
Abstract
Background:
Controversies remain regarding the surgical treatment of inguinal-, pubic-, and adductor-related chronic groin pain (CGP) in athletes.
Purpose:
To investigate the outcomes of surgery for CGP in athletes based on surgical technique and anatomic area addressed.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The PubMed and Embase databases were searched for articles reporting surgical treatment of inguinal-, pubic-, or adductor-related CGP in athletes. Inclusion criteria were level 1 to 4 evidence, mean patient age >15 years, and results presented as return-to-sport, pain, or functional outcomes. Quality assessment was performed with the CONSORT (Consolidated Standards of Reporting Trials) statement or MINORS (Methodological Index for Non-randomized Studies) criteria. Techniques were grouped as inguinal, adductor origin, pubic symphysis, combined inguinal and adductor, combined pubic symphysis and adductor, or mixed.
Results:
Overall, 47 studies published between 1991 and 2020 were included. There were 2737 patients (94% male) with a mean age at surgery of 27.8 years (range, 12-65 years). The mean duration of symptoms was 13.1 months (range, 0.3-144 months). The most frequent sport involved was soccer (71%), followed by rugby (7%), Australian football (5%), and ice hockey (4%). Of the 47 articles reviewed, 44 were classified as level 4 evidence, 1 study was classified as level 3, and 2 randomized controlled trials were classified as level 1b. The quality of the observational studies improved modestly with time, with a mean MINORS score of 6 for articles published between 1991 and 2000, 6.53 for articles published from 2001 to 2010, and 6.9 for articles published from 2011 to 2020. Return to play at preinjury or higher level was observed in 92% (95% CI, 88%-95%) of the athletes after surgery to the inguinal area, 75% (95% CI, 57%-89%) after surgery to the adductor origin, 84% (95% CI, 47%-100%) after surgery to the pubic symphysis, and 89% (95% CI, 70%-99%) after combined surgery in the inguinal and adductor origin.
Conclusion:
Return to play at preinjury or higher level was more likely after surgery for inguinal-related CGP (92%) versus adductor-related CGP (75%). However, the majority of studies reviewed were methodologically of low quality owing to the lack of comparison groups.
Keywords
Groin injuries are common in athletes from sports involving repetitive and forceful movements of the hip and pelvis. 20,35,50,77,81 Abnormalities in various anatomic structures are associated with chronic groin pain (CGP), without a true inguinal or femoral hernia. Several terms have been used to reflect the etiologic diversity of CGP: pubalgia, 8,77 groin disruption, 61 sportsmen hernia, 41 Gilmore groin, 25 sports hernia, 26 pubic inguinal pain syndrome, 9 and core muscle injury. 56 Because of the confusing and inconsistent diagnoses used to describe athletes with CGP, the Doha consensus classified extra-articular CGP into 4 entities: inguinal-, adductor-, pubic-, and iliopsoas-related groin pain. 80
While nonoperative treatment is effective in managing most acute and subacute groin injuries, surgery may be necessary to treat long-standing symptoms in athletes with inguinal-, pubic-, and adductor-related groin pain after nonoperative treatment has failed. 42,52 The surgery attempts to normalize forces across the pubic symphysis, address the superficial nerve structures in the inguinal area generating pain, and/or mitigate the secondary osseous abnormalities in the pubic bone. 8,30,47,60,84 Previous systematic reviews have assessed the effectiveness of surgical treatment for CGP in athletes. 11,31,33,54,69,76 Those reviews, however, present significant limitations: inclusion of studies with short postoperative follow-up (<6 months), 11,31,33,54,69,76 exclusion of open surgical treatment, 54 failure to include techniques to treat adductor- or pubic-related CGP, 54 lack of categorization for the surgical techniques according to the anatomic area addressed, 11,76 main outcomes not presented as return to preinjury level of activity, 33,76 and failure to include studies published in the past 5 to 10 years. 11,33,54,69,76
Recent advancements have been made in surgical techniques to address inguinal-, pubic-, and adductor-related groin pain, including the extraperitoneal laparoscopic repair and the utilization of modern meshes for reinforcement without anchoring or with fibrin glue. 57,58,63,70,71,78 These advancements have created controversy as to which technique or combination of techniques provides superior outcomes based on a specific clinical condition. Additionally, longer follow-up (>6 months) using return to previous level of activity as a measure may help in differentiating patient outcomes. Therefore, there is a need for an updated review to define surgical outcome for inguinal-, adductor, and pubic-related CGP in athletes. The purpose of this systematic review was to investigate the outcomes of surgery for CGP in athletes based on the surgical technique and anatomic area addressed.
