was 18.5 years (range, 14-27 years), and the mean number of instability events was 7.7 (range, 1-80) (1-5: 53 shoulders; 6-10: 20 shoulders; ≥11: 12 shoulders). The sports played by the male athletes were rugby (34 shoulders), American football (27 shoulders), baseball (7 shoulders), basketball (4 shoulders), judo (3 shoulders), martial arts (2 shoulders), wrestling (2 shoulders), soccer (2 shoulders), ice hockey (1 shoulder), handball (1 shoulder), water polo (1 shoulder), and naginata (similar to kendo; 1 shoulder). The athletes were attending junior high school (7 shoulders), high school (36 shoulders), or college (35 shoulders), and there were also 7 semiprofessional athletes.
While CT was usually performed at the first visit to our hospital, patients who underwent surgery a long time after the first CT scan were evaluated by CT again just before the operative procedure. CT and the reconstruction of images were performed with a whole-body scan (spiral scan, 0.5-mm slice thickness, 0.3-mm reconstruction, and 3-dimensional [3D] edit mode) with the patient lying supine in the center of the gantry table and the affected arm in the neutral position. Data in digital imaging and communications in medicine mode from the CT scans were analyzed with analysis software to perform multiplanar reconstruction.
To quantify the glenoid defect, the inferior portion of the glenoid rim was approximated to a true circle on en face 3D-CT scans that had been reconstructed with elimination of the humeral head. 10 –13 The extent of the glenoid defect was calculated as a percentage of the glenoid rim length by the equation B/A × 100%, where A is the diameter of the fitted circle and B is the width of the defect (Figure 1A). A Hill-Sachs lesion was diagnosed if an abnormal groove was detected on the posterolateral aspect of the head of the humerus. To assess the size of Hill-Sachs lesions according to the Nakagawa et al 14 and Ozaki et al 15 method, the length and width were measured on 3D-CT scans that had been reconstructed with elimination of the scapula (Figure 1B). Measurement of the length and width of each lesion was performed using en face 3D-reconstructed images that showed the Hill-Sachs lesion. The most superolateral point and the most inferomedial point of the Hill-Sachs lesion were plotted on the en face view, and a line connecting these 2 points was defined as the major axis of the lesion. Then, the longest line connecting the medial and lateral edges of the lesion perpendicular to the major axis was defined as the minor axis. Next, the lengths of the major axis and minor axis were measured to determine the length and width of the lesion, respectively. The depth of the Hill-Sachs lesion was measured on axial images obtained perpendicular to the longitudinal axis of the humeral shaft (Figure 1C). A circle was drawn that included the articular surface of the humeral head, and the depth was determined as the longest distance between the base of the lesion and this circle. The humeral head diameter was defined as the diameter of the circle on the axial slice with the largest circle. Then, each measurement was calculated as a percentage of the humeral head diameter.

Quantification method for glenoid defect size and Hill-Sachs lesion size. (A) The inferior portion of the glenoid rim was approximated to a true circle on en face 3-dimensional computed tomography (CT) scans that were reconstructed with elimination of the humeral head. The extent of the glenoid defect was calculated as a percentage of the glenoid rim length (B/A × 100%), where A is the diameter of the fitted circle and B is the width of the glenoid defect. (B) The length (L) and width (W) of Hill-Sachs lesions were measured on 3-dimensional CT scans that had been reconstructed with elimination of the scapula. The most superolateral point and the most inferomedial point of the Hill-Sachs lesion were plotted on the en face view, and a line connecting these 2 points was defined as the major axis of the lesion. Then, the longest line connecting the medial and lateral edges of the lesion perpendicular to the major axis was defined as the minor axis. Next, the lengths of the major axis and minor axis were measured to determine the length and width of the lesion, respectively. (C) The depth (D) of Hill-Sachs lesions was measured on axial images obtained perpendicular to the longitudinal axis of the humeral shaft. On an axial CT image, a circle was drawn that included the articular surface of the humeral head, and the depth of the Hill-Sachs lesion was determined as the longest distance between the base of the lesion and this circle. The humeral head diameter was defined as the diameter of the circle on the axial slice with the largest circle. Then, each measurement was calculated as a percentage of the humeral head diameter.
To determine whether a Hill-Sachs lesion was on-track or off-track, first, the width of the GT was calculated by the following formula according to the method by Di Giacomo et al 3 : GT = 0.83 × A (glenoid diameter) – B (glenoid defect). Then, the length between the rotator cuff attachments and the medial aspect of the Hill-Sachs lesion was measured as the Hill-Sachs interval (HSI) (Figure 2). If HSI > GT, the Hill-Sachs lesion was determined as an off-track lesion, and if HSI < GT, it was determined as an on-track lesion.

