
Abstract
Background:
Acromiohumeral interval (AHI) reversibility is used to evaluate whether superior humeral migration is fixed or flexible in patients with massive rotator cuff tears (MRCTs). AHI reversibility is measured as the difference in the AHI observed between standard and stress radiography. However, factors affecting AHI reversibility have not been studied in the existing literature.
Purpose:
To investigate potential factors affecting AHI reversibility in patients with MRCTs.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A retrospective analysis was conducted on 58 patients with MRCTs, who had undergone magnetic resonance imaging, computed tomography, and stress radiography of the same shoulder. Potential factors affecting AHI reversibility were evaluated by stepwise regression analysis.
Results:
A total of 58 patients (26 male, 32 female) were included in this study. The mean age of the patients was 66.4 ± 8.3 years. There were 33 patients classified as having a reversible AHI and 25 patients classified as having an irreversible AHI. Age, time from symptom onset, anteroposterior tear size, critical shoulder angle (CSA), acromial index, and subscapularis Goutallier grade were associated with AHI reversibility in univariate analysis. Multivariate linear regression analysis showed that a longer time from symptom onset and a bigger CSA were significantly associated with lower AHI reversibility. No significant association was found between AHI reversibility and sex; body mass index; activity level; tear retraction; biceps condition; deltoid cross-sectional area; and Goutallier grade of the supraspinatus, infraspinatus, and teres minor muscles. The cutoff values to predict AHI reversibility for time from symptom onset and CSA were found to be 5.5 years and 38°, respectively.
Conclusion:
Time from symptom onset (>5.5 years) and CSA (>38°) were significant independent factors of AHI reversibility. These factors should be considered for the decision-making process in patients with MRCTs.
Keywords
Superior migration of the humeral head is an inevitable consequence of progressive rotator cuff disease; thus, the acromiohumeral interval (AHI) has been described as a prognostic factor for massive rotator cuff tears (MRCTs).28,30 Multiple studies have provided evidence indicating that a preoperative AHI <7 mm on static radiography is a notable risk factor for failure of both rotator cuff repair and reconstructive procedures such as latissimus dorsi tendon transfer and superior capsular reconstruction.5,25 Conversely, several studies have reported favorable clinical outcomes in cases in which the AHI remains <7 mm after soft tissue reconstructive procedures.8,13 Could it be associated with errors in measurements, or is it more about the dynamic structure of the AHI?
The term “AHI reversibility” refers to the capability of a shoulder with superior migration on standard radiography to return to its original position on stress radiography. AHI reversibility is measured as the difference in the AHI observed between standard radiography and stress radiography with a 5-kg weight applied to the hands. The significance of AHI reversibility, a topic that has received limited attention in the literature, becomes apparent in this context. Recently, two studies proposed that an increase in the AHI on preoperative stress radiography indicated improved outcomes after rotator cuff repair and tendon transfer.10,27 Additionally, Mirzayan et al 23 found that there was a significant increase in the AHI on standing radiography compared to magnetic resonance imaging (MRI) because of a gravity effect in shoulders with Hamada grades 1 and 2, although this effect was not seen in shoulders with Hamada grades >3. While it is a known fact that AHI reversibility decreases with higher Hamada grades, the reasons behind why certain shoulders in the transitional zone between Hamada grades 1 and 3 exhibit higher AHI reversibility, while others display lower AHI reversibility, are still unknown.
A greater awareness of the factors influencing AHI reversibility in patients with MRCTs provides valuable insights into this complex condition and enhances our decision-making process when considering treatment options. The aim of the current study was to evaluate potential factors affecting AHI reversibility on stress radiography in patients with MRCTs with Hamada grade 2 or 3. We hypothesized that age, time from symptom onset, and critical shoulder angle (CSA) would affect AHI reversibility.
Methods
After receiving approval from our institutional review board, a retrospective review of all shoulder MRI scans performed at our institution between January 2022 and January 2023 was conducted to identify patients with MRCTs. The inclusion criteria were as follows: (1) patients with MRCTs who refused a surgical intervention and underwent nonoperative management, (2) shoulders with tendon retraction located at or medial to the glenoid on coronal-plane MRI, (3) shoulders with an AHI <7 mm in the Grashey view, and (4) the same shoulders having undergone computed tomography (CT) and stress radiography within 1 year. The exclusion criteria were as follows: (1) patients with severe rotator cuff arthropathy categorized as Hamada grades >3; (2) previous surgery on the same shoulder; and (3) presence of a frozen shoulder, glenohumeral arthritis, or inflammatory arthritis. Adhering to the defined criteria, 58 patients met the requirements and were included in the study.
