
Abstract
Focal chondral defects of the articular surface are a common occurrence in the field of orthopaedics. These isolated cartilage injuries, if not repaired surgically with restoration of articular congruency, may have a high rate of progression to posttraumatic osteoarthritis, resulting in significant morbidity and loss of function in the young, active patient. Both isolated and global joint disease are a difficult entity to treat in the clinical setting given the high amount of stress on weightbearing joints and the limited healing potential of native articular cartilage. Recently, clinical interest has focused on the use of biologically active compounds and surgical techniques to regenerate native cartilage to the articular surface, with the goal of restoring normal joint health and overall function. This article presents a review of the current biologic therapies, as discussed at the 2015 American Orthopaedic Society for Sports Medicine (AOSSM) Biologics Think Tank, that are used in the treatment of focal cartilage deficiencies. For each of these emerging therapies, the theories for application, the present clinical evidence, and specific areas for future research are explored, with focus on the barriers currently faced by clinicians in advancing the success of these therapies in the clinical setting.
Focal articular cartilage defects greater than 1.5 cm in diameter, if left untreated, may eventually progress to osteoarthritis (OA). OA represents a progressive decline in the articular surface of weightbearing joints. An arthritic joint can be the end result of chronic “wear and tear” injury characterized by repetitive use or as a result of a traumatic injury. Both mechanisms are initiated by focal, sometimes diffuse, areas of cartilage injury and degeneration, which propagates joint destruction through inflammatory mechanisms. Cartilage injuries are common, affecting 27 million people in the United States according to data from 2005. 56 Of people aged 18 to 44 years, 7.3% report diagnosed arthritis; in those 45 to 64 years, 30.3% report diagnosed arthritis; and in persons aged 65 years or older, 49.7% report diagnosed arthritis. This statistic highlights that with an increasing proportion of older patients seeking medical care for joint pathology, a need for early detection of cartilage defects and novel repair strategies has never been more important in preventing morbidity and maintaining mobility of the aging population. The unique structure of articular cartilage and the osteochondral unit has proven difficult for creating an optimal biologic agent to reverse the progressive nature of articular destruction as well as function to repair isolated cartilage defects. It is well understood that articular cartilage grows and maintains without blood vessels or innervation and most importantly, with a limited capacity for healing and repair after injury. 32 Chondrocytes have a limited potential for replication or migration to a site of injury, mainly due to their role in preserving a local microenvironment of extracellular matrix of collagens, proteins, lipids, and water. Therefore, the successful treatment of articular injury with biologic therapies must be highly effective in replicating the anatomic architecture of the joint surface and must be able to inherently withstand or otherwise restore resiliency of the cartilage to biomechanical forces. The biologic therapies currently available for use have widespread but variable evidence to support their clinical use at present. The current organization and treatment indications of these techniques is based on the size and location of the cartilage lesion as well as functional demands of the patient receiving treatment. 15
Stimulation and Modification of the Native Articular Chondrocytes
Despite the biomechanical stresses placed on the articular surface, there is limited potential for regrowth or repair of full-thickness cartilage defects. Biologic stimulation using cytokines and growth factors is a promising area to enhance the articular surface’s inherent ability to survive and repopulate. Through paracrine signaling cascades, enhancement of the genetic expression of chondrocytes, or stimulation and recruitment of mesenchymal stem cells that may gain access to the joint in time of acute injury, and small biological compounds or procedures with an intra-articular site of action are an exciting target for cartilage repair and regeneration.
A technique solely focused on cellular recruitment—microfracture surgery without additional biologic augmentation—is used mainly for the treatment of small lesions (<2 to 4 cm2). 35 In comparison with osteochondral autograft transfer (OAT) procedures, microfracture demonstrates similar clinical outcomes at intermediate-term follow-up. However, it is important to note that OAT patients have been reported in a retrospective study to maintain a superior level of athletic activity compared with those treated with microfracture. 55 The addition of combination growth factor substrates, such as bone marrow aspirate, have been shown by Fortier et al 31 to significantly improve the ability of microfracture to heal full-thickness defects in an animal model. Also, recent studies into the biologic mediators of the fibrotic, non–type II collagenous response generated by microfracture and acute joint trauma has shown 2 molecules (lysophosphatidic acid [LPA] and autotaxin [ATX]) that are involved in the feedback toward collagen type I (COL1) or collagen type II (COL2) production. Small molecule inhibitors significantly reduced the quantity of COL1-enriched fibrocartilage products with a concomitant increase in COL2 associated with the healthy cartilage state. 90 Therefore, further study into the cascade of ineffective fibrotic cartilage therapy and the role of widespread growth factor induction to migrating progenitor cells may increase the indications for and the quality of microfracture surgery.
