
Abstract
Background
Most published studies on injuries in the ballet dancer focus on the lower extremity. The rigors of this activity require special training and care. By understanding prevalence and injury pattern to the musculoskeletal system, targeted prevention and treatment for this population can be developed.
Purpose
To determine the incidence and prevalence of musculoskeletal injuries in ballet.
Study Design
Systematic review; Level of evidence, 4.
Methods
A systematic review registered with PROSPERO was performed using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Level 1 through 4 evidence studies reporting incidence of musculoskeletal injuries in male and female ballet dancers were included, with the numbers and types of injuries extracted from each. Injury rates were recorded and calculated based on professional status, sex, and nature of injury. Incidence was defined as number of injuries sustained over a specific time. Prevalence was defined as proportion of subjects with an injury at a given point in time.
Results
The studies analyzed reported injury incidence or prevalence in more than 1365 amateur and 900 professional dancers. The mean age was 16.2 years among amateur and 27.0 years among professional dancers. The incidence of injury among amateur dancers was 0.99 and 1.09 injuries per 1000 dance hours in males and females, respectively; 75% of injuries were overuse, with similar rates among males and females. In professional dancers, the incidence of injury was 1.06 and 1.46 injuries per 1000 dance hours in males and females, respectively, and 64% of female injuries were overuse, compared with 50% in males (P < .001). Only 3 studies provided prevalence data, including 62% prevalence of lumbosacral pain, 58% painful snapping hip, and 29% patellofemoral pain. Lower extremity injuries comprised 66% to 91% of all injuries, with the foot and ankle accounting for 14% to 57%.
Conclusion
The overall incidence of injury among amateur and professional ballet dancers is 0.97 and 1.24 injuries per 1000 dance hours, respectively. The majority are overuse in both amateur and professional dancers, with amateur ballet dancers showing a higher proportion of overuse injuries than professionals (P < .001). Male professional dancers show a higher proportion of traumatic injuries, accounting for half of their injuries (P < .001).
Ballet, or classical dance, is a popular sport and recreational activity that places extreme physical demands on the human body. Even within the realm of dance, ballet presents unique demands in terms of flexibility and strength, as well as body aesthetics. These demands influence fitness training regimens and nutritional habits. 25,41 Injury patterns in ballet would be expected to be unique, requiring a targeted approach to injury prevention and treatment. 40 Prerequisite to such a targeted treatment approach is an understanding of specific injury patterns among ballet dancers.
Various reviews on dance injuries have been published. These include heterogeneous populations of both ballet and nonballet dancers. 3,13,17,18,28,35,38,39 The majority of ballet injury investigations predominantly report lower extremity injuries. 4,16,24,26,31 –34 Less frequently reported injuries include back and upper extremity injuries. 1,3,7 Recently, as young adult hip pathology has become better understood and less invasive treatment options have become more widely available, attention has been heightened with respect to injuries of the hip. This is especially pertinent to ballet, given the stresses placed on the hip and pelvis resulting from the extreme motion required in ballet. 19
The purpose of this study was to perform a systematic review that determined the incidence and prevalence of musculoskeletal injury in ballet. The authors hypothesized that the incidence of injury would be greater than 1 injury per 1000 dance hours, with a 25% overall injury prevalence. Given the rigorous demands of strength and flexibility in ballet, most injuries were expected to affect the lower extremity.
Methods
Search Strategy
A systematic review was registered with PROSPERO (registration number, CRD42014010088) on June 5, 2014, and performed using PRISMA guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses). 22 On June 4, 2014, a PubMed (MEDLINE) search was performed using the following search string: ((((injury[Title/Abstract]) OR injuries[Title/Abstract]) OR pain[Title/Abstract])) AND ((((ballet[Title/Abstract]) OR dance[Title/Abstract]) OR dancer[Title/Abstract]) OR dancing[Title/Abstract]).
