
Abstract
Background:
Previous studies have identified the effect of sport-related concussion on health-related quality of life through the use of patient-reported outcome measures. However, there has been little research exploring the underlying mechanisms that influence these perceptions of health-related quality of life among adolescent athletes who have sustained a sport-related concussion.
Purpose:
To explore the psychosocial aspects of concussion among adolescent athletes.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 12 interscholastic athletes (4 girls, 8 boys; mean ± SD age, 15.7 ± 1.7 years; grade level, 10.2 ± 1.4) were interviewed via a semistructured interview protocol between 15 and 30 days postinjury. Data analysis was guided by the consensual qualitative research tradition. Themes and categories emerged through consensus by a 3-person research team, and bias was minimized through the use of multiple-analyst triangulation.
Results:
Participants identified numerous postconcussion symptoms that resulted in increasing difficulty with emotions (eg, irritable, easily frustrated), roles at school (eg, concentration difficulties, fatigue), and roles in their social environment (eg, letting the team down, not being able to contribute to sport). As a result, participants expressed how they tried to minimize or mask symptoms to decrease the potential of being viewed differently by their peers.
Conclusion:
Adolescent athletes perceived a significant effect of sport-related concussion on numerous areas of psychosocial and emotional health and well-being. Anticipatory guidance—with education regarding the possible signs and symptoms, risk factors, and recovery expectations following a concussion—is important to include in postinjury management. A better understanding of sport-related concussion and expected recovery could help to improve perceptions of this injury among interscholastic athletes. Additionally, best practices should be identified to assist health care professionals and school personnel in the development of temporary adjustments or formal academic adjustment policies in the secondary school setting, therefore ensuring that the patients receive the support that they need to maintain their roles as students.
Sport-related concussions are a significant public health concern among youth and adolescent athletes. Each year, between 1.1 and 1.9 million sport-related concussions occur in the United States, 5 with a majority occurring within the pediatric and adolescent age groups. 15 Concussion results in a variety of symptoms, deficits in cognition, and balance impairments that may affect the daily functioning of the patient in addition to restricting participation in sport. Historically, studies focused on the acute effects of concussion-related impairments, including symptom presentation, cognition, and balance from the time of injury through return to play. 4,29
More recently, there has been a trend to evaluate concussion from the patient’s perspective, taking a whole-person approach to the assessment and management of the injury. 49 As a result, emphasis has been placed on the effect of concussions on academic performance, 14,39,55 sleep, 2,36 emotions, 11,20,21,23,27 and quality of life. 19,22,32,35,47 These studies have collectively noted that concussion can result in increased fatigue, decreased vigor, increased total mood disturbance, depression, academic dysfunction, and lower physical and psychosocial perceptions of health. As a result, there has been an increased emphasis on concussion with respect to the implementation of academic adjustments and return to school, 56,58 as this is a primary role of adolescents. Academic adjustments can be formal or informal modifications to a student’s academic load (eg, more time for assignments) or the school environment (eg, rest breaks in a quiet room) to facilitate recovery following concussion. 14
Health-related quality of life (HRQOL) is a concept that considers the physical, psychological, and social aspects of one’s health and is defined by the individual’s experiences, beliefs, expectations, and perceptions of his or her ability to function in numerous domains of health and well-being. 45 Sport-related concussion symptoms and impairments can negatively influence aspects of HRQOL 19,22,32,35,47,52,60 and should be an important component of concussion assessment. As there is currently no patient-reported outcome measure for sport-related concussion, 49 researchers have used a combination of outcomes to assess aspects of HRQOL: generic (eg, Pediatric Quality of Life Inventory), 19,35,52 specific (eg, Beck Depression Inventory, Profile of Mood States), 20,23,27 and single item (eg, Global Rating of Change). 47 While these measures provide a basic understanding of the effect of a concussion on domains of HRQOL, they fail to provide deeper insight into the specific reasons for and meanings behind perceived perceptions of injury.
In contrast, studies based on a qualitative approach may provide better insight into the influence of a sport-related concussion on the psychosocial experiences with HRQOL as an analytic framework. It is unclear as to the magnitude of the effect of concussion on aspects of HRQOL when identified closer to the time of injury. Our purpose was to explore adolescent athletes’ perceptions regarding the psychosocial aspect following a sport-related concussion.