With regard to the addition of growth factors, the most thoroughly investigated compounds are transforming growth factor–β1 (TGFβ1), bone morphogenetic protein (BMP7), and insulin-like growth factor-1 (IGF1). 29 TGFβ1, BMP7, and IGF1 have all been shown in in vitro studies to increase chondrocyte synthetic activity and enhance matrix deposition while decreasing the catabolic activity of interleukin-1 (IL1), a widespread inflammatory cytokine implicated in the progressive destruction of an osteoarthritic joint. 8,24 Other compounds in the TGFβ family have demonstrated potential with in vitro study. 82 However, TGFβ1 has been implicated in these same studies for the stimulation of synovium, development of fibrosis, and the induction of osteophyte formation, and therefore is not a presently viable therapy for intra-articular use. At this time, BMP7 has emerged as an ideal factor for the regeneration of articular cartilage due to its anabolic yet anti-inflammatory effect, its function independent of chondrocyte age or OA, and its ability to function synergistically with other factors such as IGF1. 13,24,58 In addition, there have been several growth factors studied independently and in combination with other factors (ie, BMP7 and IGF1). 29 Chondrogenesis is known to be regulated during development by multiple growth signals that exhibit synergistic, anticatabolic, and paracrine components. This developmental paradigm has been described as the blueprint for the engineering of chondrocytes from pluripotent cells and is therefore of great importance. 89 The presence of multiple growth factors interacting in specific concentrations and gradients within the active region of cartilage during development has turned the focus for therapies to autologous, mixed biologics that are known to contain a combination of growth factors, such as platelet-rich plasma (PRP).
PRP is an autologous, highly concentrated product containing both growth factors and inflammatory mediators. Review of the literature shows a widely documented ability to enhance chondrocyte proliferation 80,91 while its effects on the differentiation and productivity of chondrocytes has been less consistently documented. Certain studies have demonstrated increased cell proliferation, upregulation, and increased synthesis of proteoglycan and COL2 effective in establishing matrix formation. 9,30,57,64 Other authors have argued that PRP is unable to induce a deposition of matrix components with no difference in extracellular matrix (ECM) formation observed when compared with other platelet and whole blood partitions. 23,45 This has significant implications for ability to restore and produce a resilient articular surface. The inconsistency in reports may be attributable to several known factors. The studies aforementioned were performed in different cell types with varying study designs, and it has been well documented that significant differences in platelet and leukocyte concentration and growth factor composition between PRP preparations exist and can result in significant physiologic differences when studied. 4,11,52,63 In one such study, leukocyte- and platelet-rich plasma (L-PRP), a preparation with higher platelet concentration and leukocytes, significantly elevated pro-inflammatory cytokines and inhibited anticatabolic substrates when compared with pure PRP (P-PRP), a lower concentration pure platelet preparation. 4 An in vitro study developed by Cavallo et al 11 for the comparison of different PRP formulations demonstrated that L-PRP and P-PRP induce distinctly different genetic effects on chondrocytes due to different concentrations of platelets, leukocytes, growth factors, and other bioactive molecules. The specific concentration of active elements within PRP and how they affect the knee articular surface is a controversial topic. Comparisons of therapeutic effect with single- versus double-spinning techniques show that double-spin techniques tend to generate pain and swelling, with similar and significant clinical improvement observed with both therapies. 27 Therefore, double-spinning may concentrate factors to a level that serves as locally proinflammatory. More research into the optimal preparation technique for an ideal PRP formulation is needed. When reported in the literature, the findings of a particular study must discuss the process of production and characterize the composition of biologic compound to aid in the standardization and reproducibility of results. 67 Recent high-level evidence has compared PRP injections with placebo (saline) and PRP with intra-articular hyaluronic acid (HA) injection. In the former, with 156 knees randomized to P-PRP versus a single saline injection, it was reported that there was a short-term effectiveness of PRP injections over placebo for relief of pain and improvement in knee function as portrayed by Western Ontario and McMaster Universities Arthritis Index (WOMAC) subscores. In comparison with HA, multiple studies have demonstrated improvement in functional scores with both HA and PRP, but a significantly greater improvement with longer efficacy was noted in the PRP group. 12,43 Younger and more active patients with low-grade degenerative changes tend to receive significant improvement and better clinical improvement compared with more degenerative joints observed in older patients. 27,43,51 However, recent studies by Filardo et al have shown no significant difference between PRP and HA injection 26 and have refuted previous evidence that PRP was superior in middle-aged patients with moderate to advanced OA. 27 Therefore, a conclusion is not readily apparent at this time. Other studies suggest that PRP may not be sufficient in itself to produce a regenerative structure but that the addition of PRP as a molecular signal increases the subchondral progenitor population released into the joint during microfracture or injury. These stimulatory effects have been documented in cell culture 53,54 and promote the use of PRP as an augment to scaffold or resident cell populations that migrate into the joint during injury or marrow stimulation techniques. 73,80 Research conclusions derived from basic science and clinical trials, well discussed in a recent review by Xie et al, 91 collectively show PRP as a promising treatment and adjunct to the management of cartilage injuries. In this recent review, the positive mechanisms that show promise for isolated cartilage repair and the reversal of osteoarthritic processes are (1) the anabolic effect on chondrocytes, mesenchymal stem cells, and synoviocytes with resultant increases in cell proliferation, ECM accumulation, and HA secretion; (2) PRP may act as a bioactive cell scaffold as clot formation occurs to physically bridge full-thickness defects and increase cartilage regeneration; and finally (3) PRP may serve to inhibit inflammation and alleviate OA symptoms, with decreased pain and improved function, with a clinically acceptable safety profile. 91 In addition to this review, the anti-inflammatory properties have been well documented along with the ability of PRP to modulate pain, leading to increased function and better symptomatic management of OA. 81,83 In order for more high-level studies to emerge, consistent attention must be paid to the specific components in each study’s PRP preparation and the specifics of study design. A review of the pros, cons, and specific areas needed for future study in the use of PRP in research and clinical treatment of symptomatic cartilage defects is provided in Table 1.
