
Abstract
Key Points
The foot and ankle complex is the most affected area by overuse injuries in both male and female ballet dancers.
No significant differences have been found between male and female ballet dancers in the prevalence, incidence, or anatomical location of overuse injuries.
The limited number of studies examining the severity of overuse injuries highlights the need for further high-quality, original research to enable meaningful comparisons.
Introduction
Overuse injuries develop gradually when a specific part of the body is subjected to repeated stress or strain. 1 Mechanisms associated with overuse injuries include repetitive movements, 2 inadequate recovery time, and excessive loading. 3 Ballet dancers may be at an increased risk of overuse injuries due to a multifactorial complex consisting of, low energy availability and high energy expenditure, and in some dancers reduced bone mineral density. 4 However, bone mineral density profiles in male and female ballet dancers have been reported to be heterogenous. 4 Whilst reduced bone mineral density has been documented in subgroups 5 characterised by low energy availability or menstrual dysfunction, it is not a universal feature amongst all ballet dancers.4,5 The prevalence of overuse injuries is generally more common than traumatic injuries in ballet. 6 However, pre-professionals have been reported to be prone to overuse injuries because of technical issues like jumping asymmetry 7 before optimal conditioning, whereas professionals are at risk because of longer training hours, higher performance demands, and cumulative physical stress over time. 8 Anatomical differences are also apparent in locations of overuse injuries; lower extremity injuries were more common in both professional 9 and pre-professional ballet dancers. 10 Moreover, in pre-professional dancers, conditions such as tenoperiostitis of the tibia and ankle impingement and tendinopathies were the most common overuse injuries. 10 Comparatively, professional dancers, experience a wider anatomical distribution of injuries in addition to the lower limb 9 due to the greater cumulative exposure. 11
With regards to sex, differences in the prevalence of certain overuse injuries, such as stress fractures, are known in other athletic populations. 12 This can be attributed to sex-specific factors with 1 example being hormonal variations and menstrual irregularities. 13 Menstrual dysfunctions can disrupt oestrogen levels, resulting in diminished bone mineral density and impaired musculoskeletal health; this increases the susceptibility to overuse injuries such as stress fractures. 14 However, whether these mechanisms result in comparable sex-related differences in ballet dancers remain uncertain due to the limited and inconsistent evidence.4,9 Other sex differences have been reported in terms of severity 4 and anatomical location. 15 Male dancers lost 9 days to injury in comparison to 3 days lost by female professional ballet dancers. 6 Anatomically, male dancers have been found to be more likely to sustain overuse injuries in the knee joint whereas female dancers in the foot and ankle. 15
Overall, the current body of evidence offer limited direct comparisons of overuse injury epidemiology between male and female ballet dancers. One review 9 has previously investigated the prevalence of overuse injuries, Smith et al 9 observed that females had a significantly higher prevalence of overuse injuries in comparison to males. Although other systematic reviews11,16 have investigated musculoskeletal injuries in pre-professional ballet dancers, they did not solely focus on overuse injuries as the main outcome. Furthermore, Smith et al 9 focussed on prevalence, revealing a considerable gap for other epidemiological outcomes like incidence, severity, and anatomical location.
Therefore, the aim of this systematic review was to analyse differences in the prevalence, incidence, severity, and anatomical location of overuse injuries between male and female ballet dancers at a professional and pre-professional level. This will allow identification of differences which can lead to clinical implications such as greater awareness of sex-specific factors in overuse injury like menstrual cycles during musculoskeletal screening in female dancers.
Methods
This review was conducted according to the PRISMA (2020) guidelines for systematic reviews 17 and registered on PROSPERO (CRD420251104232).