Methods
Literature Search
A thorough search was performed in 2 electronic databases (PubMed and Embase) to identify articles reporting the surgical treatment of CGP in athletes. The search was finalized on August 11, 2020. Additional publications were identified by reviewing reference lists and citing articles via Google Scholar. This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines 48 and was registered in the International Prospective Register of Systematic Reviews (PROSPERO: CRD42020209393). The strategy used to search the PubMed database is shown in Appendix 1.
Study Selection
Two reviewers (M.H. and R.L.M) independently screened the titles and abstracts of all citations identified by the literature search for relevance. Disagreements between the reviewers were solved by consensus. In sequence, the full text of the screened articles was assessed for eligibility by 1 reviewer (M.H.) according to the inclusion and exclusion criteria presented in Table 1. A full text was deemed not found after online search by the authors, a librarian-led search through an interlibrary loan system, and 2 unanswered emails sent to the corresponding author. When articles had the potential to satisfy inclusion criteria but were missing some critical data, we attempted to contact the authors for clarification and retrieval of the missing data. In case of ambiguous or missing data, the final decision to include the article was made by consensus among 3 reviewers (M.H., R.L.M., and S.B.).
Inclusion and Exclusion Criteria

Quality Assessment
The level of evidence for each study was determined according to guidelines from the Centre for Evidence-Based Medicine (https://www.cebm.net/2009/06/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/). Prospective studies without a control group were considered a poor-quality cohort study and were classified as level 4 evidence.
Observational studies were rated by 1 reviewer (M.H.) using criteria from the validated MINORS (Methodological Index for Non-randomized Studies). 72 The maximum possible MINORS score is 16 for noncomparative studies and 24 for comparative studies. Randomized controlled trials comparing open with endoscopic/laparoscopic surgical treatment were rated by 1 reviewer (M.H.) using a 25-point scale based on the CONSORT (Consolidated Standards of Reporting Trials) statement to assess reporting quality. 3,29
Data Extraction
Studies were reviewed, and data were extracted and recorded into spreadsheets. Data were extracted from the Methods and Results sections, including tables and graphics. The year of publication, author, and study design (randomized controlled trial, cohort study, case-control study, and case series) were recorded. The following information regarding surgical indication was extracted: number of patients, number of groins, sex of patients, age, percentage of athletes, predominant sport, duration of symptoms, surgical indication, length of nonoperative treatment before surgery, physical examination, and imaging studies performed.
The surgical access utilized in each study was categorized as open, totally extraperitoneal (TEP), or transabdominal preperitoneal (TAPP), and the following data were collected: technique summary, anatomic structures addressed, percentage of patients with additional procedures, access detail, utilization of suture repair and technique, adductor release, rectus release, mesh utilization, mesh type and anchorage, pubic symphysis resection, neurolysis or neurotomy of the superficial nerves, and the specialty of the surgeon. The anatomic regions addressed at surgery were identified as inguinal, adductor origin, and pubic symphysis. Articles including variation among patients on the anatomic areas surgically addressed were classified as mixed if the results were not presented separately per anatomic area.
Data regarding the outcomes collected from each article included statistical analysis presented, postoperative follow-up, sample lost to follow-up, return-to-play rate, time to return to sport, pre- and postoperative pain score, patient satisfaction, and other scoring. If the loss-to-follow-up information was not presented or could not be determined according to the presented data, it was rated not reported. Pain scales ranging from 0 to 100 were proportionally translated to a 0-to-10 scale to facilitate analysis and comparison. In articles presenting pain scale at rest and activity, the mean was calculated. Pain, functional, and quality-of-life scores not measured preoperatively or at least 6 months postoperatively were not considered in the results analysis. The rates of the following complications were searched in each paper: reoperation, retear or recurrence of symptoms, nerve entrapment, infection, hematoma, sexual dysfunction, and urinary dysfunction. The complication was rated as not reported if the authors were not specific about the occurrence or did not report one.
Statistical Analysis
All data were collected and analyzed using Microsoft Excel. The statistical analysis was performed using MedCalc (version 19.2.1; MedCalc Software). The mean age, duration of symptoms, and follow-up were calculated for the entire sample by weighting each study’s number of patients. Data regarding return to play at preinjury or higher level were recorded as dichotomous outcomes and combined via a proportion meta-analysis using a random-effects model. 27 The I 2 index was used to measure the amount of inconsistency in the results of the studies. 28 The mean and 95% CI were calculated for rates of return to play at preinjury or higher level. Studies in the meta-analyses were weighted according to sample size. A Freeman-Tukey transformation was used to calculate the weighted summary proportion. 15,22 The rate of return to play at preinjury or higher level, for individual studies in addition to the pooled rate, are presented as forest plots. A P value ≤.05 was considered significant for all statistical analyses.
