
Abstract
Background:
Variations in scapular morphology have been associated with the development of atraumatic rotator cuff tears (RCTs). The critical shoulder angle (CSA) accounts for both glenoid inclination and lateral extension of the acromion. The impact of the CSA on outcomes after rotator cuff repair (RCR) has not been investigated previously.
Hypothesis:
Our hypothesis was that individuals with smaller CSAs will have better patient-reported outcome scores over time compared with those with larger CSAs. Theoretically, a smaller CSA minimizes the biomechanical forces favoring superior translation of the humeral head, which may be advantageous after RCR. This is the first study to examine the relationship between the CSA and clinical outcomes after RCR.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Fifty-three patients (mean age, 61 years) with atraumatic full-thickness RCTs who underwent arthroscopic RCR were prospectively evaluated. Demographic data as well as the Western Ontario Rotator Cuff Index (WORC) score, American Shoulder and Elbow Surgeons (ASES) score, and a visual analog scale (VAS) for pain were prospectively collected at various time points up to 24 months postoperatively. Statistical analysis included longitudinal multilevel regression modeling to investigate the association between the CSA and the WORC, ASES, and VAS scores.
Results:
The overall clinical outcome, as measured by the WORC, ASES, and VAS, improved significantly (P < .0001). Controlling for demographic and clinical characteristics, a multilevel regression analysis demonstrated that the CSA was not a significant independent predictor for change in WORC (P = .581), ASES (P = .458), or VAS (P = .859) scores at 24 months after arthroscopic RCR. Interobserver and intraobserver reliability for CSA measurements resulted in interclass correlation coefficients of 0.986 and 0.982, respectively (P < .001), indicating excellent agreement.
Conclusion:
The CSA did not appear to be a significant predictor of patient-reported outcomes after arthroscopic repair of atraumatic full-thickness RCTs.
Variations in scapular morphology have been associated with the development of atraumatic rotator cuff tears (RCTs). Theories proposed by Neer, 15 Bigliani et al, 2,3 and Nicholson et al 16 focus predominantly on acromial morphology as it pertains to the pathogenesis of rotator cuff disease. These authors suggest that primary mechanical impingement of the rotator cuff is the essential underlying factor in rotator cuff disease. Conversely, alternate theories suggest a morphologic predisposition for altered shoulder biomechanics favoring the development of RCTs. 8,17,19
Most recently, Moor et al 12,14 described the critical shoulder angle (CSA), a radiographic measure that accounts for both glenoid inclination and lateral extension of the acromion (Figure 1). The CSA more completely accounts for individual anatomic variations and the subsequent biomechanical forces acting on the humeral head during shoulder abduction. Moor et al 12 demonstrated that larger CSAs (>35°) were associated with an increased prevalance of RCT, whereas smaller CSAs (<30°) were associated with glenohumeral arthritis. The correlation between the CSA and rotator cuff disease has been recently supported by several studies. 4,5,18 Furthermore, individuals without shoulder pathology had lower mean CSAs (33°) compared to those with RCTs (38°). 12 Moor et al 14 also demonstrated that the CSA is the most accurate radiographic predictor for the development of atraumatic RCTs.

The critical shoulder angle (CSA) is formed between a line extending from the superior to the inferior aspect of the glenoid and a second line extending from the inferior aspect of the glenoid to the inferolateral aspect of the acromion on true anteroposterior radiographs with the arm in neutral position. (A) Right shoulder with a CSA of 27°. (B) Right shoulder with a CSA of 41°.
The purpose of this study was to investigate the relationship between the CSA and clinical outcomes after rotator cuff repair (RCR), which has not previously been investigated. Theoretically, a smaller CSA minimizes the biomechanical forces favoring superior translation of the humeral head, which may be advantageous after RCR. We hypothesized that individuals with smaller CSAs will have better outcomes as measured by the Western Ontario Rotator Cuff Index (WORC), the American Shoulder and Elbow Surgeons (ASES) score, and the visual analog scale (VAS) for pain after RCR.
Methods
Patient Selection
The patients included in this study were a subset of a larger prospective, institutional review board–approved study, which began in March 2009 and continues to the present. This larger study evaluated clinical outcomes in patients with RCTs diagnosed either by magnetic resonance imaging or ultrasound. As part of this study, patients were asked if there was any history of trauma preceding their shoulder pain. Those who did not report a traumatic incident were deemed to have atraumatic or attritional RCTs. Adult patients with atraumatic full-thickness RCTs who underwent arthroscopic RCR were subsequently enrolled in our study. Neither acromioplasty nor distal clavicle excision was routinely performed; however, either procedure may have been performed at the surgeon’s discretion. Patients followed a standard postoperative protocol. We chose to evaluate atraumatic tears to isolate the biomechanical effects of the CSA to avoid confounding variables related to traumatic tears. Patients with radiographic evidence of concomitant pathology, including cuff tear arthropathy, posttraumatic deformity, bony abnormalities, and moderate to severe glenohumeral arthritis, were excluded.
