
Abstract
Background:
Athletic pubalgia is typically associated with male athletes participating in contact sports and less frequently with females. Endoscopic surgery may fully treat the patient with athletic pubalgia.
Purpose:
To perform an outcomes analysis of magnetic resonance imaging (MRI) and endoscopic surgery in female patients with athletic pubalgia.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Fifteen physically active female patients (mean age, 37 years) with athletic pubalgia were treated surgically via placement of total extraperitoneal endoscopic polypropylene mesh behind the injured groin area. The presence of preoperative bone marrow edema (BME) at the pubic symphysis seen on MRI was graded from 0 to 3 and correlated with pain scores after surgery. The outcome measures were pre- and postoperative pain scores and recovery to daily activity between 1 and 12 months after surgery. Results were compared with previously published scores from male athletes (n = 30).
Results:
With the exception of lower body mass index, the females with (n = 8) and without (n = 7) pubic BME had similar patient characteristics to the corresponding males. Mean inguinal pain scores (0-10) before surgical treatment were greater in females than males (during exercise, 7.8 ± 1.1 vs 6.9 ± 1.1; P = .0131). One month after surgery, mean pain scores for females were still greater compared with males (2.9 ± 1.7 vs 1.3 ± 1.6; P = .0034). Compared with female athletes with normal MRI, pubic BME was related to increased mean preoperative pain scores (8.13 ± 0.99 vs 6.43 ± 1.2; P = .0122). After 1 year, surgical outcomes were excellent or good in 47% of women.
Conclusion:
Endoscopic surgery was helpful in half of the females with athletic pubalgia in this study. The presence of pubic BME may predict slightly prolonged recovery from surgery.
Chronic inguinal pain is defined as the presence of pain in the groin region for more than 6 months. The causes of groin or pelvic pain in females include disorders of musculoskeletal, gynecologic, urologic, or gastroenterologic organs. 2,6 Sport-related groin pain, that is, athletic pubalgia, is also reported in females, with a prevalence ranging between 5% and 20%. 1,2,12,15,18,24 Other common reasons for groin pain in young, physically active females may be endometriosis, ovarian-related pain, or inguinal hernias. 1,21,22
Common musculotendinous causes for athletic pubalgia include tendinopathies from the adductor or rectus abdominus muscles, osteitis pubis associated with bone marrow edema (BME), or disruption of the posterior wall of the inguinal canal. 7,10,14,25 Sometimes a multidisciplinary investigation may reveal more than one of these reasons for athletic pubalgia. 15,23 First-line management includes rest, muscle strengthening and stretching exercises, physical therapy, anti-inflammatory analgesics, local anesthetic, or corticosteroid injections, and in resistant cases, operative management. 14,15 Surgical approaches for athletic pubalgia include open repair or laparoscopic or totally extraperitoneal techniques, with or without polypropylene mesh. 14,17 One randomized trial confirmed the efficacy of video-assisted, preperitoneal insertion of polypropylene mesh in the treatment of athletic pubalgia. 15 In male athletes with pubalgia, the presence of pubic BME had no remarkable effect on recovery from endoscopic treatment. 7
In female athletes with pubalgia, the clinical significance of BME assessed using magnetic resonance imaging (MRI) has been poorly investigated. 4,11 In the present study, our aim was to investigate the predictive role of BME in operative outcomes of female patients with athletic pubalgia. Contrary to male cases, our hypothesis was that female patients with athletic pubalgia associated with BME may have delayed recovery from surgery.