Results
Study Selection
Figure 1 shows a flowchart of the study selection process. The literature search yielded a total of 5316 articles, with 4759 unique articles. A total of 90 articles were selected for full-text analysis: the full text of 4 articles was not obtained, and 46 articles were excluded (Table 2). Seven additional articles were identified in a hand search, for a total of 47 articles in this systematic review. All articles were published between November 1991 and May 2020.

Study selection process using PRISMA flow diagram (Preferred Reporting Items for Systematic Meta-analyses). 48
Reasons for Exclusion After Full-Text Analysis

Quality of Studies
From the 47 articles selected, 44 were classified as level 4 evidence, 1 was classified as level 3, 1 randomized controlled trial as level 1b, and another randomized controlled trial as 2b. The randomized trial comparing open with endoscopic repair of the posterior inguinal wall 71 was considered a high-quality trial, with 21 of 25 points according to CONSORT-based scoring. 3,29 The second randomized trial comparing surgical with nonoperative treatment 52 was considered an intermediate-quality trial, with 14 of 25 points according to CONSORT-based scoring. 3,29 The remaining 45 articles were observational studies and scored on average 6.6 points (range, 3-13 points) according to the MINORS criteria—16 points for the 44 noncomparative studies and 24 points for the 1 comparative study 72 (Table A1). The quality of the observational studies improved modestly with time, with a mean MINORS score 72 of 6 for articles published between 1991 and 2000, 6.53 for articles from 2001 to 2010, and 6.9 for articles published from 2011 to 2020.
Patients and Surgery
The total number of patients who underwent surgery in the 47 articles was 2737, of which 94% were male and 6% were female. The mean age of the patients was 27.8 years (range, 12-65 years). The mean duration of symptoms was 13.1 months (range, 0.3-144 months). Forty-four articles (2766 patients) presented the distribution of the patients according to their sports activity. The most frequent sports were soccer (71% of the patients), rugby (7%), Australian football (5%), ice hockey (4%), American football (4%), running (3%), Irish football (2%), Gaelic football (2%), and basketball (1%).
Imaging performed preoperatively was variable among the articles and included radiography, ultrasonography, bone scintigraphy, and magnetic resonance imaging. Of the 47 studies, 34 (72%) did not require a positive imaging finding to indicate the surgical procedure; 8 (17%) required a positive imaging finding to indicate surgery; and 5 (11%) performed imaging but were not clear about the requirement of a positive finding to indicate surgery. The surgery was performed by a general surgeon in 29 (62%) of the 47 studies, by an orthopaedic surgeon in 13 (27%), by a general and orthopaedic surgeon in 4 (9%), and by a plastic surgeon in 1 (2%). From the 2737 patients, the inguinal area was surgically addressed in 2308 (84%), the adductor origin in 700 (27%), and the pubic symphysis in 68 (2.5%). The complications are presented according to each study in Table A2. An infection rate was reported in 13 studies and averaged 1.35% (range, 0%-5%). A reoperation rate was cited in 16 studies and averaged 2.4% (range, 0%-12.5%). A recurrence rate was indicated in 16 studies and averaged 4.1% (range, 0%-26%).
Inguinal Procedures
Surgical procedures limited to the inguinal area were reported in 1558 patients from 23 articles (Table 3). A mesh was utilized in 82% of these patients. All 5 articles published before 2001 did not utilize mesh for the repair of the inguinal wall. 7,26,41,59,84 In the past 20 years, only 2 (11%) of the 18 articles reported repairs without mesh reinforcement. 71,75 The posterior inguinal wall was repaired in 1513 patients in 21 studies. ∥ Repair of the anterior inguinal wall (external oblique aponeurosis) and neurotomy of the iliohypogastric or ilioinguinal nerve was performed in 45 patients in 2 studies. 30,84 Return to play at preinjury or higher level was observed in 92% (95% CI, 88%-95%) of the athletes in the 17 studies that provided this information (Figure 2). The rate of return to play at preinjury or higher level was 93% (95% CI, 89%-96%) for posterior inguinal wall repairs and 85% (95% CI, 74%-94%) for anterior inguinal wall repairs with neurotomy.
