
Abstract
Background:
High tibial osteotomy (HTO) is a valuable treatment option in the high-demand patient with chondral damage and an altered mechanical axis. Traditional opening wedge HTO performed with metal plates has several limitations, including hardware irritation, obscuration of detail on magnetic resonance imaging, and complexity of revision surgery. Recently, an all-polyetheretherketone (PEEK) HTO implant was introduced, but no studies to date have evaluated the performance of this implant with minimum 2-year outcomes compared with a traditional metal plate.
Purpose:
To compare patient outcomes and complications of HTO performed using a traditional metal plate with those performed using an all-PEEK implant.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients who underwent HTO by a single surgeon with a minimum 2-year follow-up over a 4-year period were identified. Medical records were reviewed for patient demographics, concomitant procedures, implant used, type and degree of correction, complications, reoperations, and failures. Recorded patient outcomes included EuroQol–5 dimensions (EQ-5D), resiliency, Single Assessment Numeric Evaluation (SANE), Tegner activity level scale, International Knee Documentation Committee (IKDC), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores. HTO performed using a traditional metal plate served as the control group. Statistical analysis was performed using the Student t test for continuous variables and chi-square analysis for nonparametric data, with P < .05 considered significant.
Results:
A total of 41 patients (21 in the all-PEEK group, 20 in the control group) were identified with greater than 2-year follow-up. The mean patient age was 44 years, and there were no differences between the groups with regard to demographics, degree of correction, or concomitant procedures. In addition, no significant differences were found for any of the patient-reported outcomes. Complications (10% vs 15%, respectively; P = .59), failures (10% vs 5%, respectively; P = .58), and reoperations (10% vs 30%, respectively; P = .10) were similar for the all-PEEK and control groups. However, the all-PEEK group did not have any hardware removal, while 4 patients in the control group underwent hardware removal (P = .03).
Conclusion:
This study suggests that an all-PEEK implant may be safely used with comparable outcomes and complication rates to the traditional method but with less need for hardware removal.
Opening wedge high tibial osteotomy (HTO) can be an effective treatment option for the high-demand patient who has symptomatic unicompartmental arthritis with malalignment of the mechanical axis. The technical goal of HTO is to shift the mechanical axis of the knee away from the affected side to relieve pain and optimize the joint environment. The results of HTO are promising, with rates of return to sport and return to work reported at 87% and 85%, respectively. 2
Despite these results, numerous technical factors can hinder the success of the procedure. Such factors include lateral cortex fractures, loss of correction, neurovascular injuries, delayed/nonunion, and painful hardware. 7 With the exception of external fixation methods, maintenance of the HTO correction is traditionally completed with a metal plate. These plates have been shown to have drawbacks however, especially hardware irritation. A study by Niemeyer et al 6 reported a 41% rate of hardware irritation, and the rates of hardware removal have been reported as high as 60% to 99%. 1,6 Additional disadvantages of a metal plate include the obscuration of detail on magnetic resonance imaging and an increase in the complexity of revision surgery, including the need for removal of hardware for future joint arthroplasty.
Recently, a low-profile, all-polyetheretherketone (PEEK) HTO implant has been introduced to address some of these limitations. The implant material is a radiolucent, bioinert polymer that exhibits biomechanical strength properties similar to cortical bone. 5 In addition to being a different device (Figure 1), the all-PEEK implant entails differences in surgical technique, including unique cutting guides (allowing accurate proximal tibial cuts), the hinge pin (providing a stop to the saw cut laterally so as not to create a fracture that propagates to the lateral cortex), and the ability to perform soft tissue closure directly over the implant because of its low profile. There is a paucity of data, however, on the safety, outcomes, and complications of HTO using this system. The only study to date to compare this design with a metal implant was limited to 12 months and reported a higher rate of complications in the all-PEEK group. 3 No study to date has reported a comparison with a minimal 2-year follow-up between an all-PEEK implant and a metal implant for patient outcomes or complication rates.

Schematic demonstrating the all-PEEK high tibial osteotomy system.
The purpose of this study was to compare the clinical outcomes and complications of HTO using an all-PEEK implant versus a traditional metal plate. Our hypothesis was that the all-PEEK implant would produce outcomes comparable to HTO performed with a traditional metal plate but would obviate the need for hardware removal.
Methods
After institutional review board approval, all HTO procedures performed over a 4-year period by a single orthopaedic sports medicine fellowship–trained surgeon were identified. Nearly all of the traditional plate-and-screw HTO procedures were performed during the early part of the study period, while a transition was made to all-PEEK implants over the latter study period. Only 3 traditional plate-and-screw HTO procedures were performed beyond 2012 because of logistical reasons during the transition period, while all-PEEK HTO was otherwise performed from 2012 onward. The study group of interest included patients who underwent HTO performed with an all-PEEK implant (iBalance HTO System; Arthrex) versus a control group of patients who underwent HTO performed with traditional plate-and-screw systems (ContourLock HTO Plate [Arthrex]; VS Osteotomy Plate [EBI]).
