
Abstract
Background:
The results of open and arthroscopic instability repairs have been shown to be equivalent in recent literature.
Purpose:
To compare the time to recurrence (TTR) of instability and disease-specific outcome measures in patients undergoing open and arthroscopic Bankart repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with recurrent traumatic anterior shoulder instability and a Bankart lesion on diagnostic arthroscopy underwent either open Bankart repair (OB) or arthroscopic Bankart and suture capsulorrhaphy (ABSC) using suture anchors. There was a minimum follow-up of 24 months. The primary outcome measures included Western Ontario Shoulder Instability Index (WOSI) score and time to recurrence of instability (dislocation or subluxation). Rowe score, Simple Shoulder Test, Constant score, American Shoulder and Elbow Surgeons (ASES) score, and Short Form–12 (SF-12) score were also compared.
Results:
A total of 82 shoulders in 80 patients (ABSC, n = 58; OB, n = 24) were evaluated at a mean of 39 months postoperatively. There were 4 clinical failures in the OB group (4 dislocations) and 7 clinical failures in the ABSC group (2 dislocations and 5 subluxations; P = .72 vs OB). The mean time to recurrence of postoperative instability was significantly shorter in the ABSC group (12.6 ± 2.7 months) compared with the OB group (34.2 ± 12 months; P = .04). The WOSI score in the OB group (265 ± 48.1) was better but not statistically significantly compared with the ABSC group (449.8 ± 63.8; P = .06).
Conclusion:
The time to recurrence of instability after open Bankart repair is significantly longer compared with arthroscopic Bankart repair.
Clinical Relevance:
Delayed time to recurrence after open Bankart repair suggests that the open technique may be more suited to withstand the high stress and demands of a heavy-duty profession (contact athletes and heavy manual labor).
The optimal surgical management of traumatic anterior glenohumeral instability is still a matter of debate. 1,34 The goal of surgery is to reattach the anteroinferior capsulolabral tissue and restore the capsular volume without adversely restricting the range of motion of the shoulder. The open Bankart procedure remains the gold standard for operative treatment, with long-term follow-up demonstrating low recurrence rates. The outcomes with open Bankart repair have been fairly consistent and reproducible. However, a bigger incision, risk of postoperative subscapularis failure, loss of shoulder motion, and inability to address other intra-articular lesions were some of the reasons that attracted orthopaedic surgeons to adopt arthroscopic techniques for Bankart repair. 1 Furthermore, studies have demonstrated shorter operative times, less blood loss, and ability to undergo early rehabilitation with arthroscopic Bankart repair techniques. 30,33
Early experience with the arthroscopic Bankart repair demonstrated higher failure rates. 1,6 The recurrence rates after arthroscopic Bankart repair were inconsistent and affected by the surgical experience and learning curve of the surgeon. Improvements in the arthroscopic instrumentation, use of suture anchors, refinement of soft tissue techniques for capsular volume reduction (capsular plication), and increasing familiarity with the arthroscopic techniques have resulted in improvement in the results of arthroscopic techniques and lower failure rates. 8,10,29,35 A review of the American Board of Orthopaedic Surgery (ABOS) certification examination database from 2003 through 2008 for shoulder instability repair demonstrated an increasing trend toward arthroscopic Bankart repair, with the use of open Bankart repair declining among early career orthopaedic surgeons. 28
Recent studies have demonstrated a trend of equivalent outcomes and instability recurrence rates after arthroscopic and open Bankart repair. 3,6 –9,11,14,24,37 The purpose of this study was to compare the time to recurrence of instability after open and arthroscopic Bankart repair techniques. Validated outcomes and quality of life measures were used for comparative analysis at a minimum of 24 months after Bankart repair.
Methods
This was a retrospective comparative analysis of prospectively collected data, which was approved by an institutional internal review board (IRB #05-042). Individuals became eligible for inclusion in the study if they met all the following inclusion criteria: (1) history and physical examination consistent with a traumatic anterior instability, (2) confirmation of a Bankart lesion (avulsion of the anterior-inferior glenoid labrum) on diagnostic arthroscopy, (3) no history of prior shoulder surgery, and (4) follow-up of at least 2 years. Patients with unidirectional anterior instability and a confirmed Bankart lesion were excluded if (1) there was radiographic or arthroscopic evidence of a significant injury to the glenoid requiring internal fixation or bony reconstruction, (2) there was arthroscopic evidence of other significant intra-articular pathology that would require extensive repair/reconstruction (full-thickness rotator cuff tear, large Hill-Sachs lesion), or (3) they had concomitant thermal capsulorrhaphy.
