
Abstract
Background:
The combination of a glenoid defect and a Hill-Sachs lesion in shoulders with traumatic anterior instability has been termed bipolar bone loss, and the preoperative size of these lesions has been reported to influence postoperative recurrence of instability after arthroscopic Bankart repair.
Purpose:
To investigate the influence of postoperative bipolar bone defect size on postoperative recurrence of instability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 64 male collision/contact athletes (69 shoulders) were evaluated for a minimum of 2 years after surgery, and the pre- and postoperative sizes of both lesions (glenoid defect and Hill-Sachs) were evaluated retrospectively with 3-dimensional computed tomography. The sports played by the athletes included rugby (n = 28 shoulders), American football (n = 24 shoulders), and other collision/contact sports (n = 17 shoulders). Glenoid defects and Hill-Sachs lesions were classified into 5 size categories and assigned scores from 0 (no defect) to 4 (very large defect). Patients were then classified according to the total score (sum of the scores for both lesions). The influence of pre- and postoperative bipolar bone defect sizes on recurrence of instability was investigated by using the total scores for bipolar bone defects. The influence of postoperative glenoid morphology (normal preoperative glenoid, preoperative glenoid erosion, bone union after arthroscopic bony Bankart repair [ABBR], or nonunion after ABBR) was also investigated, as well as changes in shoulders with a preoperative off-track Hill-Sachs lesion.
Results:
Of 69 shoulders, 15 (21.7%) developed recurrent instability after surgery. The postoperative recurrence rate was 0% in shoulders with a total score ≤1, while the recurrence rate was consistently higher in shoulders with a total score ≥2 at both pre- and postoperative evaluation (mean, 28.8% and 32.6%, respectively). Postoperative recurrence was uncommon when there was a normal preoperative glenoid or bone union after ABBR, while it was frequent in shoulders with preoperative glenoid erosion or shoulders with nonunion after ABBR and a total score ≥2. An off-track lesion was recognized in 9 shoulders preoperatively. It was transformed to on-track lesions in 4 of the 5 shoulders showing bone union after ABBR, and there was no recurrence in the 5 shoulders with bone union. In contrast, postoperative recurrence of instability occurred in 3 of the 4 shoulders without bone union.
Conclusion:
Postoperative recurrence was influenced by the pre- and postoperative size of bipolar bone defects. Recurrence was uncommon if bone union was achieved after ABBR, even if there had been an off-track lesion preoperatively.
Keywords
Glenoid defects and Hill-Sachs lesions have long been recognized in the treatment of traumatic anterior shoulder instability, and this combination of lesions has recently been called bipolar bone loss. It has been shown that bipolar bone loss is one of the important risk factors for postoperative recurrence of instability after stabilization surgery, especially after arthroscopic Bankart repair. Burkhart and De Beer 2 reported that patients with large bone defects, such as an inverted-pear glenoid and an engaging Hill-Sachs lesion, were not candidates for arthroscopic Bankart repair because of frequent postoperative recurrence of instability. Yamamoto et al 19 defined the contact zone between the glenoid and the head of the humerus as the glenoid track (GT), and they assessed the risk of a Hill-Sachs lesion engaging the glenoid rim with or without a glenoid defect. The width of the GT is reduced in patients with a glenoid defect, so this concept allows us to consider the influence of both lesions when assessing shoulders with anterior instability. Di Giacomo et al 4 proposed the term bipolar bone loss to describe bone defects of various sizes affecting both the glenoid and the proximal humerus. They emphasized the importance of geometric interplay between defects at these 2 sites when developing criteria for surgical treatment based on the GT concept, and they stated that converting an off-track Hill-Sachs lesion to an on-track lesion is essential to stabilize shoulders with anterior instability. Thus, it has recently been considered that assessment of bipolar bone defects is essential when planning surgery for traumatic anterior shoulder instability.
Nakagawa et al 12 investigated the relationship between glenoid defects and Hill-Sachs lesions in shoulders with traumatic anterior instability, reporting that coexistence of both lesions was a possible risk factor for recurrent instability after arthroscopic Bankart repair. In addition, Nakagawa et al 7 recently proposed a scoring system for bipolar bone defects. They reported that postoperative recurrence was influenced by the preoperative bipolar bone defect sizes and the sporting category regardless of the presence or absence of an off-track lesion. Although they performed arthroscopic bony Bankart repair (ABBR), postoperative union of the bone fragment was not investigated, and neither was the relationship between recurrent instability and the postoperative glenoid defect size. Because Nakagawa et al 10,11 showed that postoperative bone union had a significant influence on recurrence of instability after ABBR, the postoperative status of bony lesions could have influenced their finding that recurrent instability was unrelated to the preoperative glenoid defect size. Accordingly, further investigation is needed to determine the influence of the postoperative size of bipolar bone defects, including the size of the residual postoperative glenoid defect after bone union, on recurrent instability.