Methods
Experimental Design
Data were collected prospectively during the 2009-2012 academic years as part of a larger prospective investigation of the influence of sport-related concussion measures of impairment and HRQOL. 19 In-person, qualitative interviews were conducted with participants and their parents during the subacute phase after a sport-related concussion (approximately 15-30 days), with follow-up interviews during the first 2 months after the concussion. For the purpose of this study, the focus was on the initial interviews with the adolescents, which addressed their lived experiences following a sport-related concussion, with HRQOL as a theoretical framework.
Participants
Participants included 12 interscholastic athletes (4 females, 8 males) from secondary schools in the Phoenix, Arizona, metropolitan area. Criterion sampling was used to recruit potential participants. The inclusion criteria included (1) sustaining a sport-related concussion during interscholastic activity and (2) being out of participation for ≥10 days. Each participant was given a pseudonym to maintain anonymity (Table 1). This study was approved by the A.T. Still University Institutional Review Board. Adolescents provided verbal and written assent and their parents provided verbal and written consent to record the interview.
Participant Demographics

Instrumentation
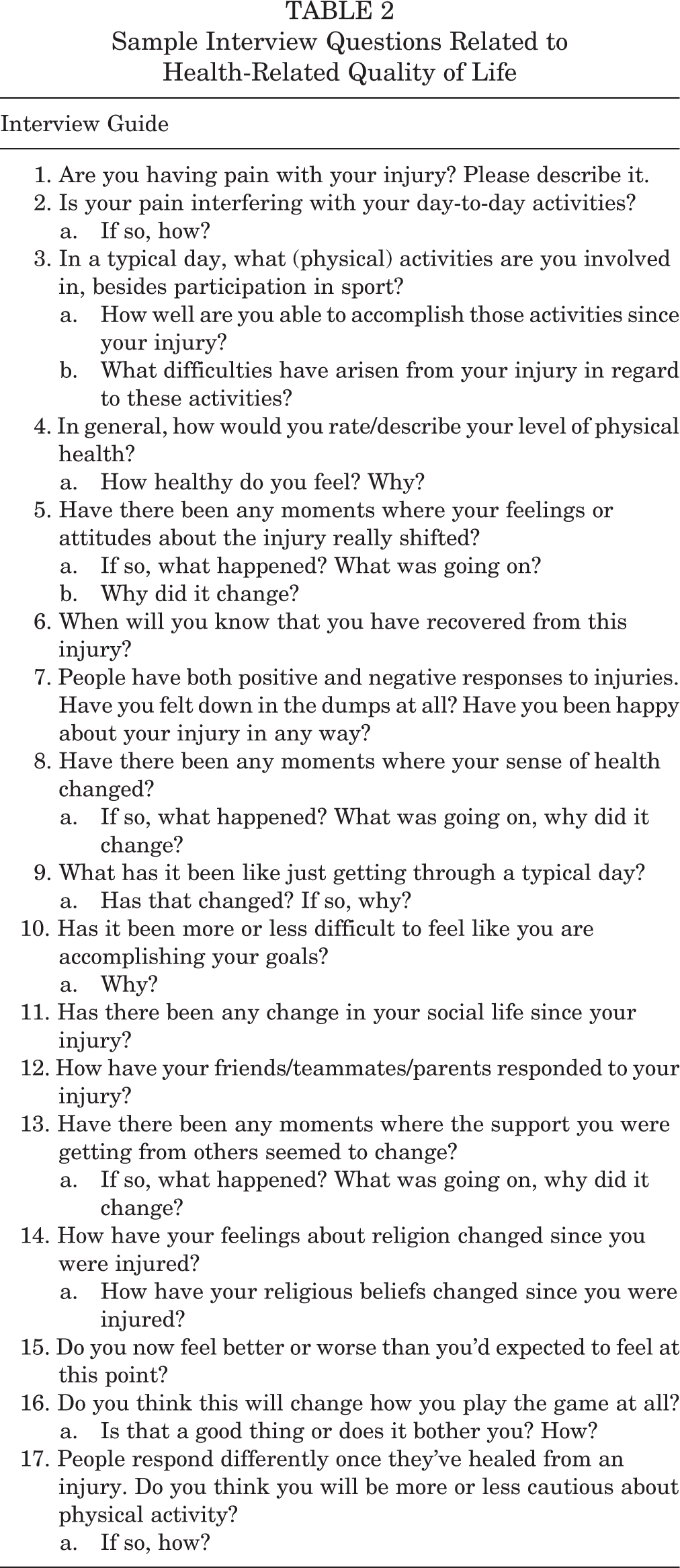
The qualitative interview protocol was developed with HRQOL as the analytical framework, as loosely based on the Short Form–36 patient outcomes tool 53,54 and utilizing the International Classification of Functioning Disability and Health (ICF) model. 33,59 The ICF provides a framework to understand and study health status, outcomes, and determinants, as well as to establish a common language among various groups and offer a holistic view, which aligns with athletic training. 44,50,59 The questions within the interview were developed to discuss the underlying factors of HRQOL—specifically, social health, emotional health, and mental health. The interview consisted of approximately 52 questions, which focused on basic demographics (5 questions), sport demographics (7 questions), current injury (3 questions), physical status/functioning (6 questions), vitality and mental health (5 questions), accomplishment and support seeking (2 questions), social status/role transitioning (3 questions), relationships (8 questions), spirituality (4 questions), expectancies (5 questions), and a series of single-item responses (4 questions). Questions also addressed the components of the ICF model, including body functions, body structures, impairments, activity, participation, activity limitations, participation restrictions, and environmental factors. 33,59 The interview protocol was pilot tested with healthy adolescents to ensure clarity and understanding of questions and to gauge the time needed for interviews. Minor modifications to the interview protocol were made after the pilot interviews. Table 2 presents a sample of interview questions included in the final interview protocol.
Sample Interview Questions Related to Health-Related Quality of Life
Procedures