Demographic and comorbidity data (age, gender, history of shoulder trauma, diabetes, tobacco use, symptom duration, and body mass index [BMI]) and written questionnaires, including the WORC, ASES score, and VAS for pain, were collected at the initial visit (baseline) and various standardized follow-up time points up to 24 months.
Radiographic Assessment
We obtained CSA measurements for 60 patients with documented atraumatic full-thickness RCTs with 24 months of follow-up. Seven patients were excluded due to unacceptable radiographic criteria, as determined by the authors who reviewed their plain radiographs (J.M.K. and A.N.). Two of the authors in this study (J.M.K. and A.N.) separately and independently assessed patient radiographs while blinded from all outcome measures and demographic data. All radiographic measurements were made electronically using PACS software (Cerner Corp). The CSA was measured as originally described by Moor et al. 12 True anteroposterior radiographs of the glenoid with the arm in neutral position were used. Four patients were excluded due to excessive arm abduction. Only radiographs with less than 20° of estimated malrotation based on the shape of the glenoid were included. This was based on the findings of Moor et al, 12 who determined that less than 20° of malrotation resulted in consistent minimal variability less than 2° in CSA assessment. If there was disagreement between the blinded reviewers regarding radiograph malrotation, the patient was excluded from the study. Three patients were excluded based on malrotation. If any deformity or osseous irregularity of the glenoid or acromion obstructed landmarks used to measure the CSA accurately, the patient was also excluded from the study. After a period of 4 months, one of the authors (J.M.K.) remeasured the CSAs of all of the patients included in the study to determine intraobserver reliability.
Patients with CSAs <38° were compared with those with CSAs >38°. The value of 38° was chosen based on several factors. Moor et al 12 determined that the mean CSA in an RCT population was 38°. We performed a preliminary analysis, which demonstrated that individuals with a CSA <38° had superior outcomes compared with those with CSA >38°. We therefore felt that this was a reasonable value to delineate between those individuals in the RCT population with a small CSA and those with a large CSA.
Statistical Analysis
Descriptive and inferential statistics were analyzed using SPSS version 22.0 (IBM Corp). The dependent variables included score change from baseline to final follow-up for ASES, VAS pain score, and WORC. The demographic, treatment, and comorbidity characteristics were described by using raw counts, measures of central tendency (eg, mean, median, or mode), and measures of data dispersion (eg, 95% CIs and standard errors) where appropriate. Paired-sample t tests were used to examine the change in clinical outcomes from baseline to 1 year and 2 years for the entire cohort for ASES, VAS pain score, and WORC. Independent-sample t tests were then conducted to explore the differences between CSA groups. Univariable and multivariable mixed methods linear regressions were conducted using 3 models for ASES, VAS pain score, and WORC (controlling for surgeon as a random variable) to investigate the predictive effect of the CSA on outcome scores across time. An a priori sample size calculation was conducted, and on the basis of estimates of a moderate to large effect size (d = 0.50), it was determined that 17 subjects per group would be needed to obtain a power of 0.80 using an estimated VAS pain score outcome for the calculation. Statistical significance was set at P < .05. Additionally, we calculated interclass correlation coefficients (ICCs) to measure interobserver agreement between the 2 reviewers (J.M.K. and A.N.) and intraobserver reliability for 1 reviewer.
Results
Fifty-three patients with 24 months of follow-up were included in the final analysis. Eighteen patients had CSAs greater than 38° (mean, 39.9°), whereas 35 patients had CSAs less than 38° (mean, 32.9°), which was statistically significant (P = .001). Controlling for demographic and clinical characteristics, a multilevel regression analysis demonstrated that the CSA was not a significant independent predictor for change in WORC (P = .581, Figure 2), ASES (P = .458, Figure 3), or VAS (P = .859, Figure 4) scores. Of note, when the CSA was analyzed as a continuous variable, it had borderline significance as an independent predictor of change in VAS pain score from baseline to 12 months (β = −2.25; P = .078; 95% CI, −4.78 to 0.226); however, not at 24 months (P = .295). Additionally, the continuous analysis did not demonstrate significance at 12 or 24 months, respectively, for the ASES (P = .440, P = .626) or WORC (P = .418, P = .416). Inter- and intraobserver reliabilities for CSA measurements resulted in ICCs of 0.969 and 0.982, respectively, indicating excellent agreement.

