
Abstract
Background:
Treatment of patients with anterior cruciate ligament (ACL) injuries is often complicated by secondary damage to the meniscus and cartilage.
Purpose:
To assess the association between time from ACL tear to ACL reconstruction (ACLR) and the presence of intra-articular injuries at the time of ACLR, including meniscal tears, irreparable meniscal tears, chondral damage, and knee compartment degenerative changes.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Consecutive patients undergoing primary ACLR performed by a single surgeon in a Canadian health system over a 5.5-year period were included. Age at ACLR, activity level prior to injury, time from injury to ACLR (TFI), presence and degree of radiographic osteoarthritic features (International Knee Documentation Committee [IKDC] score by tibiofemoral and/or patellofemoral compartment), and surgeon-recorded meniscal lesions (presence and treatment [repair or excision]) and chondral lesions (International Cartilage Repair Society [ICRS] scale grade >2) at time of ACLR were extracted from medical records. The association between TFI (in quartiles: first quartile [0-36 wk] through fourth quartile [110-1000 wk]) and each outcome was assessed with multivariable logistic regression adjusted for age at ACLR and activity level.
Results:
A total of 860 individual patient records were included. The median patient age was 27.0 years (range, 12-63 years), 47.5% were female (403/849), and 47.2% were classified as playing competitive or professional sports versus recreational sport (337/714). After adjustment for age and activity level, TFI was associated with presence of medial meniscal tear (odds ratio [OR] of fourth-quartile vs first-quartile patients, 3.86; 95% CI, 2.38-6.24; P < .001), medial meniscal tear requiring greater than two-thirds meniscectomy (OR, 5.64; 95% CI, 2.99-10.67; P < .001), medial femoral condyle chondral damage (OR, 3.42; 95% CI, 1.96-5.95; P < .001), and medial tibiofemoral radiographic osteoarthritic features (OR, 22.03; 95% CI, 5.17-93.86; P < .001). TFI was not associated with adverse outcomes in the lateral tibiofemoral or patellofemoral compartments.
Conclusion:
Increases in TFI are associated with medial meniscal tears, including irreparable medial meniscal tears, medial femoral condyle chondral damage, and early medial tibiofemoral compartment degenerative changes at time of ACLR. These findings highlight the importance of establishing a timely diagnosis and implementing an appropriate treatment plan for patients with ACL injuries. This approach may prevent further instability episodes that place patients at risk of sustaining additional intra-articular injuries in the affected knee. Further research is required to understand the implications of TFI and to determine whether decreasing the TFI alters the natural history after an ACL injury.
The anterior cruciate ligament (ACL) is the primary restraint to anterior tibial translation and provides crucial rotatory control for the knee. 23 It is subject to injury, especially in sports that require cutting and jumping. 2 Injury to the ACL is common, with an age- and sex-adjusted incidence of 68.6 per 100,000 person-years. 18
The implications of a complete ACL tear are significant. It often represents a life-changing event for the individual who sustains the injury. ACL deficiency may lead to recurrent instability episodes, which can cause subsequent and severe secondary injury to the menisci and cartilage. 4,19 ACL injury predisposes a person to radiographic signs of osteoarthritis (OA), with a 10- to 20-year incidence after injury of up to 50%. 15,19 Furthermore, the likelihood that symptomatic OA will require total knee replacement is as much as 5 times higher in ACL-injured knees than uninjured knees. 19,21 Although it is unclear whether ACL reconstruction (ACLR) changes a patient’s likelihood of developing OA, 1 it is clear that the risk of developing OA after ACL injury is increased significantly in the presence of secondary meniscal and cartilage damage, some of which may be preventable. 15,19 The medial meniscus is a secondary restraint to anterior tibial translation and is at risk in the setting of ACL deficiency. 16 The natural history of an unstable, ACL-deficient knee is medial meniscal damage and medial compartment OA. 15 Where possible, and when addressed early enough, meniscal tears are repaired; unfortunately, many tears are not amenable to repair, and the only surgical treatment appropriate for these cases is removal of the torn fragment of meniscus (partial meniscectomy). 16