Participants were recruited from 15 high schools in Arizona. If athletes remained out of activity by day 10 postinjury, the research team was notified by the school’s athletic trainer. The parent and student-athlete were contacted by the research team to participate in the qualitative study, at which time parental consent and athlete assent were obtained. Two researchers who had experience in qualitative interviews were involved in conducting the interviews with the participants. Narrative interviews were conducted to assess the meaning given to sport-related concussion and how participants perceived that it affected their health status. Interviews focused on injury occurrence as well as the physical, psychosocial, and emotional aspects of health in relation to the injury. The interview was conducted at a location of comfort to the participant and was audio recorded. After the interview, the recording was professionally transcribed. Each interview lasted approximately 45 minutes.
Data Analysis
The data analysis team included 3 researchers previously trained in the consensual qualitative research (CQR) data analysis process. 17,18 The CQR process focuses on using multiple researchers, coming to a consensus, and constantly and repetitively analyzing the cases to reach a conclusive and complete understanding of the findings. 17,18 Furthermore, data triangulation was ensured through the inherent nature of the consensus process and the use of multiple analysts to minimize researcher bias.
Data analysis via the CQR approach involves 4 progressive stages: (1) developing initial code domains, (2) separating key ideas from each domain, (3) cross-analyzing multiple interviews via development of categories and themes, and (4) identifying the frequency of participants per category. 17,18 Once the domains were developed, the 3 members of the research team coded the initial transcripts into the proper domains. When the data were placed into a domain, the next process involved separating the core ideas from each domain. 18 This allowed for the research team to more concisely summarize the statements made by the participants to develop the codebook. Finally, the research team cross-analyzed multiple interviews, which allowed for relationships, similarities, and differences to be examined. Throughout the process, categories were often modified because the researchers became more familiar with the data. After completion of the cross-analysis, the frequency occurrence for all categories was recorded. Specifically, frequency counting allowed the research team to determine the occurrence of each category across the whole sample, thus allowing for the entire sample to be represented. 18 Frequency categories are divided into 4 components: general, typical, variant, or rare. For this study, a category was considered general if it applied to all cases or all cases but 1, typical if it applied to more than half of the cases, variant if it applied to less than half of the cases, and rare if it applied to only 2 or 3 cases. 18
Results
Four main themes emerged during the data analysis: perceptions of social aspects of sport, social perspectives of a sport-related concussion, psychosocial experiences following a sport-related concussion, and single-item HRQOL responses. However, for the purpose of this study, we focused solely on the psychosocial experiences following a sport-related concussion and its corresponding categories.
