
Abstract
Background:
It remains unclear whether the tibiofemoral relationship in the sagittal plane is restored after anatomic anterior cruciate ligament (ACL) reconstruction, particularly in cases of chronic ACL deficiency (ACLD).
Hypothesis:
Patients with long-term ACLD will exhibit an anteriorly subluxed tibia both preoperatively and immediately postoperatively, even after anatomic reconstruction.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
In total, 358 patients who had undergone anatomic ACL reconstruction with autologous semitendinosus grafts were divided into 5 groups based on chronicity of ACLD: (1) 0 to 6 months, (2) 6 months to 1 year, (3) 1 to 2 years, (4) 2 to 5 years, and (5) longer than 5 years. Preoperatively and immediately postoperatively, all patients underwent lateral radiography in extension to evaluate the tibiofemoral relationship, specifically with regard to anterior tibial subluxation (ATS), space for the ACL (sACL), and extension angle. Demographic and radiographic factors were compared among the 5 groups.
Results:
Preoperative ATS values in groups 4 (mean ± SD, 2.9 ± 2.1 mm) and 5 (2.6 ± 1.9 mm) were significantly greater than in group 1 (1.6 ± 1.9 mm). Postoperatively, the tibia was posteriorly overconstrained in all groups, and there was no difference in immediately postoperative ATS among the 5 groups. Further evaluation of the tibiofemoral relationship in the sagittal plane revealed that the mean preoperative side-to-side difference in sACL (sACL-SSD) was greater in groups 4 (2.5 ± 1.6 mm) and 5 (2.2 ± 1.7 mm) than in group 1 (1.2 ± 1.5 mm). Immediately after ACL reconstruction, however, there were no group-dependent differences in sACL-SSD. No significant group-dependent differences were found for extension deficit.
Conclusion:
Chronicity of ACLD had an effect on the preoperative tibiofemoral relationship in the sagittal plane, including ATS and sACL-SSD, especially in patients with ACLD longer than 2 years. However, preoperative extension deficit was not influenced by chronicity. Immediately postoperatively, chronicity did not affect the ability of anatomic ACL reconstruction to reduce subluxation.
Chronic anterior cruciate ligament (ACL) deficiency is difficult to address, 19 even though many orthopaedic surgeons assume that it has been studied and discussed widely. This condition is associated with intra-articular lesions, such as those due to injuries of meniscus and cartilage, which may affect the clinical results of ACL reconstruction and lead to osteoarthritic changes. 19,28 In addition to meniscal and chondral lesions, long-term ACL deficiency (ACLD) gives rise to an abnormal tibiofemoral relationship in both sagittal 4 and coronal planes, 41 which can lead to osteoarthritis onset. 32 Therefore, restoration of the tibiofemoral relationship is one of the primary goals of ACL reconstruction.
Anatomic ACL reconstruction is a useful method to restore the tibiofemoral relationship after ACL rupture. 22 Previous and recent studies of the ACL footprint have paved the way for the creation of bone tunnels in footprint areas. # Additionally, anatomic ACL reconstruction enables superior biomechanical performance, 17,20,43 which allows for a reduction in initial graft tension, leading to a normal tibiofemoral relationship after surgery. 20
In terms of chronic ACLD, Almekinders et al 3,4 found that knees can exhibit uncorrectable tibial subluxation after conventional ACL reconstruction. In one of their studies, 28 patients with ACLD for more than 2 years were evaluated by stress radiography, which measured the maximum posterior position of the tibia relative to the most posterior position of the femoral condyle. This revealed that the maximum posterior position of the tibia (mean ± SD, –0.8 ± 4.0 mm) differed significantly from that of healthy volunteers (–3.9 ± 2.9 mm). 4 Meanwhile, Muller et al 25 showed that anatomic ACL reconstruction performed in either the acute or the chronic phase restored the tibiofemoral relationship within 1.0 mm on average from the contralateral normal knee; these authors noted that discrepancies in the above results were due to differences in surgical procedures. As Muller et al 25 defined “chronic” ACLD as 12 or more weeks between injury and surgery and “acute” as less than 12 weeks, discrepancies in these results could be due to differences not only in surgical procedure but also in chronicity of ACLD. Thus, in the current study, we examined in more detail whether anatomic ACL reconstruction could restore the tibiofemoral relationship in the sagittal plane, irrespective of chronicity of ACLD.