Pros, Cons, and Specific Areas Needed for Future Study in the Use of PRP in Research and Clinical Treatment of Symptomatic Cartilage Defects a

a MSCs, mesenchymal stem cells; OA, osteoarthritis; PRP, platelet-rich plasma.
Clinical Application of in Vitro–Engineered Implants
For defects too large or complex for direct stimulation with subchondral (microfracture) or growth factor stimulation (BMP7, TGFβ, PRP, etc), the implementation of autologous chondrocyte implantation (ACI) has been shown to be effective when compared with microfracture or osteochondral autograft transplantation. The originally described ACI procedure requires a 2-step surgical approach, with harvesting of a section of articular cartilage, amplification, and eventual reintroduction with a periosteal flap into the prepared chondral defect. First introduced in 1994, this remains the only autologous chondrocyte technique approved by the United States Food and Drug Administration (FDA) at present and is at least a 2-stage procedure. In a review of 20 clinical studies of ACI, Iwasa et al 43 reported that femoral defect repairs had 60% to 90% excellent-to-good clinical results after 1 to 11 years. A second review of the literature on ACI concluded that a void of strong, prospective randomized controlled data exists, with the majority of success being documented in case series. 20 A Cochrane review performed to evaluate the efficacy and safety of ACI identified 6 heterogeneous trials with 431 participants with comparisons against mosaicplasty or microfracture techniques. A conclusion was reached that insufficient evidence was present to draw conclusions regarding the efficacy of ACI, with methodological flaws of incomplete follow-up and inadequate outcome reporting hindering the reported results. 85 One such study by Knutsen et al 48,49 demonstrated no significant difference in histological quality or macroscopic result between ACI and microfracture at 2 or 5 years, although both patient groups experienced significant clinical improvement. Furthermore, recent studies have shown that the use of ACI as a revision option for a failed microfracture procedure produces significantly worse results compared with ACI used as a primary intervention. 65,72 Therefore, these recent studies suggest clinicians should consider ACI as a primary method for the repair of both large and small cartilage lesions without previous marrow-stimulatory techniques (ie, microfracture) until more high-level evidence studies refute these findings. Inconsistency in the indications of use, whether for primary repair or revision of failed microfracture, has undoubtedly confounded the clinical result of ACI. Despite these obstacles, recent newer studies have shown promising results. In 1 such study, second-look arthroscopy of ACI grafts without augmentation carried out in 22 knees (32 lesions) demonstrated normal/nearly normal grafts based on International Cartilage Repair Society (ICRS) assessment, with hyaline/hyaline-like tissue observed on 13 (65%) of 20 taken core biopsy specimens. 38 More importantly, satisfactory objective outcome scores were observed in 94.4% of patients at 24 months. In a more recent study by this group, ACI has also been demonstrated to produce a hyaline-like repair, with biomechanical properties comparable with native cartilage and superior to fibrocartilage repair via histology and indentometry testing. 39 As the largest reviews have demonstrated, a level of uncertainty regarding the use of ACI exists in the literature at present, but newer, promising findings reiterate that continued future study is warranted. 85
Following the natural history of the use of ACI, the development of a bilayered collagen I/III membrane to provide a blueprint for the replanted chondrocytes emerged in response to complications associated with hypertrophy of the periosteal flap. Collagen-covered ACI (CCACI), as this was termed, has been used exclusively in Europe and remains “off-label” for use in the United States. This technology advanced into a matrix-associated autologous chondrocyte implantation (MACI)–type procedure, with culturing of expanded chondrocytes into a matrix/membrane before implantation. Despite these advances, a recent study by Zeifang et al 92 reported no difference in the advanced MACI technique compared with the original periosteal flap ACI technique in the repair of isolated full-thickness defects of the femoral condyle.