Psychosocial Experiences Following a Sport-Related Concussion
Five categories emerged during the data analysis regarding the perceptions of the adolescent athletes’ lived experiences following a sport-related concussion: effect of symptoms, impact on emotions, effect on school role, effect on societal/social role, and minimizing/masking symptoms. Table 3 displays the frequency of participant cases per category.
Participant Cases by Category

Effect of Symptoms
The symptoms and other effects associated with sport-related concussion significantly affected the athletes’ perceived lived experiences. All participants reported having multiple concussion-related symptoms that occurred frequently over the course of their recovery; such symptoms included headaches, dizziness, sensitivity to light/noise, fatigue, trouble with sleeping, difficulty remembering, and difficulty concentrating. These symptoms resulted in pain, fatigue, feeling slowed down, and feeling not right, which inhibited the athletes’ ability to engage in their physical roles, whether activities of daily living, physical education class, sports, school, or social activities. Table 4 provides representative quotes from participants regarding the effect of the concussion on their physical role.
Representative Quotes Related to the Effect of Symptoms

Impact on Emotions
As with the impact of symptoms, participants expressed an increase in the effect of the concussion on their emotions (Table 5). Participants reported increased emotional issues, irritability, sadness, depression, and anxiousness following the sport-related concussion, and this affected their school and social roles.
Representative Quotes Related to the Emotional Effects

Effect on School Role
With regard to the effect on the participants’ school role, there was concern with the difficulties that students encountered in mental activities and participation in school. For example, many noted having difficulty concentrating, getting headaches throughout the day, experiencing increased fatigue during school, and having their grades drop owing to missing classes or not being able to complete assignments accordingly. Furthermore, there were inconsistencies noted among participants with regard to the ability of school personnel to appropriately assist them in school activities and return to the classroom. While some participants noted difficulties with the school implementation of academic adjustments (eg, academic assistance), other participants indicated that their teachers and administrators were very helpful in assisting them in the process. In rare cases, the participants had a lack of understanding for the school adjustments that were available to them before their grades started to drop, or they did not have enough issues with their grades dropping to be concerned, although they did suffer from sport-related concussion symptoms throughout their school day. Table 6 displays representative quotes from participants regarding school role.
Representative Quotes Related to School Role

Effect on Societal/Social Role
In general, participants demonstrated concern for letting their team or family down and not being able to fulfill different societal/social roles, such as an athlete, son, daughter, friend, or sibling. Table 7 provides representative quotes regarding social role. Many participants discussed the stress of being away from their team and the daily interactions with teammates. In some cases, concern was raised regarding other social activities with friends and teammates and the lack of understanding among peers regarding the seriousness of the concussion and the importance of rest to aid recovery.
Representative Quotes Related to the Effect on Social Role

Specifically, participants differed regarding the impact of their injury on their spiritual or religious life. While most participants noted the lack of importance that religion played in their lives, in rare cases some participants noted no change in their beliefs following the concussion, or they felt that there was a reason why they had sustained the concussion and were looking for something good to come out of their experiences.