Methods
Female patients (N=15) who were included in a prospective trial of athletes with pubalgia were enrolled in this study. All female athletes with specific organ-related pain (such as irritable bowel, endometriosis, hip-related, bursitis, inguinal or femoral hernia, lower abdominal muscle tear) were excluded. Diagnosis was based on consensus by an orthopaedic and general surgeon, gynecologist, sport clinician, physical therapist, and radiologist. Most female patients were nonprofessional athletes or physically active adults who participated regularly in only moderate-level sport (Table 1). The etiology and exact diagnosis of athletic pubalgia pain was based on patient history, physical examination, radiography, and MRI. The location of pain had to be in the lower abdomen near the inguinal ligament with or without tenderness over the pubic symphysis. Pain scores (range, 0-10) on a numeric rating scale (NRS) during rest and exercise (running, long-distance walking) were carefully recorded preoperatively and 1, 3, 6, and 12 months after surgery. The male controls (N = 30) had similar symptoms of athletic pubalgia as the females, and their results were published earlier. 7,15 All females were treated nonoperatively from 3 to 6 months before surgery. This included usually oral anti-inflammatory analgesics, a few injections of local corticosteroids (5 patients), and physical therapy.
Characteristics of Female and Male Patients With Pubalgia a

a Statistical evaluation was performed with the Fisher exact test and with Student t test.
The female patients were carefully evaluated by a gynecologist and a general surgeon to rule out any intrapelvic, gynecological, or intra-abdominal disease. Careful clinical examination was always performed, and ultrasound imaging and endoscopic studies (usually sigmoidoscopy) were performed if necessary. Pelvic radiographs and MRI were obtained in all patients to rule out musculoskeletal abnormalities. Pelvic MRI (Siemens Harmony 1.0 T or GE 1.5 T) was performed using routine T1-weighted, T2-weighted, and STIR (short tau inversion recovery) sequences. 4,11,13,22 The imaging parameters TR (repetition time) and TE (echo time) were usually 590 and 20 ms for T1-weighted imaging, and 4000 and 40 ms for STIR imaging, respectively. The imaging planes were coronal and axial, and slice thickness was 5 mm. All abnormal changes in MRI, including BME and an increased signal from the insertion of the adductor muscles, were recorded. 4,13 Pubic BME was graded as 0 (no edema), I (mild), II (moderate), or III (heavy) (Figure 1). The regional extent of BME at the pubic symphysis was also estimated visually and by an image-processing tool 11,16 and was graded as 0 (no increased signal), I (<2 cm area at the pubic symphysis), II (>2 cm area), and III (both rami of the pubic symphysis). All the MRI scans were reviewed independently by 2 investigators (1 radiologist, 1 surgeon). A consensus was reached if there was a difference in the MRI scan reports. Both axial and coronal images were evaluated to detect BME. The ethics committee of our hospital approved the study protocol.

Magnetic resonance images of pubic bone marrow edema (grade I = mild, grade II = moderate, and grade III = heavy).
Operative treatment was performed by an endoscopic, total extraperitoneal mesh placement behind the injured pubic bone and posterior wall of the inguinal canal. The same general surgeon performed all operations. After dissection, the insertion area was covered with a 10 × 15–cm light polypropylene mesh (Optilene, B. Braun), which was usually fixed with 2 to 3 bioabsorbable staples (Protack stapler, Tyco Healthcare). The mesh was placed bilaterally even if the symptoms were unilateral, because scarring of the preperitoneal space would most likely make it more difficult to operate later on the nonaffected side. Conventional nonsteroidal anti-inflammatory drugs or paracetamol were used for postoperative pain relief. All patients were evaluated after 1, 3, 6, and 12 months. Recovery and return to daily activities were recorded by evaluating operative complications, pre- and postoperative pain scores (NRS, 0-10) during rest and training, use of analgesics, and time to resumption of training (usually from 1 to 3 months after surgery). Subjective outcome of the patients (not validated) was asked after surgery and was reported as excellent, good, moderate, or poor.
The statistical analysis was carried out by using SPSS for Windows, Release 20.0 (IBM SPSS). Statistical evaluation was performed with the Fisher exact test between the males and females. The comparison between mean pain scores (NRS) and other continuous variables (patient characteristics) were analyzed with the Student t test. P < .05 was regarded as significant for both tests.
