
Abstract
Background:
Accumulating evidence suggests that long-term anterior cruciate ligament (ACL) deficiency can give rise to an abnormal tibiofemoral relationship and subsequent intra-articular lesions. However, the effects of chronic ACL deficiency (ACLD) on early graft failure after anatomic reconstruction remain unclear.
Hypothesis:
We hypothesized that patients with long-term ACLD lasting more than 5 years would have a greater rate of early graft failure due to insufficient intraoperative reduction of the tibia and that the preoperative and immediately postoperative abnormal tibiofemoral relationship in the sagittal plane, such as anterior tibial subluxation (ATS), would correlate with the graft status on postoperative magnetic resonance imaging (MRI).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 358 patients who had undergone anatomic ACL reconstruction with hamstring grafts were divided into 5 groups based on chronicity of ACLD: (1) 0 to 6 months, (2) 6 months to 1 year, (3) 1 to 2 years, (4) 2 to 5 years, and (5) longer than 5 years. Preoperatively and immediately postoperatively, lateral radiographs in full extension were taken in all patients to evaluate the tibiofemoral relationship, specifically with regard to ATS, space for the ACL (sACL), and extension angle. All patients underwent MRI at 6 months to reveal graft status. Groups with a high rate of graft failure were further analyzed to compare demographic and radiographic factors between the intact and failure subgroups, followed by multivariate logistic regression analysis to identify predisposing factors.
Results:
Graft failure without trauma was observed in 4 (1.8%), 0 (0%), 1 (3.7%), 3 (9.7%), and 8 patients (17.7%) in groups 1, 2, 3, 4, and 5, respectively. Of the 76 patients in groups 4 and 5, significant differences were noted between the failure and intact subgroups in preoperative ATS (4.9 vs 2.4 mm, respectively; P < .01), side-to-side differences in sACL (sACL-SSD) (4.7 vs 1.9 mm, respectively; P < .01), extension deficit (4.4° vs 1.3°, respectively; P < .01), and chondral lesions (P = .02), while postoperative ATS and sACL-SSD showed no differences. Multivariate logistic regression analysis revealed that of these factors, preoperative sACL-SSD could be a risk factor for early graft failure (odds ratio, 3.2; 95% CI, 1.37-7.46).
Conclusion
Early graft failure at 6 months increased in patients with ACLD longer than 2 years. In this population, preoperative sACL-SSD was the most significant risk factor for early graft failure on MRI. However, immediately postoperative radiographic measurements had no effect on graft failure rates.
Chronic anterior cruciate ligament (ACL) deficiency is difficult to address 16 because it may cause meniscal and chondral lesions. 16,25 In addition to these lesions, long-term ACL deficiency (ACLD) gives rise to an abnormal tibiofemoral relationship in both sagittal 3 and coronal planes, 44 which can lead to the onset of osteoarthritis. 30
As for the sagittal knee plane, a study by Mishima et al 19 using magnetic resonance imaging (MRI) revealed that anterior tibial subluxation (ATS) in ACL-deficient knees averaged 2.1 ± 1.3 mm and that the extent correlated with chronicity of the ACLD. In terms of chronic ACLD, Almekinders et al 2,3 found that knees can exhibit uncorrectable tibial subluxation after conventional ACL reconstruction. Meanwhile, Muller et al 20 showed that anatomic ACL reconstruction, performed in either the acute or the chronic phase, restored the tibiofemoral relationship within 1.0 mm on average from the contralateral normal knee, noting that discrepancies in the above results were due to differences in surgical procedures. Part 1 of the present study also revealed that although patients with longer periods of ACL deficiency had increased ATS, anatomic ACL reconstruction could restore the tibiofemoral relationship regardless of chronicity. 39
However, we have noted that in some clinical cases, even if the tibia is posteriorly overreduced immediately after anatomic ACL reconstruction, long-term ACLD seems to be accompanied by early ACL graft failure without any trauma, as seen on MRI at several months after surgery. Generally, reasons for graft failure include trauma, technical error, and poor biological healing of the graft. 11 While early graft failure may have predisposing factors, including ATS 3 and posterior tibial slope, 5,47 the exact reasons remain unclear. In addition, as the rate of early graft failure is unclear, given the assumption that this increases with chronicity of ACLD, it would be beneficial for both surgeons and patients to know what this rate is before ACL reconstruction.