Study inclusion criteria included peer-reviewed published therapeutic studies with levels 1 through 4 evidence (Center for Evidence Based Medicine [CEBM] classification) that were written in English from January 1, 1984 to June 4, 2014, to identify studies written in the past 30 years. Diagnostic and prognostic studies reporting incidence or prevalence of musculoskeletal injury in ballet were eligible. Study participants included ballet dancers from all ages, both sexes, and all levels (ie, recreational, competitive, elite amateur, professional). Conference abstracts were not eligible for inclusion. Level 5 evidence, narrative reviews, synthetic reviews (systematic reviews, meta-analyses), letters to the editor, biomechanical studies, anatomical studies, surgical studies, and basic science studies were also excluded. Non–English language investigations were excluded. Articles on other forms of dance, such as modern, hip hop, ballroom, contemporary, jazz, folk, street, Latin, and swing were excluded. Articles including both ballet and nonballet types of dance without separating out ballet injury incidence or prevalence were excluded. Finally, articles based on ballet but not addressing ballet injuries were eliminated. Case series reports focusing only on 1 specific injury in dancers (eg, flexor hallucis longus tendon injury) without injury incidence or prevalence data were excluded. Duplicate patient populations appearing in separate distinct publications were analyzed and only reported once.
Results from the search string above were initially screened based on a review of abstract or full-text of each article. Studies that were clearly irrelevant were removed. The remaining articles were obtained in full-text PDF format and reviewed.
Data Extraction
Data were extracted from each study and recorded in Microsoft Excel. Country of origin, year of publication, journal of publication, author list, amateur or professional status, definition of injury, age, sex, number of participants, number of injured participants, number of injuries, injury incidence, injury prevalence, nature of injuries (ie, acute traumatic vs chronic overuse), and injury sites/diagnoses were recorded.
Definition of Injury
Varied definitions of injury were employed by different authors among these studies. The most common definition, used by 6 studies, 2,4,6,8,29,44 was based on conditions that required at least modification of dance activities, even if no dance activities were missed. A more stringent definition used in 5 studies 5,9,12,23,43 included an element of time lost from activities. Five additional studies 10,11,27,37,42 appeared to fall into one of these first definitions but did not explicitly state whether they included an element of time lost. Three studies 14,20,30 defined injury based on participants having sought care from either an orthopaedic surgeon or a physical therapist. One study 15 based the definition of injury on the incurrence of medical expenses. One study 21 did not include a specific definition of injury.