Radiological Evaluation
To achieve standardized radiographic quality, 2 radiology technicians were specifically selected and trained. All radiographs were obtained in the standing position. The AHI measurement involved determining the distance from the undersurface of the acromion to the highest point of the humeral head on true anteroposterior radiography and stress radiography with a 5-kg weight applied to the hands. The distances from the shoulder to the cassette and the x-ray beam were kept uniform to ensure accuracy and reliability. Further, scapular rotation was prevented by stabilizing the scapula between the thorax and cassette, which was confirmed by assessing clavicular orientation. AHI reversibility was calculated as the difference in the AHI between the 2 radiographic techniques (Figure 1). Using the threshold value of 4 mm, patients were categorized into reversible and irreversible AHI groups.
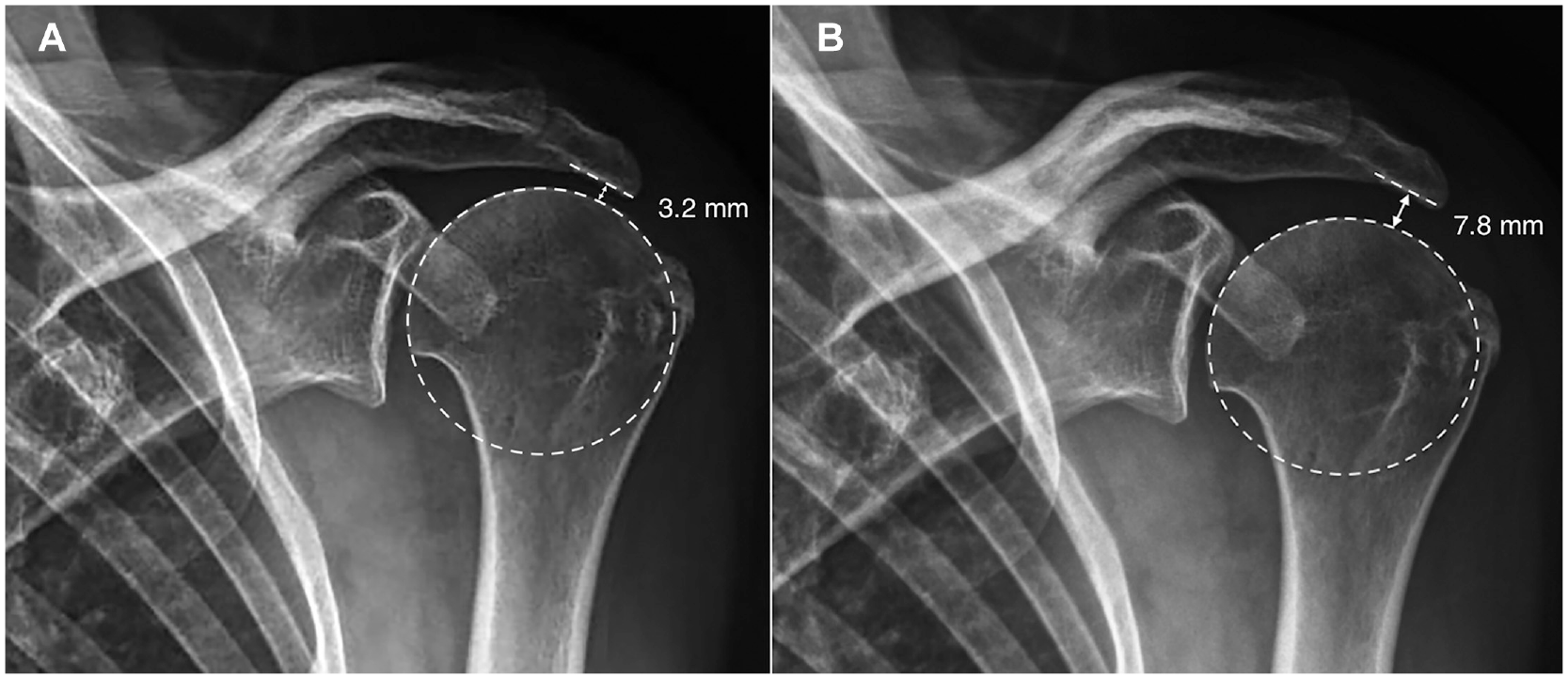
Illustration of acromiohumeral interval (AHI) reversibility on standard anteroposterior radiography. (A) The AHI measured on standard radiography. (B) The AHI measured on stress radiography with a 5-kg weight. The difference in the AHI between standard and stress radiography was used to determine AHI reversibility. Using the threshold value of 4 mm, patients were categorized into reversible and irreversible AHI groups.