With respect to early graft failure, closer observation of MRI scans has revealed that the graft is invisible or partially invisible between the notch roof and the apex of the tibial eminence (Figure 2D). 37 Thus, in the present study, the distance between the most inferior portion of the Blumensaat line and the tip of the tibial eminence was designated as space for the ACL (sACL) for direct evaluation (Figure 1). Part 1 of this study revealed that side-to-side difference in sACL (sACL-SSD) correlated moderately with ATS (r = 0.406) and could be a convenient parameter for evaluation of ATS. 39

Radiographic measurements. (A) A lateral radiograph was taken with the patient in a supine position with the knee fully extended. (B) Anterior tibial subluxation measurement. (C) Measurement of space for the anterior cruciate ligament (double-headed arrow). (D) Extension angle measurement.

Evaluation of anterior cruciate ligament (ACL) grafts on magnetic resonance imaging. (A) Scout view for coronal-oblique images. The solid line passing through the center of the tibial tunnel aperture and the graft served as a reference line for the coronal-oblique image B. (B) Coronal-oblique image. This reveals the locations of the femoral and tibial tunnels and the entire course of the ACL graft. The white line serves as a reference line for sagittal-oblique image C and passes through the center of the tibial tunnel aperture and the graft. (C) An intact ACL graft on the sagittal-oblique image. (D) A ruptured graft, which was partially invisible between the notch roof and the apex of the tibial eminence (arrows).
The first aim of part 2 of the study was to clarify differences in the incidence of early ACL graft failure at 6 months, as evident on MRI, according to chronicity of ACLD. Subsequently, we identified the population with a high rate of early graft failure and analyzed these patients further to determine predisposing factors. We hypothesized that patients with long-term ACLD lasting more than 5 years would exhibit a high rate of early graft failure and that ATS preoperatively and immediately postoperatively would affect the graft status on postoperative MRI. Results of the current study may enable us to predict patients who are at risk of early graft failure after ACL reconstruction.
Methods
Between 2009 and 2013, a total of 685 patients underwent primary isolated ACL reconstruction with hamstring tendon grafts in our hospital. Of these, 358 patients were included in this study (147 men, 211 women; mean ± SD age, 25.7 ± 11.6 years) (Table 1), according to inclusion and exclusion criteria described in part 1. 39 These 358 patients were divided into 5 groups based on the chronicity of their ACLD: 0-6 months (group 1; n = 228), 6 months to 1 year (group 2; n = 27), 1 to 2 years (group 3; n = 27), 2 to 5 years (group 4; n = 31), and longer than 5 years (group 5; n = 45).
Patient Demographics According to Chronicity of Anterior Cruciate Ligament Deficiency a

a Data reported as mean ± SD unless otherwise indicated. Chondral lesions were evaluated by Outerbridge grade. KT-2000 SSD, side-to-side difference on KT-2000 arthrometer; NS, not significant; TAS, Tegner activity scale.
bP < .01 (groups 1-4 vs group 5).
cP < .01 (group 1 vs groups 4-5, group 2 vs group 5, group 3 vs groups 4-5).
dP < .01 (groups 1-2 vs group 5).
eP < .01 (group 1 vs groups 2-5, group 3 vs group 5).
fP < .05 (group 2 vs group 5).
gP < .01 (group 1 vs group 5).
hP < .05 (groups 2-4 vs group 5).
iP < .01 (group 1 vs groups 4-5, groups 2-4 vs group 5).
Patient demographics for each of the groups are summarized in Table 1. In brief, the mean age at surgery was significantly higher in group 5 (P < .01), and preoperative Tegner activity scale results were significantly lower in groups 4 and 5 relative to other groups (P < .01). With regard to intra-articular lesions, the status of the medial meniscus worsened with time. The rate of lateral meniscus injury was the highest in group 5, demonstrating a significant difference between group 5 and groups 1 to 4 (P < .05). Chondral injuries showed increasing tendencies with chronicity of ACLD, similar to medial meniscus injuries (Table 1).