This study was undertaken to clarify the influence of pre- and postoperative bipolar bone defect sizes on recurrence of anterior instability in male collision/contact athletes undergoing arthroscopic Bankart repair. We hypothesized that recurrence of instability could be influenced by the postoperative bipolar bone defect size rather than the preoperative bipolar bone defect size.
Methods
Patient Profiles
This was a retrospective investigation of prospectively collected clinical data, and institutional review board approval was obtained. The participants were 64 consecutive male collision/contact athletes (69 shoulders) who played at a competitive level. All participants underwent arthroscopic Bankart repair for traumatic anterior shoulder instability at our hospital between January 2010 and December 2013, had evaluation of glenoid defects and Hill-Sachs lesions by pre- and postoperative computed tomography (CT) scanning, and were evaluated for a minimum of 2 years after surgery. Arthroscopic Bankart repair was performed without additional reinforcing procedures in all patients, including those with a large glenoid defect and/or a large Hill-Sachs lesion. Female patients, patients playing noncontact sport or recreational sport, patients not playing sport, and patients with recurrent instability after previous anterior stabilization surgery were excluded.
The mean age at operation was 18.4 years (range, 14-27 years); the mean age at the time of primary instability was 17.2 years (range, 14-24 years); and the mean number of instability events was 8.5 (range, 1-80). Participants were attending junior high school (5 shoulders), high school (29 shoulders), or college (30 shoulders), and there were also 5 semiprofessional athletes. The sports played by the athletes were rugby (28 shoulders), American football (24 shoulders), basketball (4 shoulders), judo (3 shoulders), martial arts (2 shoulders), soccer (2 shoulders), wrestling (2 shoulders), ice hockey (1 shoulder), water polo (1 shoulder), handball (1 shoulder), and naginata (similar to kendo; 1 shoulder). The detailed patient profiles are shown in Tables 1 and 2.
Patient Demographics a

a Values are presented as counts.
Shoulder Profiles

a Number of shoulders per range of total events.
Operative Procedures and Postoperative Rehabilitation
Arthroscopic Bankart repair was performed by the single-row suture anchor fixation technique. The anteroinferior glenohumeral ligament–labral complex was detached and mobilized from the glenoid neck to the 6-o’clock position. Because the aim of our Bankart repair is to avoid residual capsular redundancy by elevating the anteroinferior glenohumeral ligament–labral complex, capsuloligamentous tissue was separated up to 7 o’clock in the right shoulder if mobilization was inadequate or capsular laxity was severe, which was diagnosed by preoperative positive sulcus sign and by redundancy of the anteroinferior capsule at arthroscopy. To accelerate union of the anterior labrum with the glenoid, the anterior 3 to 4 mm of the articular cartilage on the glenoid was resected. Then, 4 to 7 suture anchors were placed at the anterior bone trough created in the glenoid. Screw-in metallic suture anchors (FASTak; Arthrex) were used until June 2011, and soft anchors (JuggerKnot; Zimmer Biomet) have been used since July 2011. For the treatment of bony Bankart lesions, ABBR was performed without resection of the fragment for all patients with a bony Bankart lesion regardless of the size of a glenoid defect. 11 In patients with small bone fragments, capsulolabral repair was performed without attempting to suture the bone fragment. However, larger bone fragments were carefully sutured by use of a suture hook if possible. The aim was to reattach the fragments flush with the joint surface of the glenoid. Needless to say, it is important to remove scar tissue, refresh the glenoid and fragment sufficiently, and expose the subchondral bone. The multiple piercing to the bone fragment with a suture hook was performed to stimulate the blood supply in a manner similar to the treatment for nonunion after general fracture. Even in shoulders with a large glenoid defect, no bone grafting or rotator interval closure was performed during the study period. No patients had isolated capsular tears or isolated humeral avulsion of the glenohumeral ligament (HAGL). However, capsular tears and HAGL lesions were repaired simultaneously with the arthroscopic Bankart procedure in patients with Bankart lesions. 9 Remplissage or bone grafting was not performed, even for a large Hill-Sachs lesion.