Since the first report of radiographic anterior tibial subluxation in ACL-deficient knees by Dejour et al, 8 several imaging methods have been developed to visualize this phenomenon. 4,10,11,24,25,37,42 To emphasize the instability, both Dejour et al 8 and Franklin et al 10 obtained lateral radiographs with the quadriceps maximally contracted and the knees in a fully extended position while applying load through the ankle. The current study examined lateral radiographs in order to assess the tibiofemoral relationship in the sagittal plane.
The purpose of part 1 of the current study was to examine changes in the tibiofemoral relationship in the sagittal plane, both preoperatively and immediately after anatomic ACL reconstruction with hamstring grafts, according to variability in chronicity of ACLD. We hypothesized that patients with long-term ACLD would exhibit anteriorly subluxed tibia both preoperatively and immediately postoperatively, even after anatomic reconstruction.
Methods
Between 2009 and 2013, a total of 685 patients underwent primary isolated ACL reconstruction with autologous hamstring tendon grafts at our hospital. Of these, 377 patients provided consent for lateral radiography of both knees preoperatively and immediately after ACL reconstruction in the operating room, as well as magnetic resonance imaging (MRI) scans for our other study (part 2) at 6 months postoperatively; these patients were retrospectively investigated after approval by the regional ethics committee.
Patients with a history of prior meniscectomy (n = 32), meniscal repair (n = 5), and arthroscopic debridement (n = 6) were included in the current study. Also included were patients with a history of medial collateral ligament injury that had been treated conservatively (n = 13). Exclusion criteria included any history of injury in the contralateral knee (n = 5). In addition, 14 patients were excluded due to inadequate radiographs, in which the posterior points of the medial and lateral femoral condyles showed differences in separation of more than 2 mm, as described below. Ultimately, 358 patients were included in this study (147 men, 211 women; mean ± SD age, 25.7 ± 11.6 years) (Table 1).
Patient Demographics According to Chronicity of Anterior Cruciate Ligament Deficiency a

a Data reported as mean ± SD unless otherwise indicated. Chondral lesions were evaluated by Outerbridge grade. KT-2000 SSD, side-to-side difference of KT-2000 arthrometer result; MB, multiple-bundle reconstruction; NS, not significant; SB, single-bundle reconstruction; TAS, Tegner activity scale.
bP < .01 (groups 1-4 vs group 5).
cP < .01 (group 1 vs groups 4-5, group 2 vs group 5, group 3 vs groups 4-5).
dP < .01 (groups 1-2 vs group 5).
eP < .01 (group 1 vs groups 2-5, group 3 vs group 5).
fP < .05 (group 2 vs group 5).
gP < .01 (group 1 vs group 5).
hP < .05 (groups 2-4 vs group 5).
iP < .01 (group 1 vs groups 4-5, groups 2-4 vs group 5).
Surgical Techniques and Postoperative Rehabilitation
Anatomic triple-bundle, double-bundle, and single-bundle ACL reconstructions were performed with autologous semitendinosus tendon grafts, as described previously. 1,14,29,34,38 In 31 patients, both semitendinosus and gracilis tendons were used. Although we typically prefer anatomic multiple-bundle reconstruction, for this series single-bundle reconstruction was performed in 97 patients to prepare a thick graft. As a result, this series included 59 triple-bundle (16.5%), 202 double-bundle (56.4%), and 97 single-bundle (27.1%) reconstructions. After fixation of the grafts with an Endobutton-CL (Smith & Nephew Endoscopy) on the femur, the grafts were tensioned with a total initial tension of 30 N at 15° to 20° of flexion and fixed to the tibia with double spiked plates (DSP; Meira Corp). 33
Postoperative Rehabilitation
For postoperative management, the knees were immobilized at 20° of flexion with braces postoperatively for 2 weeks. Partial weightbearing began at 3 weeks and full weightbearing at 4 weeks. Jogging and running were allowed at 3 and 4 months, respectively. Patients were allowed to return to their previous activity levels after 8 to 10 months if postoperative quadriceps and hamstring strength levels of the injured leg improved to approximately 85% and 80%, respectively, by 6 months. Strenuous labor was permitted at 6 months postoperatively.