Surgical Techniques and Postoperative Rehabilitation
Anatomic triple-bundle, double-bundle, and single-bundle ACL reconstructions were performed with autologous semitendinosus tendon grafts, as described previously 1,12,26,32,33,41 and in part 1 of this study. 39 Femoral and tibial bone tunnels were created within footprints after identification of anatomic landmarks. # This series included 59 triple-bundle (16.5%), 202 double-bundle (56.4%), and 97 single-bundle (27.1%) reconstructions. For postoperative management, the knees were immobilized at 20° of flexion with braces postoperatively for 2 weeks, with full weightbearing at 4 weeks. Patients were allowed to return to their previous activity levels after 8 to 10 months. Strenuous labor was permitted at 6 months postoperatively.
Radiographic Evaluation
Radiographic examination, including measurement of ATS, sACL-SSD, and knee extension deficit, was performed as described in part 1. 39 In brief, lateral radiographs of bilateral knees were obtained with the patients in a supine position with their knees in passive terminal extension, with their heels on a soft block (see Figure 1A). 8,20 Radiographs were excluded if the posterior points of the medial and lateral femoral condyles had more than 2 mm separation difference (Appendix Figure A1). On the preoperative radiographs, the 3 variables ATS, sACL-SSD, and knee extension deficit were evaluated (see Figure 1, B-D). Immediately postoperatively, radiographs were obtained in the operating room following graft fixation, and ATS and sACL-SSD were examined.
Evaluation of Radiographic Variables Associated With ACL Deficiency
Anterior Tibial Subluxation
ATS was defined as the difference in tibial translation between the ACL-deficient and normal knees, as previously described and established by Franklin et al 7 and others. 2,3,20 First, a line was drawn along the subchondral plate of the tibial plateau. At the posterior margin of the medial and lateral tibial plateau, lines were drawn perpendicular to the first line (Figure 1B). The shortest distance from these lines to the most posterior cortical extent of the femoral condyle was measured. Mean values for the medial and lateral sides were calculated, along with the SSD. A positive ATS indicates the anterior translation of the tibia in the ACL-deficient knee relative to the contralateral normal knee.
Space for the ACL
The distance between the tip of the tibial eminence and the most inferior portion of the Blumensaat line was measured on lateral radiographs in normal contralateral and ACL-deficient knees; this was defined as the sACL (Figure 1C). Next, the sACL-SSD was calculated, wherein a positive sACL-SSD indicates a smaller sACL in the ACL-deficient knee than in the contralateral normal knee. In other words, a positive sACL-SSD indicates ATS in the ACL-deficient knee compared with the contralateral normal knee.
Extension Angle and Extension Deficit of the Knee
On lateral radiographs, the angle between the axis of the distal one-third of the femur and the long axis of the tibia was measured as the knee extension angle (Figure 1D), while the SSD in knee extension angle was defined as the extension deficit. A positive extension deficit indicates less extension of the ACL-deficient knee.
MRI Analysis of ACL Grafts
At 6 months after ACL reconstruction, all patients were examined using a 0.4-T MRI scanner (Hitachi), as previously reported. 40,41 The knee was positioned in a coil in a nearly extended position, and fast spin-echo T2-weighted images (repetition time/echo time 3000/90 ms) were obtained in the sagittal-oblique plane at 3-mm slice thickness and 1-mm slice spacing. After sagittal-oblique scanning was completed, a coronal-oblique image of the ACL graft, which passed through the center of the tibial tunnel aperture and the graft, was obtained (Figure 2, A and B). This coronal-oblique image could show the location of the femoral and tibial tunnels and the entire course of the ACL graft and could be used to ascertain the tunnel location. Next, the sagittal-oblique image was verified to have passed through the center of the tibial tunnel aperture and the graft on the coronal-oblique image (Figure 2, A-C). If a sagittal-oblique image as described above could not be obtained, sagittal-oblique scanning was performed again to take an appropriate image.
On the sagittal-oblique MRI as described above, the status of the ACL graft was classified as “intact” or “failure” according to morphological characteristics. A failed graft was defined as one that was invisible or partially invisible between the notch roof and the apex of the tibial eminence, while an intact graft appeared thick throughout the entire graft, as described by Suomalainen et al 37 (Figure 2, C and D). Throughout this study, graft failure was judged only by morphological characteristics of the grafts. All MRIs were read by an orthopaedic surgeon (Y.T.) prior to reading any clinical data.