Functional and radiographic findings have demonstrated MACI to be an effective therapy for symptomatic, large cartilage defects when compared with microfracture, the current FDA-accepted “gold-standard.” The most recent publication to directly compare microfracture with MACI resulted from the SUMMIT (Demonstrate the Superiority of MACI implant to Microfracture Treatment) trial 76 that showed significant improvement in the activities of daily living and knee-related quality of life for patients treated with MACI compared with microfracture. Repair tissue quality was good as assessed by histology and magnetic resonance imaging (MRI), but no significant tissue quality difference was shown between treatments. A low number of treatment failures (nonresponders: MACI, 12.5% vs microfracture, 31.9%; P = .016) was observed, and there were no unexpected safety findings reported. MACI offers a more efficacious alternative than microfracture with a similar safety profile for the treatment of symptomatic articular cartilage defects of the knee, which is great progress in the treatment of large, isolated chondral lesions. 76 However, at this time, no demonstrable effect between MACI, CCACI, and ACI has been demonstrated in clinical study.
A common drawback to all these procedures is the need for a 2-stage surgical approach that requires harvest, amplification of chondrocytes, and reoperation for implantation. A variety of novel single-step techniques are now emerging, including the use of a chondrocyte conductive/inductive matrix with allogeneic fetal chondrocytes for implantation in chondral defects, and have been described as a means to generation of hyaline-like product. Known as DeNovo ET, the technology would be available as an off-the-shelf option that uses minced allograft donor cartilage to fill chondral defects and has been demonstrated to generate cartilage similar to physiologic hyaline baseline. 40,61 Other novel techniques are attempting to evolve a single-step cartilage repair procedure, 6,7,18 one such example being the Cartilage Autograft Implantation System (CAIS). In a preclinical animal study, Frisbie et al 33 demonstrated CAIS and ACI as superior to an empty defect (negative control) in equine articular defects, with CAIS being superior to ACI. In advancement to human clinical study, initial results show strong functional outcomes that persist at 2-year follow-up when compared with microfracture. 14 In this procedure, autologous hyaline cartilage was harvested arthroscopically from a nonweightbearing region of the notch or trochlear border and the harvested cartilage was mechanically minced and affixed on a synthetic absorbable scaffold using fibrin glue and implanted in an ACI-type fashion. This was shown to be safe and feasible and requires further study. 14 In recent advances, multiple studies have documented several different techniques, some combining microfracture with biocompatible matrices and others using novel cell mixtures alone, both of which have shown the ability to proliferate a hyaline-like repair in isolated defects. 6,18 Certain techniques look to use stem cells to augment the existing ACI protocol, achieving proliferation and development in a single-step procedure. 7 These types of innovation are significant, as a single-step repair procedure would serve as a point-of-care surgical procedure for the primary treatment of isolated, full-thickness chondral lesions in the knee and decrease return trips to the operating room. Further study will be needed to assess repeatability of a hyaline-like cartilage product with these surgical techniques. A review of the pros, cons, and specific areas needed for future study in the use of cartilage implants and biologic scaffolds is provided in Table 2.
Pros, Cons, and Specific Areas Needed for Future Study in the Use of Cartilage Implants and Biologic Scaffolds a
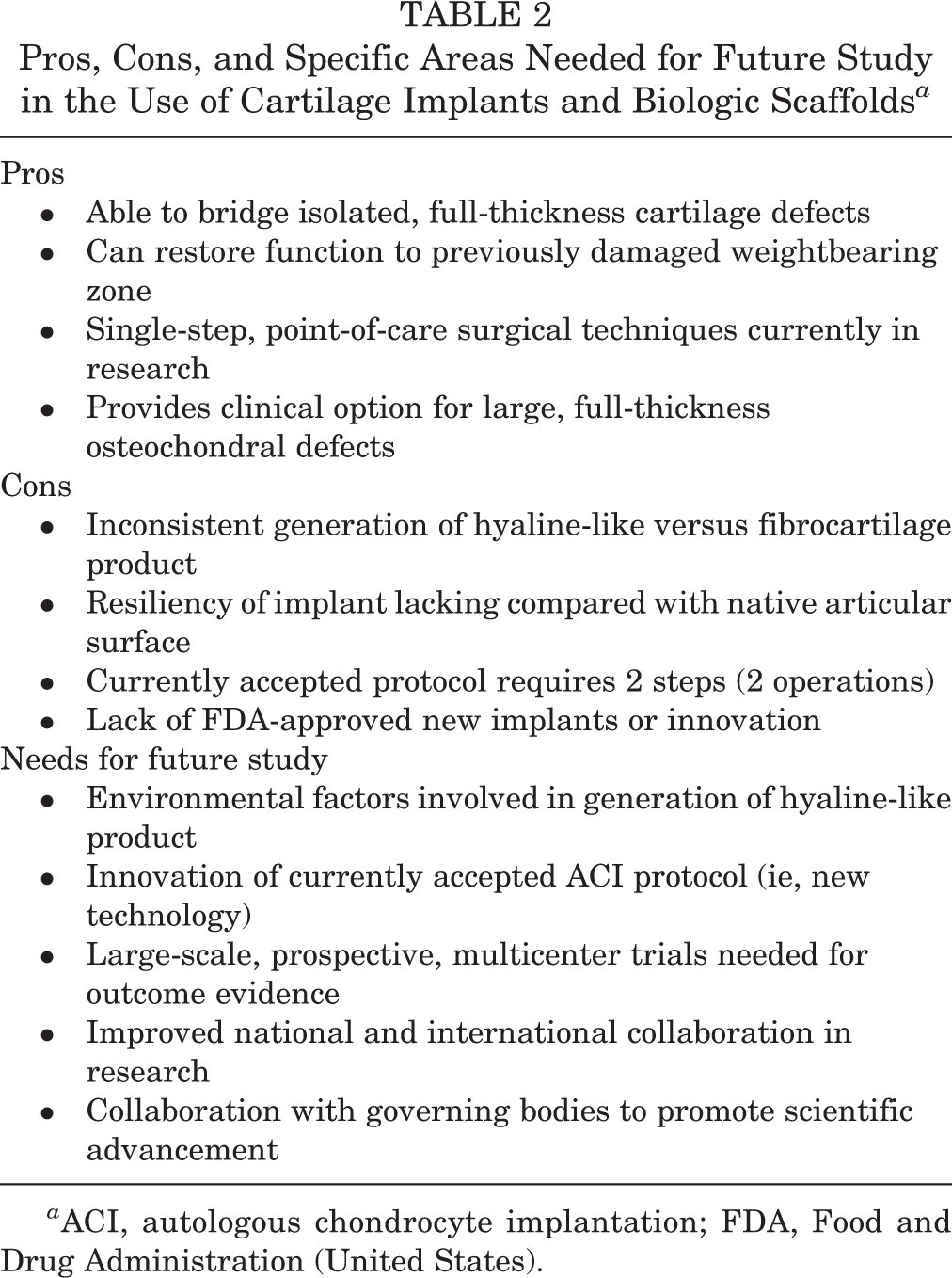
a ACI, autologous chondrocyte implantation; FDA, Food and Drug Administration (United States).
Stem Cell Therapy
