
Abstract
Background:
In recent years there has been an increasing interest in high tibial osteotomy (HTO) to treat patients with chronic knee instability due to posterolateral corner (PLC), posterior cruciate ligament (PCL), and anterior cruciate ligament (ACL) insufficiencies with concurrent malalignment in the coronal and/or sagittal plane.
Purpose:
To perform a systematic review of the use of HTO for the treatment of knee ligament instability with concurrent malalignment.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review of the literature was conducted for the treatment of combined knee ligament instability and malalignment with HTO using the Cochrane Central Register of Controlled Trials, PubMed, and MEDLINE (1980 to present); the queries were performed in July 2015. Terms searched included the following: high or proximal tibial osteotomy, unstable, instability, laxity, subluxation, tibial slope, and malalignment, in the knee joint. Inclusion criteria were as follows: HTO to treat instability of the knee joint in the sagittal and/or coronal plane, minimum 2-year follow-up with reported outcomes measures, English language, and human studies. Animal, basic science, and cadaveric studies were excluded as well as editorials, reviews, expert opinions, surveys, special topics, letters to the editor, and correspondence.
Results:
The search resulted in 460 studies. After applying exclusion criteria and removing duplicates, 13 studies were considered. Of the studies reviewed, knee ligament pathologies, previous surgeries, and measurement of knee stability were heterogeneous. However, all studies reported an improvement in knee stability after HTO. Most studies reported improvement in outcome scores. However, other studies did not provide preoperative scores for comparison. Reported complication rates ranged from 0% to 47%.
Conclusion:
Although HTO has been highly advocated and used in treating patients with ligamentous knee instability, there remains a paucity of high-quality studies. Included studies report improvement of instability as well as relatively high patient satisfaction and rate of return to sports. The heterogeneity of the pathology treated, follow-up time, and outcome measures limit comparison between studies.
High tibial osteotomy (HTO) is a widely accepted procedure to treat unicompartmental processes such as overload or osteoarthritis 14 by shifting the mechanical axis to realign the load. 3 This, in turn, can diminish pain, improve function, and ultimately lead to a slower progression toward osteoarthritis. 3
However, HTO has recently been advocated and used to treat chronic knee instabilities (such as anterior cruciate ligament [ACL], posterolateral corner [PLC], and posterior cruciate ligament [PCL] instability) 1 and ligament reconstruction failure due to malalignment 3 and to protect a concurrent ligament reconstruction. 28 The 3 main goals for HTO in ligament-deficient knees are (1) to prevent further unilateral compartment deterioration in a knee that is demonstrating signs of articular cartilage wear, (2) to protect the graft(s) from abnormally high stress in a malaligned knee, 12 and (3) to restore stability. 18 Nevertheless, additional surgery could expose the patient to an added risk from the procedure itself or from prolonged rehabilitation. 12
An important consideration in performing an HTO for the treatment of malalignment and ligament instabilities is the ability to simultaneously correct both the coronal and sagittal axis malalignment with 1 cut (biplanar osteotomy). Failure of the surgeon to recognize this ability can lead to inadvertent negative consequences for the graft (ie, increasing posterior slope with a valgus-producing HTO for an ACL-deficient patient can increase stresses on the ACL graft). 14
Literature available regarding HTO and knee instability is highly heterogeneous with respect to indications, timing, and outcomes. The purpose of this study was to systematically review the literature of HTO outcomes for knee ligament instability and malalignment to determine whether HTO improves postoperative stability, according to patient-reported stability, as well as: the Lachman test and the pivot shift test in cases of ACL deficiency, the posterior drawer test for PCL deficiency, and the reverse pivot shift test and the varus stress test in cases of PLC deficiency. Secondarily, we sought to determine postoperative patient reported outcomes, return to activity, patient satisfaction, and complication rates.
Methods
Article Identification and Selection
This study was conducted in accordance with the 2009 Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement. 17 A systematic review of the literature about the existing evidence for the treatment of ligamentous instability of the knee with HTO was performed using the Cochrane Central Register of Controlled Trials, PubMed, and MEDLINE from 1980 to present; the queries were performed in July 2015.