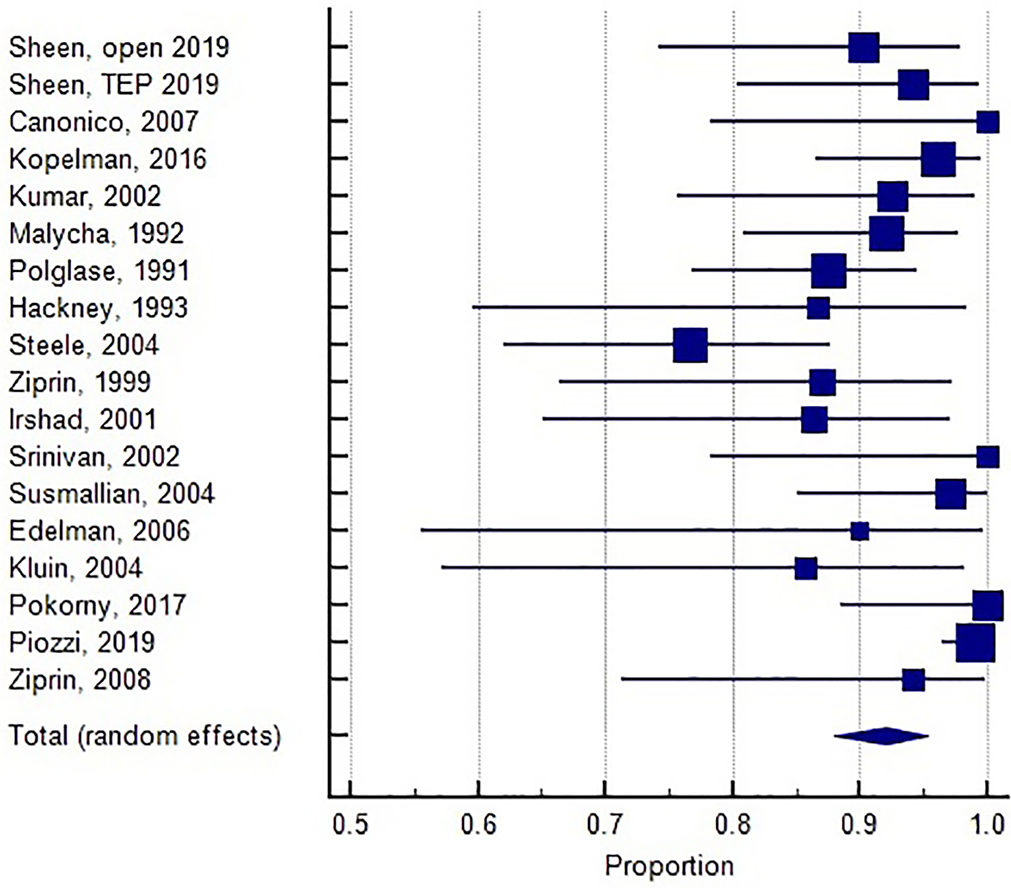
Inguinal area procedures: forest plot of return to play at preinjury or higher level. Proportions (expressed as percentage) with their 95% CIs are shown. The square markers vary in size according to the weights assigned to the studies.
Characteristics of 23 Studies Reporting Results of Surgery to the Inguinal Area for Chronic Groin Pain in Athletes a

a Blank cells indicate not reported. MINORS, Methodological Index for Non-randomized Studies; NA, not applicable; NR, not reported; NRS, numerical rating scale; RCT, randomized controlled trial; TAPP, transabdominal preperitoneal; TEP, totally extraperitoneal; VAS, visual analog scale.
b A mean postoperative follow-up <6 months was considered an exclusion criterion. The study was included in the systematic review if it did not report the mean follow-up but reported a minimum follow-up of 6 months.
c Values in parentheses: (preoperative mean; last follow-up mean).
d Roos et al 63 presented preoperative and 3-month postoperative HAGOS (Copenhagen Hip and Groin Outcome Score) but not more than 6 months of last follow-up HAGOS.
From the 21 studies (1513 patients) describing repair of the posterior inguinal wall, an open surgical approach was utilized in 10 studies (393 patients) and a TEP or TAPP approach in 12 studies (1120 patients). Mesh was inserted in 34.4% of the open repairs and in 100% of the TEP/TAPP repairs. The mesh was secured with staples or tacks by 40% of the surgeons, with sutures by 30% of the surgeons, and with fibrin glue by 15% of the surgeons. Mesh without anchorage was utilized by 15% of the surgeons, all of them performing the TEP technique. Among the 15 studies (653 patients) reporting return to play at preinjury or higher level after repair of the posterior inguinal wall, 89.5% (95% CI, 84%-94%) of the athletes with open repair and 96% (95% CI, 92%-98%) with TEP/TAPP repair were able to return at preinjury or higher level of activity, a statistically significant difference (P = .0012). A randomized controlled trial 71 compared open suture repair (31 patients) versus endoscopic mesh repair (TEP; 34 patients), and the rates of return to full sport activity were 90.3% and 94.1%, respectively, for a nonsignificant difference (P = .238).