Results
All 15 females had obscure groin (athletic pubalgia) lasting over 6 months. The pain area was either near the pubic insertion of the inguinal ligament, nonspecifically in the lower abdominal wall, or tenderness of the pubic symphysis. Patient characteristics and possible etiology of athletic pubalgia are described in Table 1. All but 4 females had sport-related pubalgia. Two females had chronic pain possibly related to childbirth, and 2 had idiopathic etiology of athletic pubalgia (Table 1). Contact sport was not a frequently observed etiological reason for pain in females. Four of the female patients had gymnastics-related groin pain (Table 1).
The mean preoperative pain scores, both at rest and during exercise, were higher in women than in men (Table 2). Pelvic MRI was normal in half of the patients in both study groups. These patients had no BME, no adductor-related edema, and no other hip, pelvic bone, or musculotendinous MRI findings. The presence of BME was demonstrated as the increased signal intensity on STIR sequences (Figure 1). Female patients with BME at the pubis symphysis had more pain than the patients without BME (numeric rating scale [NRS] scores 8.13 ± 0.99 vs 6.43 ± 1.2; P = .0122). In males, the corresponding NRS scores were similar in the BME group versus normal MRI (7.0 ± 0.74 vs 6.6 ± 1.2; P = .2970). In both study groups, the pain scores were much higher during exercise than at rest (Table 2). The female patients with BME had bilateral pain more frequently (50%) than the patients without BME (14%). The BME grade on MRI was categorized as follows: 2 females had grade I, 3 had grade II, and 3 patients had grade III edema (Table 2).
Clinical Preoperative Data of the Patients With Pubalgia a
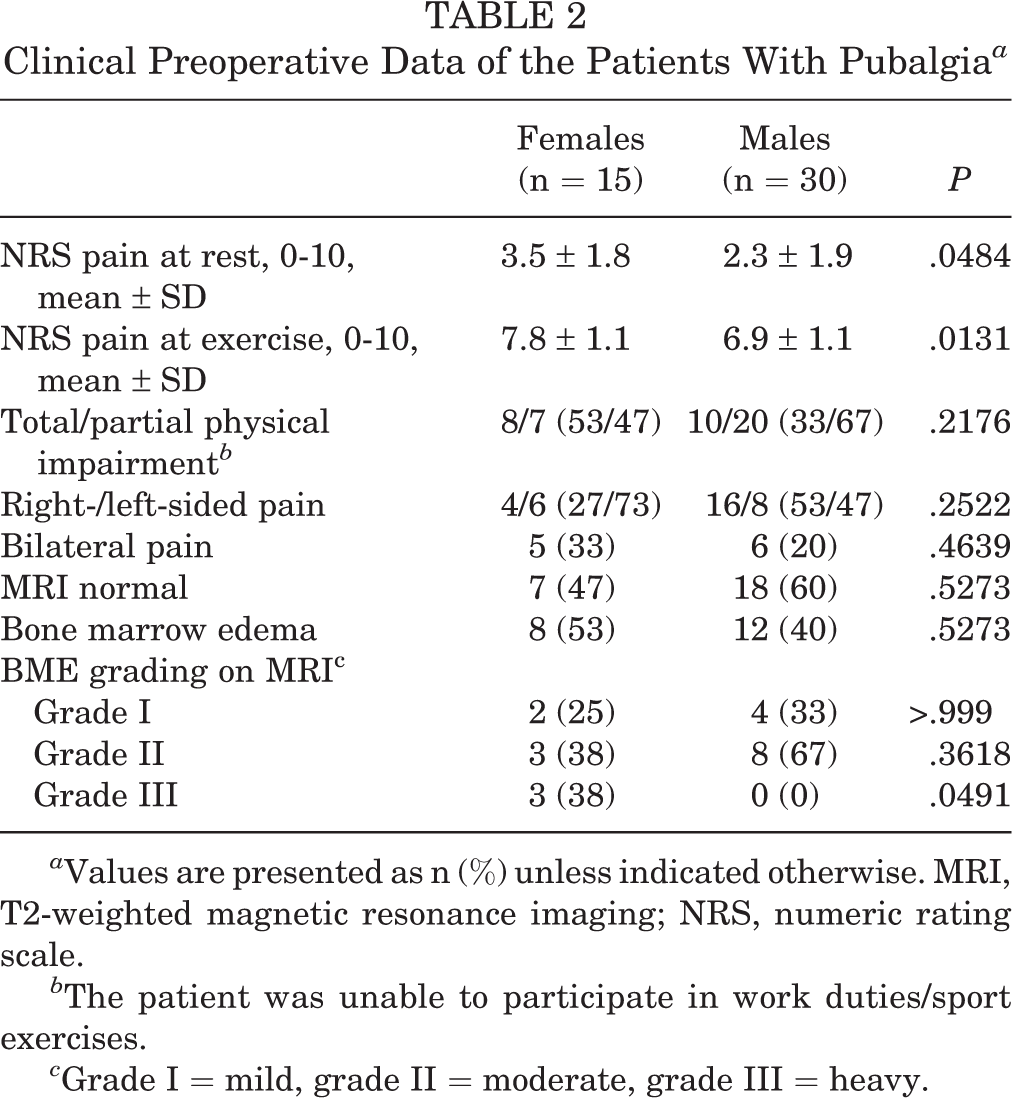
a Values are presented as n (%) unless indicated otherwise. MRI, T2-weighted magnetic resonance imaging; NRS, numeric rating scale.
b The patient was unable to participate in work duties/sport exercises.
c Grade I = mild, grade II = moderate, grade III = heavy.