The literature search strategy included the following: search 1: (“HTO” OR “High tibial osteotomy” OR “PTO” OR “Proximal Tibial Osteotomy”) AND (unstable OR instability OR laxity OR subluxation OR “tibial slope” OR “knee malalignment” OR “knee alignment” OR “chronic posterolateral” OR “revision knee surgery”); search 2: “tibia*” AND “osteotomy” AND (unstable OR instability OR laxity OR subluxation). Inclusion criteria consisted of high or proximal tibial osteotomy to treat instability of the knee joint, minimum 2-year follow-up with report on outcomes, English language, and human studies. Exclusion criteria included animal studies, basic science studies, cadaveric studies, editorials, reviews, expert opinions, surveys, special topics, letters to the editor, and correspondence. Additionally, we excluded all other joint studies besides the knee joint.
Three investigators (C.S.D., D.J.L., J.C.) independently reviewed the abstracts from all identified articles. Full-text articles were obtained for review if necessary to allow the application of inclusion and exclusion criteria. Additionally, all references from the included studies were reviewed and reconciled to verify that no relevant articles were missing from the systematic review. Inclusion and exclusion criteria were sequentially used to identify relevant articles, as shown in the PRISMA flowchart (Figure 1). For studies not available online, print copies were accessed from the library at the Steadman Philippon Research Institute, Vail, Colorado, USA.
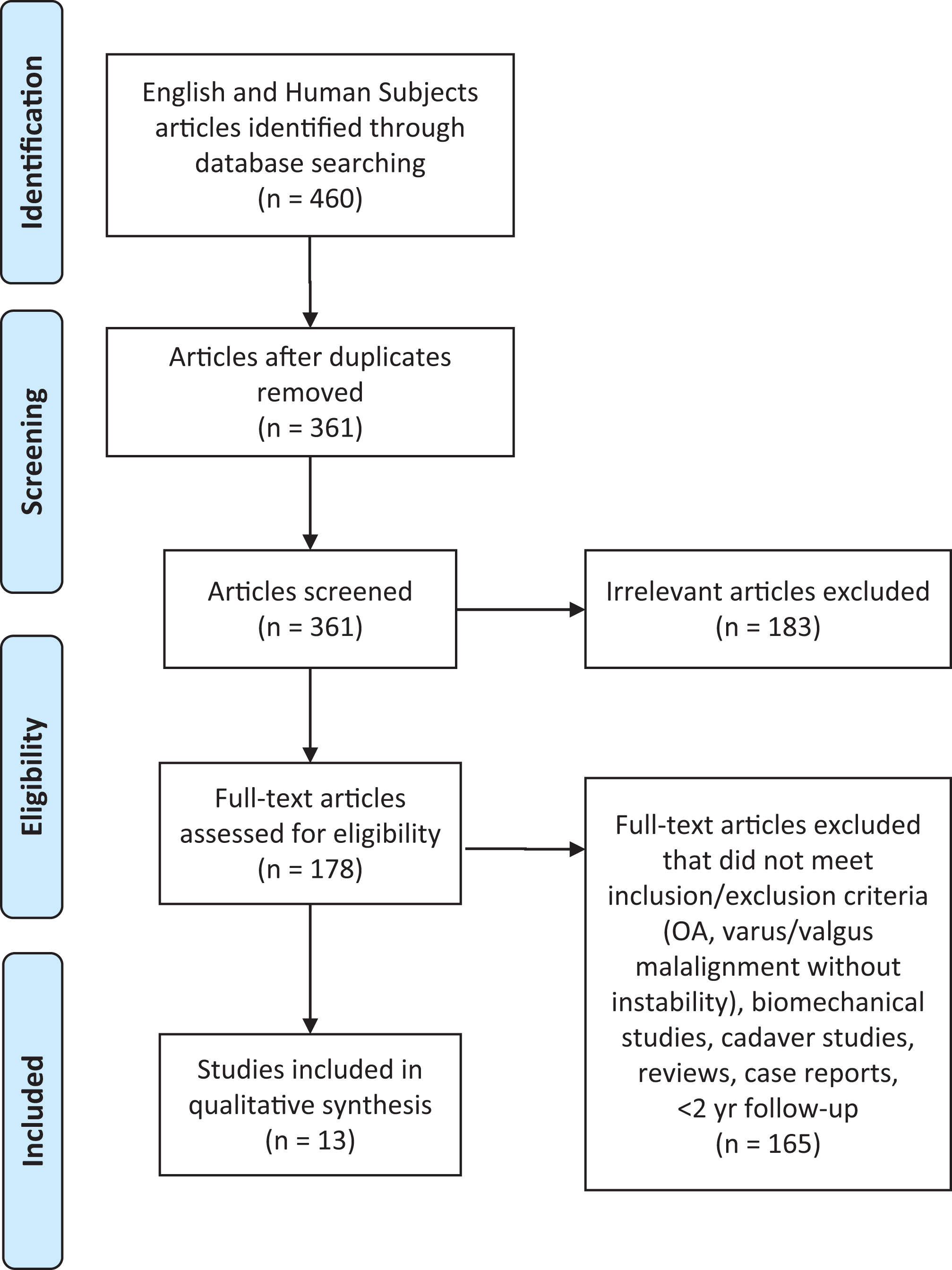
Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flowchart of the article selection with inclusion and exclusion criteria. OA, osteoarthritis.
Data Collection
Following the classification from Wright et al, 27 the level of evidence was assigned. The information was collected from the abstracts of the included studies. Pre- and postoperative instability was extracted and recorded as subjective instability, Lachman test, and pivot shift test. Additionally, patient demographics, follow-up, patient satisfaction, subjective outcomes, return to sport, and complications were extracted and recorded. For continuous variables (eg, age, timing, follow-up, outcome scores), the mean and range were collected if reported. Data were recorded into a custom Microsoft Excel spreadsheet (Microsoft Corp) using a modified information extraction table. 9