The mean Western Ontario Rotator Cuff (WORC) score at baseline (BL) and 6, 12, and 24 months after rotator cuff repair in patients with a critical shoulder angle >38° compared with those <38°.

The mean American Shoulder and Elbow Surgeons (ASES) score at baseline (BL) and 6, 12, and 24 months after rotator cuff repair in patients with a critical shoulder angle >38° compared with those <38°.

The mean visual analog scale (VAS) pain score at baseline (BL) and 6, 12, and 24 months after rotator cuff repair in patients with a critical shoulder angle >38° compared with those <38°.
Overall, patient-reported outcome scores for the entire cohort improved significantly compared with baseline (Table 1). Patients with a CSA >38° were significantly older in age. There were no differences in baseline demographic characteristics such as sex, BMI, presence of diabetes, or a history of smoking (Table 2). Additionally, there was no significant difference in comparing patients with CSAs of less than 38° to patients with CSAs greater than 38° with regard to baseline functional outcome and pain scores (shoulder activity level, ASES, WORC, and VAS). RCT and RCR characteristics were also analyzed and found to have no significant differences between CSA groups.
t Tests Demonstrating Net Change in Patient-Reported Outcomes for the Entire Cohort a

a Values are reported as mean (SD). The P value reflects the change from baseline to 2-year follow-up. Of note, the change in baseline scores to 1-year follow-up demonstrated the same level of statistical significance. The level of significance was set at P < .05. ASES, American Shoulder and Elbow Surgeons score; VAS, visual analog scale; WORC, Western Ontario Rotator Cuff score.
Demographics, Clinical Characteristics, and Outcome Scores (N = 53) a
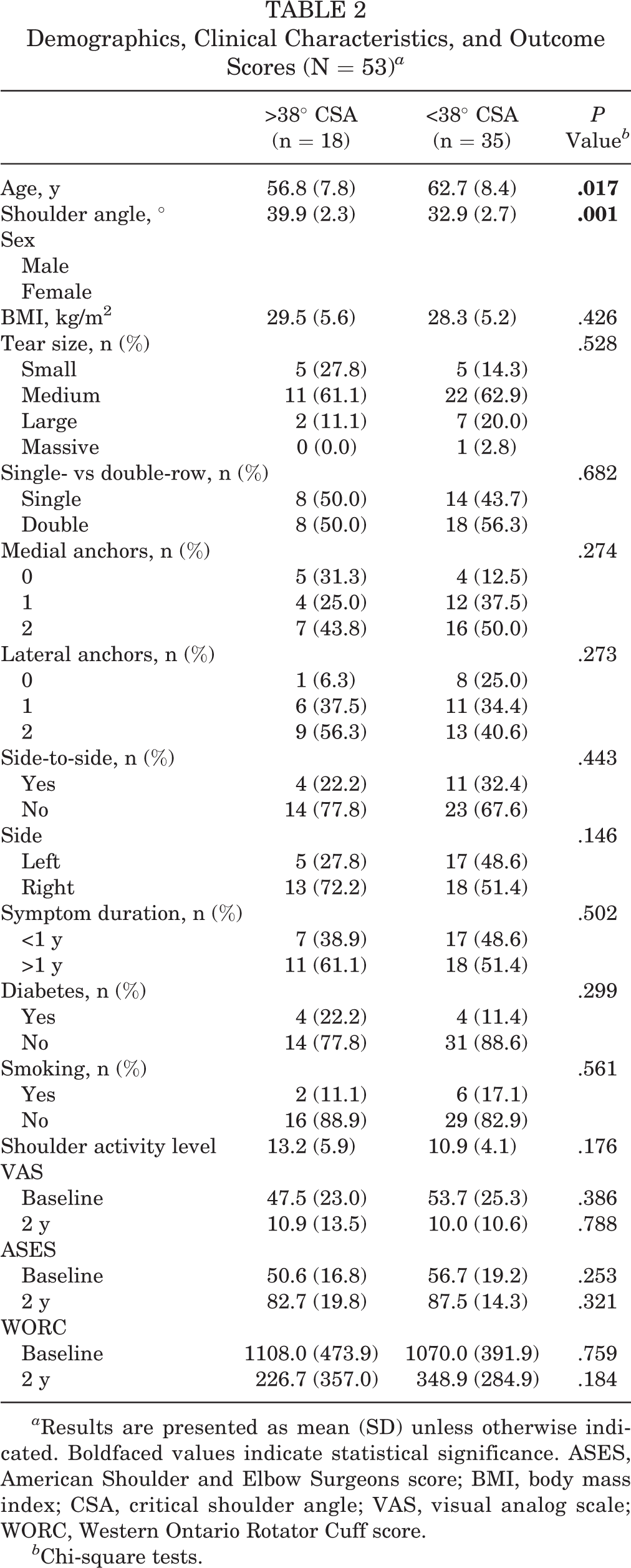
a Results are presented as mean (SD) unless otherwise indicated. Boldfaced values indicate statistical significance. ASES, American Shoulder and Elbow Surgeons score; BMI, body mass index; CSA, critical shoulder angle; VAS, visual analog scale; WORC, Western Ontario Rotator Cuff score.
b Chi-square tests.