Aside from a biologic delivery system of combined growth factors (bone marrow aspirate/bone marrow concentrate [BMA/BMC]), stem cells may also serve as an undeveloped “blueprint” capable of differentiating and re-creating a structure as complex as the osteochondral unit and articular surface. Mesenchymal stem cells (MSCs) are resident precursor cells that exist in large quantities across multiple tissue types and retain the ability to regenerate and repair tissue. The regenerative effects for the chondral surface are a direct result of the ability of MSCs to aid in the structural repair of the osteochondral unit while promoting anti-inflammatory effects across the articular environment. 28 In theory, the autologous collection and use of these cells for repairing full-thickness chondral deficits may serve as a “magic bullet” with programmed growth factor releases and alteration of the microenvironment milieu inherent to anatomic cartilage development, regeneration, and repair. MSCs reside in various tissues (bone marrow, adipose, muscle, etc), are harvestable in large quantities, 1,17,68 and have been shown to produce a variety of extracellular matrix proteins and molecules involved in the cellular process of native tissue repair. In basic science settings, they have also been shown to be reversible via specific induction techniques to a pluripotent precursor. The identification of several transcription factors, thought to play a major role in differentiation and the retention of pluripotent ability, has allowed successful induction of pluripotency from nonembryonic-derived cells. The generated “inducible-pluripotent stem cells” are promising and currently under study. 74 Most important, in using these organized repair blueprints, the joint microenvironment and dosing of proanabolic anti-inflammatory signaling can be regulated by intrinsic cellular feedback mechanisms rather than relying on repeated iatrogenic dosing. The MSCs derived from adipose, muscle, and synovium have been evaluated for their ability to restore focal cartilage defects and reverse catabolic joint environments of progressive OA via either articular injection or scaffold implantation.
As stated above, promising results have demonstrated reproducible hyaline-like cartilage product with proper cell induction and stimulation across MSCs collected from various tissue types, including bone marrow, adipose tissue, and synovium. The first MSCs identified and examined for clinical use were bone marrow–derived MSCs (BMSCs), primarily because of their high quantity in adult patients and ease in collection. 28,68 Clinical applications were explored for both expandable cultured cells and concentrated unmodified aspirate (bone marrow aspirate concentrate [BMAC]). Used alone or in conjunction with other biologic therapies (microfracture, collage scaffold, chondrocyte transfer, etc), BMAC collected from various bone marrow extraction sites have emerged as a therapy with good chondrogenic and osteogenic potential. 1,28,68 Fortier et al 31 demonstrated improved full-thickness repair, confirmed with histologic and MRI evidence, with the generation of a filled chondral defect and increased integration with surrounding cartilage when incorporated with microfracture. Similar studies suggest that BMAC in combination with collagen- or scaffold-covered defects promotes hyaline-like cartilage development with a seamless incorporation of new cartilage product. 25,34 Preclinical animal studies with BMSCs have also demonstrated generation of a stable, hyaline-like cartilage product with the use of scaffold or via intra-articular injection for delivery. 62,93 In clinical studies, symptoms of isolated defects and OA have shown to be improved after surgical implantation of BMSCs with a stable effect several years postoperatively. Repairs with BMSCs have demonstrated both fibrocartilage and hyaline-like tissue products, 86,87 with some BMSC implants achieving significant defect filling and congruity with neighboring cartilage. 37,46 Direct comparison between ACI and BMSC implantation by Nejadnik et al 70 in 2010 showed a similar pattern of clinical and subjective improvement up to 2 years postoperatively but concluded BMSC as favorable because of a decrease in operations (single-stage vs 2-stage), cost, and donor morbidity compared with ACI.