Patients in this retrospective study were operated on by 1 of 4 sports medicine fellowship–trained orthopaedic surgeons between 1998 and 2003. Patients were treated with either open Bankart repair using suture anchors and capsular shift (OB group) or arthroscopic Bankart repair with suture anchors and suture capsulorrhaphy (ABSC group) as per the surgeon’s preference. One surgeon preferred open Bankart repair to the arthroscopic repair technique in collision athletes, males younger than 25 years, manual laborers, patients with poor capsular tissue (noted at the time of diagnostic scope), and history of multiple dislocations prior to repair. All surgeons contributed to the OB and ABSC groups.
Surgical Technique
After the administration of intrascalene nerve block, patients were sedated and positioned for surgery. Depending on surgeon preference, the patients were positioned in either beach chair or lateral decubitus positions for the arthroscopic procedures. Open procedures were performed in a conventional beach chair position. A thorough examination under anesthesia (EUA) confirmed anteroinferior laxity.
In the OB group, after performing a thorough diagnostic arthroscopy, the open Bankart repair with anteroinferior capsular shift was performed as described by Neer and Foster. 25 Using a deltopectoral approach, the subscapularis was exposed, incised laterally, and carefully dissected off the capsule. The glenohumeral joint capsule was split horizontally and “T’d” laterally. Each leaflet was tagged and retracted superiorly and inferiorly to expose the glenoid. This allowed full access for identification and mobilization of the Bankart lesion. The labral tear was confirmed and the glenoid footprint lightly debrided to bleeding bone on the anterior glenoid rim. Utilizing suture anchors (GII; Mitek-Depuy Synthes), the labrum was reduced and securely fixed onto the glenoid rim. With the arm in 20° of external rotation, the leaflets of the capsule were sutured in a “pants-over-vest” fashion, taking up any redundancy in the capsule (capsular shift). Prior to tying the sutures over the shortened capsule, the arm was taken through a full range of motion to ensure adequate stability while maintaining maximum range of motion. The subscapularis was repaired anatomically using number 2 nonabsorbable high-strength sutures.
The arthroscopic techniques began with a standard diagnostic arthroscopy from a posterior portal. 26 Once the pathology was deemed to be limited to the anterior-inferior labrum and the anterior capsule, the anterosuperior and anterior portals were created and appropriate-sized cannulas placed. After elevating the scarred labrum and preparing the glenoid rim to reveal bleeding subchondral bone, 0 PDS (Ethicon) was used to place the shuttling suture through the labrum with the use of the Spectrum suture passer (Conmed Linvatec). The first passing suture was brought through the redundant capsule in a location inferior to the first intended anchor location (usually at 6 o’clock). It was then brought beneath the detached labrum. After the placement of the passing suture, the first suture anchor (3-mm BioFASTak; Arthrex Inc) or Panalock suture anchor (Mitek-Depuy Synthes) was placed on the face of the anteroinferior glenoid rim (7 o’clock for the left shoulder and 5 o’clock for the right shoulder). The sutures were shuttled through the labrocapsular tissue utilizing the previously passed shuttling suture at the 6-o’clock position. This suture placement resulted in a significant capsular shift and elimination of capsular patulence when sutures were tied together using an arthroscopic knot. Subsequent suture anchors were placed proximally at 4 o’clock and 3 o’clock for right shoulder and at 8 o’clock and 9 o’clock for left shoulder. The number of suture anchors used in the repair varied depending on the extent of pathology (2-5 anchors). The rotator interval was closed with a 0 PDS suture.
Postoperative Rehabilitation
A standardized postoperative protocol consisted of 4 weeks in an abduction sling immobilizer. Formal physical therapy for gentle supervised range of motion commenced after the immobilizer was removed at 4 weeks. Active strengthening began at 8 weeks once full physiologic range of motion was achieved. Full return to collision sports was prohibited until 6 months.