Discussion
The findings of this study suggest that the CSA does not appear to be an independent predictor of patient-reported outcomes at 2 years after arthroscopic repair of atraumatic full-thickness RCTs. Interestingly, the CSA may influence midterm pain scores as it had borderline significance as an independent predictor of change in pain VAS at 12 months (P = .045). To our knowledge, this is the first study to evaluate the effect of the CSA on patient-reported outcomes after atraumatic RCR.
Individual variations in acromial and glenoid morphology are often implicated in the pathogenesis of rotator cuff disease. Early theories focused primarily on the role of the acromion in RCTs. Neer 15 recognized the mechanical conflict between the rotator cuff and the acromion and subsequently termed this condition impingement syndrome. Other authors have used both cadaveric models and 3-dimensional imaging to investigate the correlation between acromial slope and rotator cuff disease. 2,3,10,16 Currently, significant controversy exists regarding whether the morphologic characteristics observed in the acromion are a contributor or consequence of rotator cuff disease.
Recent theories regarding the pathogenesis of RCTs have focused on the roles of both the glenoid and acromion as they pertain to altered shoulder biomechanics. Hughes et al 8 were among the first to describe the relationship between glenoid inclination and rotator cuff disease. In their cadaveric study, 8 the degree of superior inclination of the glenoid was significantly greater in those shoulders with full-thickness RCTs compared with shoulders without RCTs. The authors hypothesized that increased glenoid inclination would result in a larger shear force vector on the humeral head at the glenohumeral joint. 8 This has 2 important implications: A reduced amount of deltoid force would be required to produce superior migration of the humeral head, and the rotator cuff would be required to exert a greater compensatory force to balance the force of the deltoid when attempting to stabilize the humeral head within the glenoid. Wong et al 21 subsequently demonstrated the former point in a cadaveric model in which they varied the degree of glenoid inclination and measured the force required to produce superior migration of the humeral head. A positive glenoid inclination of 10° resulted in a 30% decrease in the force required to produce superior migration. 21
Nyffeler et al 17 incorporated similar biomechanical principles into their description of the acromial index (AI). The AI is the ratio of the distance in the vertical plane extending from the glenoid to the lateral aspect of the acromion compared with the distance from the glenoid to the lateral aspect of the humeral head. Nyffeler et al 17 purported that a more laterally extending acromion would produce a more vertically directed net force vector during deltoid contraction. As a result, there may be a greater propensity for superior humeral head migration in individuals with a large AI, resulting in rotator cuff impingement and subsequent rotator cuff disease. In their series, an increased AI was significantly associated with attritional full-thickness RCTs. 17 Other studies have failed to identify a positive correlation between AI and attritional RCTs. 1,11
The CSA is a novel radiographic parameter that combines the biomechanical principles proposed by Hughes et al 8 and Nyeffeler et al 17 by accounting for both glenoid inclination and lateral extension of the acromion. A recent study 14 comparing the AI, lateral acromial angle (LAA), CSA, and acromial slope concluded the CSA was the most accurate radiographic predictor of the presence of a degenerative RCT. This study also found that the AI and the LAA were accurate predictors of RCTs, whereas there was no significant correlation with the sagittal morphology of the acromion. 14
Large CSAs may result in a propensity for superior humeral head translation during shoulder abduction. 7,8,12,17 A large CSA occurs when there is a superiorly inclined glenoid in conjunction with a laterally extending acromion. This morphologic combination theoretically produces an increased shear force vector on the humeral head and therefore less direct compressive force within the glenoid. At the same time, a more laterally extending acromion may result in more vertically oriented deltoid muscle fibers, producing a more superiorly directed net deltoid force vector, particularly at lower degress (between 10° and 60°) of shoulder abduction. 7 A recent cadaveric study by Katthagen et al 9 reported one of the first attempts to surgically decrease the CSA by reducing the lateral extension of the acromion via lateral acromioplasty. The authors were able to decrease the overall CSA by almost 3° while safely preserving the deltoid origin. 9
After RCR, patients with a larger CSA theoretically experience increased force on their rotator cuff compared with patients with a smaller CSA. Increased force on the rotator cuff coupled with superior translation of the humeral head may potentially lead to compromised repair integrity, which may result in inferior patient-reported outcome scores.