Adductor Origin Procedures
Surgical procedures limited to the adductor origin/rectus abdominis insertion were reported in 349 patients from 8 studies (Table 4): 95 patients in 4 studies underwent open adductor tenotomy 1,32,40,68 ; 157 patients in 2 studies had puncture adductor tenotomy 2,62 ; 85 patients in 1 study had repair of the rectus abdominis–adductor longus aponeurotic plate 19 ; and 12 patients in 1 study had adductor fasciotomy and obturator nerve anterior branch neurectomy. 13 Return to play at preinjury or higher level was observed in 75% (95% CI, 57%-89%) of the athletes after adductor tenotomy as the only procedure (Figure 3).

Adductor origin procedure: forest plot of return to play at preinjury or higher level. Proportions (expressed as percentage) with their 95% CIs are shown. The square markers vary in size according to the weights assigned to the studies.
Characteristics of 8 Studies Reporting Results of Surgery to the Adductor Area for Chronic Groin Pain in Athletes a

a Blank cells indicate not reported. EQ-5D, European Quality of Life–5 Dimensions Scale; GDS, Groin Disability Score; HOS, Hip Outcome Score; HOOS, Hip disability and Osteoarthritis Outcome Score; MINORS, Methodological Index for Non-randomized Studies; NR, not reported; NRS, numerical rating scale for pain; SF-36, Short-Form Health Survey; VAS, visual analog scale.
b Values in parentheses: (preoperative mean; last follow-up mean).
Pubic Procedures
Surgical procedures limited to the pubic symphysis were reported in 30 patients from 2 studies (Table 5): 23 patients in 1 study underwent pubic symphysis curettage, 60 and 7 patients in another study underwent pubic symphysis arthrodesis. 82 Return to play at preinjury or higher level was observed in 84% (95% CI, 47%-100%) of these athletes (Figure 4).

Pubic symphysis procedures: forest plot of return to play at preinjury or higher level. Proportions (expressed as percentage) with their 95% CIs are shown. The square markers vary in size according to the weights assigned to the studies.
Characteristics of 2 Studies Reporting Results of Surgery to the Pubic Symphysis for Chronic Groin Pain in Athletes a

a Blank cells indicate not reported. MINORS, Methodological Index for Non-randomized Studies; NR, not reported; VAS, visual analog scale.
b Values in parentheses: (preoperative mean; last follow-up mean).
Inguinal + Adductor Origin Procedures
Five studies reported the results of posterior inguinal wall repair in association with adductor tenotomy in 211 patients 17,32,46,65,79 (Table 6). Return to play at preinjury or higher level, reported in 4 of the studies (199 patients), was observed in 89% (95% CI, 70%-99%) (Figure 5).

Combined inguinal + adductor origin procedures: forest plot of return to play at preinjury or higher level. Proportions (expressed as percentage) with their 95% CIs are shown. The square markers vary in size according to the weights assigned to the studies.
Characteristics of 5 Studies Reporting Results of Posterior Inguinal Wall Repair Associated With Adductor Tenotomy for Chronic Groin Pain in Athletes a

a MINORS, Methodological Index for Non-randomized Studies; NR, not reported.
Pubic Symphysis + Adductor Origin Procedures
One article with 30 patients reported the results of pubic symphysis resection in association with bilateral adductor release and partial tenotomy of the rectus abdominis. 14 At a mean follow-up of 36 months, the authors noted 100% return to play, 100% satisfaction from the patients, and a mean time of 8 months to return to sport.
Mixed Surgery
A study reporting variation among patients on the surgical technique was classified as mixed if the results were not separated by anatomic area; 10 studies with 559 patients were classified as such (Table 7). Return to play at preinjury or higher level ranged from 90% to 97% of the athletes in this group of studies.