Statistical Analysis
Data were analyzed by use of SPSS Statistics version 19.0 (IBM Corp). Analysis of variance (ANOVA) and Tukey post hoc test were used to compare continuous variables among the 5 groups. ANOVA and the Games-Howell post hoc test were used to facilitate comparisons of Tegner scores and meniscal and chondral lesions in the 5 groups. As for ACL graft failure, groups with a 7% or higher failure rate were further examined to clarify risk factors, as a systematic review by Wiggins et al 45 revealed an ipsilateral ACL reinjury rate of 7%. Independent t test and chi-square test were used to assess differences between the intact and failure subgroups with respect to continuous variables and ordered variables, respectively. Of these examined factors, those showing a significant difference (P < .05) were further analyzed by use of multivariate logistic regression models to determine which factors could predict early ACL graft failure on MRI. For the most predictive factor, receiver operating characteristic (ROC) curve analysis was used to identify the optimal cutoff point for the graft failure between subgroups. For all statistical tests, significance was set at P < .05.
Results
Early Graft Failure on MRI
MRI at 6 months showed that a total of 16 patients (4.5%) had evidence of graft failure and that groups 4 and 5 had high incidences of graft failure, at 9.7% and 17.8%, respectively (Table 2). In the 4 patients with graft failure in group 1, the mean Tegner score was 8.5 (range, 7-9), and 3 of those proceeded with their rehabilitation beyond the planned program. All 11 patients with graft failure in groups 4 and 5 (14.5%) suffered failure without any episode of postoperative trauma. Of these 11 patients, the postoperative Lachman test was negative in 5 knees, 1+ in 5 knees, and 2+ in 1 knee. The postoperative pivot-shift test was negative in 6 knees, glide in 4 knees, and clunk in 1 knee. SSD with KT-2000 arthrometer testing in the 11 patients showed 2 peaks around 1 and 4 mm (Figure 3).
Early Graft Failure According to Chronicity of Anterior Cruciate Ligament Deficiency a

a Anterior cruciate ligament chronicity: group 1 = 0-6 months, group 2 = 6 months to 1 year, group 3 = 1 to 2 years, group 4 = 2 to 5 years, group 5 = >5 years. MRI, magnetic resonance imaging.
bP < .01 (groups 1, 2, 3 significantly less than group 5).

The distribution of KT-2000 arthrometer side-to-side difference (SSD) values in 76 patients (groups 4 and 5). The average SSD values in the total and the failure (gray) cases were 1.1 ± 1.8 mm (95% CI, 0.7-1.6) and 2.7 ± 2.2 mm (95% CI, 0.9-4.4), respectively.
Risk Factors for Early Graft Failure in Patients Experiencing ACLD More Than 2 Years
To identify predisposing factors for early graft failure, we examined the 76 patients in groups 4 and 5 (mean age, 34.6 years) and divided them into intact (n = 65) and failure (n = 11) subgroups based on MRI findings. Possible risk factors were compared between the 2 subgroups.
The intact and failure subgroups did not differ significantly in patient demographics, including mean age at ACL reconstruction, body mass index, Tegner score, or preoperative SSD on KT-2000 arthrometer (Table 3). With regard to meniscal and chondral lesions, severe cartilage lesions (defined as grade >III) were found in 10 knees (90.9%) in the failure subgroup, revealing a significant group-dependent difference (P < .05) (Table 3). Radiographic results are also summarized in Table 3. Preoperative ATS in the failure subgroup (mean ± SD, 4.9 ± 1.4 mm) was significantly greater than that in the intact subgroup (2.4 ± 1.8 mm) (P < .01). Mean immediately postoperative ATS tended to be greater in the failure subgroup compared with the intact subgroup, although no significant difference was found. Mean preoperative sACL-SSD in the failure subgroup (4.7 ± 1.6 mm) was significantly greater than that in the intact subgroup (1.9 ± 1.3 mm) (P < .01). As was observed with ATS, immediately postoperative sACL-SSD also tended to be greater in the failure subgroup compared with the intact subgroup, although no significant difference was found. Even in the failure subgroup, overreduced knee was noted immediately postoperatively in 72.7% and 81.8% of patients, as evaluated by ATS and sACL-SSD, respectively.
Comparison of Demographic and Radiographic Variables Between the Intact and Failure Subgroups a

a Data reported as mean ± SD unless otherwise indicated. sACL, space for the anterior cruciate ligament; SSD, side-to-side difference.
b Bolded P values indicate statistically significant difference between groups.
c Chondral lesions were evaluated by Outerbridge grade.