Adipose tissue also serves as a reservoir for MSCs. Adipose-derived MSCs (ADMSCs) can be recovered from liposuction aspirates 94 but can also be readily collected from human infrapatellar fat pads 22 and have the potential for differentiation into cartilage, as well as bone, tendon, and muscle. 79 The incorporation of autologous ADMSCs into scaffolds, after isolation and proper induction, with surgical implantation has shown to be successful in repairing full-thickness chondral defects with hyaline-like cartilage with seamless incorporation with native cartilage. Further analysis of these repairs demonstrated extracellular proteins, gene products, and surface markers were found to be consistent with native hyaline cartilage. 21,60 Direct injection of ADMSCs, concentrated or in combination with other biologic compounds, has demonstrated improvement in clinical pain and function outcomes without major adverse events. 50,71 In an overall review of the literature, consensus exists that ADMSCs at baseline have lower chondrogenic potential compared with either bone marrow– or synovial-derived cells. 26,66,79 However, recent advances made in the augmentation of ADMSCs with high-dose, combination growth factors (including TGFβ2 and BMPs) may increase this chondrogenic potential, albeit with increased detrimental inflammatory reaction. 28,47 This highlights the need for more study of ADMSCs and growth factor stimulation prior to application in clinical studies.
Synovial-derived stem cells are emerging as an additional promising source of MSCs, with greater chondrogenic potential than ADMSCs or BMSCs and less osteogenic potential. 19,69 Animal studies have demonstrated full-thickness lesion healing with an appearance similar to neighboring cartilage and high histological correlation scores. This suggests an increased chondrogenic ability as well as great potential for reproducible hyaline-like cartilage production, which would serve as an improvement from existing cartilage regeneration techniques.
At present, there are no clinical comparisons available in the literature regarding the optimal MSC source for cartilage regeneration. As mentioned above, correlations have been drawn between increased chondrogenic capability and the effectiveness of repair. However, as is seen with PRP and BMAC, a complex interplay of inflammatory modulation and repair potential needs to be established for incorporation of a consistent, hyaline-like product. Further characterization of the physical and biochemical properties of presumed “repaired defects” is needed. An important study by Ando et al 2 demonstrated that despite excellent chondrogenesis and defect filling, inferior tissue quality at the superior edge of cartilage does not adequately retain water and establish a resilient extracellular matrix. This will likely lead to an eventual failure of the repair product due to the high level of stress within an active joint. Therefore, continued study regarding the chondrogenic potential of MSCs, the organization and development of the osteochondral unit, and the interplay between environmental factors and intrinsic cellular potential is needed to advance this aspect of regenerative medicine. A review of the pros, cons, and specific areas needed for future study in the use of stem cells for regeneration of articular cartilage is provided in Table 3.
Pros, Cons, and Specific Areas Needed for Future Study in the Use of Stem Cells for Regeneration of Articular Cartilage a

a BMAC, bone marrow aspirate concentrate.
Identified Barriers to Research Advancement and Clinical Implementation
The use of biologics, including PRP, growth factors, bioengineered scaffolds, and stem cells, offers promising improvements in the prevention and treatment of OA in the active and aging populations. Isolated, full-thickness cartilage lesions cause significant morbidity and loss of function and initiate the inflammatory cascade toward diffuse joint arthritis. Early diagnosis and cartilage restoration/repair protocols, made available by continued research and large clinical trials, may reverse the cascade toward OA and provide additional years of pain control and high function. The following is a summary of the future direction for this field of study and what advances or innovations need to be discovered through collaborative, large-scale studies.