Outcome Measures
Primary outcome measures included the Western Ontario Shoulder Instability Index (WOSI) score and the presence of symptomatic postoperative instability (dislocation episode or symptomatic instability). The WOSI score is a patient-reported disease-specific quality of life measure for shoulder instability. 16 It has 4 domains (physical, sports/recreation/work, lifestyle, and emotional) and a total of 21 items. The best possible total score is zero, which indicates that the patient has no decrease in shoulder-related quality of life. The worst possible score is 2100 and represents a significant decrease in shoulder-related quality of life. 15 Data from a prospective randomized controlled trial demonstrated that an individual change in the WOSI score of approximately 10% (220 points) represents a minimal meaningful clinical change. 17
The final follow-up was performed at a minimum of 2 years after surgery. A physical examination was performed, including range of motion and manual strength testing. Residual instability was assessed with a documented history of recurrence of dislocation, subluxation by history, or documentation of a positive apprehension and relocation test during physical examination. Patients were evaluated with the American Shoulder and Elbow Surgeons evaluation tool (ASES), the Simple Shoulder Test (SST), and the Constant-Murley, Rowe, and WOSI scores. Patients who had moved out of the area or who were unable to return were interviewed via telephone to obtain the modified ASES score and the SST (n = 8). None of these patients had recurrence of dislocation or subluxation based on the history obtained over telephone. The number of patients with missing data at follow-up is shown in the Appendix.
Statistical Analysis
Descriptive statistics to characterize the groups were reported using means and standard deviations or proportions where appropriate. Inferential statistics were used to compare outcome measures between the OB and ABSC. These included the chi-square for categorical variables and the Student t test for continuous variables. The alpha level for all statistics was set at ≤.05. All statistical analyses were performed using GraphPad Prism (GraphPad Software Inc).
Results
Demographics and Patient Characteristics
From 1998 to 2003, 123 patients (126 shoulders) were found to be eligible for this study. Each was found to have a confirmed Bankart lesion in the setting of symptomatic, unidirectional anterior instability on physical examination and arthroscopy (Table 1). Twenty-six patients underwent arthroscopic Bankart repair with thermal capsulorrhaphy and were excluded. After further application of inclusion and exclusion criteria and accounting for patients who declined to participate in this study or who were lost to follow-up (n = 7), 80 patients (82 shoulders; OB, n = 24; ABSC, n = 58) were available for follow-up and analysis (Table 1). The mean age of the patients was 24 years (OB, 24 ± 8.5 years; ABSC, 24.8 ± 9.3 years). The mean follow-up was 39 ± 15.3 months for both groups. The mechanism of injury in the various treatment groups, hand dominance, and other injury details are presented in Table 1. The 2 treatment groups were similar with regard to the injury characteristics but there was a greater proportion of males (P = .056) and collision athletes (P = .08) in the open Bankart repair group.
Demographics and Injury Characteristics of the Study Population a

a Data are presented as mean ± standard error of the mean (95% CI) unless otherwise indicated.
Instability Events (Clinical Failures)
There were 4 postoperative instability events in the OB group (4/24) and all 4 were dislocations following a traumatic event (Tables 2 and 3). In the ABSC group there were 2 postoperative dislocations and 5 symptomatic subluxations (7/58). There was no significant difference between the open and arthroscopic groups with respect to the postoperative recurrence of instability (P = .72). However, the clinical failures in the OB group presented at a mean of 34.2 ± 12 months postoperatively compared with the ABSC group, which presented at a mean of 12.6 ± 2.7 months, and this difference was clinically significant (P = .04). None of female patients had recurrence of dislocation after surgery.