Early and appropriate care for the patient with ACL injury is critical for optimal outcomes. Treatment (whether surgical or not) should be focused on the prevention of further instability episodes that place the meniscus and cartilage at risk, and it may involve recommendations for activity modification and lifestyle change. 17,20 The surgical treatment, ACLR, is designed to restore rotatory stability by reconstructing an “anatomic” ACL. 23 ACLR is indicated in individuals with ACL injury who have functional instability with activities of daily living or in individuals who wish to return to sports that require rotational stability (ie, cutting sports such as soccer, football, and basketball). 23 The ACL clinical practice guidelines of the American Academy of Orthopaedic Surgeons (AAOS) recommend that when ACLR is indicated, it should be performed within 5 months of the initial injury to protect the meniscus and cartilage. 20
The purpose of this study was to assess the association between time from ACL tear to ACLR and the presence at the time of reconstruction of meniscal tears, irreparable meniscal tears requiring meniscectomy, chondral damage, and knee compartment radiographic features of OA. It was hypothesized that an increase in time from injury to ACLR (TFI) would be associated with increased odds of irreparable medial meniscal tears as evidenced by the increased number of medial meniscectomies involving greater than two-thirds of the meniscus.
Methods
Ethical approval for this retrospective chart review was obtained from a local ethics review board.
Data Sources
Anonymized data were accessed from the International Knee Documentation Committee (IKDC) surgical documentation forms of all patients who underwent ACLR by the senior author (D.O.) between December 1, 2010, and May 30, 2016. All clinical and radiological assessments were performed by the senior author. Records were kept as part of the patients’ medical charts, which were held in the possession of the senior author. Patients who underwent revision ACLR were excluded.
Data Extraction
TFI (in weeks) recorded on the day of ACLR was extracted from each IKDC form. Age was extracted from the IKDC form as it had been recorded on the day of each surgery. Activity level, defined by the senior author as recreational (not a member of an organized team), competitive (a member of an organized team), or professional, was similarly extracted as it had been recorded.
Data on secondary damage, including presence of meniscal tear, irreparable meniscal tear requiring greater than two-thirds excision, chondral damage (according to the International Cartilage Repair Society [ICRS] criteria), and radiographic signs of OA (IKDC grade), were extracted from the standardized IKDC scoring form that had been completed at the time of surgery. All data were recorded in a Microsoft Excel spreadsheet. Missing data points were occupied with a placeholder.
Data Analyses
Multivariable logistic regression including age at ACLR and activity level was performed through use of Stata (version 13; StataCorp LP) to assess the association between TFI and presence of meniscal tear, irreparable meniscal tear requiring meniscectomy, chondral damage (ICRS grade ≥2), and radiographic OA (IKDC grade “mild” or higher). Because TFI is a continuous variable, data were analyzed according to quartiles, which were established by defining cut points at the 25th, 50th, and 75th percentiles. As many patients around these cut points had the same TFI in weeks, the number of patients in each quartile were not equal in size. The association between TFI and index variables was described with odds ratios (ORs) and 95% CIs. For each regression model, a Wald test was used to confirm whether TFI (broken into quartiles) was associated with each outcome. A power analysis revealed that to detect a difference in meniscal tear proportions of 0.25 and 0.45 between 2 groups, with power of 0.80 and alpha .05, the required sample size was 92. 3
Results
A total of 876 primary ACLR patients were identified. Sixteen patients did not have TFI recorded and were excluded, leaving 860 patients for inclusion in the analysis. Twelve did not have age recorded, 11 did not have sex recorded, and 146 did not have level of play recorded (on the IKDC form). All other data were complete.
Demographics, including age at ACLR and activity level stratified by TFI quartiles, are summarized in Table 1. Overall, the median age of participants was 27.0 years (range, 12-63 years), 47.5% were female (403/849), and 47.2% were classified as playing competitive or professional sports versus recreational sport (337/714).