Minimizing/Masking Symptoms
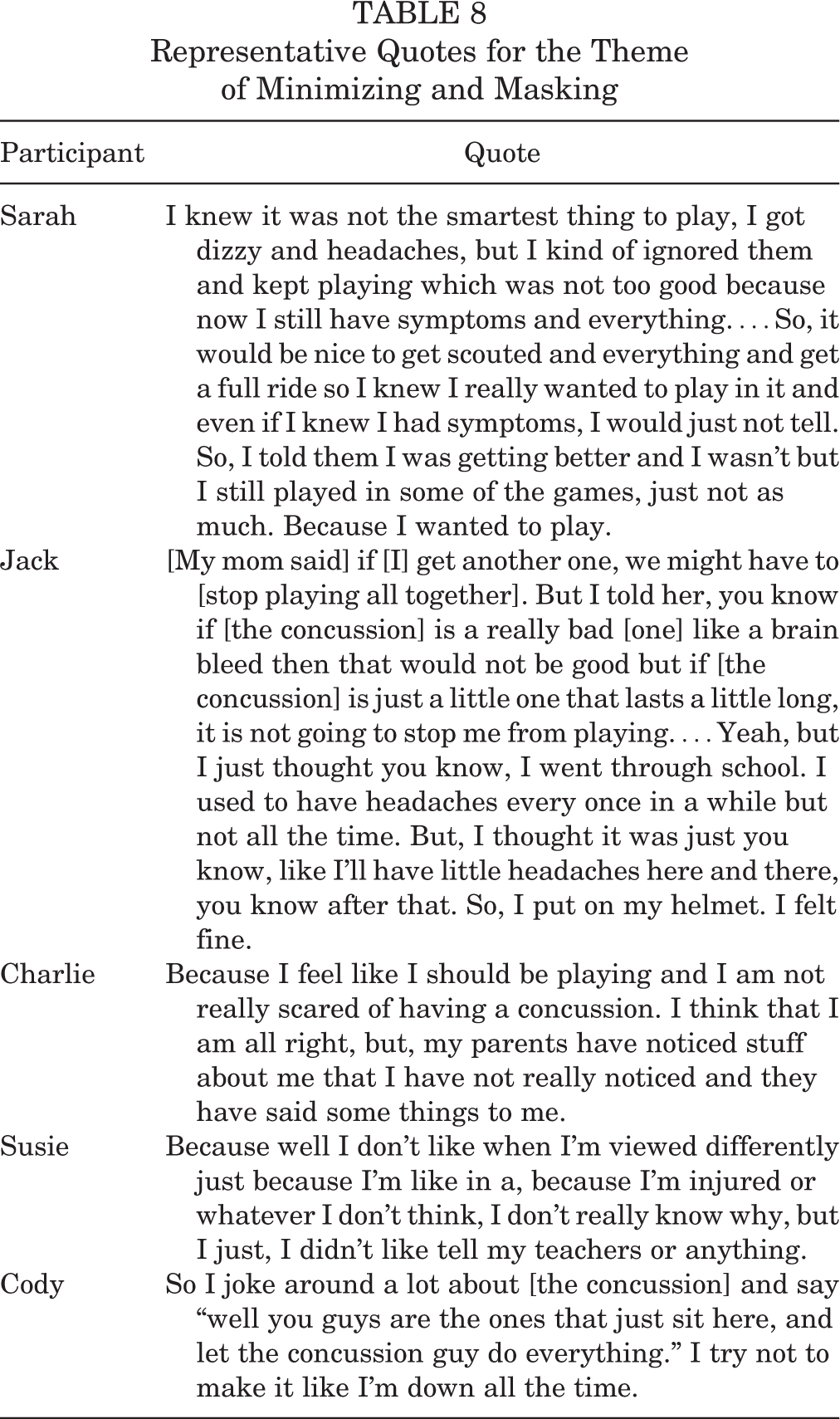
As a result of the negative effect of the concussion on numerous psychosocial and emotional experiences, participants noted that they often tried to minimize or mask the symptoms that they were experiencing, either to keep playing or to reduce the perceptions of their peers regarding their sport-related concussion. They expressed that they were afraid of being made fun of or that they did not want to be viewed differently than their teammates because of their sport-related concussion. While many understood the importance of rest and recovery, the underlying tension regarding not being an active team member led some participants to not report symptoms, as a means to stay involved and feel normal. While this strategy worked for some participants, others noted that symptoms worsened or their recovery time was delayed because of minimizing and masking symptoms and not following management recommendations. Table 8 provides representative quotes.
Representative Quotes for the Theme of Minimizing and Masking
Discussion
Our main findings indicated that adolescents felt that their sport-related concussion affected numerous aspects of their life, including emotional, school, and social aspects. Specifically, the participants expressed that their sport-related concussion and resulting symptoms caused them to miss out on everyday activities, such as experiencing school, playing sports, or having a social life. Participants were discouraged because of the inability to participate in their sport and maintain their academics as a result of the symptoms associated with their injury. Furthermore, participants perceived that they were being treated differently, and as a result, they tried to minimize their signs and symptoms so that they could be viewed as normal.