Definition of the Hill-Sachs interval (HSI). The HSI is defined as the length between the rotator cuff attachments and the medial aspect of the Hill-Sachs lesion. FP, footprint of rotator cuff attachment; HS, Hill-Sachs lesion; L1, medial margin of rotator cuff attachment; L2, medial aspect of Hill-Sachs lesion.
After the above-mentioned data were obtained, bipolar bone loss in male athletes was investigated as follows. First, glenoid defects and Hill-Sachs lesions were classified into 5 categories according to the size of the bone defects, referring to the criteria of Nakagawa et al, 14 and were allocated scores from “0” for no defect to “4” for very large defect (Table 1). Then, to combine the sizes of the glenoid defect and the Hill-Sachs lesion, the scores for both lesions were summed, and the patients were classified into 5 classes according to the total score: class 1, 0-1 point; class 2, 2 points; class 3, 3 points; class 4, 4 points; and class 5, ≥5 points (Figure 3).
Categories and Scores by Size of Bone Defects According to Nakagawa et al 14 a

a Values are shown as percentages.

Classification of bipolar bone loss according to the total score of glenoid defect size and Hill-Sachs lesion size: class 1 (0-1 points), class 2 (2 points), class 3 (3 points), class 4 (4 points), and class 5 (≥5 points).
First, the prevalence of bipolar bone loss in male athletes was investigated. Then, postoperative recurrence rates of instability after arthroscopic Bankart repair for patients with at least 2 years of follow-up were compared for each glenoid defect size and each Hill-Sachs lesion size and were also compared among the classes of bipolar bone loss. Postoperative recurrence was defined as any report of a dislocation or subluxation. Furthermore, to clarify the relationship between our scoring system for bipolar bone loss and the GT concept, the postoperative recurrence rate in shoulders with an off-track lesion was compared with the recurrence rate in shoulders with an on-track lesion for each class of bipolar bone loss. Finally, the postoperative recurrence rate for each class of bipolar bone loss was compared among 3 sporting categories: rugby, American football, and other sports.
Operative Procedures and Postoperative Rehabilitation
All operative procedures were performed in the lateral decubitus position by a single surgeon (S.N.). Arthroscopic Bankart repair was performed by the single-row suture anchor fixation technique. The anteroinferior glenohumeral ligament (AIGHL)–labral complex was detached and mobilized from the glenoid neck to the 6-o’clock position. Because the aim of Bankart repair is to avoid residual capsular redundancy by elevating the AIGHL-labral complex, capsuloligamentous tissue was separated up to the 7-o’clock position in the right shoulder if mobilization was inadequate or capsular laxity was severe. To accelerate union of the anterior labrum with the glenoid, the anterior 3 to 4 mm of the articular cartilage on the glenoid was resected. Then, 4 to 7 suture anchors were placed at the anterior bone trough created in the glenoid. Screw-in metallic suture anchors (FASTak; Arthrex) were used until June 2011, and soft anchors (JuggerKnot; Zimmer Biomet) have been used since July 2011. Because of their smaller diameter and easier insertion, more anchors have been inserted in each shoulder after introduction of the JuggerKnot soft anchor (5-7 anchors vs 4-6 FASTak anchors) regardless of sporting category. 7 For the treatment of bony Bankart lesions, arthroscopic bony Bankart repair was performed without resection of the fragment. 10,12 Bony Bankart lesions were identified during surgery and were repaired in 38 shoulders among 55 shoulders with a glenoid defect. Even in shoulders with a large glenoid defect, no bone grafting or rotator interval closure was performed during the study period. No patients had isolated capsular tears or isolated humeral avulsions of the glenohumeral ligament (HAGLs). However, capsular tears and HAGLs were repaired simultaneously with the arthroscopic Bankart procedure in patients with Bankart lesions. 8 If the patient had a HAGL, the capsular attachment of the humeral head was refreshed, and the lesion was repaired with 2 or 3 single-loaded suture anchors. Remplissage or bone grafting was not performed even for a large Hill-Sachs lesion.
Patients wore a brace (allowing 90° of internal rotation and 0° of abduction) for 4 weeks postoperatively and started passive range-of-motion exercises after 2 weeks. Until 4 weeks after surgery, flexion and external rotation with the arm at the side were restricted to 150° and 30°, respectively, but no restriction was required after 4 weeks. Return to contact training and competition was not permitted for at least 6 months and 8 months after surgery, respectively.
Statistical Analysis
Statistical analysis was performed with the Fisher exact probability test, the unpaired Student t test, and 1-factor analysis of variance, as appropriate, and significance was accepted at P < .05.
Results
Prevalence of Bipolar Bone Loss in Male Athletes
A glenoid defect was recognized in 55 shoulders (64.7%), and the mean size in 85 shoulders was 9.2% (range, 0%-28.5%). On the other hand, a Hill-Sachs lesion was recognized in 60 shoulders (70.6%), while the mean length was 28.5% (range, 0%-70.5%), its mean width was 15.3% (range, 0%-39.4%), and its mean depth was 6.8% (range, 0%-17.3%). A combination of both lesions was recognized in 43 shoulders (50.6%), while an isolated glenoid defect and an isolated Hill-Sachs lesion were recognized in 12 shoulders (14.1%) and 17 shoulders (20.0%), respectively. Neither a glenoid defect nor a Hill-Sachs lesion was recognized in 13 shoulders (15.3%). The prevalence of bipolar bone loss according to our scoring system is shown in Table 2. The incidence of shoulders in each class was almost similar and was approximately 20% for all combinations of the glenoid defect size and the length, width, and depth of the Hill-Sachs lesions.
Prevalence of Bipolar Bone Loss According to Our Scoring System