Inclusion criteria for those undergoing HTO included physiological age less than 55 years, mechanical axis malalignment, higher desired activity level (Tegner >3), and those who were not good candidates for arthroplasty. Exclusion criteria included physiological age greater than 55 years, lower desired activity level (Tegner <3), lack of motivation, and those who would be better suited for arthroplasty. All patients had failed conservative treatment in the form of oral anti-inflammatory drugs, physical therapy, bracing, and activity modification and chose operative intervention to either maintain an active lifestyle or obtain pain relief.
Medical records were reviewed with reference to patient demographics, concomitant procedures, type of correction, degree of correction, complications, reoperations, and failures according to the type of implant used. No changes in the operative technique occurred during the study period. A complication was defined as an adverse event directly related to the index procedure, such as infection, fracture, deep venous thrombosis (DVT), hardware loosening as defined by radiolucent lines around hardware, or nonunion. Failure was defined as progression to knee arthroplasty or nonunion. A reoperation was defined as any subsequent procedure related to the index procedure, including hardware removal.
In addition to reviewing medical records, patients were contacted to retrieve latest follow-up patient-reported outcomes via mail or electronic completion. Resiliency, EuroQol–5 dimensions (EQ-5D), Single Assessment Numeric Evaluation (SANE), Tegner activity level scale, International Knee Documentation Committee (IKDC), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores were obtained in this manner. Resiliency is a measure of a patient’s ability to respond to adverse life events, while the EQ-5D is a standardized measure of overall health status or outcome. The SANE is an easily administrable evaluation based on the patient’s assessment of the affected area as a percentage of normal. The Tegner scale is a measure from 1 to 10 of successive levels of activity achieved, while the IKDC and WOMAC are commonly reported measures of knee outcomes.
These outcome variables as well as the aforementioned demographics, operative characteristics, complications, failures, and reoperations were compared between the all-PEEK group and control group. Statistical analysis for continuous variables was performed with the Student t test, while chi-square analysis was used for nonparametric data, with P < .05 considered significant.
Results
Overall, 66 patients underwent HTO from 2010 to 2014. We were able to contact and obtain a minimum 2-year follow-up on 41 of these patients, with 21 treated with an all-PEEK implant and 20 with a traditional metal plate and screws. Representative postoperative radiographs for each group are shown in Figure 2. All patients were bone grafted with a morselized allograft of cancellous bone and demineralized bone matrix. Eleven patients in the all-PEEK group and 14 patients in the control group were lost to follow-up, with no difference in the attrition rate between the groups (P = .56). The mean length of follow-up overall was 39 months (range, 24-64 months), with a slightly longer follow-up in the control group versus the all-PEEK group (47 vs 32 months, respectively; P < .05). The mean age overall was 44 years (range, 22-57 years), with no statistical difference between the groups (Table 1). Likewise, there were no differences in the sex distribution (76% vs 60% male, respectively; P = .26) or tobacco use (5% vs 20%, respectively; P = .14) between the all-PEEK and control groups (Table 1).

Postoperative radiographs of patients who underwent high tibial osteotomy with the (A) all-PEEK implant or (B) traditional metal plate implant.
Patient Demographics

In terms of surgical procedures, there was no overall difference between the all-PEEK and control groups in concomitant procedures (71% vs 60%, respectively; P = .44). The nature of the concomitant procedures did slightly differ between the groups, with more meniscal allografts in the all-PEEK group, but this did not reach statistical significance (24% vs 5%, respectively; P = .08) (Table 2). There were a similar number of microfracture procedures performed in the all-PEEK and control groups (48% vs 55%, respectively; P = .64). Two patients in the all-PEEK group underwent both microfracture and meniscal allograft transplantation, while 1 patient in this group underwent both of these procedures in addition to receiving an osteochondral allograft.
Concomitant Procedures

There was no significant difference in the complication rate between the all-PEEK and control groups (10% vs 15%, respectively; P = .59) (Table 3). Complications in the all-PEEK group included 1 patient with complex regional pain syndrome and 1 patient with DVT, while those in the control group included 1 patient with nonunion requiring a reoperation, 1 patient with hardware loosening without the need for removal, and 1 patient with an infection. Failure rates were not statistically different (10% vs 5%, respectively; P = .58), with 2 patients progressing to total knee arthroplasty in the all-PEEK group and 1 patient with nonunion in the control group. The overall reoperation rate likewise did not reach statistical significance, although it was notably lower in the all-PEEK group in comparison with the control group (10% vs 30%, respectively; P = .10). Both of the 2 reoperations in the all-PEEK group consisted of the aforementioned progression to total knee arthroplasty at 14 months and 24 months. Subsequent operations in the control group consisted of 4 hardware removals (21, 24, 26, and 36 months) for symptomatic hardware, with 1 performed in conjunction with receiving a subsequent osteochondral allograft (36 months), 1 nonunion revision (24 months), and 1 irrigation and debridement for an infection (1 month). The rate of hardware removal was significantly higher in the control versus the all-PEEK group (20% vs 0%, respectively; P = .03) (Table 3).