Our findings are supported by other studies that identified a negative impact on aspects of HRQOL following sport-related concussion 19,22,47,51,52 or mild traumatic brain injury 9,32,35 among children and adolescents. All but 1 of these investigations used patient-reported outcomes in evaluating HRQOL, which allows for standardization administration and measurement but does not necessarily take into account the relevance of the questions or additional meaning behind the lived experiences of the adolescents. 8 While there are limited qualitative studies of HRQOL following concussion to which we can compare our results, a study by Iadevaia et al 22 interviewed adolescent athletes approximately 1 year following concussion and reported themes that were similar to the current work. These authors interviewed 7 high school athletes and their parents approximately 1 year following the concussion and reported 4 major themes: significant effect of concussion symptoms, feelings of frustration, influence on school, and nature of interpersonal and team relationships that negatively affected HRQOL. These findings are important in our understanding of concussion but are limited by the 1-year recall. In our study, interviews were conducted within the first month following concussion, allowing for an acute perspective in close proximity to the injury.
Effect of Symptoms
All participants in our study discussed a significant impact on their physical functioning (limitations in physical activities attributed to the concussion) as well as their physical role (limitations in activities attributable to the concussion) and identified concussion-related symptoms as the primary consequence that affected other aspects of their everyday living while preventing them from participating in their sport. Our findings are similar to those reported by Iadevaia et al, 22 in which physical symptoms were found to be the greatest challenge postconcussion and influenced emotional, social, and school abilities. The most commonly cited symptoms within our study included headaches, dizziness, nausea and vomiting, and sensitivity to light and noise, which were similar to previously published studies 22,28 and were a primary reason why participants were unable to participate in their sport. While the literature reports that concussion symptoms tend to subside by 7 to 10 days postinjury for adults, 31 many of our participants noted prolonged symptoms and physical changes that included fatigue, dizziness, nausea, and headaches, which they discussed as having the greatest impact on their ability to participate in sport or everyday activities. The presence of these symptoms is important, as current recommendations suggest refraining from physical activity while symptomatic 3,31 ; however, this notion is being questioned, with some evidence supporting the implementation of active rehabilitation and subthreshold exercise to aid recovery, 12,26,42 which may also improve the patient’s psychological and emotional well-being. Clinicians may want to consider allowing subsymptom, supervised activity to allow patients to engage in some activity as they recover from their concussion.
Impact on Emotions
All our participants discussed multiple factors, including physical and emotional symptoms, which ultimately affected their emotional role or resulted in limitations in activities. Participants commonly reported that their concussion resulted in frustration, depression, anxiety, or irritability. While it is possible that these symptoms were preexisting, they can also occur as a result of the sport-related concussion, especially when the individual is held out of play. 20,21 Specifically, participants noted feelings of isolation, as well as frustration with slow progress in recovery and not being able to participate in sport or activity, which is consistent with the qualitative study by Iadevaia et al. 22 Owing to the individualized nature of recovery, lack of specific time frames for returning to activities, and recommendations for physical and cognitive rest, patients can feel isolated and alone, which may in turn result in psychosocial and emotional issues that should be addressed as part of the concussion management plan. 34 Prior studies also identified emotional issues following concussion, with frustration stemming from the longevity of symptoms, relationship changes, and time missed from school and sport, 20 –22,40 consistent with the findings of our study. The causes of emotional issues following concussion have been speculated to be linked to a combination of factors, including depression, mood disturbances, stress and anxiety, not being understood by peers, and other psychological factors. 37
Effect on School Role
Sport-related concussion symptoms often made it difficult for the participants in this study to function normally within the classroom setting. Participants found that engaging in cognitive activity, such as participating in class or reading, increased their physical symptoms, which made it difficult to concentrate. Difficulties in school exacerbated participants’ emotional symptoms (ie, anxiety) or current symptoms to be more severe and prolonged. To facilitate recovery, current recommendations suggest a brief period of cognitive rest following concussion, 14 and evidence supports an initial short period of rest to improve outcomes. 48 However, an indirect consequence of cognitive rest and/or academic adjustments is a perceived sense of falling behind in class, which may perpetuate a cycle of anxiety and other psychosocial symptoms. Therefore, the nature and duration of cognitive rest or the use of academic adjustments should be individualized, taking into account the delicate balance between aiding recovery and further isolating the patient.