In 9 patients in the failure subgroup, the tibia was reduced posteriorly immediately after ACL reconstruction, and this was followed by graft failure on MRI at 6 months (Figure 4). The mean preoperative extension deficit was 1.3° ± 2.8° in the intact subgroup and 4.4° ± 2.6° in the failure subgroup, showing a significant difference. These results suggest that chondral lesions, preoperative extension deficit, preoperative ATS, and preoperative sACL-SSD correlate with worse ACL graft outcomes on MRI at 6 months after surgery.

Representative cases of graft failure. Case 1 (A-D) and case 2 (E-H). (A, E) Lateral radiographs of intact knees. (B, F) Preoperative anterior cruciate ligament (ACL)-deficient knees with anterior tibial subluxation. (C, G) Posteriorly reduced tibia after ACL reconstruction. (D, H) Graft failure at 6 months.
Multivariate Logistic Regression Analysis of Predisposing Factors
We identified factors that could predict ACL graft failure at 6 months using multivariate logistic regression models. Four factors, including chondral lesions, preoperative extension deficit, preoperative ATS, and preoperative sACL-SSD, were used for multivariable logistic regression analysis. Preoperative sACL-SSD (odds ratio, 3.2; 95% CI, 1.37-7.46) was found to be a strong risk factor for early graft failure (Table 4).
Multivariate Logistic Regression Analysis of Factors Influencing Early Graft Failure a

a Bolded values indicate statistically significant difference between groups. ATS, anterior tibial subluxation; preop, preoperative; sACL-SSD, side-to-side difference in the space for the anterior cruciate ligament.
For the preoperative sACL-SSD, the ROC analysis highlighted a cutoff value of 3.6 mm as the optimal threshold for differentiating between the intact and failure subgroups (sensitivity 94%, specificity 91%) (Figure 5).
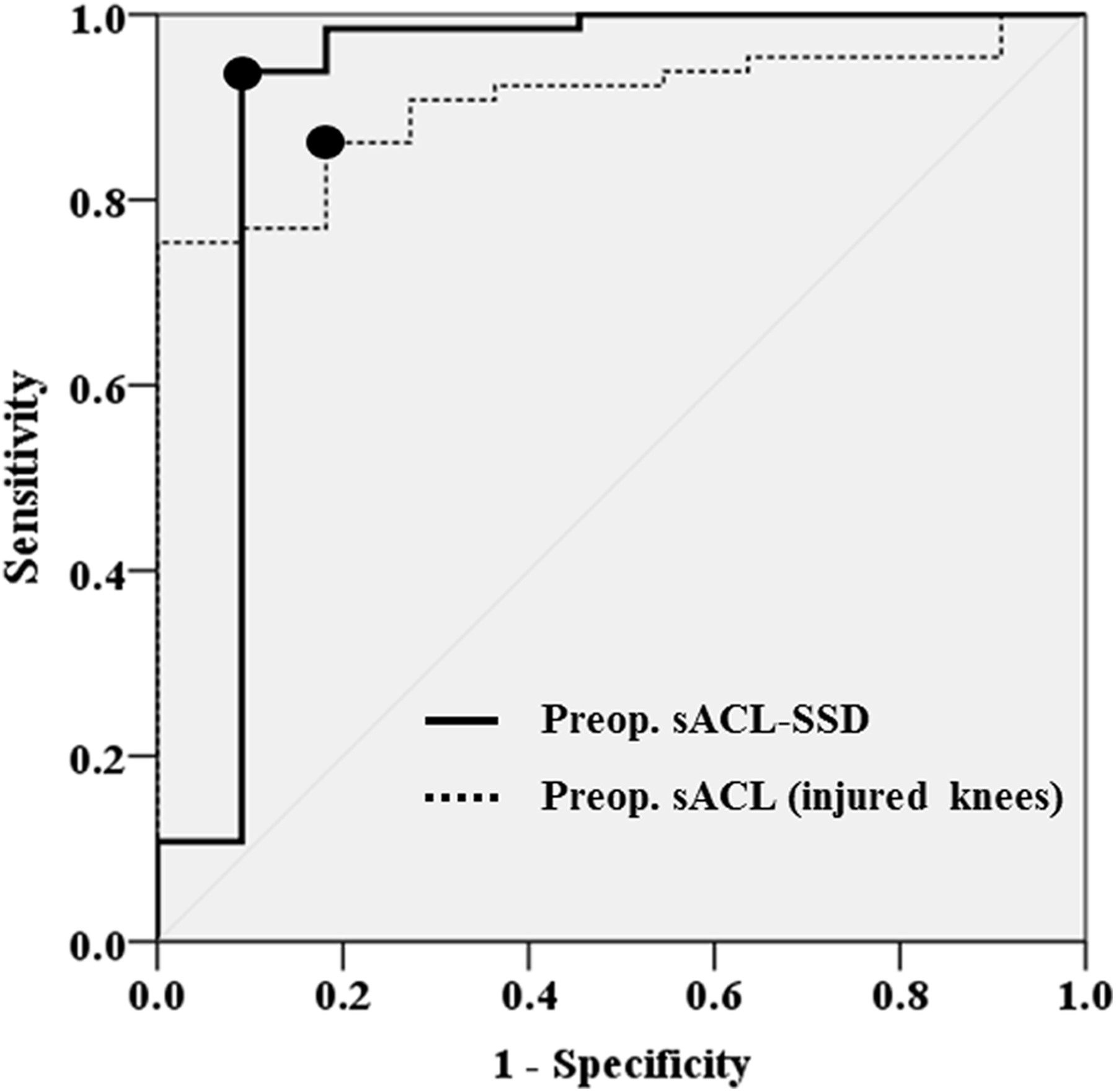
Receiver operating characteristic (ROC) curves of preoperative side-to-side difference in space for the anterior cruciate ligament (sACL-SSD) (solid line) and preoperative sACL in the injured knees (dotted line). The area under the ROC curve was 0.909 (95% CI, 0.758-1.000; P < .001) for sACL-SSD, and the cutoff point value was 3.57 mm: sensitivity 0.938, specificity 0.909. The area under the ROC curve was 0.903 (P < .001; 95% CI, 0.833-0.974) for preoperative sACL in the injured knees, and the cutoff point value was 10.2 mm: sensitivity 0.862, specificity 0.818. Preop., preoperative.
Discussion