Overall, clinical scores were similar between the all-PEEK and control groups, respectively (SANE, 76.5 vs 67.1 [P = .25]; IKDC, 61.9 vs 53.8 [P = .23]; WOMAC, 21.5 vs 28.2 [P = .32]). There were also no between-group differences in the remaining outcome scores (EQ-5D, 6.8 vs 6.9 [P = .82]; Tegner, 3.6 vs 3.7 [P = .92]). There was no difference in resiliency between the groups (P = .96) (Table 4).
Procedure Characteristics

a Defined as progression to total knee arthroplasty or nonunion during follow-up.
b For any reason (including hardware removal, further articular cartilage procedure, etc).
Outcome Measures a
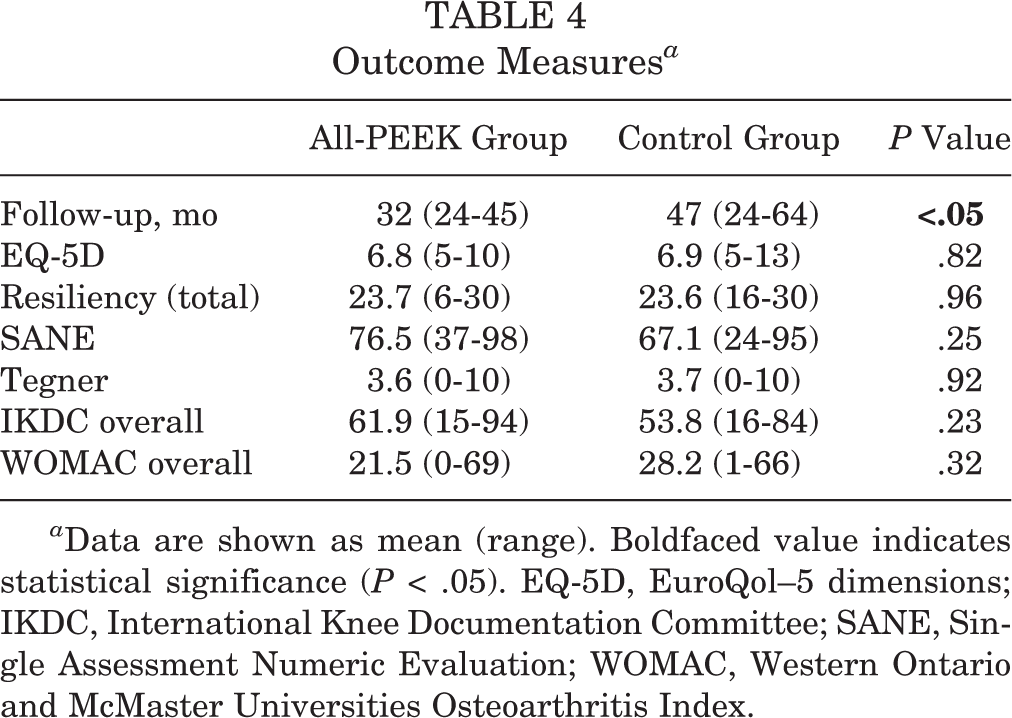
a Data are shown as mean (range). Boldfaced value indicates statistical significance (P < .05). EQ-5D, EuroQol–5 dimensions; IKDC, International Knee Documentation Committee; SANE, Single Assessment Numeric Evaluation; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Discussion
The results of this study show that the all-PEEK group exhibited similar clinical outcomes to the control group but with a lower reoperation rate for symptomatic hardware in HTO in active patients with mechanical malalignment. Furthermore, there were no differences in the complication rate between the 2 groups.
Few previous studies have evaluated the all-PEEK implant system. Getgood et al 3 published a case-control study of 32 patients in which they compared the all-PEEK system to the second-generation Puddu system (Arthrex) and TomoFix (DePuy Synthes), and they reported a higher complication rate in the all-PEEK group but a similar efficacy profile. However, the study was multicenter, involving 5 different surgeons, and the follow-up was limited to 12 months. Furthermore, there was only 1 microfracture procedure performed and no meniscal allografts received among their total 64 patients. Ghinelli et al 4 published a case series of 15 patients who underwent HTO using the all-PEEK system, and they reported an overall safe profile with satisfactory results. However, the study was limited, with a small number of patients and lack of a comparison group.