As a result of missing school because of concussion symptoms or medical appointments, more than half of the participants self-reported that their grades significantly decreased following concussion. Many of our study participants indicated that they struggled to complete class assignments and had trouble keeping up with homework and concentrating during tests, resulting in frustration about their academic performance and role as a student. While we did not document formal academic outcomes but rather identified the adolescents’ perceptions of their academic performance, the literature on academic dysfunction is relatively new and mixed. One study identified academic dysfunction following sport-related concussion, 55 whereas a population-based study did not find any reduction in grade point average among high school student-athletes in the year following a concussion. 39
Interestingly, all our participants were eventually able to get support from teachers to allow them to have more time on assignments and tests, but 6 participants stated that some teachers were not as supportive (ie, the participant was “faking it” to get out of the assignment). However, this may have been due to a lack of communication or understanding among the student-athlete and/or members of the concussion management team. 57 Regardless, it highlights one area where improved communication and postinjury education may be required to ensure that the patient, family, and medical and school personnel are on the same page.
Effect on Societal/Social Role
It has been speculated that social interactions and interpersonal relationships with family and friends are a key component to the perception of one’s HRQOL, especially among adolescents. 16 Owing to the impact of physical and emotional symptoms, 11 of the 12 participants reported that they participated in fewer social activities because they were suffering from their symptoms. They were not able to participate in their normal activities, such as hanging out with friends or family, because they would get recurring symptoms, such as fatigue, headaches, sadness, anger, or irritability. Participants’ interpersonal relationships were altered by frustration, anger, and irritability toward their immediate family, which is consistent with the adolescent athletes studied by Iadevaia et al. 22 We also found that in some cases, the relationships with friends and teammates were supportive and understanding, whereas 6 participants reported that some of their friends or teammates described them as “fakers.” All the participants revealed a feeling of betrayal toward their team because they could not be at practice or play in games. This could be caused by self-imposed pressure or pressure from coaches, family members, or friends, thus causing them to feel as though they are letting their team down or that they are no longer a part of the team, as noted by Iadevaia et al. 22
The study participants also described lower self-esteem levels because they were not able to fulfill their roles as a student, friend, teammate, and son/daughter. Three studies 1,22,43 found that patients with traumatic brain injury presented significantly lower self-esteem and adaptive behaviors and reported increased levels of loneliness, maladaptive behavior, and aggression. 22,43 It is crucial to the well-being of the student-athlete that all psychological and behavioral concerns be addressed as part of the concussion management plan 34 and that health care providers follow up with the adolescent daily to monitor psychological, behavioral, and academic deficits and provide guidance during recovery. This may be in the form of anticipatory guidance, in which instructions are provided to the patient and parent that describe symptoms to be concerned about and when it is necessary to seek re-evaluation. 25,41 While 1 study identified that 82% of patients received emergency department discharge instructions following concussion that included anticipatory guidance, 41 this may not often be the case. Clinicians should investigate means of including anticipatory guidance in their patient consultations and should consider using educational technology, 1 mode of which has preliminarily been shown to have positive outcomes following mild traumatic brain injury as evaluated in the emergency department. 25
Minimizing/Masking Symptoms
Perhaps our most important finding regarding the lived experiences of adolescents following concussion is their perceived need to minimize and mask symptoms to bring a sense of normalcy to their lives. There is a consensus among sports medicine professionals that sport-related concussions are difficult to diagnose and manage because of underreporting or athletes minimizing/masking their symptoms to avoid detection of the concussion or hasten return to play. 30,38 More than half the participants in our study expressed that they tried to minimize or mask their postinjury symptoms from coaches, parents, teammates, friends, and athletic trainers because they did not want to feel different than their peers, be made fun of or thought of as a faker, or be withheld from participating in their sport, school, or social activities. These findings are similar to those of Iadevaia et al, 22 who reported that the desire to maintain a normal life, including at school, caused adolescents to participate in cognitive and physical activities before their symptoms had fully subsided. In addition, several studies of concussion reporting intention identified similar findings with adolescents understanding the dangers of concussion but not reporting concussion-like symptoms. 6,24,38 Specifically, adolescents identified several barriers to reporting concussion symptoms, including difficulty with telling when one is injured, thinking that athletes are supposed to play injured, having fear of letting teammates down, and being removed from play for reporting symptoms. 6 Similarly, not thinking that the symptoms were serious, not wanting to be removed from the game, and not wanting to let down teammates or coaches were identified in another study investigating knowledge and reporting of concussion among adolescents. 38 Collectively, these findings suggest an important avenue for continuing education regarding the importance of reporting concussion symptoms to adults.