Radiographic Evaluation
Previous radiographic studies demonstrated the utility of lateral radiographs of the knee in the fully extended position for evaluating anterior tibial subluxation in both ACL-deficient and ACL-reconstructed knees. 3,10,11,25 Additionally, anterior tibial subluxation in a supine position seemed to indicate a more severe condition than that occurring in a standing position. 8 Furthermore, as lateral radiographs in passive terminal extension are easily taken for a large cohort of patients, lateral radiographs of bilateral knees were obtained with the patients in a supine position with their knees in passive terminal extension, with their heels on a soft block (Figure 1). 11,25 For the radiography, the film cassette was placed on the medial side of the knee at a distance of 150 cm from the x-ray source. Lateral radiographs included 12 cm of distal femur, 12 cm of proximal tibia, and the superimposed femoral condyles. Radiographs were excluded if the posterior points of the medial and lateral femoral condyles had more than 2 mm separation difference, as described below.

Positioning for radiography. A lateral radiograph was taken with the patient in a supine position with the knee in passive terminal extension, with the heel on a soft block.
On the preoperative radiographic images, we evaluated 3 variables, as described below: anterior tibial subluxation (ATS), side-to-side difference in space for the ACL (sACL-SSD), and knee extension deficit. Immediately postoperatively, radiographs were obtained in the operating room following graft fixation, and 2 variables, ATS and sACL-SSD, were examined.
Evaluation of Radiographic Variables Associated With ACL Deficiency
Anterior Tibial Subluxation
ATS was defined as the difference in tibial translation between the ACL-deficient and normal knees, as previously described and established by Franklin et al 10 and others. 3,4,25 First, a line was drawn along the subchondral plate of the tibial plateau. At the posterior margin of the medial and lateral tibial plateau, lines were drawn perpendicular to the first line (Figure 2A). The shortest distance from these lines to the most posterior cortical extent of the femoral condyle was measured (Figure 2B). Mean values for the medial and lateral sides were calculated, along with the side-to-side difference. A positive ATS indicates the anterior translation of the tibia in the ACL-deficient knee relative to the contralateral normal knee. Throughout the study, the absolute values of measurements in millimeters were used and were not normalized using the size of the tibia to account for differences in magnification; this was because a standardized radiographic technique was used for each patient, which minimizes variability in magnification, as described previously. 3,4,10,25

Radiographic measurement. (A) Anterior tibial subluxation measurement. A line was drawn along the subchondral plate of the tibial plateau. At the posterior margin of the medial and lateral tibial plateau, lines were drawn perpendicular to the first line. (B) The shortest distance from these lines to the most posterior cortical extent of the femoral condyle was measured (yellow lines). Mean values for the medial and lateral sides were calculated, along with the side-to-side difference. (C) Measurement of space for the anterior cruciate ligament (double-headed arrow). (D) Extension angle measurement.
Space for the ACL
The present study used space for the ACL (sACL) as another tool to evaluate the tibiofemoral relationship in the sagittal plane because it was seemingly difficult to identify the posterior margin of the tibial plateau due to the osteophyte formation “cupola sign” 6 that was evident in some clinical cases with long-term ACLD. The distance between the tip of the tibial eminence and the most inferior portion of the Blumensaat line was measured on lateral radiographs in normal contralateral and ACL-deficient knees; this was defined as sACL (Figure 2C). Next, the sACL-SSD was calculated, wherein a positive sACL-SSD indicates a smaller sACL in the ACL-deficient knee than in the contralateral normal knee. In other words, a positive sACL-SSD indicates an anteriorly subluxed tibia in the ACL-deficient knee compared with the contralateral normal knee. The sACL was also evaluated by use of absolute values in millimeters, as performed in the ATS evaluation, because a standardized radiographic technique was used for each patient. In patients for whom the tip of the tibial eminence was difficult to identify, corresponding points on the tibial eminence were determined around the tip, and the sACL was measured in the ACL-deficient knee and the contralateral normal knee, followed by calculation of the sACL-SSD. In such cases, evaluation of the sACL-SSD would reduce the variation of sACL measurement.
To determine the reproducibility of the sACL measurements, data from 50 patients were randomly selected and assessed. Intraobserver and interobserver reliabilities were assessed by intraclass correlation coefficients (ICCs). The sample size was estimated by the software G*Power 3.1.9.2 (Franz Faul, University of Kiel), considering an effect size of 0.50, power of 0.80, and α = .05, resulting in 29 samples. Thus, for assessment of intraobserver reliability, a single orthopaedic surgeon (Y.T.) measured the sACL twice in each of the 50 patients, with an interval of 14 days between measurements. A 1-way random effects model was used to determine intraobserver ICC. For assessment of interobserver reliability, 2 orthopaedic surgeons (Y.T. and K.K.) independently measured the sACL in 50 patients, and a 2-way random effects model was used to calculate interobserver ICC.