Influence of Each Glenoid Defect Size and Hill-Sachs Lesion Size on Postoperative Recurrence of Instability
There were 75 shoulders with at least 2 years of postoperative follow-up. Fifteen of these shoulders (20.0%) experienced a recurrence of instability.
Postoperative recurrence rates for each glenoid defect size and Hill-Sachs lesion size are shown in Tables 3 and 4. Recurrent instability was seen in only 1 shoulder without a glenoid defect (3.7%), while it occurred in 29.2% of shoulders with a glenoid defect regardless of their size. Postoperative recurrence rates were significantly different among the 4 defect size groups (P = .0278), and there was also a significant difference between the presence and absence of a glenoid defect (P = .0075). Similarly, recurrent instability was seen in only 1 shoulder without a Hill-Sachs lesion (4.5%), while recurrence was seen in 26.4% of shoulders with a Hill-Sachs lesion regardless of their size. Postoperative recurrence rates were not significantly different among the 5 classes based on the length, width, and depth of the Hill-Sachs lesion (length: P = .0785; width: P = .157; depth: P = .115) and also did not reach significance between shoulders with and without a Hill-Sachs lesion (P = .0535).
Postoperative Recurrence Rates for Each Glenoid Defect Size

Postoperative Recurrence Rates for Each Hill-Sachs Lesion Size

Influence of Bipolar Bone Loss on Postoperative Recurrence of Instability
Recurrence rates for each class were also compared according to the combined sizes of the glenoid defect and Hill-Sachs lesion using our scoring system (Table 5). When the glenoid defect and the length of the Hill-Sachs lesion were assessed, the recurrence rates were 0% for shoulders in class 1 (0-1 point), 12.5% for class 2 (2 points), 33.3% for class 3 (3 points), 28.6% for class 4 (4 points), and 31.3% for class 5 (≥5 points). When the glenoid defect and the width of the Hill-Sachs lesion were assessed, the recurrence rates were 0% for shoulders in class 1, 16.7% for class 2, 28.6% for class 3, 27.3% for class 4, and 31.6% for class 5. When the glenoid defect and the depth of the Hill-Sachs lesion were assessed, the recurrence rate was 0% for shoulders in class 1, 8.3% for class 2, 26.7% for class 3, 28.6% for class 4, and 35.3% for class 5. Accordingly, no recurrence was recognized solely in shoulders with a score ≤1 point for any combination of the glenoid defect size and the length, width, and depth of Hill-Sachs lesions. There was a significant difference between shoulders with a score ≤1 point versus a score ≥2 points (glenoid defect and Hill-Sachs lesion length: P = .0167; width: P = .0086; depth: P = .0167) and between shoulders with a score ≤2 points versus a score ≥3 points (P = .0087, .0182, and .0061, respectively). There was no significant difference in the recurrence rates of shoulders with 3, 4, or 5 points.
Postoperative Recurrence Rates for Each Class of Bipolar Bone Loss

Relationship Between Our Scoring System and the GT Concept
Off-track Hill-Sachs lesions were recognized in 9 shoulders (12.0%) among 75 shoulders with at least 2 years of follow-up. Postoperative recurrence was recognized in 3 (33.3%) of 9 shoulders with an off-track lesion and 12 (18.2%) of 66 shoulders with an on-track lesion. There was no statistically significant difference between shoulders with an off-track lesion and shoulders with an on-track lesion (P = .372).
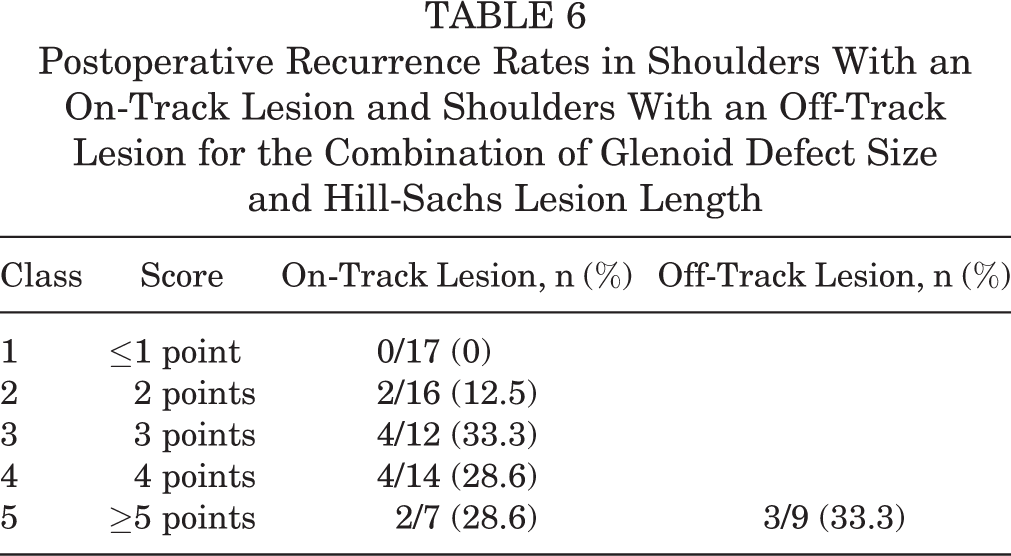
Recurrence rates in shoulders with an on-track lesion and shoulders with an off-track lesion for each class according to the combined sizes of the glenoid defect and Hill-Sachs lesion are shown in Tables 6 to 8. While most of the shoulders with an off-track lesion belonged to class 5 for any combination of the glenoid defect size and the length, width, and depth of Hill-Sachs lesions, only 2 players belonged to class 4 for the combination of glenoid defect size and Hill-Sachs lesion depth. While the presence of off-track lesions was one of the major causes for the postoperative recurrence of shoulders with a score ≥5 points (class 5), postoperative recurrence was also recognized even in shoulders with an on-track lesion.
Postoperative Recurrence Rates in Shoulders With an On-Track Lesion and Shoulders With an Off-Track Lesion for the Combination of Glenoid Defect Size and Hill-Sachs Lesion Length
Postoperative Recurrence Rates in Shoulders With an On-Track Lesion and Shoulders With an Off-Track Lesion for the Combination of Glenoid Defect Size and Hill-Sachs Lesion Width