Characteristics of 10 Studies Reporting Results of Surgery in Different Anatomic Areas for Chronic Groin Pain a
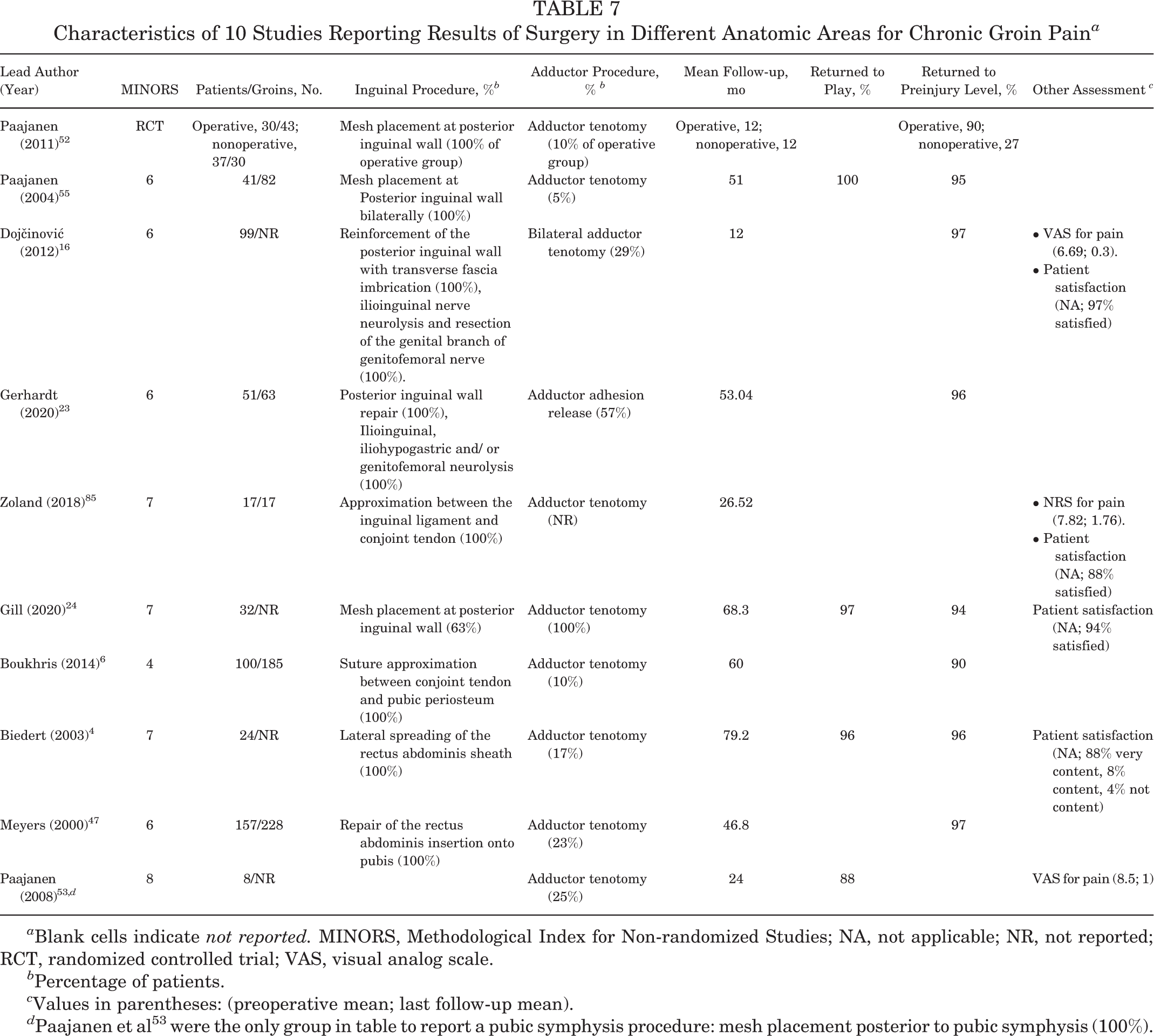
a Blank cells indicate not reported. MINORS, Methodological Index for Non-randomized Studies; NA, not applicable; NR, not reported; RCT, randomized controlled trial; VAS, visual analog scale.
b Percentage of patients.
c Values in parentheses: (preoperative mean; last follow-up mean).
d Paajanen et al 53 were the only group in table to report a pubic symphysis procedure: mesh placement posterior to pubic symphysis (100%).
Discussion
The present systematic review found that the rate of return to play at preinjury or higher level was 92% in athletes after surgical procedures limited to the inguinal area, 75% after surgery limited to the adductor origin, 84% after surgery limited to the pubic symphysis, and 89% after combined surgery in the inguinal and adductor origin. Athletes with inguinal-related pain presented a better prognosis than athletes with adductor-related pain (P < .001). Although return to preinjury level in athletes with inguinal-related pain was more frequent (92%) than in those with pubic-related pain (84%), the difference was not statistically significant (P = .12). The 10 studies composing the mixed group demonstrated variation among patients on the anatomic areas surgically addressed, without separation of results per technique, and reported return to play at preinjury or higher level from 90% to 97%. The present systematic review included articles with a follow-up >6 months and used returning to previous level of activity as an outcome to help differentiate outcomes after surgery for inguinal-, pubic-, and adductor-related groin pain.
We found that return to play at preinjury or higher level was more frequent in TEP/TAPP repair (97.1%) than open repair of the posterior inguinal wall (89.5%) for athletes with inguinal-related CGP. However, a high-quality randomized controlled trial reported a nonsignificant difference on return to full sport activity when comparing open suture repair (90.3%) versus TEP repair (94.1%; P = .238). 71 The mean time to return to sport was cited in 12 (57%) of the 21 studies involving repair of the posterior inguinal wall. A comparison on the time to return to sport between open and TEP/TAPP repair was not feasible owing to variation or a lack of definition on the meaning of "return to sport" among authors (ie, if returning to training or competition).