Bias
There can be inherent selection and performance bias in evidence level 3 and level 4 studies because of the lack of randomization and prospective comparative control groups, especially in populations characterized by heterogeneity in injuries. Selected studies were reviewed to ensure that authors minimized bias while recognizing the constraints present with such studies.
Results
The systematic search performed using the previously mentioned keywords identified 361 studies after duplicates were removed. Of these, 183 were not related to our topic, leaving 178 studies. Of these, 66 studies did not include or report on instability, and 27 of the remaining studies did not report on outcomes. Other studies that were eliminated included 25 cadaveric/biomechanical studies, 18 reviews, 13 case reports, 10 expert opinions, 4 surgical technique reports, 1 that did not include HTOs, and 1 instructional course lecture. After applying all exclusion criteria, 13 studies were considered for insightful data, including 3 studies 1,18,25 with all opening-wedge cases and 6 studies 19 –22,26,28 with all closing-wedge cases. Four studies 2,4,5,15 included a mixture of opening- and closing-wedge osteotomies (Tables 1-4). The included studies reported on a total of 353 patients treated with HTO for several different etiologies of knee instability. The mean follow-up was reported between 2.5 and 12 years. 4,19 There was substantial heterogeneity of indications, subjective outcomes, and objective outcomes within the included studies. The most commonly reported measures were subjective instability, patient satisfaction, return to sport, and complications. On the contrary, the use of subjective outcomes scores varied widely.
Instability and Joint Laxity a

a ACLR, anterior cruciate ligament reconstruction; HTO, high tibial osteotomy; PCLR, posterior cruciate ligament reconstruction; PLCR, posterolateral corner reconstruction; postop, postoperation; preop, preoperation.