Postoperative Recurrence Rates in Shoulders With an On-Track Lesion and Shoulders With an Off-Track Lesion for the Combination of Glenoid Defect Size and Hill-Sachs Lesion Depth

Influence of Sporting Categories on Postoperative Recurrence
The postoperative recurrence rate was 32.1% (9/28) for rugby players, 16.7% (4/24) for American football players, and 8.7% (2/23) for other athletes (wrestler: n = 1; handball player: n = 1). The postoperative recurrence rate of instability was not significantly different among the 3 sporting categories (P = .118).
Recurrence rates for each class were compared according to the combined sizes of the glenoid defect and Hill-Sachs lesion in 3 sporting categories (Tables 9-11). The classes for which postoperative recurrence was not recognized were clearly distinguished among the 3 categories. No recurrence was recognized in shoulders categorized as class 1 in rugby players, in shoulders categorized as class 1 or 2 in American football players, and in shoulders categorized as class 1, 2, or 3 in other athletes for all combinations of the glenoid defect size and the length, width, and depth of Hill-Sachs lesions. Accordingly, in class 2 shoulders, postoperative recurrence was solely recognized in rugby players, and in class 3 shoulders, recurrence was recognized in rugby players and American football players.
Postoperative Recurrence Rates for Each Glenoid Defect Size and Hill-Sachs Lesion Length

Postoperative Recurrence Rates for Each Glenoid Defect Size and Hill-Sachs Lesion Width

Postoperative Recurrence Rates for Each Glenoid Defect Size and Hill-Sachs Lesion Depth