Patients wore a brace (allowing 90° of internal rotation and 0° of abduction) for 4 weeks postoperatively and started passive range of motion exercises after 2 weeks. Until 4 weeks after surgery, flexion and external rotation with the arm at the side were restricted to 150° and 30°, respectively, but no restriction was required after 4 weeks. Return to contact training and competition was not permitted for at least 6 and 8 months after surgery, respectively.
Evaluation of Bipolar Bone Defects on CT Examination
While CT was usually performed at the first visit to our hospital, patients who had surgery a long time after the first CT scan were evaluated by CT again just before the operation. CT scanning and reconstruction of images were performed with a whole-body CT scan (spiral scan, 0.5-mm slice thickness, 0.3-mm reconstruction, and 3-dimensional [3D] edit mode), with the patient lying supine in the center of the gantry table and the affected arm in the neutral position. Data in Digital Imaging and Communications in Medicine (DICOM) mode from the CT scans were analyzed with analysis software to perform multiplanar reconstruction (MPR).
To quantify the glenoid defect, the inferior portion of the glenoid rim was approximated to a true circle on en face scans reconstructed with elimination of the humeral head, and the extent of the glenoid defect was calculated as a percentage of the glenoid rim length (B/A × 100%, where A is the diameter of the fitted circle and B is the width of the defect). 7,10 –12 The width of the bone fragment (C) was measured on the image that gave the clearest view of the articular surface of the fragment. 10,11 The size of the bone fragment was defined relative to the glenoid rim and calculated as a percentage (C/A × 100%). A Hill-Sachs lesion was diagnosed if an abnormal groove was detected on the posterolateral aspect of the head of the humerus. The width of each Hill-Sachs lesion was measured on 3D CT scans reconstructed with elimination of the scapula according to the method of Ozaki et al, 13 with the width of the lesion being defined as the longest line connecting the medial and lateral edges of the lesion on the en face view. The humeral head diameter was measured as the diameter of the circle on the axial slice with the largest circle. Then, each measurement was normalized to the humeral head diameter.
To determine whether a Hill-Sachs lesion was on-track or off-track, the width of the GT was calculated according to the method by Di Giacomo et al 4 : GT = 0.83 × A (glenoid diameter) – B (glenoid defect). Then, the distance between the rotator cuff attachments and the medial aspect of the Hill-Sachs lesion was measured as the Hill-Sachs interval (HSI). A lesion was classified as off-track if the HSI was larger than the GT, while it was on-track if the HSI was smaller than the GT. 7
Postoperative CT evaluation was performed at least once in all patients who were available for follow-up. However, this was a retrospective study, so the timing of CT was highly variable. ABBR was performed in 29 shoulders, and all of them underwent postoperative evaluation for >6 months after surgery to evaluate bone union. To assess bone union, 3D CT and MPR images were used. 10,11 Continuity between the bone fragment and glenoid in all MPR slices was considered bone union. When discontinuity was detected in some or all MPR slices, this was termed nonunion.
The actual postoperative glenoid defect size on final CT was defined as the postoperative glenoid defect size in shoulders with bone union. To quantify the postoperative glenoid defect size, the inferior portion of the glenoid rim was approximated to a true circle, as was done for preoperative evaluation, and the defect was measured at the 4-o’clock position (right shoulder), which was reported to be the direction of dislocation. 14 However, the defect size measured by excluding the bone fragment was defined as the postoperative glenoid defect size in shoulders without bone union.