All shoulder MRI examinations were performed using a 1.5-T MRI scanner (MAGNETOM Aera; Siemens Healthineers). Shoulder MRI included the following sequences: T1-weighted and fat-saturated T2-weighted sagittal oblique sequences, fat-saturated T2-weighted coronal oblique and axial sequences, and proton density–weighted axial sequences. The MRI scans were evaluated to determine tear size, tear retraction, deltoid cross-sectional area, 9 and grade of fatty degeneration according to the Goutallier classification 6 (Figure 2). Tear size and tear retraction were defined as the maximum defect size on sagittal oblique images and coronal images, respectively. To ensure measurement standardization, shoulder CT scans (Revolution EVO; GE HealthCare) were utilized for accurate and consistent assessments of CSA, acromial index (AI), and glenoid inclination2,4,20 (Figure 3). To assess intraobserver and interobserver reliability, the first author (A.E.O.) repeated the measurements after a minimum interval of 2 weeks, and the results were compared to those of an experienced radiologist (E.G.).

Assessment of (A) tear size, (B) Goutallier grade of rotator cuff muscles, and (C) deltoid cross-sectional area on magnetic resonance imaging.

Morphological evaluation performed via computed tomography (CT) with multiplanar reconstruction slices. (A) The critical shoulder angle (CSA) measurement. (B) The acromial index (AI) measurement. To determine the AI, the glenoacromial distance (GA) was divided by the glenohumeral distance (GH). (C) The glenoid inclination measurement. Glenoid inclination was calculated by subtracting the β-angle from 90°.
The following patient characteristics were recorded using a medical recording database system: age, sex, body mass index, time from symptom onset, and activity level. The activity level of each patient was evaluated based on 4 categories (occupation, preferred sports activities, exercise frequency, and exercise duration) utilizing scoring tables as described earlier, resulting in activity level scores ranging from 4 to 12 points. 16
Statistical Analysis
Statistical analyses were performed using SPSS (Version 22.0; IBM). Descriptive statistics were presented as the mean ± standard deviation. The normality of distributions was assessed using the Shapiro-Wilk test. Univariate analysis to identify variables associated with AHI reversibility was conducted using the chi-square, Fisher exact, and Mann-Whitney U tests. Possible factors identified in univariate analysis were included in multivariate linear regression analysis to determine independent predictors of AHI reversibility. Multicollinearity was assessed using the variance inflation factor, with a value <5 indicating stable regression. Potential variables that were found to be statistically significant were loaded into receiver operating characteristic analysis to evaluate discriminative capacity. A previous study identified a threshold value of 4.0 mm for AHI reversibility to predict achieving a patient acceptable symptom state. 27 Utilizing the threshold value, patients were categorized into reversible and irreversible AHI groups to reveal cutoff values for potential factors. The threshold for acceptable capacity was an area under the curve (AUC) >0.80. Intraclass correlation coefficients >0.8 were considered excellent, while values between 0.5 and 0.8 were considered good. Power analysis indicated that a sample size of 58 was sufficient to detect significant correlations, with an effect size (Cohen d) of 0.6, a type 1 error of 5%, and a power of 80%. P values <.05 were considered statistically significant.
Results
A total of 58 patients (26 male, 32 female) were included in this study. The mean age of the patients was 66.4 ± 8.3 years (range, 51-80 years). The mean time from symptom onset was 4.6 ± 3.5 years (range, 1-10 years). All patients had MRCTs, with superior migration evident on standard standing shoulder radiography. The mean AHI on true anteroposterior radiography was 3.8 ± 2.5 mm (range, 1.1-6.9 mm). The mean AHI difference between standard and stress radiography was 4.2 ± 1.7 mm (range, 0.1-7.8 mm). There were 33 patients classified as having a reversible AHI and 25 patients classified as having an irreversible AHI. Patient and shoulder characteristics based on AHI reversibility are shown in Tables 1 and 2, respectively. The intraobserver and interobserver reliability for the radiological measurements were determined to be good to excellent, with intraclass correlation coefficients ranging between 0.78 and 0.95 (Table 3).