Earlier detection and diagnosis of isolated cartilage injury must be achieved. The collagen network and proteoglycan content of cartilage becomes disrupted prior to morphologic change of the articular surface and can therefore be paramount in the early diagnosis of isolated articular deficits and diffuse osteoarthritic changes. However, often a full-thickness cartilage deficit may be observed in the first clinical encounter. Advanced compositional MRI techniques that focus on early changes in the substructure of the osteochondral unit (ie, ultrashort echo time [UTE]–T(2)*, T2 mapping, and glycosaminoglycan chemical exchange-dependent saturation transfer/delayed gadolinium-enhanced MRI of cartilage [gagCEST/dGEMRIC]) may provide an opportunity to prognosticate a full-thickness deficit after a traumatic knee injury that normal MRI cannot evaluate. 5,10,41,42,88 This may influence weightbearing protocols and activity level, but more importantly, may provide clinicians an opportunity to treat the developing lesion with a biological factor (ie, PRP, growth factor, or MSC population) that encourages repair and prevents the cascade toward a full-thickness deficit. 36,75,84 For this clinical scenario to be possible, standardization of these advanced imaging techniques must first be achieved across preclinical and clinical research studies. These noninvasive techniques must be further validated in their ability to detect microstructure changes that can accurately prognosticate further injury and also serve to better quantify repair techniques as successful or unsuccessful in regenerating hyaline-like tissue that exhibits the mechanical and biochemical properties of native cartilage. Furthermore, research efforts must also focus on establishing that a documented “hyaline-like regenerate on advanced imaging” has equivalent functional testing and patient-reported outcomes in clinical practice. In establishing this relationship, significant changes to the clinical management and prognoses of articular defects can be made. Along with this goal of early diagnosis, continued search for a blood- or tissue-borne biomarker for OA would be paramount in the prevention or early treatment of OA. This would allow for the development of screening standards for joint disease and aid clinicians in their patient-specific diagnostic tests and treatments based on the level of biomarker observed. More study must also be directed to the characteristics of an ideal host for biologic therapy. The role of lifestyle, diet, baseline activity level, and other medical comorbidities in biologic treatments must be further elucidated. Further understanding of these factors and their role in regenerative medicine will guide the use of autologous versus allogeneic cellular products.
Once the diagnosis has been made and the host characteristics analyzed, among the first questions that need to be answered in developing the ideal biologic treatment are what is/are the ideal cell type(s) for the repair of cartilage lesions and what corresponding growth factors or intra-articular environment will optimize the ability of these cells to proliferate. A large number of studies have demonstrated the anti-inflammatory and chondrogenic properties of various different cell types but no clear champion has emerged. This is primarily due to a lack of standardization across research protocols (ie, how cells are collected, how they are cultured, what animal models are used, how results are quantified, etc). There are currently more than 15 different devices being used for the collection and production of an autologous PRP product, with documented differences noted across each preparation. This level of variability is confounding and significantly detracts from the ability of clinicians and researchers to establish a gold standard regarding cell count, growth factor concentration, host characteristics, and other variables. To achieve a level of uniformity across techniques, more large-scale collaborative efforts are needed. Large-scale data collection must be invoked at both preclinical and clinical research levels to generate valid conclusions regarding the ideal cell types, biologic preparations, and growth factors needed to optimize the regeneration of native, hyaline-like cartilage.
The remaining discussion must focus on the surgical implant (ie, how will the chondrogenic and osteogenic cells with appropriate factors be best integrated into the existing cartilage lesion). In designing the optimal regenerative/reparative scaffold, there are several factors that need to be addressed. First, the implanted scaffold should be able to re-create the entire osteochondral unit. The multiple levels of this structure each contribute to the success of native cartilage. Initial attempts at restoring native structure have generated an inferior product that does not demonstrate the resilience of healthy cartilage. This is likely due to the paradigm of hydrostatic and sheer pressures across the various substructures in the osteochondral unit and the ability of the implanted scaffold/cellular product to replicate this. A repair that does not balance the forces of the stressful intra-articular unit, though initially hyaline-like with uniform incorporation, will propagate and disrupt the healed graft, leading to overall clinical failure. More studies must be done in vitro and in vivo with advanced imaging and quantitative compositional data so that scaffolds can be characterized in an optimal fashion to replicate the function of the native osteochondral unit. When cartilage healing occurs in vivo, without biologic augmentation, repopulation from the subchondral unit and the outer synovial layer is observed. 44 A scaffold should thus aim to repair cartilage from the subchondral bone to the cartilage–synovial fluid interface. The biologic and physical properties of regenerating the entire osteochondral unit must be elucidated in future works. Second, the implanted scaffold or graft should be able to immediately load share so as to not alter the forces applied across the healthy, native articular surface. Advances in cell culture may achieve this level of production, where hydrostatic and other mechanical forces can be applied to the cellular grafts at early stages in their development. This may allow for earlier weightbearing postoperatively and a restoration of joint mechanics, and this prolonged stimulation of the graft may activate developmental cascades needed to optimize the entire osteochondral unit. This level of advance will require a widely collaborative effort across multiple levels of expertise to enhance the culture strategies so that a “ready product” is introduced during surgery on the isolated defect.