Extension Angle and Extension Deficit of the Knee
In lateral radiographs, the angle between the axis of the distal one-third of the femur and the long axis of the tibia was measured as the knee extension angle (Figure 2D), while the side-to-side difference in knee extension angle was defined as the extension deficit. A positive extension deficit indicates less extension of the ACL-deficient knee.
Exclusion Criteria for Radiographs
We regarded radiographs as inadequate when the posterior points of the bilateral femoral condyles were farther than 2 mm apart. Rotation can affect the measurement of radiographs in the current study, especially for the sACL. The mean ± SD sACL in 358 patients was 12.4 ± 1.8 mm and 13.9 ± 1.7 mm in the ACL-deficient and contralateral normal knees, respectively. Mean sACL-SSD was 1.5 ± 1.6 mm. When the posterior points of the bilateral condyles were 2 mm apart and the sACL was 13.9 mm, sACL measurements differed by 0.0293 mm (0.21% of sACL and 1.95% of sACL-SSD). When this distance was 3 mm, the difference in measurement increased up to 0.0711 mm (0.51% of sACL and 4.74% of sACL-SSD) (Appendix Figure A1). Thus, we defined “inadequate radiographs” as described above.
Statistical Analysis
Data were analyzed by use of SPSS version 19.0 (IBM Corp). Analysis of variance (ANOVA) with Tukey post hoc test was used to compare continuous variables among the 5 groups. ANOVA with the Games-Howell post hoc test was performed to facilitate comparisons for ordered variables among groups. The level of significance was set at P < .05.
Results
In total, the 358 patients were divided into 5 groups based on their preoperative duration: group 1, 0 to 6 months (228 patients); group 2, 6 months to 1 year (27 patients); group 3, 1 to 2 years (27 patients); group 4, 2 to 5 years (31 patients); and group 5, more than 5 years (45 patients). Mean age at surgery was significantly higher in group 5, and preoperative Tegner activity scale scores were significantly lower in groups 4 and 5 relative to the other groups (Table 1). With regard to intra-articular lesions, status of the medial meniscus (MM) worsened significantly in groups more than 6 months from injury (Table 1). The rate of untreated MM decreased progressively from group 1 (75.4%) to group 5 (28.9%). The rate of lateral meniscus injury was the highest in group 5, demonstrating a significant difference between group 5 and groups 1 through 4 (Table 1). There was an increasing tendency of chondral injury as ACLD chronicity increased, similar to MM injuries (Table 1).
Radiographic Variables According to ACLD Chronicity
Radiographic variables are summarized in Table 2 and Appendix Table A1. The tibiofemoral relationship in the sagittal plane showed a mean overall preoperative ATS of 1.9 ± 1.9 mm. As the tibia was posteriorly translated immediately after ACL reconstruction, the mean overall ATS was –3.1 ± 2.5 mm. Although preoperative ATS values in groups 4 (2.9 ± 2.1 mm) and 5 (2.6 ± 1.9 mm) were significantly greater than that in group 1 (1.6 ± 1.9 mm) (P < .01), there was no difference in immediately postoperative ATS among the 5 groups (Table 2). Further evaluation of the tibiofemoral relationship in the sagittal plane revealed that the mean preoperative sACL-SSD was 1.5 ± 1.6 mm, followed by a decrease in sACL-SSD to –3.3 ± 2.3 mm as a result of a posteriorly overconstrained tibia (Table 2). With regard to the relationship between chronicity and sACL-SSD, preoperative sACL-SSD was significantly greater in groups 4 (2.5 ± 1.6 mm) and 5 (2.2 ± 1.7 mm) than in group 1 (1.2 ± 1.5 mm) (P < .01). Immediately after ACL reconstruction, however, no group-dependent differences were noted in sACL-SSD (Table 2). The percentages of patients who achieved a posteriorly overconstrained knee postoperatively were 90.2% and 93.3% according to ATS and sACL-SSD, respectively. Furthermore, the mean overall immediately postoperative ATS and sACL-SSD was less than 1 mm in 96.3% and 97.7% of patients, respectively. We found no significant group-dependent differences in extension deficit.