Evaluations
After these parameters were obtained, the sizes of the bipolar bone defects were investigated, and each glenoid defect and each Hill-Sachs lesion was classified into 5 categories according to bone defect size with reference to the criteria of Nakagawa et al 7,12 (scores from 0 [no defect] to 4 [very large defect]) (Table 3). To assess the combined size of the glenoid defect and the Hill-Sachs lesion, we summed the scores for both lesions, and the patients were classified into 9 categories based on the total score (0-8) according to our modification of our earlier scoring system. 8
Categories and Scores According to the Size of Bone Defects

First, the influence of pre- and postoperative bipolar bone defect sizes on recurrence of instability after arthroscopic Bankart repair was investigated by using the total scores for bipolar bone defects. Postoperative recurrence was defined as any report of dislocation or subluxation, which was confirmed by physical examination and/or imaging studies (magnetic resonance imaging, CT). Subluxation was defined as an episode of shoulder instability that did not require manual reduction by a health care provider, while dislocation was defined as instability that required manual reduction by a health care provider. Second, the pre- and postoperative bipolar bone defect sizes and the postoperative recurrence rate were investigated in 3 sporting categories: rugby, American football, and other sports. Third, to clarify the influence of the preoperative glenoid defect and the preoperative bone fragment of a bony Bankart lesion, as well as the influence of bone union after ABBR, the postoperative recurrence rate was compared among shoulders with the following glenoid morphologies: normal preoperative glenoid (no glenoid defect), preoperative glenoid erosion (no bone fragment despite the presence of a glenoid defect), bone union after ABBR, and nonunion after ABBR. For shoulders with bone union after ABBR, the postoperative changes of the size of bipolar bone defects were also investigated. Finally, to clarify the relationship between our scoring system for bipolar bone defects and the GT concept, postoperative changes of the total score, the presence of a postoperative off-track lesion, and the postoperative recurrence rate were investigated in shoulders with a preoperative off-track lesion.
Statistical Analysis
For statistical analysis, comparison of mean values between 2 groups was performed with Student t test, while comparison of mean values among 3 groups was done with 1-factor analysis of variance and the Kruskal-Wallis test, and a post hoc Tukey test was performed after analysis of variance. Comparison of the postoperative recurrence rate was conducted with the Fisher exact probability test. Statistical significance was set at P < .05.
Results
Influence of Pre- and Postoperative Bipolar Bone Defect Size on Recurrence of Instability
In all 69 shoulders, while the mean size of the preoperative glenoid defect was 9.5% (range, 0%-28.5%), the mean size of the postoperative glenoid defect was 6.2% (0%-28.5%), showing a significant reduction from before surgery (P < .0001). On the other hand, the mean size of the Hill-Sachs lesion was 14.9% (0%-37.0%). The mean size of the bipolar bone defects showed a significant decrease from a total score of 3.1 (0-7) preoperatively to a total score of 2.7 (0-7) postoperatively (P < .0001).
Of the 69 shoulders, 15 (21.7%) developed recurrent instability after surgery. At the time of recurrence of instability, dislocation was recognized in 4 shoulders, while subluxation was recognized in 11 shoulders.
The influences of the pre- and postoperative glenoid defect size and Hill-Sachs lesion size on the postoperative recurrence of instability are shown in Tables 4 and 5. While the recurrence rate in patients without a pre- or postoperative glenoid defect and a Hill-Sachs lesion was low, the rate in the other patients with either bone defect was consistently high regardless of their size.
Influences of Preoperative Glenoid Defect Size and Hill-Sachs Lesion Size on the Postoperative Recurrence of Instability

a There were no shoulders with a score of 4. Dashes indicate there were no shoulders for that category.
Influences of Postoperative Glenoid Defect Size and Hill-Sachs Lesion Size on the Postoperative Recurrence of Instability

a There were no shoulders with a score of 4. Dashes indicate there were no shoulders for that category.
Based on the total score for the combined sizes of the preoperative glenoid defect and Hill-Sachs lesion, the recurrence rate was 0% in 17 shoulders with a total score ≤1, while it was consistently higher in 52 shoulders with a total score ≥2 (mean, 28.8%). When the postoperative glenoid defect and Hill-Sachs lesion were assessed, 23 shoulders had a total score ≤1 with no recurrence of instability, while the recurrence rate was higher in the 46 shoulders with a postoperative total score ≥2 (mean, 32.6%) (Table 6). There was a significant difference between shoulders with a total score ≤1 and shoulders with a total score ≥2 at pre- and postoperative evaluations (P = .0146 and P = .0013, respectively).