Statistical Analysis
Chi-square analysis was used to compare the numbers of dancers with overuse verses traumatic injuries among males and females and amateurs versus professionals.
Results
Twenty-one studies were included in the final analysis (Figure 1). No article reported the presence of a financial conflict of interest. Eight articles denied the presence of any conflict of interest. In 13 articles, conflict of interest was simply not addressed. There were more than 1365 amateur and 900 professional dancers analyzed (Table 1). The mean age (±SD) was 16.2 ± 1.02 years among amateur and 27.0 ± 1.08 years among professional dancers.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram developed from this systematic review of 21 studies.
Study Demographics a

a F, female; M, male.
Distribution of Injuries
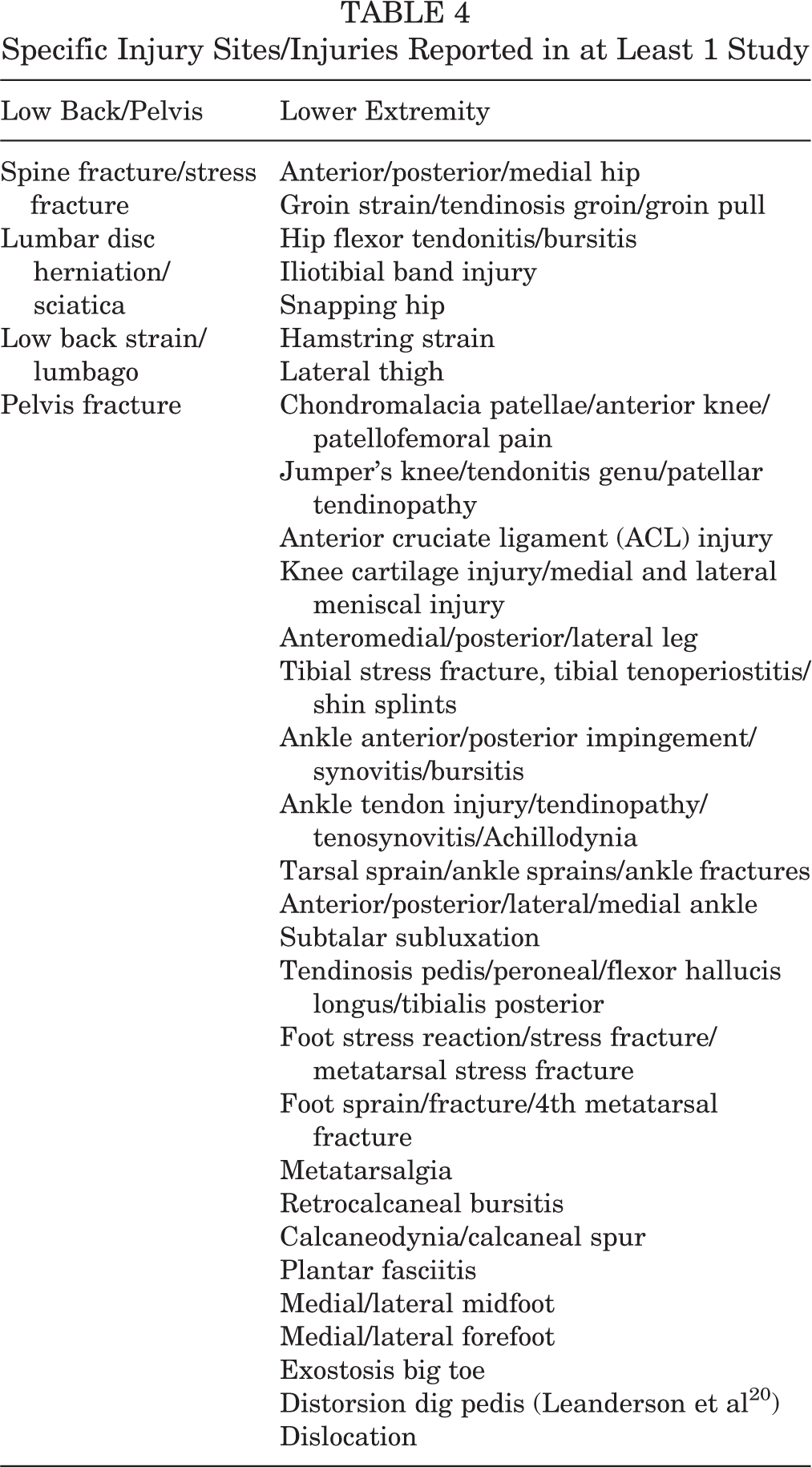
Twelve studies ‡ reported distribution of injuries based on body site. Percentages of total injuries per body site either were reported or were calculated from the number of injuries for each site. Due to a lack of a uniform injury site classification scheme across studies, pooling data to calculate overall percentages for each site was not possible. However, grouping sites into broader categories such as lower extremity (LE) or foot and ankle was possible. In the amateur groups (Table 2), 3 studies excluded upper extremity (UE) injuries. Two of these also excluded traumatic injuries. In these studies excluding UE injuries, LE injuries accounted for 86% to 93% of injuries, with 18% to 46% of total injuries occurring in the foot and ankle. Of those reporting injuries from all body sites, the LE injuries comprised 75% to 91% of total injuries, with foot and ankle accounting for 39% to 53%. In the professional groups and unspecified groups, a similar pattern was seen (Table 3). LE injuries made up 66% to 78% of all injuries, with 14% to 57% of all injuries involving the foot and ankle (Table 4).
Distribution of Injuries Among Amateur Dancers a

a LE, lower extremity; misc, miscellaneous; UE, upper extremity.
Distribution of Injuries Among Professional or Unspecified Dancers a

a C-spine, cervical spine; L-spine, lumbar spine; LE, lower extremity; misc, miscellaneous; T-spine, thoracic spine; UE, upper extremity.
Specific Injury Sites/Injuries Reported in at Least 1 Study
Injury Prevalence
Only 3 studies provide prevalence data. Drezewska and Sliwinski 11 reported a prevalence of lumbosacral pain in 62% of 71 dancers, with no significant difference in prevalence between females and males. Winslow and Yoder 42 reported a 29% prevalence of patellofemoral pain in a sample of 41 female ballet students. Winston et al 43 reported on a sample of 87 professional and amateur dancers with a 91% prevalence of snapping hip, of which 58% were painful. However, only 8% of the dancers reported having to take time off from dancing due to pain.