Discussion
There has been no previous detailed report regarding the prevalence of bipolar bone loss in male athletes. In the present study, a combined lesion was recognized in almost half of the athletes investigated. As bipolar bone loss was almost equally divided among the 5 classes of our scoring system, it appears to be appropriate for evaluating the influence of the extent of bipolar bone loss on the postoperative recurrence of instability.
There have been few previous clinical studies on the critical extent of bipolar bone loss for postoperative recurrence of instability. Regarding the critical size for both lesions according to biomechanical analysis, Itoi et al 4 and Yamamoto et al 20 reported that it was 20% to 25% for glenoid bone loss, while Kaar et al 5 reported 31% of the humeral head diameter for Hill-Sachs lesions. Walia et al 16 –18 investigated the influence of bipolar bone loss on shoulder instability and range of motion by using a computer-based finite element approach and cadaveric biomechanical study design. Based on biomechanical data, they defined the critical size as >25% for an isolated glenoid defect and >31% for an isolated Hill-Sachs lesion, while the combination of a 20% glenoid defect and 6% Hill-Sachs lesion or the combination of a 10% glenoid defect and 19% Hill-Sachs lesion reduced shoulder joint stability to 70% and 69% of normal, respectively. Arciero et al 1 also reported that bipolar bone defects have an additive negative effect on glenohumeral stability. In their study, the medium Hill-Sachs lesion group with a glenoid defect ≥2 mm (8% glenoid defect) demonstrated a significant reduction of translation force after Bankart repair, while a glenoid defect ≥4 mm (15% glenoid defect) was required to produce a statistical decrease of translation force after repair in the small Hill-Sachs lesion group. According to the results of both author groups, 1,16 –18 adequate bony stability cannot be expected after Bankart repair in shoulders with a small glenoid defect and medium Hill-Sachs lesion or shoulders with a medium glenoid defect and small Hill-Sachs lesion. These combinations seem to correspond to class 3 in our system, in which postoperative recurrence was frequently recognized, so alternatives to arthroscopic Bankart repair may be indicated for male athletes with this degree of combined bone loss. On the other hand, no recurrence was recognized in shoulders categorized as class 1, and their stability was almost normal according to Walia et al, 18 so arthroscopic Bankart repair is suitable for all male athletes in this class. Accordingly, our scoring system for bipolar bone loss was shown to correspond well with the previous biomechanical data.
Regarding the relationship with the GT concept, in the present study, 12.0% of our participants had an off-track Hill-Sachs lesion. Because our participants were male competitive athletes, the ratio of an off-track lesion might be slightly larger than the ratio of 7.4% in a report by Kurokawa et al. 6 No significant difference was seen in the recurrence rate between shoulders with off-track lesions (33.3%) and those with on-track lesions (18.2%). Most of the off-track Hill-Sachs lesions belonged to class 5 according to our scoring system, and they were shown to be one of the major causes for postoperative recurrence in class 5 shoulders. On the other hand, as postoperative recurrence was frequently recognized in shoulders with an on-track lesion, even in shoulders categorized as class 2 or 3, on-track lesions were not always safe after arthroscopic Bankart repair. Thus, while the presence of an off-track lesion may be a contraindication for arthroscopic Bankart repair, the absence of an off-track lesion does not guarantee high success rates.