Satisfaction and Outcomes a

a ACLR, anterior cruciate ligament reconstruction; HSS, Hospital for Special Surgery; HTO, high tibial osteotomy; IKDC, International Knee Documentation Committee; PCLR, posterior cruciate ligament reconstruction; PLCR, posterolateral corner reconstruction; postop, postoperative; preop, preoperative; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Return to Sport a
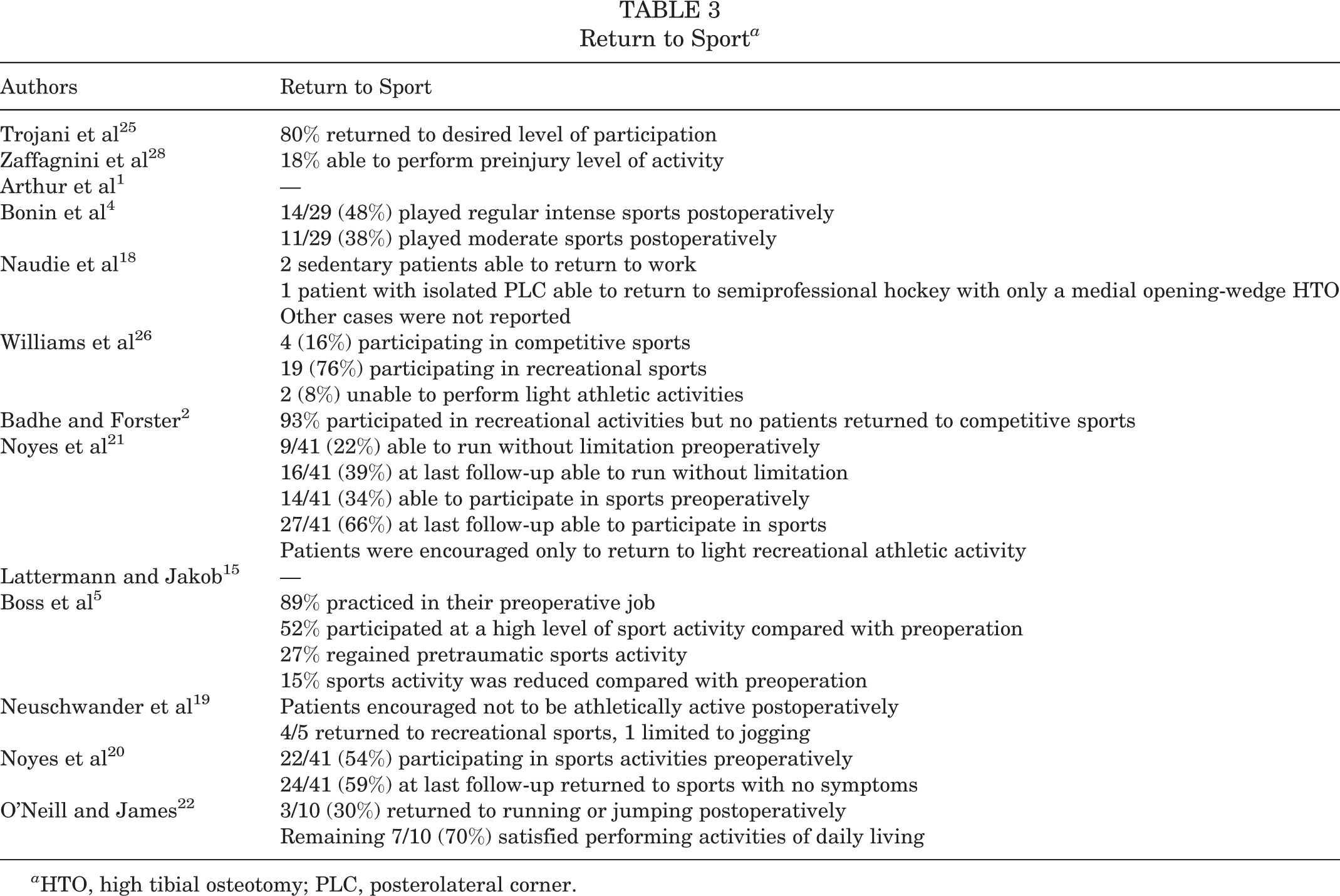
a HTO, high tibial osteotomy; PLC, posterolateral corner.