Clinical Failure Rates and Outcome Scores in Treatment Groups a
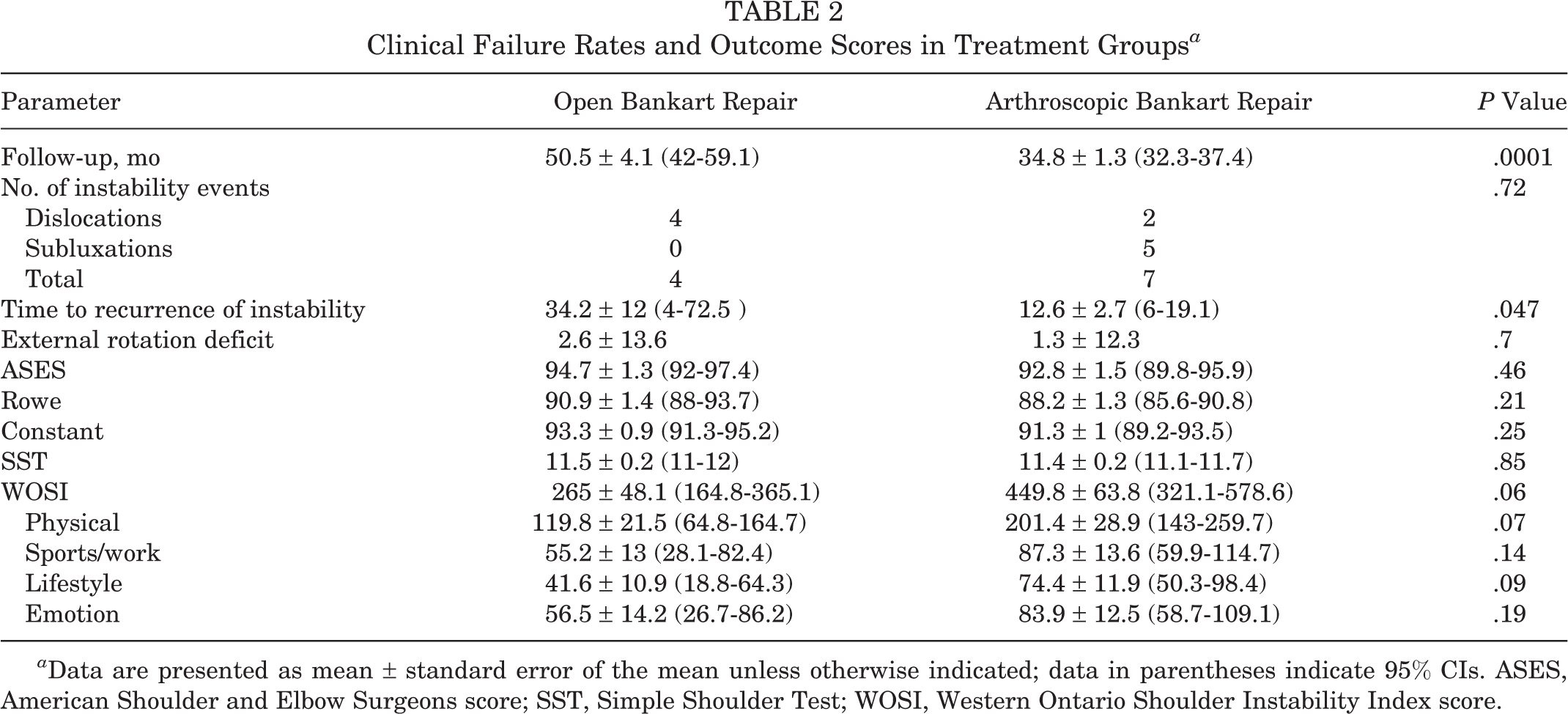
a Data are presented as mean ± standard error of the mean unless otherwise indicated; data in parentheses indicate 95% CIs. ASES, American Shoulder and Elbow Surgeons score; SST, Simple Shoulder Test; WOSI, Western Ontario Shoulder Instability Index score.