Distribution of Demographics by Quartiles a
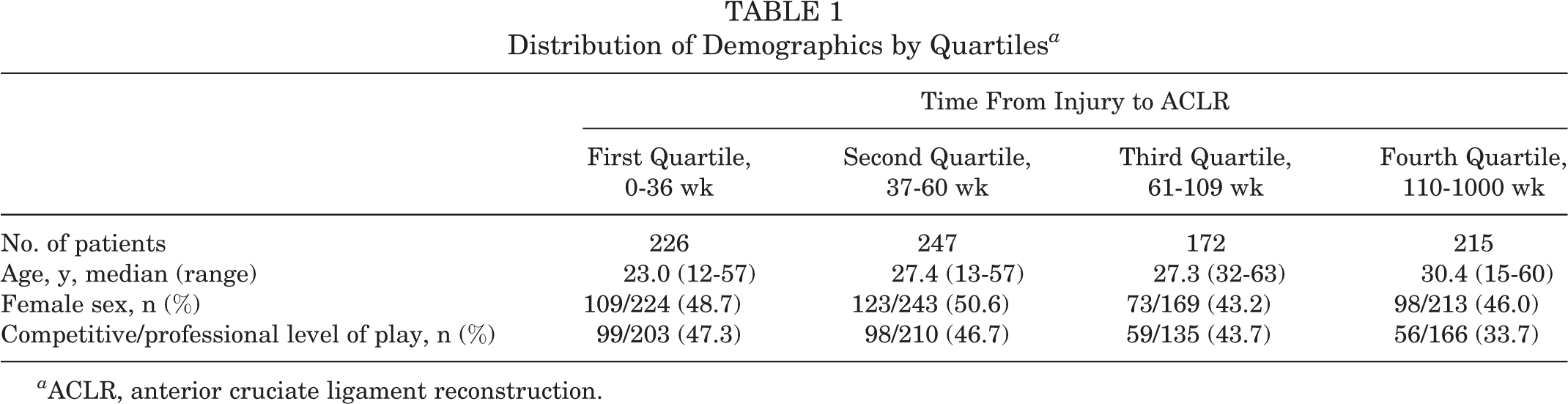
a ACLR, anterior cruciate ligament reconstruction.
At the time of ACL reconstruction, 76.6% (659/860) of patients had a meniscal tear (58.1% medial [500/860], 46.9% lateral [403/860], 28.4% both [244/860]). The proportion of patients with meniscal injury increased with increased TFI (Table 2).
Prevalence of Meniscal Tears by Quartiles a

a Values are expressed as % (n).
Partial medial meniscectomy involving greater than two-thirds of the meniscus was performed in 16.7% of all patients (144/860), or 28.8% of all patients with medial meniscal tears (144/500). The proportion of patients requiring partial meniscectomy increased with increased TFI. Medial meniscal repair was performed in 12.6% of all patients (108/860), or 21.6% of all patients with medial meniscal tears (108/500). Lateral meniscectomy involving greater than two-thirds of the meniscus was performed in 3.3% of all patients (31/860), or 7.7% of all patients with lateral meniscal tears (31/403). Lateral meniscal repair was performed in 0.93% of all patients (8/860), or 2.0% of all patients with lateral meniscal tears (8/403) (Table 3).