The most important finding of the present study was that 14.5% of patients suffering from ACL deficiency for more than 2 years showed early graft failure even after anatomic ACL reconstruction with hamstring grafts. Additionally, in this population, preoperative ATS as determined by sACL-SSD was found to affect graft status at 6 months.
Generally, causes of graft failure include trauma, technical error in surgery, and failure of graft incorporation, either alone or in combination with one another. 11 As the 76 patients in groups 4 and 5 had significantly lower Tegner scores, they actually had no episode of trauma. In addition, ACL grafts in the present study seemed to be localized within the anatomic footprint because no grafts were found anterior to the resident’s ridge at the femur and anterior to Parsons’ knob at the tibia, as confirmed by a combination of sagittal-oblique and coronal-oblique MRI. 40,41 Therefore, in the current study, the graft tears in the failure subgroup would be attributed to failure of graft incorporation.
Higher graft failure rate on MRI with ACLD more than 2 years may be due to several reasons, including meniscal and chondral abnormality, 3,22,27,42 older age, 15 and worse healing environment. In terms of medial meniscal dysfunction (MMD), a high rate of excision of the medial meniscus (66.7%) was found in 76 patients with ACLD more than 2 years. The current study showed that medial meniscus status did not affect early graft failure in this population at 6 months. However, previous studies have reported the possibility that MMD increases anterior tibial translation, both preoperatively and postoperatively. 22,23,27 A biomechanical study by Musahl et al 22 showed that excision of the medial meniscus resulted in 5.5 mm of additional anterior translation during a 68-N Lachman test, even after isolated transection of the ACL. Although severe anterior translation due to both ACL and meniscal deficiency could be restored by anatomic ACL reconstruction, especially with the double-bundle procedure, 23 Parkinson et al 27 found that MMD was the most significant factor predicting graft failure in single-bundle anatomic ACL reconstruction. These results indicate that a further follow-up study might clarify the effect of MMD on graft failure on MRI. Patient age increased according to chronicity, especially in patients with ACLD more than 5 years. Kinugasa et al 15 examined the effect of patient age on the morphologic characteristics of ACL grafts and revealed that synovial coverage of the grafts was significantly poorer in younger patients, while clinical outcomes were comparable regardless of age.