Complications a
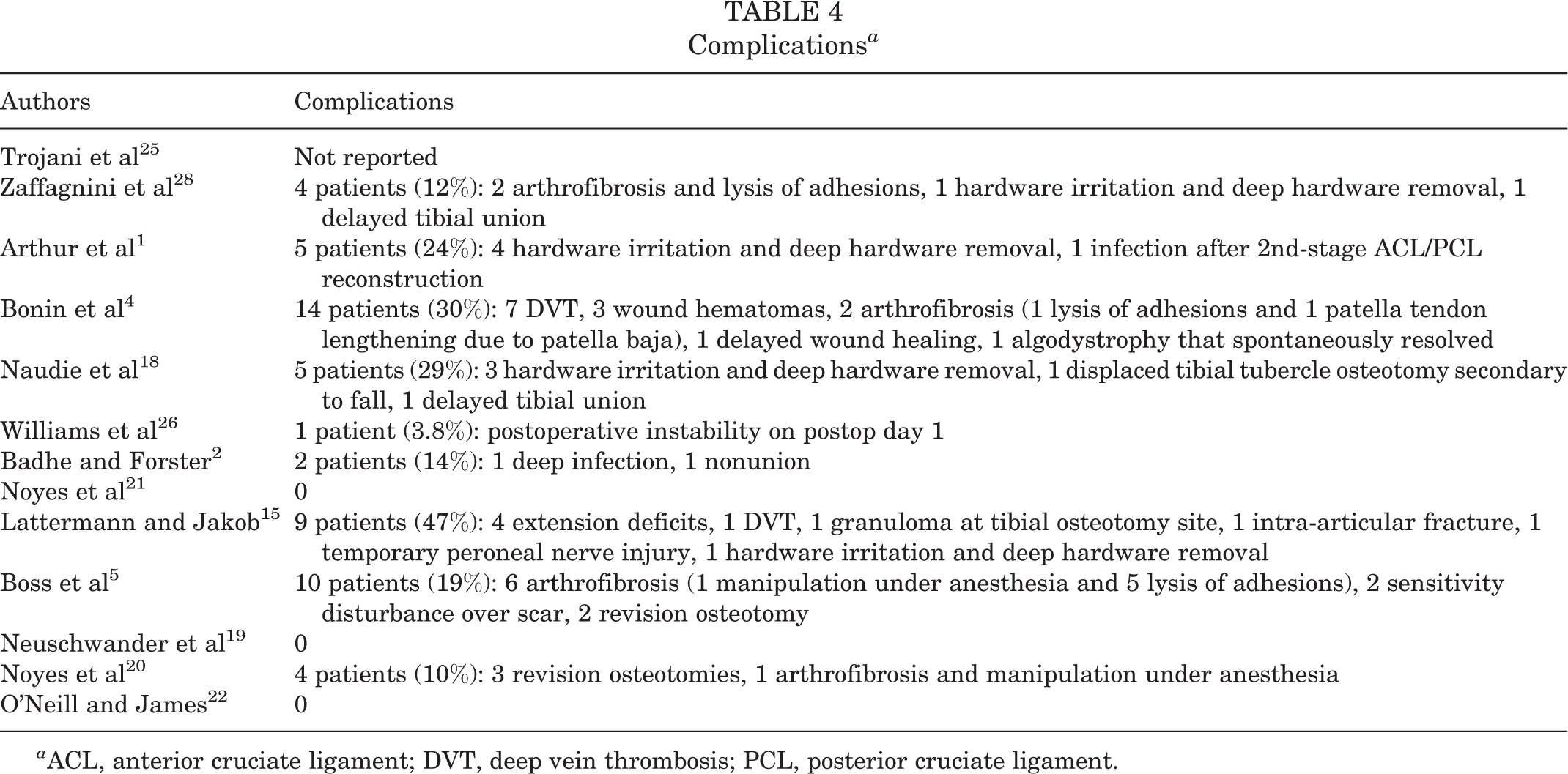
a ACL, anterior cruciate ligament; DVT, deep vein thrombosis; PCL, posterior cruciate ligament.