Radiographic Variables According to Chronicity of ACLD a
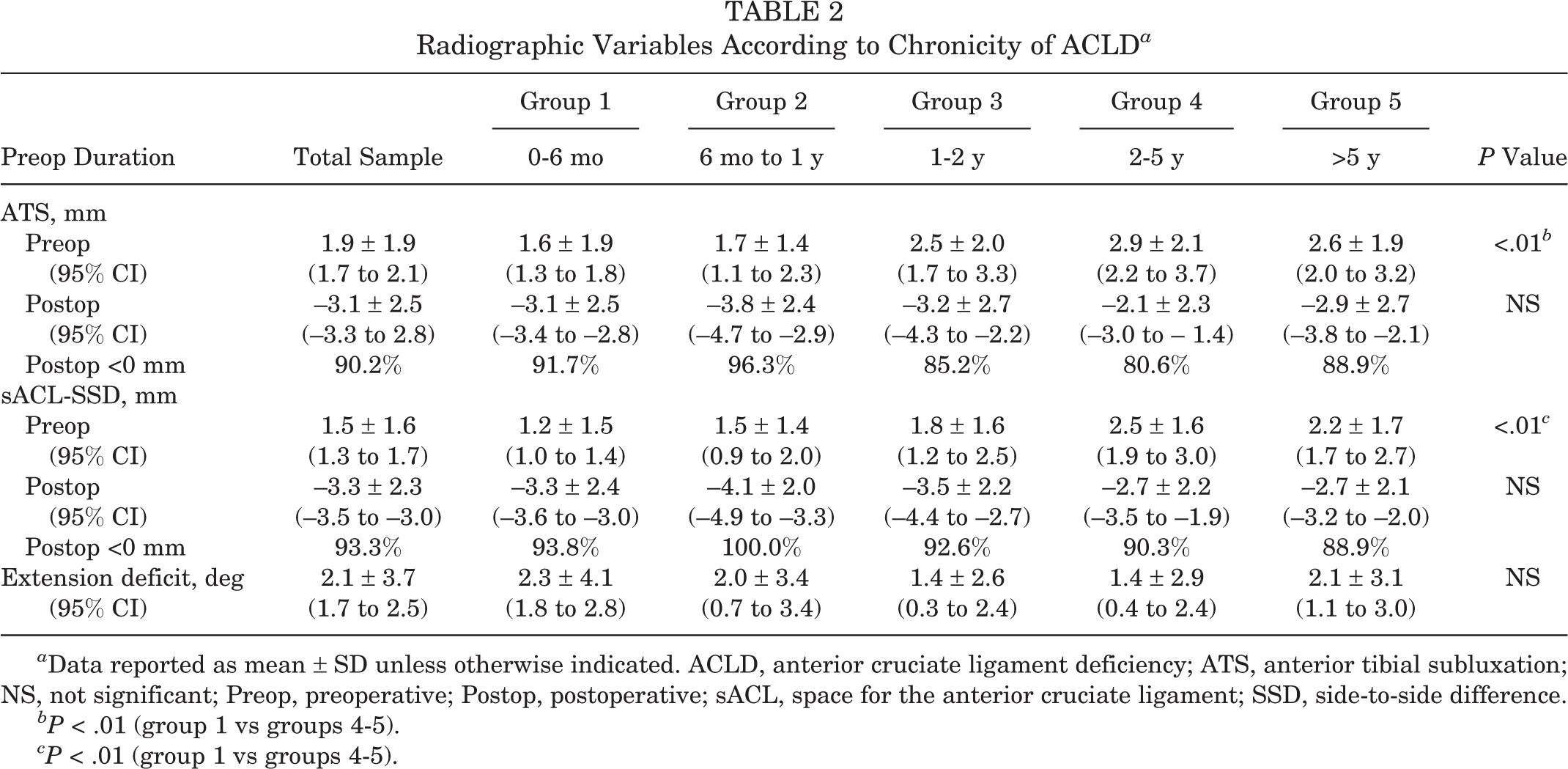
a Data reported as mean ± SD unless otherwise indicated. ACLD, anterior cruciate ligament deficiency; ATS, anterior tibial subluxation; NS, not significant; Preop, preoperative; Postop, postoperative; sACL, space for the anterior cruciate ligament; SSD, side-to-side difference.
bP < .01 (group 1 vs groups 4-5).
cP < .01 (group 1 vs groups 4-5).
Characteristics of the sACL and sACL-SSD
Intra- and interobserver reliabilities for the sACL were high (interobserver ICC, 0.847; intraobserver ICC, 0.859). Mean sACL in the ACLD knees was 12.4 ± 1.8 mm, which was significantly smaller than that in normal knees (13.9 ± 1.7 mm, P < .01) (Appendix Table A1). Correlations of sACL and sACL-SSD with other radiographic variables are summarized in Table 3. The sACL-SSD showed a weak correlation with ATS (r = 0.406), but no association was found with extension deficit. Knee extension angle did not seem to be associated with radiographic variables such as the ATS, sACL, or sACL-SSD (Table 3).