As for failure of graft incorporation of ACL grafts, larger preoperative sACL-SSD was a possible reason. Although precise reasons for such failure are still unclear, overtensioning of the graft has been proposed as a potential candidate. 46 Yoshiya et al 46 found that graft incorporation was affected by excessive graft preload as well as by myxoid degeneration and decreased graft strength. When the tibia is posteriorly overreduced by anatomic ACL reconstruction, as confirmed by immediately postoperative lateral radiographs, it tightens the posteriorly restraining structures such as the posterior cruciate ligament and posterior capsule, as discussed by Almekinders et al. 3 Thus, we surmise that in patients with more severe preoperative ATS, the structures become more taut in response to the posteriorly overreduced tibia. If the structures become lax and absorb the force, excessive load is not applied to the graft; nevertheless, excessive in situ graft force might remain.
The current study showed that preoperative ATS as evaluated by sACL-SSD could be associated with early graft failure in patients with ACLD more than 2 years. To our knowledge, only 2 radiographic studies, those by Almekinders et al 3 and Muller et al, 20 have examined whether preoperative ATS affects the postoperative tibiofemoral relationship in sagittal alignment, even though many orthopaedic surgeons assume that it has already been studied and discussed widely. Although Muller et al 20 concluded that anatomic reconstruction performed in either the acute or the chronic phase enables patients to achieve a more normal tibiofemoral relationship in sagittal alignment, the investigators defined chronic ACLD as 12 or more weeks from initial injury to reconstruction. However, in our study, only 1.4% of patients with ACLD less than 2 years had early graft failure, while this occurred in 14.5% of those who had ACLD for more than 2 years. Thus, in addition to the results as previously reported, the current study clarified that the combination of chronicity and an anteriorly subluxed tibia can lead to graft failure at 6 months.
The current study also found that preoperative sACL-SSD in patients with ACLD more than 2 years was significantly greater in the failure subgroup than the intact subgroup, as was preoperative ATS. However, preoperative SSD on KT-2000 arthrometer did not show a similar tendency (see Table 3). This discrepancy might be due to differences in knee flexion angles at the time of measurement. When sACL-SSD and ATS were measured at full extension, the posterior capsule tightened. However, it might become lax in some cases when KT-2000 arthrometer measurement was done at 15° to 20° of flexion while remaining tight in other patients. Postoperatively, the KT-2000 arthrometer SSD in the 11 failure cases showed 2 peaks, at around 1 and 4 mm (see Figure 3), and the existence of the 2 peaks could also be due to the difference in posterior tightness among patients.
Severe chondral injuries and increased extension deficit were also related to graft failure in this study. These pathological conditions seem to be associated with osteoarthritic changes due to chronicity of ACLD. Cuéllar et al 6 reported that synovial fluid biomarkers including interleukin 6 and monocyte chemotactic protein 1 (MCP-1/CCL-2) were the strongest predictors of severe cartilage lesions and that matrix metalloproteinase–3 levels were consistently elevated in all operative samples. These inflammatory cytokines might affect graft maturation. As for extension deficit, we hypothesize that it represented a tight posterior capsule, which might occur in knees with increased sACL-SSD, as described above. Further investigation is required to clarify the meaning of the extension deficit.
In part 1 of this study, we found that sACL could serve as a convenient parameter to evaluate ATS. 39 In part 2, sACL-SSD was shown to be a predisposing factor for early graft failure. Given that the cutoff value to discriminate between the intact and failure subgroups was 3.6 mm, patients who have both ACLD more than 2 years and preoperative sACL-SSD greater than 4 mm should be closely monitored for graft failure without trauma. In terms of radiographic evaluation, although ATS has been reported to be useful, 2,7,20 identification of the posterior edge of the tibial plateau seems to be difficult, particularly in patients with bony spurs at the posteromedial tibial plateau. 4,21 Although an MRI study by Tanaka et al 38 demonstrated the superiority of MRI compared with radiographs in evaluating anterior knee subluxation, radiographic evaluation might still be beneficial given its accessibility.