On the other hand, the influence of the extent of bipolar bone loss on postoperative recurrence was dependent on the type of sporting activity. Using our scoring system, the safe zone for arthroscopic Bankart repair could be determined clearly by a combined assessment of the glenoid defects and Hill-Sachs lesions. Rugby players with bipolar lesions had a high postoperative recurrence rate even when there was little bone loss. American football players with little bone loss had lower rates of instability than rugby players but higher rates than other athletes. This suggests that the type of sport also has a significant effect on recurrence, independent of bone loss. Nakagawa et al 9,10 reported that the recurrence rate was higher among rugby players compared with other athletes and that rugby players had a high recurrence rate despite a small glenoid defect. Therefore, the indications for stabilization surgery should be decided by considering both the extent of bipolar bone loss and the sporting category.
As a strength of the present study, we developed a method that allowed the influence of various combinations of bipolar bone loss on postoperative recurrence to be compared simply and easily using a scoring system for the extent of bipolar bone loss 14 and our classification based on the total score. Even if a detailed measurement of the extent of bipolar bone loss is difficult, a qualitative classification of lesions on 3D-CT scans (as none, small, medium, large, and very large) will allow preliminary decision making about operative indications, and a detailed measurement can be postponed because the size of a Hill-Sachs lesion on 3D-CT is very prominent and easy to detect.
There are several limitations to the present study. First, the method that we used for the quantification of Hill-Sachs lesions was not so simple because an assessment of 3 parameters was required; thus, the number of parameters should be reduced if possible. As the results of our scoring system were similar between Hill-Sachs lesion length, width, or depth, we can recommend that Hill-Sachs lesion width is most useful to make it quicker and easier for clinicians to use our scoring system. First, an assessment of the depth is complicated because we have to use multiplanar reconstruction images. Second, while the GT concept is now the most important method of evaluating the operative indications for stabilization surgery, the Hill-Sachs lesion width appeared to correspond best to the HSI.
Another limitation was that while we performed arthroscopic bony Bankart repair, which was arthroscopic Bankart repair without resection of the bone fragment, postoperative union of the bone fragment was not investigated. Furthermore, the relationship of postoperative recurrence of instability with the postoperative glenoid defect size was not investigated. In addition, postoperative recurrence of instability is not solely dependent on osseous factors. Recurrent injuries to the joint capsule/soft tissues have a significant influence on the recurrence rate, especially in patients with multiple dislocations. Nakagawa et al 8 have reported that capsular tears and HAGLs influence the postoperative recurrence of instability when combined with Bankart lesions.
Another limitation was that this was a retrospective study of a single surgical procedure. It is not known if a different surgical procedure will decrease the recurrence rate in patients with combined bone loss. Finally, there were a small number of athletes in each sporting category. Analysis with a larger number of athletes may show further differences between sports with regard to the importance of combined bone loss.
Conclusion
We developed a scoring system to evaluate the extent of bipolar bone loss in patients with anterior shoulder instability. Our scoring system for combined bone loss was predictive of recurrent instability after arthroscopic Bankart repair in male athletes. This system appears to be more predictive for recurrence than the GT concept. Rugby players and American football players had higher rates of recurrence with lower amounts of bone loss.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Yukioka Hospital, Osaka, Japan.