Correlations Among Radiographic Variables a

a Bolded values indicate the correlation between ATS and sACL-SSD, preoperatively and postoperatively. ACLD, anterior cruciate ligament deficiency; ATS, anterior tibial subluxation; Ext, extension; Preop, preoperative; Postop, postoperative; r, Pearson coefficient; sACL, space for the anterior cruciate ligament; SSD, side-to-side difference.
bP < .01.
cP < .05.
Discussion
The most important finding of the present study was that the immediately postoperative tibiofemoral relationship in the sagittal plane as determined by ATS and sACL-SSD did not show significant differences, regardless of chronicity of ACLD. Additionally, preoperative ATS and sACL-SSD significantly increased in patients who had ACLD for more than 2 years.
The mean value of the preoperative ATS in the current study was 1.9 ± 1.9 mm. In an MRI study by Mishima et al, 24 the preoperative ATS averaged 2.1 ± 1.3 mm and was compatible with our result. However, Dejour et al 8 and Franklin et al 10 reported mean values of 6.5 mm and 7.5 mm, respectively, which were obviously larger than our result. The reason for the lower preoperative ATS in our study is likely due to the difference in applied load to the leg. Both Dejour et al 8 and Franklin et al 10 measured ATS on true lateral radiographs while the knee was in full extension and the quadriceps was maximally contracted, with a load produced by a weight suspended from the ankle.
As for chronicity of ACLD, the preoperative ATS in the current study changed in a time-dependent manner, as Mishima et al 24 previously described. The ATS in the current study significantly increased in patients with ACLD for more than 2 years. Reasons why there was more ATS in patients with more chronic ACLD might include MM dysfunction and stretching of the posterior capsule. Ramp lesions, which are meniscal lesions involving the peripheral attachment of the posterior horn of the MM, increased according to chronicity, with an incidence of 18% in patients with ACLD more than 2 years. 18 A biomechanical study by Ahn et al 2 showed that MM posterior horn longitudinal tears in ACL-deficient knees resulted in a significant increase in anterior tibial translation at all flexion angles except 90°. Furthermore, as for timing of ACL reconstruction, Tandogan et al 39 examined the relationship between intra-articular lesions due to ACL insufficiency and the time from initial injury and reported that MM tears and chondral lesions increased due to the chronicity of ACLD. The MOON (Multicenter Orthopaedic Outcomes Network) study by Nguyen et al 28 revealed a significantly higher number of complete MM tears in the chronic group versus the acute group (49.0% vs 22.5%) when the investigators defined acute ACL reconstruction as less than 3 months and chronic ACL reconstruction as more than 6 months. Since the rate of excised MM drastically increased from group 1 (8.8%) to group 2 (37.0%) in the current study, better clinical results may be obtained when ACL reconstruction is performed within 6 months of the initial injury.
Another important finding in the current study was that chronicity did not affect ability to correct ATS with anatomic ACL reconstruction. With regard to ATS after ACL reconstruction, conventional nonanatomic reconstruction could not reduce the anteriorly subluxed tibia. 3,4 In addition, 28 patients who had ACLD more than 2 years were evaluated on stress radiographs, which revealed that the maximum posterior position of the tibia (–0.8 ± 4.0 mm) differed significantly from that of healthy volunteers (–3.9 ± 2.9 mm). 4 In contrast, Muller et al 25 reported that anatomic reconstruction, performed in either the acute or the chronic phase, reduced the ATS to 1.0 ± 2.1 mm, which shifted the patient closer to achieving a normal tibiofemoral relationship. Although we hypothesized that patients with long-term ACLD would exhibit anteriorly subluxed tibia both preoperatively and immediately postoperatively even after anatomic reconstruction, our results support the conclusions of Muller et al, 25 because approximately 90% of patients were able to achieve a posteriorly overconstrained tibia immediately after anatomic ACL reconstruction with hamstring grafts.