Summary of Meniscal Treatment by Quartiles a
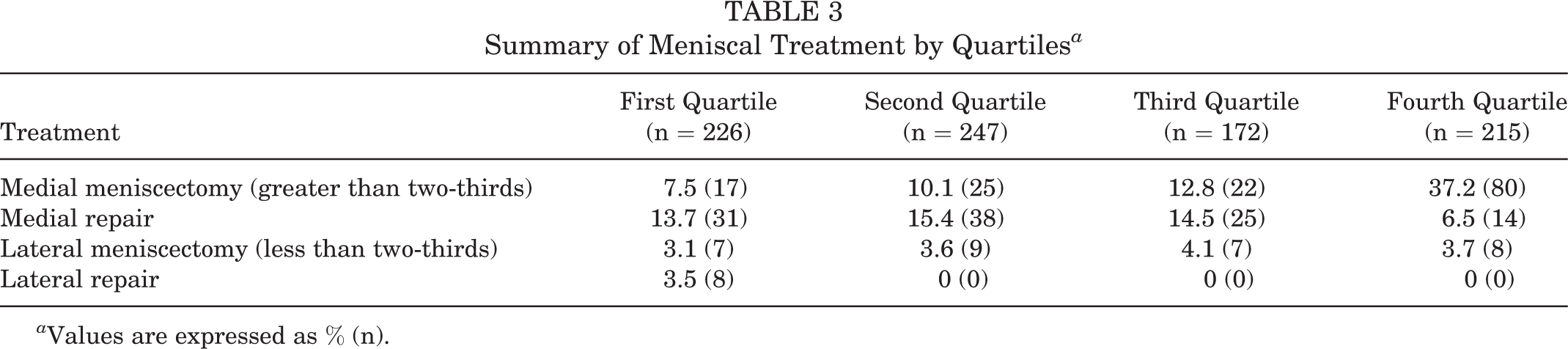
a Values are expressed as % (n).
Chondral damage of at least ICRS grade 2 was observed on the medial femoral condyle in 21.9% of all patients (188/860), on the lateral femoral condyle in 6.2% (53/860), on the tibia in 2.1% (medial tibial plateau, 8/860; lateral tibial plateau, 10/860), and in the patellofemoral compartment in less than 1.6% (14/860). The proportion of patients with medial chondral damage increased with increased TFI (Table 4).
Summary of Chondral Damage by Quartiles a

a Values are expressed as % (n).
Radiographic OA of at least an IKDC mild category was identified in the medial compartment in 10.2% of patients (88/860), in the lateral compartment in 3.5% (30/860), and in the patellofemoral compartment in 0.81% (7/860). The proportion of patients with OA changes increased with increased TFI (Table 5).
Summary of Radiographic Changes by Quartiles a

a Values are expressed as % (n).
After adjustment for age and activity level, TFI was significantly associated with the presence of a medial meniscal tear (OR of fourth-quartile vs first-quartile patients, 3.86; 95% CI, 2.38-6.24; P < .001), medial meniscal tear requiring greater than two-thirds meniscectomy (OR, 5.64; 95% CI, 2.99-10.67; P < .001), medial femoral condyle chondral damage (OR, 3.42; 95% CI, 1.96-5.95; P < .001), and medial tibiofemoral radiographic osteoarthritic features (OR, 22.03; 95% CI, 5.17-93.86; P < .001). The association of TFI (broken down into quartiles) and outcome was confirmed in each model through use of the Wald test (P < .0001 for each). After adjustment for age and level of play, no association was identified between TFI and likelihood of meniscal repair or development of meniscal or cartilage damage or radiographic OA of the lateral or patellofemoral compartments.
Alternatively, these data may be expressed as an OR per week of TFI. After adjustment for age and level of play, each week of TFI was associated with presence of medial meniscal tear (OR, 1.0059; 95% CI, 1.0040-1.0079; P < .001), medial meniscal tear requiring greater than two-thirds meniscectomy (OR, 1.0039; 95% CI, 1.0025-1.0053; P < .001), medial femoral condyle chondral damage (OR, 1.0031; 95% CI, 1.0017-1.0045; P < .001), and radiographic OA (IKDC grade of “mild” or higher) of the medial compartment (OR, 1.0048; 95% CI, 1.0033-1.0064; P < .001) (Table 6).
Summary of Statistically Significant Findings a

a IKDC, International Knee Documentation Committee; TFI, time from injury to anterior cruciate ligament reconstruction.