Demographic and Injury Characteristic of Patients With Postoperative Recurrence of Instability a
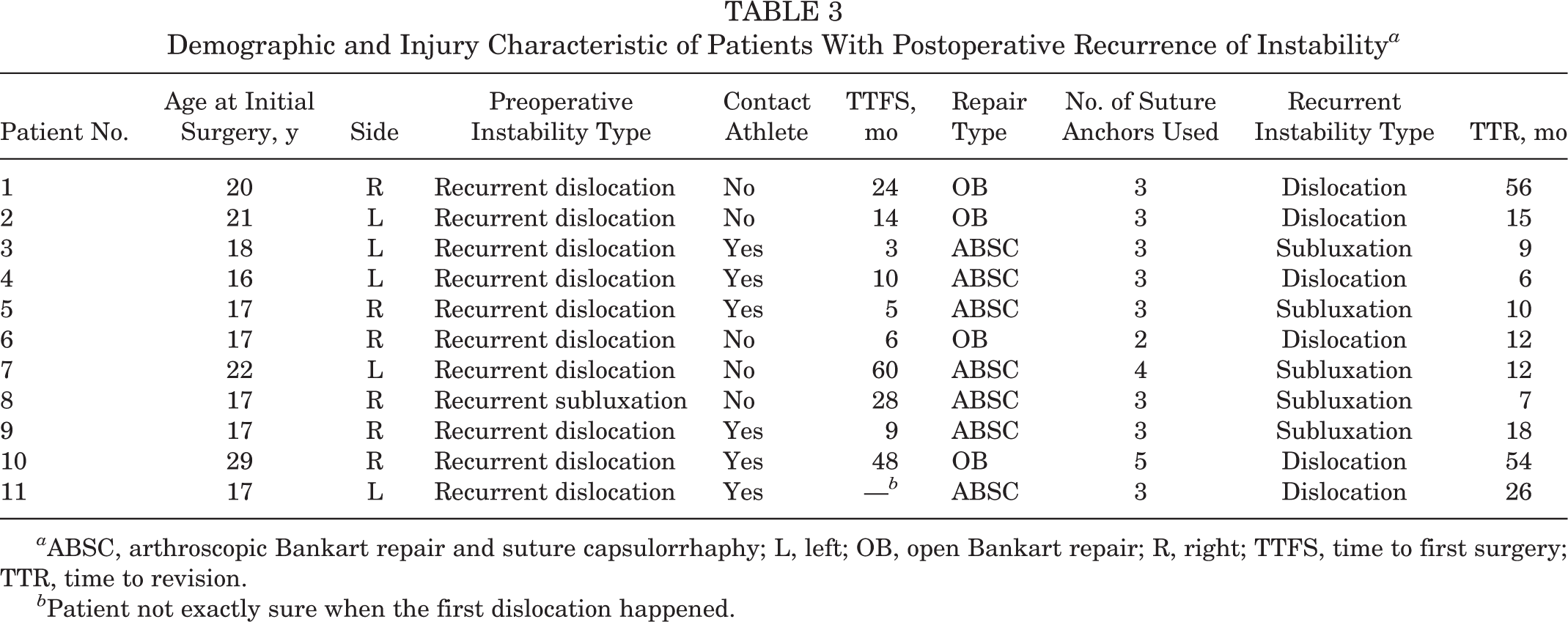
a ABSC, arthroscopic Bankart repair and suture capsulorrhaphy; L, left; OB, open Bankart repair; R, right; TTFS, time to first surgery; TTR, time to revision.
b Patient not exactly sure when the first dislocation happened.
In a subgroup cohort of collision athletes, 1 collision athlete had a recurrent dislocation postoperatively (1/12; recurrence rate, 4%) in the OB group compared with 5 contact athletes (5/17; recurrence rate, 29%) in the arthroscopic group. In the open group (OB), revision surgery was performed for 3 of the 4 failures (1 refused surgery). In the ABSC group, 4 of the 7 failures underwent revision surgery, and 3 patients with recurrent subluxation in the ABSC group refused surgery.
Outcome Measures
The WOSI scores at final follow-up were lower but not significantly better in the OB group (265 ± 48.1) compared with the ABSC group (449.8 ± 63.8; P = .06). There were no significant differences between the OB and ABSC groups with respect to the 4 domains of WOSI score (physical, sports/recreation/work, lifestyle, and emotional) (Table 2). It has been reported that the mean WOSI score in healthy volunteers with asymptomatic shoulders is 82.7 ± 155. 5 The WOSI score in the open group was closer to the WOSI scores reported in asymptomatic shoulders (difference of 182 points) compared with the ABSC group (difference of 367 points from normal score).
There were no significant differences between the OB and ABSC groups for the ASES, Constant, Rowe, and SST scores. Furthermore, there were no significant differences between the 2 groups with respect to range of motion including external rotation deficit (Table 2).
Discussion
The results of this study demonstrate that failure rates (dislocation or subluxation) after open (OB) and arthroscopic Bankart repair with suture capsulorrhaphy (ABSC) were not significantly different. The time to recurrence of postoperative instability after arthroscopic Bankart repair was significantly shorter (P = .04) compared with the open Bankart repair. Furthermore, the WOSI scores (shoulder instability–specific outcome scores) in the open Bankart repair group were better but not statistically different from the arthroscopic Bankart repair group.