The number of studies on the surgical treatment of CGP in athletes has consistently increased in the past decade. From the 47 articles reviewed, 8 were published between 1991 and 2000, 15 between 2001 and 2010, and 24 between 2011 and 2020. Only 2 (4%) were randomized controlled trials: 1 high-quality trial comparing open with endoscopic repair of the posterior inguinal wall 71 and 1 intermediate-quality trial comparing surgical with nonoperative treatment. 52 Although both trials were published in the past decade, the quality of the observational studies improved modestly with time, with a mean MINORS score 72 of 6 for articles published between 1991 and 2000, 6.53 for articles published from 2001 to 2010, and 6.9 for articles published from 2011 to 2020. Regarding the 45 observational studies, just 1 scored above 10 points. 40 The main reason for the low MINORS scores observed was the lack of a control group in 44 of the 45 observational studies (98%) (Table A1). Serner et al 69 addressed the low quality of the studies on surgical treatment for CGP in athletes. The authors reported a moderate and inverse correlation between study quality and treatment success (P < .001; r = –0.41); that is, low-quality studies showed significantly higher treatment success from 1985 and 2014.
CGP may present very differently from one athlete to another. In 1985, Brunet 8 categorized cases of athletes with CGP into 3 groups: abdominal parietal pathology, musculotendinous pathology of the adductors, and microtraumatic pubic osteoarthropathy. 21 In 2015, the Doha consensus presented a similar classification of CGP in athletes, with 4 entities: inguinal-, adductor-, pubic-, and iliopsoas-related groin pain. 80 Our review did not comprise articles discussing surgical procedures at the iliopsoas tendon, given that iliopsoas tendon–related problems are addressed with intra-articular procedures involving the hip joint. Despite the Doha agreement and the efforts of Brunet on classifying CGP in athletes, 8,21,80 most articles from the current systematic review did not present the frequency of clinical or imaging findings specific to the inguinal, adductor, or pubic symphysis. One exception was the study by Kajetanek et al, 32 who utilized radiographs, ultrasonography, and magnetic resonance findings to classify patients with abdominal wall injuries, adductor tendon injuries, or both.
In studies using mesh for repair of the posterior inguinal wall, the mesh was secured with staples, tacks, or sutures by 70% of the surgeons. Fibrin glue or mesh without anchorage was used by 30% of the surgeons inserting mesh for the surgical treatment of inguinal-related CGP in athletes, particularly in the past 5 years. 57,58,63,71,78 This tendency is explained by the increased risk of chronic pain associated with tack utilization in laparoscopic inguinal hernia repair. 70 Mesh insertion without anchorage or glue is possible in the TEP technique, which does not violate the peritoneum and allows the abdominal pressure to maintain the mesh positioning. 63,71 Despite the theoretical advantage of the glue or no anchoring in comparison with tacks or staples, comparison among the mesh fixation methods was not feasible in the present systematic review owing to differences in surgical techniques among authors in surgical aspects other than mesh fixation. In addition, sensory changes and symptoms of entrapment of the superficial inguinal nerves were researched by just 1 study 23 (Appendix 2).
Hip joint abnormalities have been associated with abnormal forces across the pubic symphysis and secondary pubic pain. 5,39,66 In patients with femoroacetabular impingement, surgically addressing the hip impingement often results in improvement of the pubic-related complaints. 39,66 The present systematic review did not include articles in which the primary surgery was performed in the hip joint. Given the biomechanical role of the hip joint on the pelvic girdle, future studies on CGP in athletes should consider the inclusion of physical examination findings on the hip, particularly the flexion, extension, adduction, abduction, and rotational range of motion.
One article reported the influence of symptom duration on the surgery results of 64 patients with inguinal-related CGP. 59 The authors observed a better chance of full recovery in patients with <2 years of symptoms. From the 11 athletes with symptoms lasting >2 years, 2 (18%) considered themselves completely cured, 7 (64%) partially cured, and 2 (18%) were dissatisfied with surgery. 59
Four articles reported bilateral repair of the posterior inguinal wall in all operated cases, independently if 1 side was asymptomatic. 45,55,57,75 Matikainen et al 45 and Paajan et al 55 justified the bilateral placement of a mesh on the posterior inguinal wall because scarring of the preperitoneal space would most likely prevent a later operation of the nonaffected side. Piozzi et al 57 and Van Meirhaeghe et al 79 argued that performing a TAPP procedure unilaterally could not fully balance and stabilize the anatomic region.