Injury Incidence
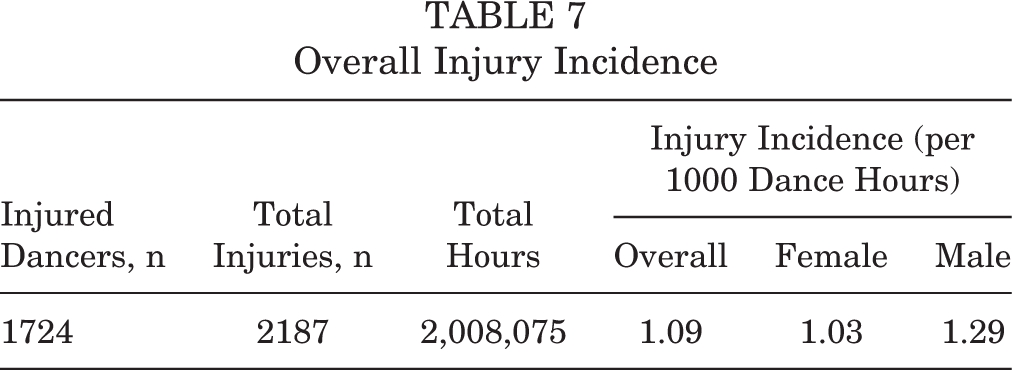
Incidence was reported as either a rate of injury per 1000 dance exposures, 4,12,14,23 or more commonly, per 1000 dance hours. 2,4,12,14,20,30,44 Seven studies reported injury incidence per 1000 dance hours, including 4 amateur populations 2,12,14,20 and 3 professional populations. 2,30,44 Among the amateur populations (Table 5), 1147 total dancers (769 female, 378 male) accumulated 1073 injuries (522 in females, 353 in males; some studies did not specify sex) during 1,111,133 total dance hours. This corresponds to 0.97 (range, 0.77-2.40) injuries per 1000 dance hours overall, with 0.99 (range, 0.8-2.19) injuries per 1000 dance hours for females and 1.08 (range, 0.8-2.81) injuries per 1000 dance hours for males. Among the professional populations (Table 6), 577 total dancers (96 female, 91 male, 390 unspecified) accumulated 1114 injuries (538 in females, 576 in males) over 896,942 total dance hours. This corresponds to 1.24 (range, 0.62-4.44) injuries per 1000 dance hours overall, with 1.06 (range, 0.56-4.14) injuries per 1000 hours in females and 1.46 (range, 0.70-4.76) injuries per 1000 dance hours in males. Combining amateur and professional populations (Table 7) results in 1724 total dancers with 2187 total injuries over 2,008,075 hours, or 1.09 injuries per 1000 dance hours. Overall, female and male dancers had rates of 1.03 and 1.29 injuries per 1000 dance hours, respectively.
Injury Incidence Among Amateur Dancers

Injury Incidence Among Professional Dancers

Overall Injury Incidence
Injury Characterization
Six studies characterized injuries as traumatic verses overuse, including 2 from professional ballet populations 2,30 and 4 from amateur populations. 12,14,20,29 In the amateur groups (Table 8), 1096 injuries among 975 dancers were reported. Overuse injuries made up 75% (range, 72%-82.9%) of all injuries in this demographic. Only 1 study 20 subdivided injuries based on sex, with overuse injuries comprising approximately 77% of injuries in both males and females. Among professional dancers (Table 9), 1102 injuries among 261 dancers were reported; 57% (range, 56.7%-57.4%) of these injuries were reported as overuse injuries. In this group, injuries in females comprised 64.4% (range, 61.5%-66.3%) of overuse injuries, while overuse injuries in males totaled 50.1% (range, 48.8%-52.7%). When amateur and professional populations were pooled together (Table 10), 2198 injuries among 1236 dancers were predominately overuse injuries, accounting for 65.9% of total injuries. Overuse injuries in females accounted for 68.6% of injuries compared with 56.2% in males.
Nature of Injuries Among Amateur Dancers

Nature of Injuries Among Professionals

Overall Traumatic Versus Overuse Injuries

Discussion
The purpose of this study was to determine the incidence and prevalence of musculoskeletal injury in ballet. As hypothesized, the incidence of injury was high, with most injuries affecting the lower extremity. The incidence of injury among amateur dancers was 0.99 and 1.09 injuries per 1000 dance hours in males and females, respectively. Seventy-five percent of injuries were due to overuse, with similar rates among males and females. In professional dancers, the incidence of injury was 1.06 and 1.46 injuries per 1000 dance hours in males and females, respectively. Sixty-four percent of female injuries were due to overuse, while 50% of injuries in males were attributed to overuse. There was a notable paucity of studies reporting prevalence of ballet injuries. Only 3 studies provided prevalence data, including 62% prevalence of lumbosacral pain, 29% prevalence of patellofemoral pain, and 58% prevalence of painful snapping hip. Overall, lower extremity injuries comprised 66% to 91% of all injuries, with foot and ankle accounting for 14% to 57% of these.