HTO in ACL-Deficient Knees
Eleven of the studies evaluated the effect of HTO in patients with ACL deficiency. Seven of the studies had HTO with ACL reconstruction either concurrently or as a staged procedure, while 1 study performed HTO as the treatment procedure. In 3 studies, the subjects had either HTO alone or HTO with ACL reconstruction. Two of the 11 studies reported on knee stability using the pivot shift and Lachman tests; 2 studies reported on patient subjective feeling of instability, pivot shift, and Lachman tests; 1 study used only the Lachman test; and 3 studies did not report on knee stability (Table 1). HTO alone was reported to improve knee stability in ACL-deficient knees. However, combined HTO with ACL reconstruction either as a staged procedure or simultaneous procedure was reported to improve postoperative stability better than HTO alone, as judged by patient-reported stability, the Lachman test, and the pivot shift test. HTO alone did not always restore adequate stability. Nonetheless, Noyes et al 20 reported no significant difference between patients treated with HTO alone and those treated with HTO and ACL reconstruction. However, it should be noted that in this study patients were advised to only return to light recreational athletic activities.
The knee outcome subjective scores were also used in some studies, but the outcome scores used were heterogeneous. Three studies reported on Tegner activity score with a preoperative mean of 3.5 in 2 studies and a postoperative mean of 5.0 in 3 studies. Neuschwander et al 19 did not report preoperative Tegner score. The Lysholm score was reported in only 2 studies. The Lysholm score improved from 48.6 preoperatively to 81.7 postoperatively. Six studies reported the International Knee Documentation Committee (IKDC) scores. The mean preoperative IKDC score was 48.5 based on 2 studies. In 4 studies, the mean postoperative IKDC score was 73.6. In the other 2 studies, the knees were evaluated as normal or nearly normal (IKDC “A” and “B”) in 60.5%, abnormal (IKDC “C”) in 32.5%, and severely abnormal in 7% of patients.
High Tibial Osteotomy in PLC-Deficient and Combined PLC-Deficient Knees
Four studies 1,2,18,21 included patients with combined PLC-deficient knees. There were few patients with combined ligament pathologies in the studies included in this review. Furthermore, combined ligament injuries were highly heterogeneous. Patients with combined ligament pathology were treated first with HTO, and those with persistent instability were treated with a staged ligament reconstruction. Arthur et al 1 reported on 21 patients with combined chronic PLC deficiency and genu varum malalignment. In their study, 38% of the patients obtained satisfactory stability after HTO and did not require ligament reconstruction. Naudie et al 18 reported on 17 knees in 16 patients that received either medial opening-wedge HTO or combined medial opening-wedge HTO with tibial tubercle osteotomy for hyperextension-varus thrust. Among them, 5 of 16 patients reported continued posterolateral instability and went on to have second-stage PCL reconstruction after initial HTO. 18 In a study by Noyes et al, 21 all patients (N = 18) with triple varus (tibiofemoral varus geometry, separation of lateral compartment, increased external tibial rotation and hyperextension with varus recurvatum) included in the study required PLC reconstruction, while those with double varus (tibiofemoral varus geometry, separation of lateral compartment due to deficiency of the lateral soft tissue) did not need this procedure after HTO. None of the studies reported pre- and postoperative grading of instability tests for patients with PCL and or PLC deficiencies.
Patient Satisfaction, Complications, and Return to Sport
Patient satisfaction at final follow-up was reported in 7 studies and ranged from 75% to 97%, 5,25 with improvement in subjective stability and all outcomes scores regardless of preoperative diagnosis and procedure performed. Of patients who were dissatisfied in this systematic review, 1 had significant weight gain postoperatively and others expressed dissatisfaction from not being able to return to a desired level of activity. 14,27 In 1 study, the majority of patients emphasized that they would prefer exact and realistic activity counseling prior to surgery to adjust their postoperative goals. 15
Rates of return to sport were reported in 11 of 13 studies and ranged from 18% to 80%. 23,28 However, the definition of return to sport varied between studies as did counseling on postoperative limitations, making comparison difficult. For example, in the study by O’Neill and James, 22 only 30% of patients returned to running or jumping activities while 70% of patients were satisfied performing activities of daily living. The study by Neuschwander et al 19 discouraged patients from returning to athletic activity, and the study by Noyes et al 21 recommended only returning to light recreational athletic activities.