Last, scientific advancements in the laboratory and preclinical setting have been delayed from advancement into clinical practice due to regulations and restrictions from the US FDA. This discussion regarding the biologic therapies for rotator cuff, meniscus, and cartilage was well outlined in a recent review by Anz et al. 3 In 1997, the US FDA set forth in Title 21, Part 1271 of the Code of Federal Regulations, an approach to all articles “containing or consisting of all human cells, tissues, and cellular and tissue-based products (HCT/Ps) intended for implantation, transplantation, infusion, or transfer into a human recipient” (US Department of Health and Human Service 21, CFR Part 1271). A tiered approach based on assessment of patient risk divides biologic products into a lower risk category governed by section 361 of the Public Health Service Act (PHSA) and a higher risk category regulated by section 351 of the PHSA. A “351 product” must follow tissue practices and manufacturing standards approved by the FDA on a case-by-case basis and must also pass a premarket approval process with clinical trials and an active investigational new drug (IND) application in place. There are notable time and financial costs required to adequately achieve this proof of concept, and thus, the application of products into clinical practice in a timely manner has been prolonged. To differentiate a low-risk 361 product from a high-risk 351 product, compounds must have been prepared with minimal manipulation, intention for homologous use (must be reintroduced into a patient for its native use), without combination of products, and with safety data demonstrated by lack of systemic effects. 3 If the product vying for clinical use does not meet all 4 aforementioned criteria, it is labeled with 351 status and must garner premarket approval as described above. Most orthopaedic stem cell and growth factor interventions will require passage of 351 regulations. Specific examples of activities that require 351 regulation by the FDA include culture expansion of MSCs prior to reimplantation (more than minimal manipulation) and the use of ADSCs acquired from liposuction via intra-articular injection (nonhomologous use). 3,59 Without completion of premarket approval and an approved biologics license, stem cell products excluded from 361 status are unable to be marketed or offered. Though warranted for the continuation of safe therapies offered to patients, these regulations delay the advancement of newer, peer-reviewed techniques from further clinical application.
With the acknowledgment of past progression of research in the field of stem cells and biologic therapies, the FDA has retained the right to regulate and monitor the use of stem cells in clinical settings. An example of a regulatory mechanism that limits clinical study and advancement is the FDA regulation that cells must not leave the operating room (ie, cannot be modified or expanded in culture) prior to their reimplantation. 3 The impact of this regulation is demonstrated when cultured and induced BMSCs are compared with autologous BMAC. Culture expansion would provide a fine-tuned approach to biologic augmentation; however, because of these regulations, study into the specific characterization and augmentation of the BMSCs is not clinically applicable at this time. Instead, a surgeon must depend on recovery and reinjection without augmentation to produce an adequate cell count and aspirate. However, unlike the characterized samples from laboratories, yield from intraoperative recovery and reinjection is inconsistent and less well defined. Subsequently, this indirectly confounds the patient-reported and objective outcomes because the aspirates that are reinjected and evaluated for clinical improvement have not been isolated, cultured, and characterized, and therefore, conclusions about specific active mediators can be difficult. This increases the variability of the treatment because a predetermined optimal cell count or growth factor composition cannot be standardized nor can a precise characterization of host stem cells, or host PRP, be performed prior to reimplantation. Host variability, the regional tissue source of the collected aspirate(s), and potential inadequate collection all lead to uncertainty regarding observed clinical outcomes. Despite successful research advancements, specifically in ACI, there has been minimal advancement of clinical trials and the emergence of new technologies into the clinical setting. Scientists and clinicians have to base their study design and biologic augmentation off what is allowed under current regulation and not what has been shown in peer-reviewed studies to be effective and believed to be safe. Many have approached this reality by adapting to the regulations rather than attempting to advance a new technology through the application process for a novel therapy. This is illustrated in the fact that despite multiple studies demonstrating superior results with new therapies in preclinical study compared with previously accepted gold standard techniques, 16,77,78,84 there have been no introductions of novel therapies since the approval of ACI approximately 20 years ago.
The next several years should prove to be important in setting the framework for the use of biologic strategies to heal full-thickness cartilage defects and articular injury. At present, experimental techniques, including the method of production for a biologic compound or cellular concentrate, patient population, and outcome measures, are variable, making the production of a consensus statement or comparing peer-reviewed works difficult. There is a need for a collaborative effort, multicenter studies, and standardized biologic regimens for the treatment of cartilage injury. Cell populations and potential injectable compounds (ie, PRP, BMAC, and MSCs) will need to be better defined as to their composition of growth factors, profile of expression, and their direct effect on the joint microenvironment. Combination therapies must be evaluated to better replicate the anticatabolic, proanabolic, and organized manner of chondrocyte proliferation and incorporation. New experimental techniques will need to be developed to allow for the development of novel scaffolds capable of replicating the osteochondral unit with preconditioned ability to bear stress soon after implantation. This will also depend on evidence-based characterization of the individual therapies; otherwise, it may produce more confusion as to the component parts of any combination therapy and how it exerts its effect on damaged tissue. Last, partnering with regulatory bodies will be important to allow for the collaborative efforts of scientists, engineers, and physicians to advance clinical therapies capable of achieving a meaningful increase in the functional status of patients.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: The 2015 American Orthopaedic Society for Sports Medicine (AOSSM) Biologics II Think Tank was sponsored by RTI Surgical. The outcomes and opinions from this Think Tank are solely those of the authors and do not reflect any influence from the sponsor. R.F.L. is a consultant for and receives royalties from Arthrex, Ossur, and Smith & Nephew.
Acknowledgment
The authors acknowledge the significant contributions to the Biologics II Think Tank by Barton J. Mann, PhD (deceased), Director of Research for AOSSM. His work to advance the field of sports medicine is greatly appreciated, and he will be missed by all.