Eligibility Criteria
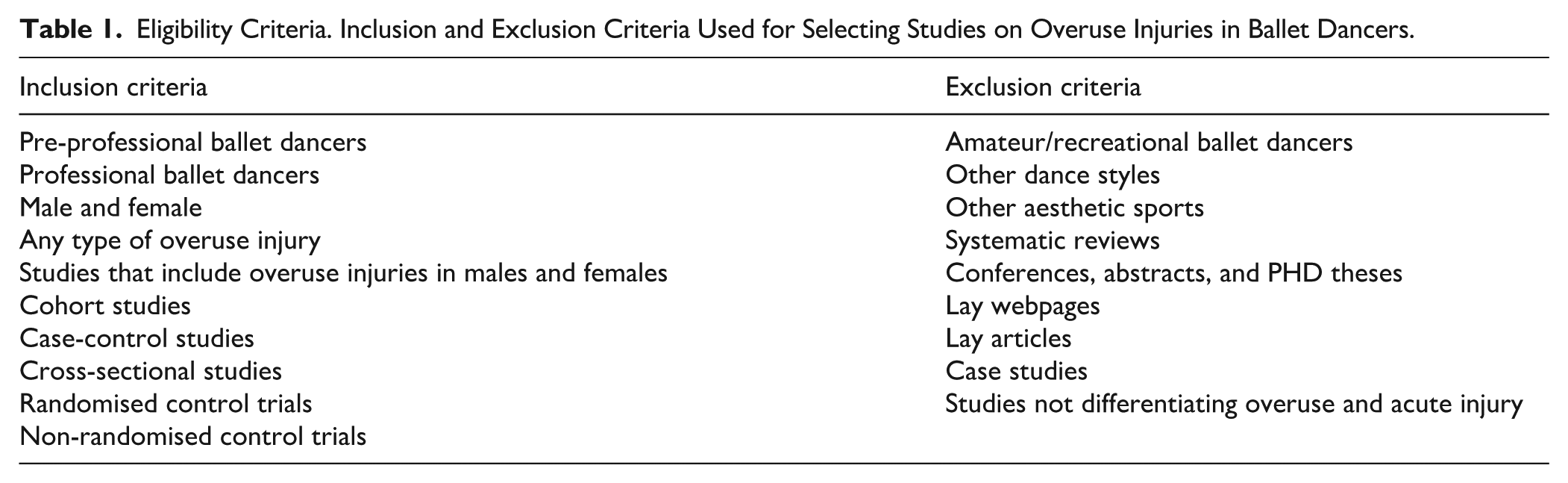
The eligibility criteria were modelled in a Population, Exposure, Comparator, Outcome (PECO) format. 18 The population were professional and pre-professional male and female ballet dancers, and the exposure was ballet training. Amateur/recreational ballet dancers were excluded. The comparison was between male and female ballet dancers, and the outcomes included prevalence, incidence, severity, and anatomical location of overuse injuries.
Detailed information on the inclusion and exclusion criteria can be seen in Table 1.
Eligibility Criteria. Inclusion and Exclusion Criteria Used for Selecting Studies on Overuse Injuries in Ballet Dancers.
Information Sources
Studies were identified and retrieved across 3 electronic databases (PubMed, Web of Science, and Embase). The search was conducted on 01 July 2025 by 4 independent reviewers (R.R., A.W., S.T., T.R.). Citation searching was conducted by 4 independent reviewers (R.R., A.W., S.T., T.R.) on 06 July 2025 and identified 2 further studies.
Search Strategy
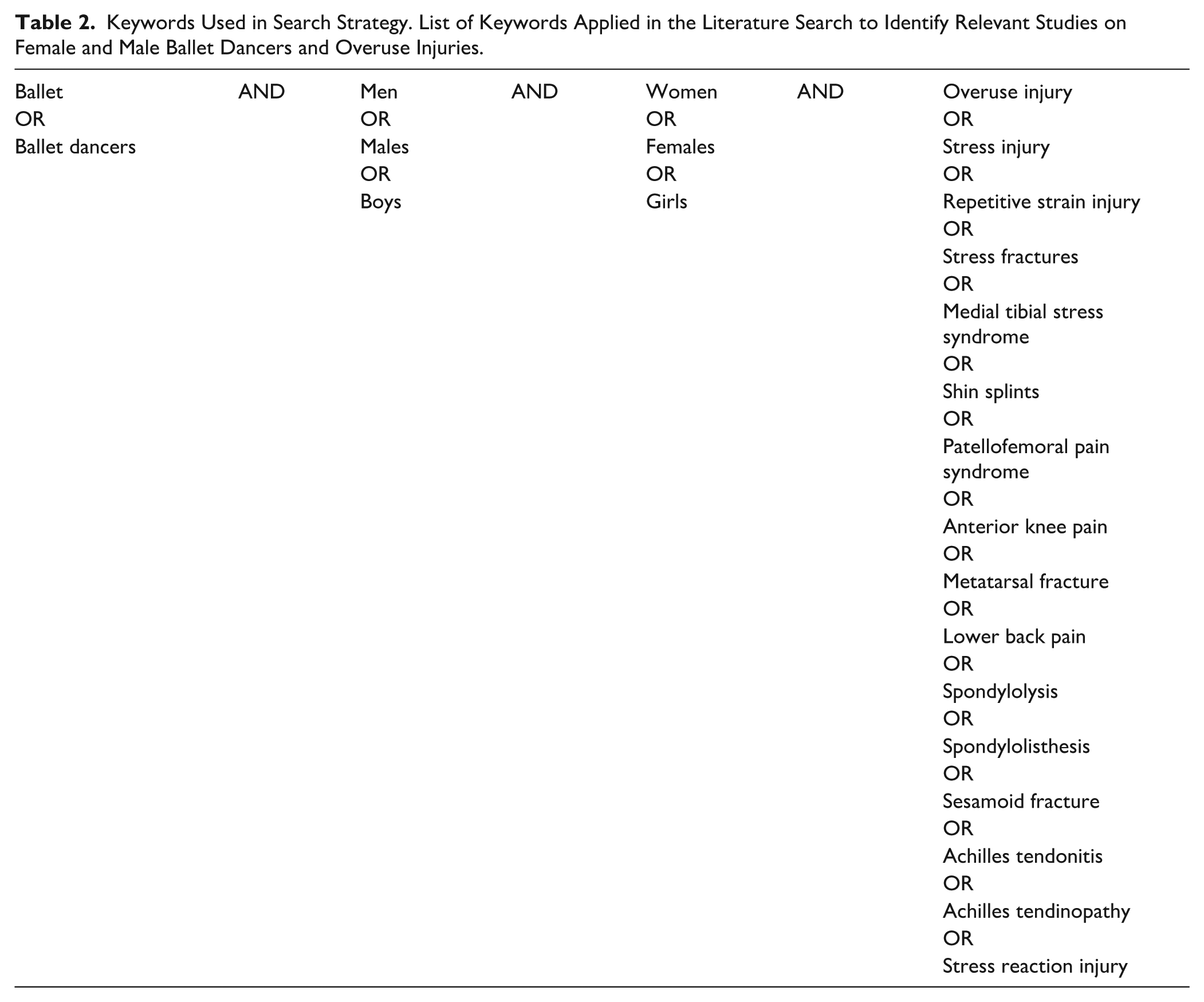
The search strategy evolved from the PECO format of the eligibility criteria. Synonyms were used with these keywords to expand the reach of the search terms (Table 2). This systematic review did not focus on 1 specific type of overuse injury; keywords like “Medial Tibial Stress Syndrome” and “Achilles Tendinopathy’ were also included. This allowed the initial search to be broader. However, a timeframe filter was set; only studies from and after 2000 were included.
Keywords Used in Search Strategy. List of Keywords Applied in the Literature Search to Identify Relevant Studies on Female and Male Ballet Dancers and Overuse Injuries.
Selection Process