Patient Characteristics a

Data are shown as mean ± SD (range) or n (%).
Shoulder Characteristics a

Data are shown as mean ± SD or No. Values in bold (P < .05) are statistically significant. AHI, acromiohumeral interval.
Intraobserver and Interobserver Reliability a
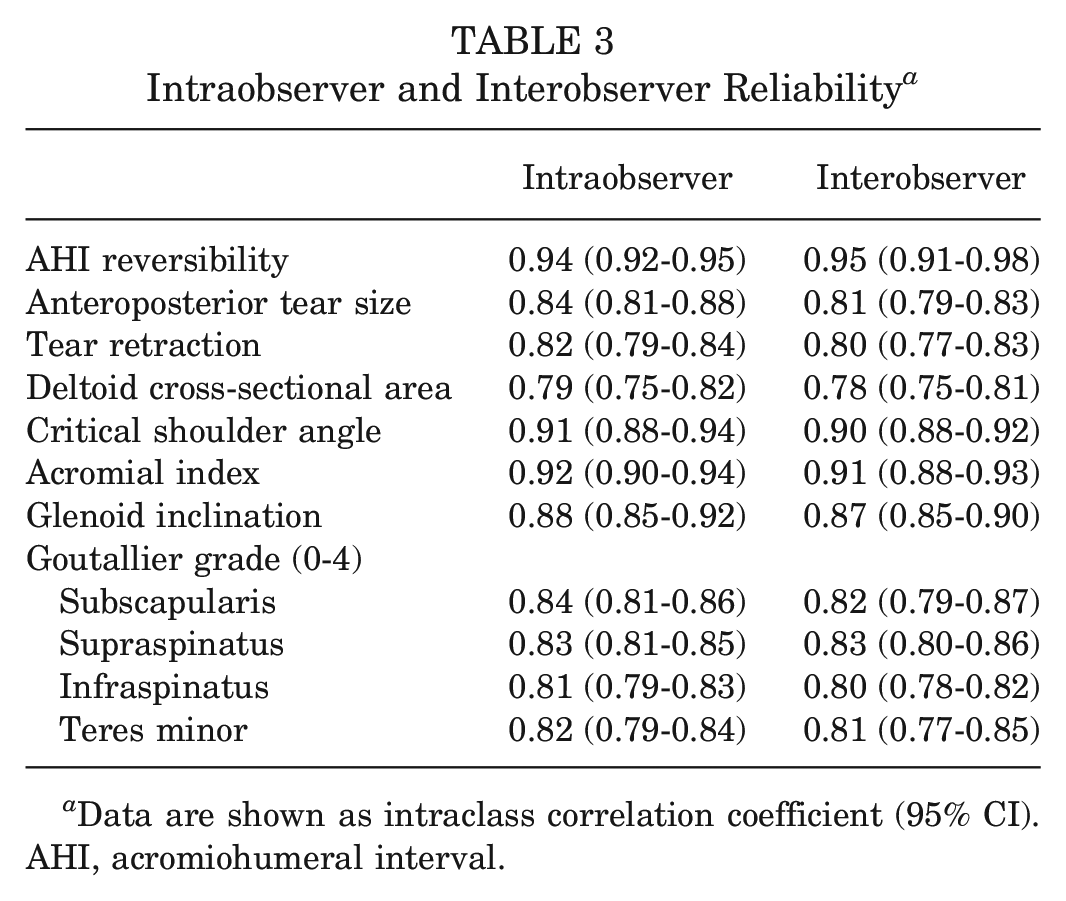
Data are shown as intraclass correlation coefficient (95% CI). AHI, acromiohumeral interval.