Complications were reported in 12 of 13 studies, ranged from 0% 19,21,22 to 47%, 9 and included a wide variety of pathologies. The most commonly reported complication was postoperative stiffness due to arthrofibrosis that resulted in loss of range of motion. Postoperative stiffness accounted for a total of 11 patients in 4 of the 13 studies. 4,5,20,28 All of these patients underwent manipulation under anesthesia with or without arthroscopic lysis of adhesions. Hardware irritation requiring surgical removal was reported in 4 studies 1,14,18,20 and was experienced by 9 patients. Delayed tibial union was a reported complication in 2 patients 18,28 (1 was treated with an external fixator and 1 was treated with prolonged protected weightbearing) and nonunion in 1 patient 2 (treated with an external fixator), all of whom went on to complete union and outcome scores that were not significantly different than their cohorts. Of note, Bonin et al 4 reported postoperative deep vein thrombosis confirmed by ultrasound in 23% of their patient population. Across all studies, only 1 other case of deep vein thrombosis was reported. 14 The summarized results of HTO regarding instability are listed in Table 1, patient satisfaction and outcomes in Table 2, complications in Table 3, and return to sport in Table 4.
Discussion
The most important finding of this systematic review was that HTO has an important role in treating patients with knee ligament instability, with good reported outcomes for ACL, PCL, and combined PLC injuries in the knee. Knee ligament injuries are heterogeneous, and therefore, a thorough preoperative diagnostic workup is important, including clinical examination and imaging studies (particularly long leg alignment radiographs and stress radiographs for PCL and collateral ligament injuries).
High tibial osteotomy can either be performed alone, with simultaneous ligament reconstruction, or as a staged procedure with HTO first followed by ligament reconstruction in cases of persistent instability. There are conflicting results of whether to perform ACL reconstruction simultaneously with HTO. In a study by Noyes et al, 20 the authors reported no significant differences between patients treated with HTO alone, HTO with a Losee-type extra-articular procedure, or HTO with ACL reconstruction regarding symptoms of pain, swelling, and giving way. Lattermann and Jakob 15 reported high complication rates with simultaneous HTO and ACL reconstruction procedures compared with either HTO alone or a staged procedure. No other study in this review reported a high complication rate with simultaneous HTO and ACL reconstruction procedures. The other studies included in this review suggest that HTO can be safely performed simultaneously with ACL reconstruction. 4,5,19,20,22,25,26,28 A recent systematic review by Li et al 16 reported improvement of subjective scores, and most participants returned to recreational sports after a simultaneous HTO and ACL reconstruction in young patients with medial compartment osteoarthritis and ACL deficiency.
A staged procedure, however, seems to be advantageous in knees with PLC and PCL injuries. Several studies performed high tibial osteotomy first followed by ligament reconstruction performed at a later stage for patients who had persistent instability. The rationale for performing HTO first is to correct malalignment and protect any future reconstruction grafts from excessive stress and to restore stability. Several studies reported improvement of stability in patients with posterolateral and/or lateral ligament deficiency to the degree that they did not require secondary ligament reconstruction procedures. 1,18,20 However, a staged procedure has the disadvantage of longer rehabilitation. Therefore, different etiologies of knee instability may require different approaches.
Addressing both the coronal and sagittal planes is essential to restore knee stability. Biplanar HTO simultaneously addresses alignment in the coronal plane and tibial slope in the sagittal plane. Recently, Dejour et al 7 reported on the outcomes of second-revision ACL reconstruction combined with tibial deflexion osteotomy (when it exceeds 12°) at minimum follow-up of 2 years suggesting that tibia slope correction protects a reconstructed ACL graft from stress failure. Likewise, Sonnery-Cottet et al 24 performed a proximal tibial anterior closing-wedge osteotomy in a re-revision ACL reconstruction setting in 5 patients with a mean follow-up of 31.6 months. They reported that this combined procedure restored knee stability and function with satisfactory clinical outcomes. A biomechanical study by Giffin et al 8 showed that increasing the tibial slope results in an anterior shift in the tibial resting position, which is accentuated under axial loads. Their findings suggest that decreasing the tibial slope may be protective in an ACL-deficient knee. 8,23 Furthermore, the authors theorized that decreasing the tibial slope minimizes the anteroposterior component of the joint contact forces and thereby decreases the anterior subluxation of the tibia relative to the femur. This may alleviate the anterior instability symptoms in patients with chronic ACL deficiency. This can be a potential alternative for older patients with degenerative osteoarthritis in whom ACL reconstruction is a relative contraindication. On the contrary, these findings by Giffin et al 8 suggest that increasing the tibial slope may be beneficial in reducing tibial sag in a PCL-deficient knee. 8,23 This will theoretically relieve the posterior instability symptoms in patients with chronic PCL injuries.