One of the advantages of anatomic ACL reconstruction is superior biomechanical results. A cadaveric study by Yagi et al 43 revealed that the anatomic ACL reconstruction was able to more closely restore knee kinematics. Under a 134-N anterior tibial load at 30° of knee flexion, mean values of anterior tibial translation were 6.4 ± 2.4 mm, 10.2 ± 2.5 mm, and 7.8 ± 2.3 mm in intact, conventional single-bundle, and double-bundle reconstructions, respectively. 43 Mae et al 20 showed that the graft tension to restore normal anterior-posterior laxity was significantly lower in anatomic double-bundle reconstruction than in isometric bisocket reconstruction. Mae et al 21 also found that anatomic double-bundle ACL reconstruction with 20 N of low initial tension achieved good clinical outcomes at 2 years postoperatively. Using a mechanized pivot-shift test, Musahl et al 27 revealed that anterior tibial translation was 1.7 ± 3.0 mm, 4.4 ± 1.0 mm, and –1.7 ± 3.3 mm for intact knees, conventional single-bundle reconstruction, and the anatomic double-bundle technique, respectively. In addition to these examples of normalization in anterior-posterior translation, a kinematic study by Matsuo et al 22 clarified the possibility that anatomic triple-bundle reconstruction restores a normal tibiofemoral relationship in the sagittal plane. These results indicate that anatomic reconstruction could be a more efficient procedure to restore the normal kinematics of the tibiofemoral joint.
With regard to differences in surgical procedures, although group 5 in the current study included far more patients treated with anatomic single-bundle reconstruction, the immediately postoperative tibiofemoral relationship in the sagittal plane as determined by ATS and sACL-SSD showed no significant differences, regardless of chronicity of ACLD. However, other studies have found that the anatomic double-bundle procedure has superior biomechanical results compared with the anatomic single-bundle procedure. 5,16 In one of those studies, side-to-side differences in anterior tibial translation measured with a KT-1000 arthrometer were significantly higher in the single-bundle group (2.2 ± 1.4 mm) than the double-bundle group (1.1 ± 1.0 mm). 5 In a biomechanical study using the quadriceps tendon, Kim et al 16 found that anatomic double-bundle reconstruction restored anterior tibial translation to the normal knee, while that of the single-bundle procedure differed at the flexion position. A follow-up study is required to determine the long-term outcomes of these various surgical procedures.
In terms of the posteriorly overreduced tibia in the present study, the tibia was located in a 3.1-mm posterior position compared with the normal knee immediately postoperatively. Mae et al 21 showed that the side-to-side difference in anterior laxity as measured by KT-2000 arthrometer was 3.7 mm immediately after anatomic double-bundle ACL reconstruction with the patient under anesthesia. Matsuo et al 22 revealed that 3 weeks after anatomic triple-bundle ACL reconstruction, the tibia was at a 2.0-mm posterior position but returned to the normal position 6 months later. These results indicate that a postoperatively overreduced tibia may gradually return to the normal position.
Another important finding of the current study was that the sACL can serve as a convenient parameter to evaluate anterior tibial subluxation. In terms of radiographic evaluation, ATS has been reported to be useful. 3,10,25 Although the sACL-SSD also appeared to reflect anterior tibial subluxation, it correlated only moderately with ATS (r = 0.406) (Table 3). There might be two reasons to explain the lack of a strong correlation between the two measurement methods. The first is the difference in directions used to measure ATS and sACL; namely, measurement of the sACL began from the tip of the tibial eminence and approached the inferior part of the Blumensaat line, while ATS was measured along with the tibial plateau. The other reason involves degenerative changes occurring in the posteromedial part of the medial tibial plateau. Brunkhorst and Johnson 6 described the “cupola sign” as an adaptive response to anterior translation. This is an osteophyte on the posteromedial edge of the tibia that is seen on lateral radiographs. Mullis et al 26 also observed these osteophytes in the degenerative knee. Since ACL-deficient knees gradually show subtle changes around the posterior edge of the tibial plateau, precise measurement of the tibiofemoral relationship in the sagittal plane on radiographs can be difficult in some cases. The sACL, which basically reflects the width along the course of the ACL (or the graft), could also be useful for detecting anterior tibial subluxation and could be more suitable for evaluation of knees with degenerative changes than ATS, partly because measurement of the sACL is susceptible to these changes. Although an MRI study by Tanaka et al 37 demonstrated the superiority of MRI examination compared with radiographic examination in evaluating anterior knee subluxation, radiographic evaluation might still be beneficial given its accessibility.
As for preoperative motion loss, extension deficit in the current patients averaged 2.1° ± 3.7°, and chronicity did not affect the deficit. McHugh et al 23 reported that patients lacking 1° to 4° of extension preoperatively had similar outcomes compared with patients lacking 5° or more preoperatively. Although we tried to resolve the preoperative loss, as generally recommended, 7 stricter management might be required to control preoperative extension deficit.