Univariate analysis showed that older age (P = .032), a longer time from symptom onset (P = .001), a larger anteroposterior tear size (P = .013), a bigger CSA (P < .001), a greater AI (P = .033), and a higher subscapularis Goutallier grade (P = .041) were all significantly associated with decreased AHI reversibility (Table 4). The aforementioned factors were included in multivariate linear regression analysis to evaluate the combined effects of multiple covariates and to determine the significant influencing factors of AHI reversibility. The AI was excluded in the multivariate regression model because there was multicollinearity between the AI and CSA. Other factors potentially influencing AHI reversibility were included in multivariate regression analysis. Multivariate regression analysis showed that a longer time from symptom onset (β = −0.962 [95% CI, –1.133 to −0.791]) and a bigger CSA (β = −0.184 [95% CI, −0.298 to −0.066]) were significantly associated with decreased AHI reversibility. No significant association was found between AHI reversibility and sex; body mass index; activity level; tear retraction; biceps condition; deltoid cross-sectional area; and Goutallier grade of the supraspinatus, infraspinatus, and teres minor muscles.
Factors Affecting AHI Reversibility a
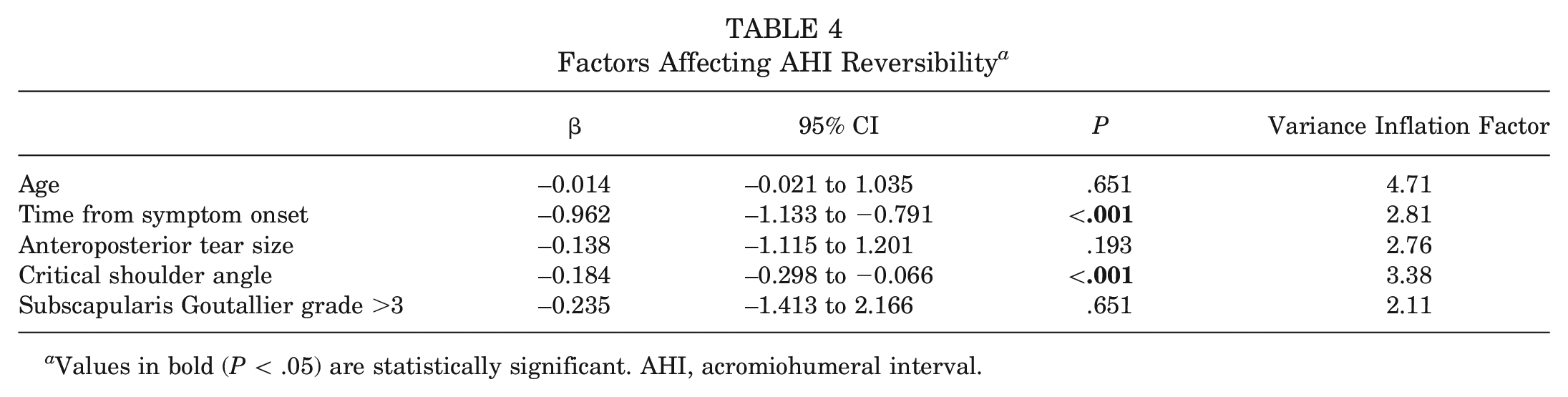
Values in bold (P < .05) are statistically significant. AHI, acromiohumeral interval.
Furthermore, receiver operating characteristic analysis revealed adequate discrimination for time from symptom onset and CSA in predicting AHI reversibility. A time from symptom onset of 5.5 years was determined to be 74% sensitive and 91% specific for AHI reversibility (AUC = 0.93) (Figure 4). A CSA of 38° was determined to be 62% sensitive and 90% specific for AHI reversibility (AUC = 0.84) (Figure 5).