Opening-wedge HTO has been reported to increase the tibial slope. 1,13,23 The degree of slope change also depends on the positioning of the plate, as reported by LaPrade et al 13 (anteriorly placed plates increase the sagittal plane slope and posteriorly placed plates can decrease the slope). It has been recommended to use opening-wedge HTO in patients with chronic PCL injuries and/or posterolateral instability where increasing the tibial slope is desired. 18 In opening-wedge osteotomy, the fibula is not disrupted, which reduces the risk of fibular migration and disruption of the proximal tibiofibular joint. Therefore, opening-wedge osteotomy is particularly advantageous in chronic posterolateral corner injuries. Badhe and Forster 2 reported better results with opening-wedge HTO than closing-wedge HTO in patients with triple varus deformity. Closing-wedge HTO has been reported to decrease the tibial slope. 6,19,21 Closing-wedge HTO has therefore been advocated for chronic ACL-deficient knees where decreasing the tibial slope is desired. Both opening- and closing-wedge HTO have been reported to decrease the patellar height. 11,13 The possibility of a shortened patellar tendon should be evaluated when considering a bone–patella tendon–bone autograft for a later ACL reconstruction.
Favorable outcomes of combined HTO and ligamentous procedures are evident in this systematic review. Studies with combined ACL reconstruction and HTO tended to report higher postoperative activity levels when compared with HTO alone. However, postoperative Tegner activity scores improved in all patient groups, even those who had received HTO alone. This may be more reflective of the impact knee instability has on activities of daily living. Noyes et al 20 reported good results and no significant difference between HTO alone compared with both HTO with ACL reconstruction and HTO with extra-articular Losee procedure. For this reason, HTO is an interesting option in patient populations where ligament reconstruction does not always have favorable outcomes, such as older patient populations and patients with low general activity demands.
As an alternative to HTO, distal femoral osteotomy may be useful for the treatment of malaligned knees with medial knee ligamentous instability. Hetsroni et al 10 recently performed a biomechanical analysis of lateral opening-wedge distal femoral osteotomy in valgus malaligned cadaveric knees that were superficial medial collateral ligament–deficient. They reported a decrease in medial joint opening at 30° of knee flexion when under a valgus load of 9.8 N. Clinical studies that focus on the results of a distal femoral osteotomy in patients with combined genu valgus malalignment and chronic medial collateral ligament injuries are needed.
There were some limitations to our study. First, this systematic review included almost entirely level 4 evidence studies consisting of retrospective and prospective case series. Second, despite increased attention of HTO in the ligament-deficient patient, only 2 of the included articles were published in the past 8 years. Additionally, because of the complex injuries of included patients, the reported patient population was considerably heterogeneous. Furthermore, many of these patients had additional ligament reconstructions performed at the same time or staged so the improvement in outcomes may be related wholly or in part to the ligament reconstructions. While we believe conclusions can be drawn from this study, these 2 factors limit the usefulness of performing a quantitative meta-analysis of the pooled patient data. Therefore, a qualitative analysis was performed. Finally, as there were a large number of articles reviewed, relevant articles may have been missed and inadvertently excluded. We attempted to control for this error with 3 reviewers who independently reviewed each article.
Conclusion
High tibial osteotomy has been reported to be useful for the treatment of ligament-deficient knees with significant varus or sagittal plane malalignment. However, there is need for additional high-quality comparative studies in this patient population involving combined HTO and ligament reconstruction versus ligament reconstruction alone.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. receives royalties from Arthrex and Smith & Nephew; is a paid consultant for Arthex, Ossur, and Smith & Nephew; receives research support from Arthrex, Linvatec, Ossur, and Smith & Nephew; and has patents pending with Ossur and Smith & Nephew.