Discussion
The results of this study demonstrate that increases in TFI have a significant association with the presence of additional abnormalities in the medial compartment of the knee at the time of ACLR, such as medial meniscal tears (including irreparable medial meniscal tears requiring greater than two-thirds meniscectomy), medial femoral condyle cartilage damage, and radiographic findings consistent with early OA. Increases in TFI were not associated with any increase in the rate of additional abnormalities in the lateral or patellofemoral compartments of the knee.
These results are consistent with the findings of prior studies demonstrating that delayed ACLR is associated with an increase in the incidence of intra-articular abnormalities including meniscal tears and cartilage damage at the time of surgery compared with early surgery. 6,7,9 –14,16 Although several previous studies have investigated the relationship between the timing of ACLR and the presence of intra-articular abnormality at the time of surgery, it is difficult to draw conclusions with regard to the acceptable upper limit for TFI for several reasons: The definition of early versus late surgery varies widely in the literature (between 4 and 52 weeks), 7,10 the outcome measures used to quantify intra-articular abnormality are not standardized, and many of these studies are small retrospective reviews.
In the current literature, several studies have reached the consensus that patients waiting longer than 12 months have a higher incidence of cartilage and meniscal damage. 6,7,9,11,12 The earliest time point that has been shown to be associated with a statistically significant increase in intra-articular injury is 3 months. 16 In the current study, the first quartile of patients included those whose TFI was as high as 36 weeks (9 months).
In addition to the increase in the absolute number of medial meniscal tears, increased TFI is associated with more irreparable tears as evidenced by increased rates of greater than two-thirds medial meniscectomy. This suggests that increased TFI decreases the likelihood that meniscal tears will be repairable at the time of surgery. In our patient population, each 10-week increase in TFI was associated with a 6% increase in the odds of having a medial meniscal tear at the time of ACLR, a 4% increase in the odds of having an irreparable tear requiring greater than two-thirds meniscectomy, a 3% increase in medial femoral articular cartilage damage, and a 5% increase in radiographic OA. Having said that, we found only modest increases in associated abnormality over the first 3 quartiles and a much larger increase in associated abnormality in the fourth quartile (>2 years). These findings are largely in keeping with prior studies that have demonstrated increased rates of meniscectomy with increasing TFI in populations of patients undergoing ACLR. Krutsch et al 14 found that meniscal repair was possible in 77.2% patients treated within 6 months of injury versus 46.7% of those treated after 6 months (P = .022). Similarly, Kluczynski et al 13 observed fewer meniscectomies in patients with a TFI of less than 6 weeks (OR, 0.48; 95% CI, 0.24-0.97).
The findings of the current study support the position that with recurrent instability episodes, the medial meniscus is at greater risk of injury than the lateral meniscus. 22 This observation was initially described by Cipolla et al, 8 who showed that medial meniscal damage was more common in a chronic ACL-deficient knee and lateral meniscal damage was more common in an acutely ACL-injured knee.
Our patient cohort showed a significant discrepancy in TFI based on patient age and activity level. Athletes considered competitive or professional had significantly lower TFIs compared with recreational athletes. Likewise, younger patients had lower TFIs. Overall, our study allowed limited ability to comment on the factors contributing to differences in TFI. These limitations exist for several reasons. The retrospective nature of our patient database allowed for analysis based on limited patient demographic information, and other significant patient factors that influenced TFI may not have been captured. Furthermore, the designation of activity level was subjective, and the age and activity level of patients may be confounding variables. The factors contributing to increased TFI warrant further investigation because of the significant irreversible pathological changes in the knee that are associated with increased TFI. This may prove to be a difficult area to study because not all patients with ACL injury require ACLR. Depending on factors such as patient age, activity level, goals, and preferences, many patients can be successfully managed with activity modification, lifestyle change, and rehabilitation with the aim of avoiding further injury to the knee. 17,20 Although some patients will cope with an ACL-deficient knee, many patients will have recurrent instability episodes. It remains a challenge for clinicians to accurately determine which patients are likely to cope with their injury. By the time nonoperative treatment has failed in a given patient, irreversible damage to his or her knee may have already occurred. One must balance the potential for irreversible damage with the risk of performing ACLR in patients who may never require it. Other factors that may contribute to increased TFI include delays in diagnosis, wait times for diagnostic testing, and specialist referral, although these delays will differ based on region and are likely less problematic in competitive private health care systems.