The introduction of suture anchors and refinements in the soft tissue techniques to address capsular redundancy have lowered the recurrence rates of arthroscopic Bankart repair. 30,40 In addition, selection criteria have improved outcomes with arthroscopic repair as significant bone loss and poor quality capsular tissue has been identified to be negative prognostic factor for success with arthroscopic techniques. 2,31 Our results using modern arthroscopic techniques for instability repair in patients with documented recurrent traumatic anterior instability without significant bone loss demonstrate equivalent failure rates to open Bankart repair. These results are similar to other studies that have compared failure rates in open and arthroscopic techniques for instability using suture anchors for Bankart repair. ¶ In a prospective randomized controlled trial, Bottoni et al 3 demonstrated no significant difference in the failure rates between open and arthroscopic Bankart repair. There were 3 failures (2 open repair and 1 arthroscopic repair), and the outcome measures were not significantly different between the 2 groups. The operative time was significantly shorter for the arthroscopic repair compared with the open Bankart repair. Fabbriciani et al 7 reported no significant difference in instability rate between the open and arthroscopic repair in a prospective randomized trial that included 30 patients in each treatment arm. Interestingly, there was no recurrent instability in both treatment groups but there was significant loss of external rotation in the open group. A recent study by Owens et al 27 reported no significant difference in the recurrence of instability after open or arthroscopic Bankart repair. However, the number of patients in the study groups was rather small (10 open, 9 arthroscopic). Long-term studies comparing open to arthroscopic Bankart repair have reported similar results, with no difference in recurrence rates and incidence of arthritis between the 2 groups. 12,39 In contrast to the aforementioned studies including randomized controlled trials by Fabbriciani et al 7 and Bottoni et al 3 and meta-analyses, Mohtadi et al 24 recently reported a significantly greater failure rate with arthroscopic instability repair compared with open repair in a prospective, expertise-based, randomized clinical trial. A total of 196 patients with recurrent posttraumatic anterior shoulder instability were randomized to open (n = 98) or arthroscopic instability repair (n = 98). There was no significant difference in the ASES score, WOSI score, and shoulder range of motion. The recurrence rate in the arthroscopic group (23%) was significantly greater than the open group (11%) in the 2-year follow-up period.
In contrast to the aforementioned studies, we demonstrate that the time to recurrence of instability after arthroscopic Bankart is significantly shorter than in the open Bankart repair. Furthermore, WOSI scores were better in the open repair group compared with the arthroscopic repair group. There were no subluxations in the open Bankart repair group. We believe that these are important findings in our study that point to the possibility of the open Bankart repair being more durable compared with the arthroscopic repair. We and others believe that heavy manual laborers and contact or collision athletes are specific patient subgroups that are considered to have a greater risk of recurrence after Bankart repair given the demand put on the repair by the nature of their jobs. 19,22,23,32,36 It has been suggested that open Bankart repair may be a more durable option for this subgroup. In a retrospective level 4 study, Cho et al 4 demonstrated that a collision athlete demonstrates a higher recurrence rate after arthroscopic Bankart repair compared with a noncollision athlete. Rhee et al 32 retrospectively analyzed 48 shoulders (46 patients) in collision athletes who underwent arthroscopic or open Bankart repair techniques for the treatment of recurrent anterior shoulder instability. In this cohort, 16 shoulders underwent arthroscopic stabilization and 32 underwent open Bankart repair. At a mean follow-up of 72 months, open stabilization demonstrated a significantly lower recurrence rate (P = .04) compared with arthroscopic instability repair. Larrain et al 18 retrospectively analyzed 204 anterior instability repairs in collision athletes at a mean follow-up of 5.9 years. Patients without significant bone loss, humeral avulsion of anterior glenohumeral ligament (HAGL), and poor-quality capsular tissue were treated with arthroscopic stabilization and all others underwent open stabilization. Using these criteria, the authors reported an overall recurrence instability rate of 8.3% in collision athletes treated with arthroscopic Bankart repair. In a recent study, Yamamoto et al 38 reported a higher recurrence rate in contact athletes compared with noncontact athletes after Bankart repair. Furthermore, the recurrence rates were higher after arthroscopic repair compared with open Bankart repair. In our study, 50% of subjects in the open group (12/24) were collision athletes (vs 29.3% [17/58] in the ABSC group; P = .08). Of the 4 recurrences in the open group, only 1 occurred in a contact athlete and the other 3 were secondary to significant trauma (fall or fight). Of the 7 recurrences in the ABSC group, 5 were in contact athletes (Table 3). Although, a collision athlete is not necessarily a contraindication for arthroscopic Bankart repair, the senior author believes that consideration should be given to open Bankart repair in a collision athlete and manual laborer, especially if they are younger than 25 years, have had multiple prior dislocations, and have poor capsular tissue, excessive tissue laxity, and HAGL lesion. However, this finding needs to be investigated further with a prospective randomized study in this specific population group.