Influence of Pre- and Postoperative Bipolar Bone Defect Size on Postoperative Recurrence Rate a
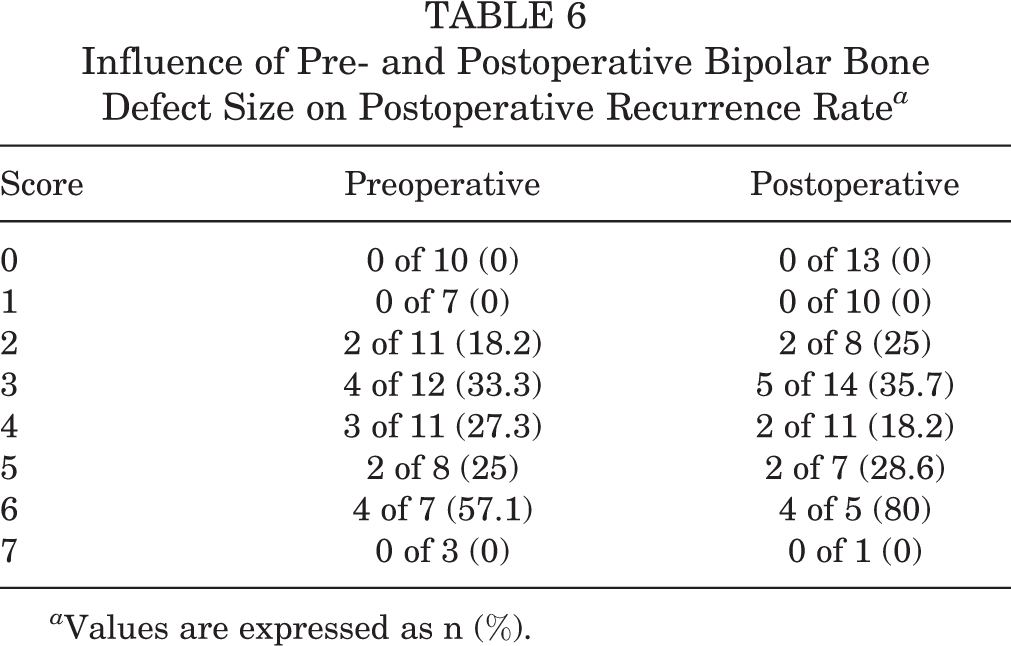
a Values are expressed as n (%).
Bipolar Bone Loss and Postoperative Recurrence Rate in Each Sporting Category
The mean glenoid defect size significantly decreased from 10.3% preoperatively to 7.2% postoperatively in rugby players (P = .0291) and from 9.8% to 4.1% in American football players (P = .0031), while it did not change in other collision/contact athletes (7.8% to 7.7%; P = .3322) because there were only 3 athletes in this category who had a preoperative glenoid defect accompanying a bone fragment. Two of these were small fragments that healed after ABBR, and 1 was a large fragment that developed a nonunion. There were no significant differences in pre- and postoperative glenoid defect size among the 3 groups. There were also no significant differences among the 3 groups with regard to the size of the Hill-Sachs lesion (Table 7).
Bipolar Bone Defect Size in Each Sporting Category

The postoperative recurrence rate was 32.8% (9 of 28) for rugby players, 16.7% (4 of 24) for American football players, and 11.8% (2 of 17) for other collision/contact athletes. There was no significant difference among the 3 groups (P = .26).
Influence of Postoperative Glenoid Morphology
The preoperative bipolar bone defect sizes in each postoperative glenoid morphology are shown in Table 8. ABBR was performed in 29 shoulders, and all 29 underwent postoperative evaluation, with the mean final evaluation time being 14.7 months (range, 6-54 months) after surgery. Bone union was confirmed in 17 shoulders (58.6%), but bone union was not obtained in 10 shoulders (including 1 shoulder with partial union), and the bone fragment seen on preoperative CT disappeared in 2 shoulders. In shoulders showing bone union after ABBR, the mean glenoid defect size decreased significantly from 16.8% (range, 5.3%-26.3%) preoperatively to 2.4% (0%-11.6%) postoperatively (P < .001). While the mean size of the preoperative bone fragment was 7.4% (1.1%-22.6%), its size was not significantly different between shoulders with bone union and shoulders with nonunion (union, 7.6%; nonunion, 6.9%; P = .7172). According to our scoring system, the bipolar bone defect size decreased after bone union, and the mean total score declined significantly from 3.4 to 2.4 (P < .0001).
Preoperative Bipolar Bone Defect Sizes in Each Postoperative Glenoid Morphology

The recurrence rate was 4.2% (1 of 24 shoulders) for shoulders with normal preoperative glenoid, but it increased to 43.8% (7 of 16 shoulders) for shoulders with preoperative glenoid erosion. Also, the recurrence rate was 5.9% (1 of 17 shoulders) for shoulders showing bone union after ABBR, but it rose to 50% (6 of 12 shoulders) for shoulders without bone union after ABBR.