An additional challenge related to the desire to minimize and mask symptoms is that sport-related concussions do not have any outward signs or symptoms and rely on the patient to provide a truthful report of her or his current symptoms. In some instances, participants felt that peers did not think they were really hurt because their peers could not actually see the injury. Seven of the 12 participants expressed that their teachers and friends were often the ones who thought that they were faking to get out of different tasks, such as school assignments or sport practice. As a result of being called a faker or being made fun of, the participants described how they minimized and masked their symptoms in an attempt to bring a sense of normalcy to their lives.
Furthermore, this desire to minimize and mask symptoms may stem from wanting to avoid management practices that often recommend restriction of physical and cognitive activities until acute symptoms resolve, at which time a graded return to activity progression begins. 3,15,31 However, there is some speculation, supported by the current study and others, that complete or strict rest can actually increase symptom burden, 10,46 which has led to calls for restructuring the concept of “rest” and allowing supervised symptom-limited cognitive and physical activity as a means of treating concussion. 7,13 One rationale provided for these changes in the management approach is that the use of complete rest may be seen as further punishment by removing participants from their sports, social interactions, team environments, and digital lives, resulting in increased stress and anxiety and lower self-esteem. 10,13 The concussion management team needs to be sensitive to these issues and prescribe a balance between rest and activity that is communicated to the patient, parents, and other support personnel.
Limitations
Our study is not without limitations. From 15 schools within a single geographic area, we recruited participants who had been held out of sports participation for at least 10 days, sampling from those with a more prolonged recovery. These findings may not generalize to individuals who have a relatively quick or uncomplicated recovery from their concussion. Furthermore, we did not have access to the participants’ medical histories to determine whether preexisting underlying issues related to emotional or psychosocial health were present. However, participants described their experiences following concussion in relation to their perceived preconcussion health status.
Conclusion
Our study identified the perceived effect of sport-related concussion on psychosocial and emotional health status among adolescents. As expected, participants noted a significant effect of concussion-related symptoms on their physical health status. However, these symptoms also influence their emotional, school, and social health status. In an attempt to overcome these factors, adolescents often minimized and masked their symptoms, which could negatively influence their recovery by leading to premature return or unrecognized prolonged symptoms.
These findings suggest that concussion management needs to move beyond the monitoring of impairments (eg, cognitive function) and address the whole person to adequately evaluate all domains of health status and to develop concussion management strategies that are sensitive to emotional, social, and psychological stressors. Health care providers and school personnel managing concussion need to understand the possible impact of the injury on areas outside of sports participation and institute policies to aid the individual through recovery. Anticipatory guidance on the effect of concussion and expectations throughout recovery may improve compliance in reporting concussion symptoms, following recommendations for activity restriction, and progressively returning to the classroom and playing fields. Clinicians should also address areas of psychosocial health during evaluations to better understand the effect of the concussion on each patient and provide appropriate management strategies that address all areas of importance to the patient. Future studies of rest and treatment for concussion should also include patient-report outcomes related to these important areas of HRQOL.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was funded by the National Operating Committee on Standards for Athletic Equipment.
Ethical approval for this study was obtained from the A.T. Still University Institutional Review Board Committee (tracking No. 2009-20).
Acknowledgment
The authors thank John Parsons, PhD, ATC, for his contributions to the participant interviews.