Analyzing injury rates or incidence is challenging. Reporting based on injuries per 1000 dance hours or injuries per 1000 dance exposures provides a standardized method of reporting injury rates. Assuming that dance hours or dance exposures both within and among groups of comparison are uniform in intensity, these methods of reporting allow for easy comparison across populations studied for various amounts of calendar weeks, months, or years. In the amateur dancers reviewed here, there were similar rates of injury between males and females: 0.99 and 1.09 injuries per 1000 dance hours, respectively. Injury rates were also noted to rise with increasing age among students. Overuse injuries accounted for the majority of injuries, comprising 75% of all injuries, with similar rates for male and female dancers.
At the professional level, these trends changed. In general, the injury rate increased compared with the amateur level. Males had a higher rate of injury, at 1.46 injuries per 1000 dance hours, while the injury rate in females was little changed, at 1.06. Additionally, the nature of the injuries also changed. Traumatic injuries accounted for more of the overall injuries among professionals. While overuse injuries still accounted for the majority of female injuries at 64%, 50% of injuries in males were traumatic.
Unfortunately, a review of point prevalence of injuries in ballet revealed a surprising paucity of data. Only 3 studies reported prevalence of musculoskeletal injuries or conditions. Being able to understand what injuries exist and the numbers of dancers affected by injury at a given point in time would be valuable information, especially for a ballet company. Further quantification based on sex, position, time of season, and so on, would also provide useful guidance for management of the company.
Examining relative distributions of injuries allows for identification of body sites that are most prone to injury and suggests which body sites should be targeted for treatment and prevention efforts to have the most significant impact, whether from a time lost or financial perspective. Reviewing the list of specifically reported injuries across all the articles in this review is also revealing. This may be helpful for identifying further study opportunities for elucidating additional specific injuries in the context of ballet. For example, while snapping hip due to iliopsoas tendinitis/bursitis has been reported, no mention is made of femoroacetabular impingement and associated pathology.
Without a standardized methodology for injury surveillance among ballet dancers, pooling data and making meaningful comparisons among ballet populations to guide injury prevention efforts proves difficult, as highlighted in this review. Key elements of an effective approach would include a consensus definition of injury, a standardized method of reporting exposure and injury incidence, and a uniformly applied injury classification scheme. In these studies, the method of defining injuries varied widely, including need for activity modification, time lost from activity, need for consultation with a health care practitioner, or even incurrence of financial cost. Each of the varied definitions of injury has its nuances, but adoption of a single standard would facilitate reliable comparisons among different populations of dancers. Additionally, while many of the recent studies analyzed here reported injury incidence as injuries per 1000 dance hours, this clearly has not been standardized. Finally, injuries should be classified based on a uniformly adopted classification scheme. One example is the Orchard Sports Injury Classification System (OSICS), which was initially developed in 1992 for injury surveillance in rugby and Australian rules football. 36 Subsequently, it has been revised and expanded for international use in other sports, such as soccer and cricket. Each of these aspects of a standardized approach to injury surveillance would enable pooling of data across studies and populations in ballet, facilitating more efficient and more reliable efforts at injury prevention.
Study limitations include heterogeneity in definitions of injury among the studies analyzed, heterogeneity in methods of reporting injury rates, and heterogeneity in methods of reporting injury sites. As with any systematic review, the quality of the review is only as good as the data from the individual studies analyzed. For example, some studies employed questionnaires to elicit injury data, inherently prone to recall bias, rather than prospectively collecting injury incidence and prevalence. Further limitations include variability in study design and conduct, subject demographics, level of dance participation, length of follow-up (or time of enrollment for assessment of incidence), and heterogeneity in clinicians making the diagnosis of injury. Furthermore, the lack of any objective short- or long-term assessment, such as plain radiographs or magnetic resonance imaging, precludes analysis of the effect of dancing on the health of the dancer’s body. In essence, does the extreme motion and stress placed on the dancer’s body have long-term effects on the occurrence of degenerative conditions such as osteoarthritis? This study does not answer that question. However, it does provide an impetus for future research at the authors’ institution and other institutions interested in preservation of the health of the ballet dancer.
Conclusion
In this review, the overall incidence of injury among amateur and professional dancers was calculated to be 0.97 and 1.24 injuries per 1000 dance hours, respectively. The majority of ballet injuries were due to overuse in both amateur and professional dancers, with amateur ballet dancers showing a slightly higher proportion of overuse injuries than professionals. Male professional dancers showed a relatively higher frequency of traumatic injuries, which account for half of their injuries.
Footnotes
Notes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.