The mean pain scores during exercise at 1 and 6 months after surgery were higher in females than in males (Figure 2, Table 3). Women with pelvic pain were not as satisfied after endoscopic surgery than males. The number of female patients with moderate/poor outcome was 8 versus 4 in males (P = .001) (Table 3). Time to return to full sport or daily physical activities was 1 to 2 months longer in the BME group than in the non-BME group in both females and males. The mean time to return to sport was 5.6 ± 1.2 months in females and 3.5 ± 1.1 months in males with BME. The corresponding values in non-BME athletes were 3.6 ± 1.2 and 2.0 ± 1.1 months for females and males, respectively.

Mean pre- and postoperative pain scores at exercise after endoscopic surgery in chronic pelvic pain. The pain scores were higher in females than in males preoperatively and after 1 and 6 months of surgery (P < .05).
One-Year Outcome Analysis of Endoscopic Operation (Extraperitoneal Polypropylene Mesh) a

a NRS, numeric rating scale.
Discussion
The main finding of our study was that pubic BME was contributing to females’ athletic pubalgia, but the causal relationship is not clear. This is contrary to males, where the presence of pubic BME had no remarkable long-term effect on recovery from endoscopic surgical treatment of athletic pubalgia. 7 Reactive changes (edema) in the symphysis pubis may be a consequence of overuse injury, contact sport injury, delivery, or it may sometimes be idiopathic in females. The second main finding was that athletic pubalgia in females was more painful both before and after surgical treatment compared with males. The mean pain scores during exercise at 1 and 6 months after surgery were higher in females than in males. On the basis of patients’ subjective outcome, endoscopic surgery was helpful in about half of female athletic pubalgia compared with 90% of males. Percentage of excellent or good outcome was significantly lower in women (47%) than in men (87%) (P = .01).