Recurrence rates were also compared according to the combined sizes of the postoperative bipolar bone defects (Table 9). Among shoulders with normal preoperative glenoid and shoulders showing bone union after ABBR, postoperative recurrence of instability was recognized in only 1 shoulder from each subgroup, for a total of 3 shoulders. In shoulders showing bone union after ABBR, large bone defects were frequently seen before surgery, but postoperative recurrence was only noted in 1 shoulder; that shoulder had a preoperative total score of 4. However, among shoulders with preoperative glenoid erosion and shoulders with nonunion after ABBR, there was no postoperative recurrence of instability when the total score was ≤1, but recurrence rates were consistently high for shoulders with a total score ≥2 (mean, 50% for erosion, 54.5% for nonunion).
Influence of Postoperative Bipolar Bone Defect Size on Postoperative Recurrence Rate Among Postoperative Glenoid Morphologies a

a Values are presented as n (%). Dashes indicate there were no shoulders for that category. ABBR, arthroscopic bony Bankart repair.
Changes in Shoulders With a Preoperative Off-Track Hill-Sachs Lesion
Preoperatively, off-track Hill-Sachs lesions were recognized in 9 shoulders (13.0%). Postoperative recurrence of instability was noted in 3 of the 9 shoulders (33.3%) with an off-track lesion versus 12 of the 60 shoulders (20%) with an on-track lesion, with no significant difference of the recurrence rate between shoulders with off-track and on-track lesions (P = .396).
While the total score for preoperative bipolar bone defect size was ≥6 in 8 of 9 shoulders with an off-track lesion, the postoperative score decreased to ≤5 in 5 shoulders showing bone union after ABBR (Table 10). Among the 5 shoulders showing bone union, the Hill-Sachs lesion was transformed to an on-track lesion in 4 shoulders, and no recurrence was recognized in the 5 shoulders with bone union. In contrast, postoperative recurrence of instability occurred in 3 of the other 4 shoulders without bone union.
Changes of Bipolar Bone Defects in Shoulders With a Preoperative Off-Track Lesion a

a ABBR, arthroscopic bony Bankart repair.
Discussion
In a previous study, 12 we reported that bipolar bone defects had a significant influence on postoperative recurrence of instability after arthroscopic Bankart repair, but the combined size of the lesions did not significantly influence recurrence. In fact, we found that the recurrence rate was high even when the combined lesions were small, and we emphasized that coexistence of both lesions was a possible risk factor for recurrent instability, although larger combined bone defects have generally been considered the significant risk factor. Finite element analysis and cadaveric studies performed by Walia et al 16 –18 and Arciero et al 1 indicated that combined defects of the glenoid and humeral head show an additive negative influence on glenohumeral stability. To facilitate investigation of the influence of various combinations of bipolar bone defects on postoperative recurrence of instability, we 7 developed a scoring system for bipolar bone defects and reported that higher scores (larger lesions) were associated with a greater risk of recurrent instability.
The present study showed that the safe zone (no postoperative recurrence) for male collision/contact athletes was extremely restricted to a total score ≤1 at pre- and postoperative evaluations. This suggests that only shoulders with a small glenoid defect (≤1) or a small Hill-Sachs lesion (≤1) were safe from recurrent instability after surgery in such athletes. However, even if a large preoperative bipolar bone defect existed, the risk of postoperative recurrence after ABBR was markedly lower when the glenoid defect size was reduced by bone union and the bipolar bone defect size decreased after surgery. Thus, our modification of our earlier scoring system 8 was shown to predict recurrent instability in male collision/contact athletes undergoing arthroscopic Bankart repair, and the safe zone could be determined more accurately by assessing the Hill-Sachs lesion combined with the postoperative glenoid defect rather than the preoperative glenoid defect. Although predicting bone union is difficult, the postoperative glenoid defect size can be estimated from the preoperative defect size and the size of the bone fragment of a bony Bankart lesion by assuming that bone union will occur. 10 Accordingly, the indications for arthroscopic Bankart repair should be determined from the predicted postoperative glenoid defect size and the preoperative Hill-Sachs lesion size.