A large CSA theoretically requires the rotator cuff to work harder and exert a greater compensatory force to stabilize the humeral head within the glenoid during shoulder movement to establish an adequate fulcrum. Recently, Gerber et al 7 conducted a biomechanical study that addressed the later 2 points. They demonstrated that larger CSAs were associated with decreased compressive force and increased shear force at the glenohumeral joint compared with smaller CSAs. Furthermore, the supraspinatus tendon load increased by 35% to compensate for the increased shear force. 7 Moor et al 13 reported an increased shear force vector at the glenohumeral joint with more superior glenoid inclination in a recent biomechanical study.
Conversely, more neutral inclination of the glenoid and less extension of the acromion (small CSA) results in a net deltoid force vector that is more horizontally directed toward the glenoid in line with the force vector of the rotator cuff. This was recently demonstrated in a biomechanical study, where the authors reported increased glenohumeral joint stability in smaller CSAs. 20 In these instances, the rotator cuff would not have to exert as much compensatory force when balancing the force of the deltoid, since the deltoid force vector is more collinear with that of the rotator cuff and there is less vertical shear component at the glenohumeral joint. Gerber et al 6 reported better functional outcomes after latissimus dorsi transfer in individuals with smaller CSAs, which they attributed to improved glenohumeral joint stability secondary to the decreased work required from musculotendinous force balancing. We hypothesized that in a similar regard, individuals with a smaller CSA may have a biomechanical advantage after RCR resulting in improved functional scores compared with those with a larger CSA; however, this was not the case in our study.
There are several limitations to this study. We utilized validated patient-reported outcome scores to evaluate the influence of the CSA on patient function after RCR. While these scores provide a clinical assessment of patient function, they may not reflect the integrity of the rotator cuff or how the CSA is associated with rotator cuff healing. We did not obtain additional imaging (magnetic resonace imaging or ultrasound) to assess for rotator cuff retear or have histological evidence to suggest impaired healing as a result of larger CSAs. Future studies evaluating the CSA would benefit from having this information as it would more directly associate the biomechanical implications imparted by the CSA with the clinical status of the rotator cuff. Additionally, we are limited by the length of follow-up, which even at 2 years may be preliminary. This study is also subject to recall bias because patients were classified as having atraumatic tears based on their self-reported history. Another potential limitation is lack of inclusion of a musculoskeletal radiologist. We feel that the relative ease of determining the CSA in addition to the excellent agreement demonstrated by the interoberver and intraobserver reliabilities support the validity of the measurements. Finally, we are limited by the size of this study and the patient distribution by CSA. There are no epidemiologic studies to date that describe the mean and normal distribution of CSAs in the population. Our analysis consisted of twice as many patients with CSAs less than 38° compared with those with CSAs greater than 38°, which may either reflect an epidemiological trend or unbalanced distribution within our cohort.
This study also has several strengths. This is the first study to attempt to characterize an association between the CSA and clinical outcomes after RCR. This is an important step in light of the recent paradigm shift, whereby the etiology of rotator cuff disease may be in part due to altered shoulder biomechanics occurring secondary to variations in individual scapular anatomy. In our attempt to investigate the relationship between individual scapular morphology and outcomes after RCR, we are limited by the intrinsic parameters of the CSA, which only accounts for glenoid inclination and lateral extension of the acromion.
The CSA provides a 2-dimensional representation of complex 3-dimensional shoulder biomechanics. Tétreault et al 19 demonstrated an important relationship between glenoid version and RCTs, indicating that glenoid version also influences the force vectors acting on the rotator cuff. It is possible that to fully investigate the relationship between individual scapular anatomy and outcomes after RCT one would have to incorporate the 3-dimensional morphology of the glenoid into this analysis.
Conclusion
Variations in scapular morphology are implicated in the pathogenesis of rotator cuff disease and the outcomes after RCR. While the CSA is a strong radiographic predictor of rotator cuff pathology, it does not appear to have a predictive effect on outcomes after arthroscopic repair of atraumatic full-thickness tears. This is the first study to examine the relationship between the CSA and outcomes after RCR. Further investigation is necessary to elucidate the relationship between individual scapular anatomy and rotator cuff disease.
Footnotes
The authors declared that they have no conflicts of interest in the authorhip and publication of this contribution.
Ethical approval for this study was obtained from the University of Michigan Medical School Institutional Review Board (IRB registration: IRB00001996).