Athletic pubalgia was associated with BME in MRI in half of the patients in the present study. Subchondral BME in a pattern reminiscent of osteoathritis is the hallmark MRI finding of osteitis pubis 13,16 and it represents a painful, noninfectious inflammation of the pubic symphysis. 3,9 Initially associated with urologic procedures, osteitis pubis has been described as a complication of various obstetrical and gynecological procedures, including vaginal deliveries. 26 Although the pathogenesis of BME is not clear, periosteal repetitive trauma (overuse injury) seems to be an important initiating event in the female athletes. 5 Also, with more women participating in sporting activities, more patients may present to the physician with BME and osteitis pubis. Radiographic findings of long-standing osteitis pubis include reactive sclerosis. The major differential diagnosis is bacterial osteomyelitis. Pubic edema is not always associated with clinical symptoms and pain, as recent studies indicate asymptomatic soccer or hockey players have BME. 4,11,16 An abnormality of the conjoint tendon, tendinopathy of the inguinal ligaments and, in some patients, incipient osteitis pubis (BME) may be a manifestation of the same disease entity, that is, repetitive strain injury or acute disruption of the musculotendinous complex attached to the pubic tubercle (athletic pubalgia).
Athletic pubalgia offers a diagnostic challenge for the sports medicine clinician and surgeon. A recent Doha consensus suggests diagnostic categorization based on 4 clinical entities: adductor, pubic/inguinal, ilipsoas, or hip pathology. 27 Athletic pubalgia is not a common presentation in female athletes in sports medicine. 19 Routine examination in females includes history, clinical status, lower abdominal ultrasound, and, more frequently, pelvic MRI to rule out endometriosis or musculoskeletal dysfunction. 13,19,22 In the present study, all patients were examined carefully prior to operation to rule out any other reason for groin pain. Female chronic inguinal/pelvic pain has multifactorial etiology, and roughly only one-fifth of women may have pain associated with musculoskeletal causes. 6 In a study including 239 women with chronic hip/groin pain, the origin was the hip joint in 109 (77%), iliopsoas in 24 (17%), BME in 5 (4%), and adductor-related pain in 4 (3%) cases. 19
The results of this study demonstrated that endoscopic treatment was effective for athletic pubalgia in females. This treatment is analogous to inguinal hernia surgery in females, where endoscopic treatment utilizing mesh is now widely suggested. 8 There is no evidence-based consensus available for operative treatment of athletic pubalgia in females. 10,14,25 Without a clear clinical and pathological diagnosis, subsequent management is difficult. Open and laparoscopic repairs produce good results; the latter may allow earlier return to full sport, 17 but comparative studies between open and laparoscopic procedures in athletic pubalgia do not exist. Video-assisted repair of chronic pubalgia (total extraperitoneal), particularly in athletes, has many theoretic advantages. The posterior position of mesh behind the conjoint tendon and pubic bone theoretically creates a stronger support than conventional anterior hernioplasty. Furthermore, the preperitoneal technique is less invasive than open anterior techniques. 8,17 Postoperative pain and wound complications are less frequent after laparoscopic surgery than in open surgery. The combination of complex anatomy in the groin area, variability of presentation, and the nonspecific nature of the signs and symptoms make the diagnostic process somewhat problematic. 5 It has recently been stressed that in some patients with athletic pubalgia, both hip and pubic regions are chronically injuried. 20
A limitation of our study is the small number of patients. This study was based on single-center operative cases of female groin pain. We collected the data prospectively, including also MRI. Another limitation was that we had no data of nonoperatively treated female patients with groin pain.
To conclude, if nonoperative management fails in the treatment of athletic pubalgia, endoscopic surgery is an efficient method to help female patients with athletic pubalgia. Our study indicated that endoscopic surgery is helpful in over half of female patients with athletic pubalgia, compared with 90% of males. Contrary to males, 7 the presence of pubic BME in females may predict slightly prolonged recovery from surgery. The role of MRI is diagnostically useful to exclude other marked pathology of the groin region (eg, endometriosis, tumors, muscle rupture, various bursitis, impingement, or arthrosis of the hip joint). 1,19
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Research Ethics Committee, Hospital District of Northern Savo.