Strategies for preventing early graft failure include the use of bone–patellar tendon–bone (BTB) grafts, notchplasty, preoperative restoration of the tibiofemoral relationship, and a decelerated rehabilitation program. The use of BTB grafts has emerged as an alternative, with several studies reporting smaller rupture rates for BTB grafts compared with hamstring tendon grafts 18 ; however, the superiority of BTB grafts remains unclear. 14 Since 60% of patients in the present study with ACLD more than 2 years had an extension deficit of 5° or more, contralateral BTB grafts could be harvested for these knees to address postoperative anterior knee problems more promptly. 31 Notchplasty can be useful for graft failure prevention, although it remains unknown whether notchplasty affects the restoration of the tibiofemoral relationship. With respect to the preoperative tibiofemoral relationship, rehabilitation before surgical treatment may be useful for restoring extension deficit, which is beneficial not only for early graft tears but also for postoperative patellofemoral problems. 24 However, sACL-SSD and/or ATS might not improve with preoperative rehabilitation. In patients with SSD 5 mm or greater, ATS may be controlled with a more invasive method such as an external fixation device. 36
Limitations of this study include the different sample sizes between groups, the small sample size of the failure subgroup, the lack of information regarding posterior tibial slope, and the fact that the patients underwent only a single MRI evaluation with 0.4-T MRI at 6 months. Additionally, this study used only MRI to determine graft failure. Furthermore, the other causes of graft failure, including trauma and technical errors, were not strictly evaluated in the current study, although there were no episodes of postoperative trauma in the failure cases. In terms of technical errors, specifically for tunnel position, we have usually evaluated bone tunnel and graft using both sagittal-oblique and coronal-oblique MRI, 17,41 which showed that none of the bone tunnel was malpositioned.
As for sample size, we could not evaluate half of the patients who had undergone ACL reconstruction. The power analysis for radiographic measurement with G*Power revealed that the sample size was small, except for measurement of preoperative sACL-SSD (Appendix Table A1). Although further follow-up studies are required, the timing of our MRI evaluation seems to be appropriate for detection of early graft failure without trauma, given that patients typically return to sports after 6 months postoperatively. In addition, we did not correlate the graft status to knee functional score, although we found laxity in patients with ACLD more than 2 years.
Another limitation was that the present study used only radiographic examination to evaluate anterior tibial subluxation. Other modalities, including MRI and computed tomography scans, could evaluate the medial and lateral tibial subluxation separately. 38 Thus, because the lateral side of the posterior tibial slope was difficult to determine, data for the posterior tibial slope were excluded from the current study. Furthermore, although this did not likely affect the current results, the 0.4-T MRI was relatively low for current scientific standards, so a superior grade MRI should be used in future studies. That said, a recent study by Muller et al 20 found that lateral radiographs are useful and reliable for evaluation of the postoperative tibiofemoral relationship. Additionally, this method can be adapted to large cohorts of patients.
Conclusion
Part 1 of this study demonstrated that the tibiofemoral relationship in the sagittal plane, which was evaluated by ATS and sACL-SSD, was significantly abnormal in patients with ACLD lasting more than 2 years. 39 The tibia could be posteriorly overreduced immediately after anatomic ACL reconstruction with the hamstring tendon, regardless of ACLD chronicity. However, part 2 of the study revealed that patients with ACLD more than 2 years exhibited a 14.5% early graft failure rate. In this population, mean preoperative sACL-SSD was significantly greater in the failure subgroup (4.7 ± 1.6 mm) than in the intact subgroup (1.9 ± 1.3 mm). The ability to reduce ATS with reconstruction using hamstring grafts did not affect failure rates. Patients with sACL-SSD more than 4 mm should be monitored closely for signs of early graft failure.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Okaka Rosai Hospital Ethics Committee.
Acknowledgment
The authors thank the following individuals for their support: Tomozo Minoura, Mitsutaka Matsuo, and Motomasa Terauchi.
Notes
Appendix
Sample Size Calculation for Radiographic Variables With G*Power a

| Radiographic Variable | No. of Groups | Power | α | Effect Size | Total Sample Size |
|---|---|---|---|---|---|
| sACL-SSD (preop) | 5 | 0.80 | .05 | 0.31 | 130 |
| sACL-SSD (postop) | 5 | 0.80 | .05 | 0.25 | 190 |
| ATS (preop) | 5 | 0.80 | .05 | 0.24 | 210 |
| ATS (postop) | 5 | 0.80 | .05 | 0.25 | 215 |
| Extension deficit | 5 | 0.80 | .05 | 0.11 | 945 |
a ATS, anterior tibial subluxation; preop, preoperative; postop, postoperative; sACL-SSD, side-to-side difference in the space for the anterior cruciate ligament.