Most articles (96%) in the present systematic review did not assess the athletes pre- and postoperatively with validated and quantitative functional scores. Comparison among surgical techniques was compromised by the use of qualitative assessments or quantitative scores of relatively low sensitivity to athletes, such as pain scales. Validated quantitative scores assessing performance level were cited in 3 articles: 2 with pre- and postoperative scores 2,40 and 1 with postoperative scores. 19 Utilizing return to play to compare treatments may result in overestimating the level to which the athletes’ performance has recovered. 51 Frequency and time to return can be interpreted very differently by distinct examiners or patients: return to training, return to competition at a lower intensity, or return to full competition. Kajetanek et al 32 minimized the impreciseness of the outcome by rating return to play as return to training, running, and competition. The sensitivity of return-to-play data to detect differences among surgical techniques may be particularly decreased in professional athletes, as some may return to sports without improvement in their symptoms for financial issues. The utilization of return to play at the preinjury level may be more sensitive to differences, although it is still far from ideal. Pain scales also have important limitations, and most articles citing a pain score did not specify if it referred to pain at rest or during activity. An additional weakness of many studies in our systematic review was the utilization of examiner-reported scores. Patient-reported outcomes have been demonstrated to be superior to examiner-reported scores. 44 Future investigations on the surgical treatment for CGP should utilize quantitative and validated patient-reported functional scores to facilitate comparison among studies and surgical techniques. Examples of patient self-administered scoring systems with consistent testing in active and athletic populations include the Hip Outcome Score, the Non-arthritic Hip Score, and the International Hip Outcome Tool. 12,43,49
Previous systematic reviews studied the surgical outcomes for CGP in athletes but did not compare outcomes based on clinical condition and/or surgical technique. 11,76 Two systematic reviews compared the outcomes of surgical and nonoperative treatments. 31,33 King et al 33 found return-to-play rates of 86%, 96%, 84%, and 96% at 23, 7.2, 18.3, and 21.9 weeks for pubic-, abdominal-, adductor-, and abdominal/adductor-related groin pain, respectively. In a more recent review, Jørgensen et al 31 reported return to habitual activity after inguinal hernia repair, adductor tenotomy, and combined inguinal hernia repair with adductor tenotomy to be 94%, 90%, and 97% after a median of 10, 12, and 10 weeks, respectively. The limitations of the King and Jørgensen reviews include not defining return to previous level of sports participation, not comparing specific procedures within each clinical entity, and including reports of short-term outcomes in their results. 31,33 Additionally, the King review comprised literature only to June 2013. 33 A review by Paajanen et al 54 compared laparoscopic (TAPP) and endoscopic (TEP) repair of inguinal-related CGP in athletes. The authors found 86% and 97% recovery for TAPP and TEP, respectively, with the same median return to sporting activity of 28 days. 54
There has been an effort to better categorize athletes with CGP in the past decade. The Doha consensus was published in 2015 and will ideally serve as the foundation for cohort and randomized trials based on specific categories. 80 The diagnosis of CGP is still essentially clinical, with the inherent limitations attributed to the subjectivity of the examiners. The advancement in the surgical techniques to treat CGP has surpassed by far any progress on the diagnosis of CGP. Therefore, additional research on the physical examination, imaging, and injections will be essential to help clinicians categorize their cases into the diverse disorders causing CGP. Future cohort studies and randomized trials with more detailed patient categorization are fundamental to define the best treatment approach for patients with CGP and will allow more definitive recommendations.
The present systematic review has a number of limitations. First, only 4% of the studies were randomized controlled trials, 52,71 and 98% of the observational studies did not present a control group. As with all systematic reviews, the power of the findings is directly proportional to the quality of the studies. Second, pre- and postoperative validated quantitative scores assessing performance level were reported in 2 articles (4%). 2,40 The lack of functional scores decreases the sensitivity of studies to detect changes between pre- and postoperative status and to compare the effect of different surgical techniques in athletic performance. Third, the present systematic review assumed that the anatomic area surgically addressed corresponded to the predominant origin of the symptoms. However, most studies did not present the frequency of physical examination and imaging findings according to the inguinal, adductor, and pubic anatomic area. Therefore, patients with similar clinical presentations could have undergone surgery in distinct anatomic areas according to the expertise of the surgeon. Fourth, the techniques for each procedure had been refined over the reporting years. Earlier studies may not be fully representative of current practice, and both older and newer studies were weighted equally. Last, as with all systematic reviews, it is possible that relevant articles or patient populations were not identified with our search criteria.
Conclusion
Our analysis showed that return to play at preinjury or higher level is more likely after surgery for inguinal-related CGP (92%) in comparison with surgery for adductor-related CGP (75%). However, the majority of studies on the surgical treatment of CGP in athletes was methodologically of low quality because of the lack of comparison groups. Future research on the surgical treatment of CGP in athletes should utilize quantitative and validated functional scores to facilitate comparison among surgical techniques.
Footnotes
Final revision submitted January 25, 2021; accepted February 24, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.B. has received teaching fess and research financial support from Smith & Nephew, outside the submitted work. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.