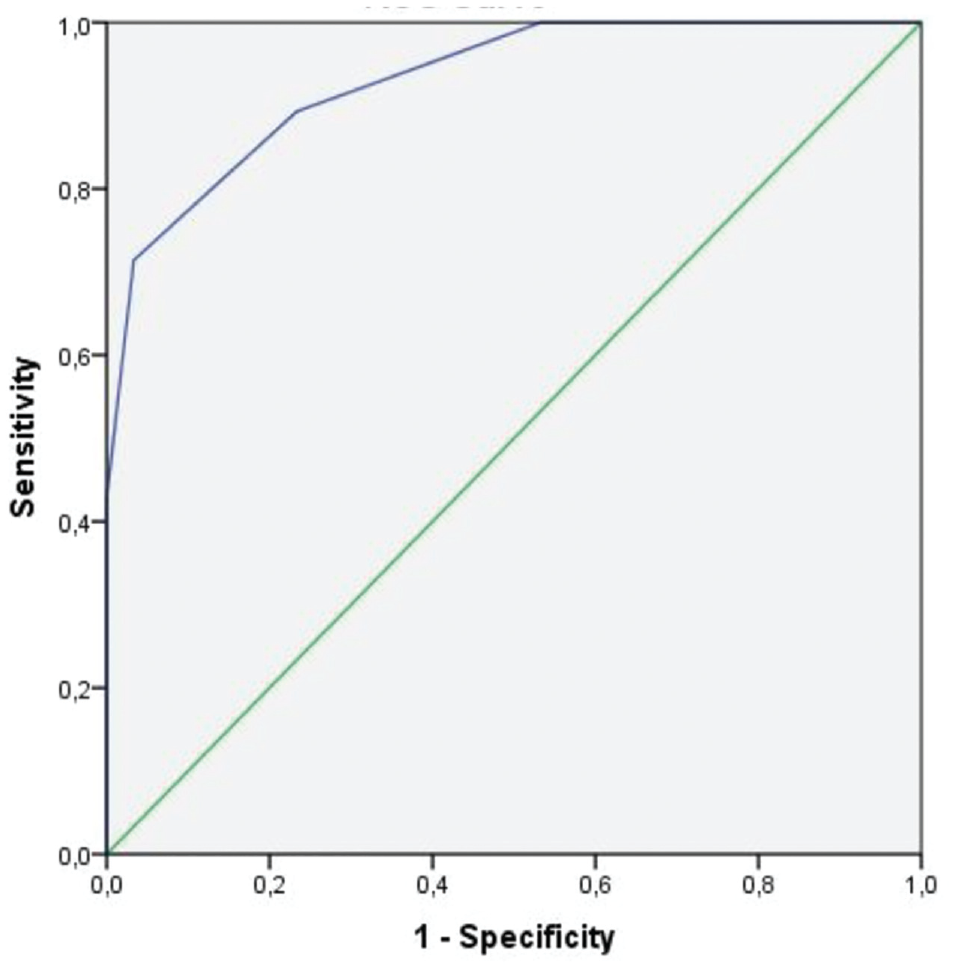
Receiver operating characteristic analysis of time from symptom onset as a predictor of acromiohumeral interval (AHI) reversibility. Area under the curve = 0.93. A time from symptom onset of 5.5 years was 74% sensitive and 91% specific for AHI reversibility.

Receiver operating characteristic analysis of critical shoulder angle (CSA) as a predictor of acromiohumeral interval (AHI) reversibility. Area under the curve = 0.84. A CSA of 38° was 62% sensitive and 90% specific for AHI reversibility.
Discussion
The goal of the present study was to determine whether there were potential factors that affect AHI reversibility in patients with MRCTs. The most important findings of the present study were that AHI reversibility had a significant association with time from symptom onset, indicating that a prolonged duration (>5.5 years) since the initial appearance of symptoms demonstrated less AHI reversibility. Also, CSA had a notable effect on AHI reversibility, indicating that a higher CSA (>38°) corresponded to diminished AHI reversibility.
Superior migration of the humeral head is a well-known prognostic factor that is a consequence of an unbalanced force couple in patients with MRCTs.15,28,30 The goal of both rotator cuff repair and reconstructive procedures is to create a stable fulcrum, rebalancing force couples and improving joint kinematics by a recentered humeral head. 7 Unfortunately, there is a lack of definitive evidence regarding the effectiveness of various surgical options to achieve these biomechanics, thus selecting the most appropriate treatment for each patient is a significant challenge. 17 In this context, AHI reversibility serves as a potential explanation for the varying postoperative outcomes in patients with a smaller preoperative AHI.10,27 In their study, Jeon et al 10 identified a significant association between outcomes after arthroscopic rotator cuff repair of MRCTs and an increase in the AHI >3.2 mm on preoperative stress radiography. Similarly, an inadequate AHI improvement was identified as a predictive factor for the likelihood of retears after superior capsular reconstruction. 19 Therefore, careful attention should be paid to AHI reversibility in addition to the static AHI when making decisions related to treatment options.