The present study showed that a preoperative normal glenoid was preferable for achieving a favorable clinical outcome after arthroscopic Bankart repair. However, if a bone fragment existed in a shoulder with a preoperative glenoid defect and if bone union was achieved after ABBR, the clinical outcome was still favorable and similar to that of athletes with a preoperative normal glenoid. In a separate study, 11 we reported that when postoperative union of the bone fragment was achieved in patients with bony Bankart lesions, the recurrence rate was significantly lower, and glenoid rim morphology became closer to normal because the united bone fragment was frequently enlarged by remodeling. Kitayama et al 5 also studied glenoid rim morphology after ABBR and reported that it was normalized in all patients after 5 to 8 years of follow-up. Therefore, we do not consider a large preoperative glenoid defect to be a definite contraindication to arthroscopic Bankart repair, which should be performed if a bone fragment is detected, since postoperative bone union is one of the most important factors for improving the clinical outcome in male collision/contact athletes. While in the present study the size of the bone fragments was not different between shoulders with bone union and nonunion, as larger (or longer) bone fragments seemed to be advantageous for bone union and recovery of preoperative glenoid defect, aggressive ABBR should be performed in such cases. However, the high recurrence rate in patients with glenoid erosion suggests that these patients should be treated with a bone-block procedure (Latarjet or Bristow procedure).
Regarding the GT concept, 13.0% of our participants had an off-track Hill-Sachs lesion, which was slightly higher than the ratio of 7.4% reported by Kurokawa et al, 6 probably because our sample was based on male collision/contact athletes. There was no significant difference in the recurrence rate of instability between shoulders with off-track lesions (33.3%) and on-track lesions (20%). Most off-track Hill-Sachs lesions were found in shoulders with a total score ≥6 according to our scoring system. In all 5 shoulders with off-track Hill-Sachs lesions and postoperative bone union, the total score decreased to ≤5 after surgery, and the Hill-Sachs lesion was transformed to an on-track lesion in 4 shoulders. Also, there was no recurrence of instability among all 5 shoulders with bone union, while there was postoperative recurrence in 3 out of 4 shoulders without bone union. This suggests that bone union is also necessary for successful arthroscopic Bankart repair in shoulders with an off-track lesion. Needless to say, patients with an off-track lesion accompanying small or no bone fragment should be treated with a bone-block procedure or remplissage.
A strength of the present study was that we clearly demonstrated the efficacy of our scoring system for bipolar bone defects. While the GT concept can determine only whether a Hill-Sachs lesion is on-track or off-track, our scoring system can quantitatively compare several lesion categories based on the total score, allowing the influence of various combinations of bipolar bone defects on postoperative recurrence to be easily compared. Furthermore, even if detailed measurement of bipolar bone defect size is difficult, qualitative classification of the lesions based on 3D CT images (as none, small, medium, large, and very large) will allow preliminary decision making about operative indications, and detailed measurement can be postponed.
A limitation of the present study was that this scoring system assumes that Hill-Sachs defects are as important as glenoid defects, while no previous report has clearly shown this. Another limitation was the method of quantifying lesions on CT scans. Several investigators have reported the difficulty of quantifying preoperative glenoid defects, 3,15 but evaluation of postoperative glenoid defects has been even more complicated. 10,11 After ABBR, the shape and position of the bone fragment varies, so the postoperative glenoid defect size would have differed slightly according to the CT slice used for measurement. However, if bipolar bone defect size could be evaluated by using the area or volume, investigation of the relationship between these lesions would become easier, so development of new methods for both lesions would be desirable. The retrospective design of the study was also a limitation. While preoperative CT data that had been collected prospectively were used to evaluate preoperative bipolar bone defects, the timing of postoperative CT was highly variable, so it inevitably had an influence on the assessment of bone union and the postoperative glenoid defect size. The postoperative glenoid defect size was measured in shoulders with nonunion by assuming that there was no bone fragment. However, some kind of bony support could be expected even in shoulders with fibrous union. As measurement of bipolar bone defects was done by 1 observer, inter- and intraobserver agreement rate was not investigated. A further limitation was that this was a study of a single surgical procedure. It is not known if a different surgical procedure, including a bone-block procedure for a large glenoid defect and a remplissage procedure for a large Hill-Sachs lesion, would decrease the recurrence rate in patients with combined bone defects. As the final limitation, postoperative recurrence of instability is not solely dependent on osseous factors. The factors regarding surgical technique, number of suture anchors, length of the labral/Bankart lesion, and quality of the soft tissue should be investigated.
Conclusion
Postoperative recurrence was influenced by the pre- and postoperative size of bipolar bone defects. Recurrence was uncommon if bone union was achieved after ABBR, even if there was an off-track lesion preoperatively.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Yukioka Hospital Institutional Review Board.