The clinical outcomes of patients in the current study who underwent HTO employing the all-PEEK implant are comparable to those published in a previous study by Ghinelli et al. 4 At 2-year follow-up, they reported outcome scores of 73.6 for the IKDC and 3.1 for the Tegner scale. In the current study, the clinical scores at a mean follow-up of 3.9 years were 61.9 for the IKDC and 3.6 for the Tegner scale. The slightly lower IKDC scores in the current study may be a reflection of the concomitant procedures performed in these patients. Although 12 patients (80%) in the Ghinelli et al 4 study underwent partial meniscectomy, only 3 of these also underwent focal cartilage repair, with 1 of these involving a meniscal scaffold. In contrast, in the current study, 24% of patients in the all-PEEK group underwent meniscal allograft transplantation, and 48% underwent microfracture. Thus, the cohort in our study may have had lower baseline IKDC scores because of more severe knee abnormalities.
Although indications for when to perform concomitant procedures to address meniscal or cartilage lesions can be controversial, the senior author (D.J.W.) generally performs arthroscopic surgery on all patients undergoing HTO. Often, there is a meniscus to debride or abrasion chondroplasty to perform if there is a large area of grade IV changes. If there are advanced cartilage changes on both the femoral and tibial sides, cartilage restoration will not be pursued. However, if the patient exhibits higher activity demands and has more focal areas of cartilage lesions, the appropriate cartilage and meniscal procedures will be added for joint restoration.
The complication rate in the all-PEEK group in our study was 10%, with the 2 complications being complex regional pain syndrome and DVT in separate patients. The study by Getgood et al 3 also reported 1 case of DVT. In addition, their study reported 2 intraoperative fractures in their all-PEEK group but attributed such errors to the early learning curve. They subsequently moved the fulcrum of the osteotomy more distally from the joint line. We did not have any intraoperative fractures, likely because of the avoidance of placing the osteotomy too close to the joint line.
Of note, with metal implants used in other systems, patients often report high rates of soft tissue irritation (41%), which often leads to hardware removal with rates as high as 60% to 99%. 1,6 There were no hardware removal procedures performed in the all-PEEK group, while the control group had 4 patients (20%) who required hardware removal. The overall follow-up of the control group was in fact longer than that of the all-PEEK group; however, hardware removal in the control group occurred at 21, 24, 26, and 36 months, which fell well within the follow-up period for the all-PEEK implant. This lower rate of hardware removal may be caused by the low profile of the all-PEEK implant and its bioinert properties. A theoretical advantage of the all-PEEK implant includes the ease of magnetic resonance imaging without metal artifacts. This issue becomes important with the need for future imaging to monitor meniscal and cartilage abnormalities. Finally, there is no need to remove the all-PEEK implant to perform total knee arthroplasty, as was the case in 2 patients of the all-PEEK group, thus making revision surgery faster and simpler.
However, there are some potential issues with the use of the all-PEEK implant. In the setting of an infection, if hardware removal is necessary, it would be difficult to maintain any construct stability. In our cohort, we had 1 patient who required irrigation and debridement but did not need hardware removal. In more complex arthroplasty cases involving stems and augments, the all-PEEK implant may need to be removed.
The current study does have some limitations. Because the all-PEEK system has only recently been developed, the number of patients enrolled was small. While a general observation of some improvement in outcome scores was noted in the all-PEEK group, this did not reach statistical significance. A larger number of patients may have allowed us to reach statistical differences in both outcome scores and reoperation rates. It remains to be seen, however, whether these differences are clinically important. Second, 2 consecutive groups of patients undergoing different types of techniques were compared. A randomized study would have potentially decreased any unforeseen bias or variables. In addition, neither baseline clinical scores nor body mass index data were obtained for either group, which would have allowed us to compare baseline differences and also note changes in improvement between the groups. The control group did have a greater number of smokers, but this did not reach significance. Third, the rate of meniscal transplants was likely higher in the all-PEEK group but did not result in a higher complication rate. While this represents a potential confounder, it might be expected that these more complex cases would lead to higher complication rates if it were to affect outcomes. Fourth, there was a lack of postoperative radiographic data to track changes in alignment or slope. Fifth, 2 different plates were used in the control group, which introduces a potential confounding variable. Finally, the study’s mean follow-up period was 3.3 years. Although this is the longest follow-up study to date for this novel HTO system, a longer follow-up would have allowed us to better evaluate the progression to total knee arthroplasty between the groups.
Conclusion
Using an all-PEEK implant for HTO leads to comparable clinical outcomes and complications to traditional methods, with a decreased rate of hardware removal because of soft tissue irritation.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Greenville Health System.