The findings of the present study showed that the time from symptom onset was an independent predictive factor of AHI reversibility. Several studies have examined the natural history of rotator cuff tears and found that approximately 50% of such tears worsen over a 4-year period.14,24,26 Moosmayer et al 24 reported that for patients who underwent nonoperative treatment, over a 9-year period, outcomes generally remained satisfactory, but there existed a risk of symptom recurrence and a deterioration in anatomic factors. Furthermore, Jeong et al 11 highlighted that the occurrence of postoperative osteoarthritis progression was higher among patients in the retear group, regardless of improvements in the functional status after rotator cuff repair. Consistent with these data, our study showed that the time from symptom onset was negatively correlated with AHI reversibility, irrespective of the long-term functional status. One plausible explanation is that with an extended time from symptom onset, the progression of the degenerative process of rotator cuff arthropathy and the unopposed upward pull of the deltoid muscle led to superior migration of the humeral head, which became increasingly irreversible.
Another relevant finding of the current study is the significant effect of the CSA on AHI reversibility. There has been an ongoing debate regarding the effect of the CSA on rotator cuff tears. 22 While various studies have shown an association between a CSA >35° and an increased risk of rotator cuff disease, some have reported that the CSA is unlikely to be related to rotator cuff tears.1,29 Biomechanically, an increase in the CSA leads to a more vertical deltoid muscle vector that forces the humeral head to migrate superiorly, resulting in a greater load on the superior rotator cuff tendons.28,29 The ongoing CSA controversy may be linked to challenges in obtaining precise measurements, caused by positioning errors on true anteroposterior radiography and the considerable variability in 3-dimensional scapular morphology due to scapular rotation. 33 The use of CT with multiplanar reconstruction slices in the current study aimed to ensure more accurate CSA measurements. 20 Nevertheless, CT is unnecessary if accurate radiographs are obtained. However, inferences should not be drawn from measurements taken on incorrect images. Our findings revealed that the CSA was negatively correlated with AHI reversibility.
The variability in AHI reversibility among shoulders in the transitional zone between Hamada grades 2 and 3 serves as a reminder that rotator cuff arthropathy is a complex and long-term process. The association between tear progression and symptom presentation may not always be reliable, as patients adapt to structural changes over time. 18 Also, it has been reported that the severity of radiographic findings may not relate to symptoms in glenohumeral arthritis. 12 Similarly, it can be also suggested that there is no correlation between tear progression and arthropathy progression. It seems more reasonable that AHI reversibility is associated with the progression of arthropathy rather than tear progression. Age, sex, tear size, and grade of fatty infiltration are all considered as potential factors that influence tear progression.21,32 Our study’s results indicated that time from symptom onset and CSA played more significant roles in AHI reversibility and therefore in arthropathy progression.
AHI reversibility also holds substantial importance in the decision-making process for the surgical treatment of younger patients with Hamada grades 2 and 3 rotator cuff arthropathy. The optimal treatment choice remains a controversy in this group of patients, and AHI reversibility may serve as a threshold in determining whether to prefer soft tissue or prosthetic reconstructive procedures. Despite several review articles analyzing the outcomes of these treatment options, a definitive superior technique has not been conclusively identified.3,17 The consensus among shoulder surgeons is that superior capsular reconstruction is contraindicated and not considered a viable option for patients older than 70 years with pseudoparesis and an irreparable subscapularis tear. 31 The results of the current study emphasize that lower AHI reversibility, a long time from symptom onset (>5.5 years), and an increased CSA (>38°) are potential factors that can negatively affect final outcomes after soft tissue reconstructive procedures.
Limitations
Several limitations were encountered in the present study, notably its retrospective nature and the relatively small sample size, possibly leading to some results being underrepresented. Also, this study was particularly focused on radiological examinations and did not address the prognosis of rotator cuff tears or explore potential treatment options. Although good to excellent interobserver reliability and intraobserver reliability were demonstrated for all measurements, it is important to recognize that scapular rotation inevitably occurs on stress radiography, therefore having an impact on the AHI. A patient’s muscle weakness or overall fitness may also impact AHI reversibility. These findings have practical implications, suggesting the potential use of a preoperative radiological parameter for predicting clinical outcomes. Further confirmation of AHI reversibility’s predictive role might be obtained through a future prospective randomized controlled study.
Conclusion
Time from symptom onset (>5.5 years) and CSA (>38°) were significant independent factors of AHI reversibility. These factors should be considered for the decision-making process in patients with MRCTs.
Footnotes
Final revision submitted June 22, 2024; accepted July 3, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Samsun University (SUKAEK-2023 5/23).