The WOSI score is a validated outcomes instrument that is designed specific for shoulder instability. 16 Kirkley et al 15 –17 reported that a difference of 10% (220 points) between the 2 groups correlates to a minimal meaningful clinical difference. Furthermore, a 22% difference in WOSI score represents a moderate improvement in shoulder-related quality of life. In our study, the mean WOSI score in the OB group (WOSI, 265) was lower (better) compared with the ABSC group (WOSI, 450), but the differences were not statistically significant. It has been reported that the mean WOSI score in the healthy volunteers with asymptomatic shoulders is 82.7 ± 155. 5 Interestingly, the difference between the WOSI scores in the open group and mean WOSI score of asymptomatic shoulders was lower compared with the differences between the WOSI scores of ABSC group and asymptomatic shoulders.
The highlights of this study include a relatively large patient cohort with a mean follow-up of more than 3 years to capture the majority of recurrences. We included both symptomatic subluxators and dislocators as postoperative clinical failures and believe it is important to consider both when comparing the results of different techniques of shoulder instability repair. We excluded all known variables associated with a higher failure rate in the arthroscopic bankart repair (significant bone loss, HAGL, large Hill Sachs) in our selection of patients and compared the outcomes between the 2 techniques using validated instability outcome scores (WOSI).
We realize the limitations of this study. First, this study is a retrospective comparative analysis of prospectively collected data and is limited by the inherent bias associated with retrospective study design. Second, the indication for a particular Bankart repair technique (OB or ABSC) was as per the discretion of the surgeon, and there was no randomization, which is a source of bias. Males who were younger than 25 years and involved in collision sports underwent open Bankart repair due to preferred recommendations of the senior author. Third, blinding was incomplete during the clinical assessment because of easy identification of the OB group patients due to the presence of a bigger scar from open surgery. Fourth, arthroscopic techniques for instability continue to improve, and results of arthroscopic Bankart repair and patient selection criteria have improved since this study was done. The results of this study should be interpreted keeping this fact in mind.
Conclusion
This retrospective study demonstrates that the time of recurrence of instability is significantly shorter with arthroscopic Bankart repair compared with the open Bankart repair technique. However, the recurrence of instability (dislocation and symptomatic subluxation) and instability-specific outcome measures (WOSI scores) were not significantly different between the open and arthroscopic Bankart repair techniques.
Footnotes
One or more of the authors has declared the following potential conflicts of interest or source of funding: A.D.M. is a consultant for and receives research support from Arthrex. R.A.A. is a consultant for and receives research support from Arthrex, Depuy-Mitek, Soft Tissue Regeneration, and Biomet.
Notes
Acknowledgment
The authors thank Robin Leger for her significant contribution toward data collection.
Missing Data in Each Group at Final Follow-up for All Outcome Measures a

| Outcome Measure | Follow-up Obtained, % | |
|---|---|---|
| Open Bankart Repair | Arthroscopic Bankart Repair | |
| ASES | 88 | 93 |
| Rowe | 88 | 79 |
| Constant | 88 | 79 |
| SF-12 | 83 | 74 |
| SST | 88 | 93 |
| WOSI | 92 | 76 |
a ASES, American Shoulder and Elbow Surgeons score; SF-12, Short Form–12; SST, Simple Shoulder Test; WOSI, Western Ontario Shoulder Instability Index score.