TFI may serve as a surrogate for other factors that influence the incidence of additional intra-articular abnormality at the time of ACLR. For example, the number of repeated instability episodes after the initial injury may be just as important as the TFI. 22 Kluczynski et al 13 found that the number of patient-reported instability episodes (that were consistent with a pivot-shift mechanism) correlated with the incidence of medial meniscal tears after adjusting for TFI. Specifically, greater than 10 episodes doubled the likelihood of requiring a medial meniscectomy. 13 After asking patients whether they had experienced a reinjury prior to ACLR, Chen et al 5 used a logistic regression analysis to demonstrate that having a repeat injury was associated with an increased incidence of meniscal and cartilage damage diagnosed at the time of surgery. Even though TFI may be a surrogate measure, it is more objective than asking patients to recall instability episodes, which may be prone to recall bias; further, patients may find it difficult to differentiate between instability episodes versus occasions when the knee feels as though it gives out due to quadriceps weakness without a pivot-shift mechanism. For these reasons, TFI is a more easily studied metric. Additionally, TFI is a potentially modifiable factor, and evidence that supports the benefit of decreased TFI can be used to promote expedited ACL surgery in resource-limited health care systems.
The findings of this study confirm the importance of the relationship between TFI and the presence of additional intra-articular abnormality in the medial compartment of the knee at the time of ACLR surgery. Although not confirmed by prospective studies, current available evidence supports performing ACLR in a timely manner when it is indicated. The AAOS recommends 5 months as the maximum acceptable limit for TFI; however, evidence shows that additional benefits may be gained below this threshold.
16,20
Based on these findings, the following recommendations can be made: Prospective studies are necessary to confirm that interventions aimed at lowering TFI and preventing subsequent instability episodes reduce the incidence of intra-articular abnormality at the time of surgery. Practitioners should establish the TFI of their patient population, as this may vary on a regional basis. Practitioners should establish and monitor TFI targets. The AAOS guideline of 5 months represents a reasonable target for time to ACLR; however, there may be benefits to adopting a lower threshold. Reasonable efforts should be made to reduce TFI by identifying and mitigating any factors that impede expedient treatment of patients with ACL injuries.
Strengths and Limitations
This study included a large cohort of patients from a single surgeon in a single-payer health care system, and the data were recorded at the time of surgery. Data were uniformly collected by a single experienced surgeon using reliable criteria to quantify the severity of associated injuries and the nature of treatment required. TFI was calculated in weeks, and we used a multivariate regression analysis rather than using arbitrary time points to define early versus delayed treatment. We believe these findings are generalizable to other patient populations where limited resources necessitate longer surgical wait times. Study weaknesses include the retrospective nature of the data retrieval, the bias toward earlier surgery in younger and competitive athletes, the inherent inaccuracy of determining greater than two-thirds meniscectomy, and the lack of outcome data.
Conclusion
Increased TFI was associated with the presence of irreparable medial meniscal tears, medial femoral condyle chondral damage, and early medial knee compartment degenerative changes at the time of surgery. These findings highlight the importance of establishing a timely diagnosis and implementing an appropriate treatment plan for patients with ACL injury. These steps may prevent further instability episodes that place patients at risk of sustaining additional intra-articular injuries in the affected knee. Further research is required to understand the implications of TFI and determine whether decreasing the TFI alters the natural history after an ACL injury.
Footnotes
Acknowledgment
The authors thank Ambikaipakan (Sentil) Senthilselvan, PhD, School of Public Health, University of Alberta, for his assistance with statistical analysis.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Alberta (Pro00064295).