Limitations of this study include the different sample sizes between groups, no reliability measurement of ATS and extension deficit, different surgical techniques, a lack of follow-up evaluation by radiographs and clinical symptoms, and the potential variability in tibial rotation before and immediately after ACL reconstruction. The deviation in sample sizes between groups was inevitable given the necessarily earlier timing of surgical treatment for patients with ACLD, considering the relationship between chronicity of ACLD and intra-articular lesions. 28,39 In the follow-up study (part 2), we focused on the preoperative and immediately postoperative tibiofemoral relationship in the sagittal plane with regard to whether it affects the status of ACL grafts. In terms of tibial rotation, the preoperative internally rotated tibia could be externally overconstrained immediately after ACL reconstruction. 22 In addition, the current study evaluated a 2-dimensional projection of a 3-dimensional position. As the potential variability in tibial rotation might lead to differences in measurement, another limitation was that the present study used only radiographic examination. Other modalities, including MRI and computed tomography scans, would be able to evaluate the medial and lateral tibial subluxation separately 37 as well as the tibiofemoral relationship in the coronal plane. 41 That said, the study by Muller et al 25 found that lateral radiographs were also useful and reliable for evaluation of the postoperative tibiofemoral relationship. Additionally, this method can be adapted to large cohorts of patients.
Conclusion
Chronicity of ACLD affected the preoperative tibiofemoral relationship in the sagittal plane, including ATS and sACL-SSD, especially in patients with ACLD more than 2 years. However, preoperative extension deficit was not influenced by chronicity. Immediate postoperatively, chronicity did not affect ability of anatomic ACLR to reduce subluxation. The tibia was generally overconstrained posteriorly regardless of the preoperative ATS.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Osaka Rosai Hospital Ethics Committee.
Notes
Appendix
Radiographic Variables According to Chronicity of ACLD a

| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | |||
|---|---|---|---|---|---|---|---|
| Preop Duration | Total Sample | 0-6 mo | 6 mo to 1 y | 1-2 y | 2-5 y | >5 y | P Value |
| sACL, mm | |||||||
| Preop (normal knee) | 13.9 ± 1.7 | 13.9 ± 1.7 | 13.8 ± 1.9 | 14.1 ± 1.8 | 14.5 ± 1.7 | 13.6 ± 1.6 | NS |
| Preop (injured knee) | 12.4 ± 1.8 | 12.6 ± 1.6 | 12.3 ± 1.8 | 12.3 ± 1.5 | 12.1 ± 2.0 | 11.4 ± 1.8 | <.01 b |
| Preop (SSD) | 1.5 ± 1.6 | 1.2 ± 1.5 | 1.5 ± 1.4 | 1.8 ± 1.6 | 2.5 ± 1.6 | 2.2 ± 1.7 | <.01 c |
| sACL, mm | |||||||
| Postop (injured knee) | 17.2 ± 2.2 | 17.2 ± 2.2 | 17.9 ± 2.0 | 17.7 ± 2.2 | 17.2 ± 2.3 | 16.2 ± 2.2 | <.01 d |
| Postop (SSD) | –3.3 ± 2.3 | –3.3 ± 2.4 | –4.1 ± 2.0 | –3.5 ± 2.2 | –2.7 ± 2.2 | –2.7 ± 2.1 | NS |
| Postop SSD <0 mm | 93.3% | 93.8% | 100.0% | 92.6% | 90.3% | 88.9% | |
| Extension, deg | |||||||
| Normal knee | 6.0 ± 4.5 | 6.1 ± 4.6 | 6.2 ± 4.5 | 6.0 ± 4.4 | 5.7 ± 4.3 | 5.5 ± 4.6 | NS |
| Injured knee | 3.9 ± 4.9 | 3.8 ± 5.0 | 4.1 ± 4.6 | 4.6 ± 5.0 | 4.3 ± 3.6 | 3.4 ± 5.0 | NS |
a Data reported as mean ± SD unless otherwise indicated. ACLD, anterior cruciate ligament deficiency; ATS, anterior tibial subluxation; NS, not significant; Preop, preoperative; Postop, postoperative; sACL, space for the anterior cruciate ligament; SSD, side-to-side difference.
bP < .01 (group 1 vs groups 4, 5).
cP < .01 (group 1 vs groups 4, 5).
dP < .01 (group 2 vs group 5).