Studies were added to Covidence 19 software to streamline and aid the process. Duplicates found by Covidence were automatically removed and any other duplicates were manually removed. Two independent reviewers (R.R., A.W.) were involved in all stages of the screening process: title, abstract, and full text. After the reviewers agreed on a decision, the study was either removed or moved to the next stage of screening. Discrepancies and conflicts were resolved by a third reviewer (MA) who was not involved in the initial selection phase of the screening process.
Data Collection Process
Data extraction was performed manually with no use of automation tools. As with the selection process, 2 independent reviewers were involved in the data extraction process. After the reviewers (R.R., R.D.) independently performed the data extraction process, a third independent reviewer (M.A.) looked at the extracted items and finalised the collected information. Discrepancies were solved by reaching consensus.
Data Items
The outcomes included: prevalence, incidence per 1000 hours, severity (time loss due to injury), and anatomical location of overuse injuries. The outcome measures were used to compare the difference in overuse injuries between male and female ballet dancers.
Other extracted information included: author, year of publication, study design, study length, number of participants, age, definition, reporting and number of overuse injuries, number of total injuries and dance exposure.
No changes were made to eligibility criteria in this process. However, not all studies were compatible with all the items that were extracted. If the studies included had information present on any of these outcomes, they were extracted in the data collection process.
Risk of Bias and Quality Assessment
To assess the risk of bias, the quality assessment tools utilised were the Newcastle-Ottawa Scale (2000) 20 for cohort studies and AXIS (2016), the critical appraisal tool for cross-sectional studies. 21 Two reviewers (R.R., R.D.) independently assessed the quality of each study using the appropriate tools. The scores were reviewed independently (M.A.), and any discrepancies were discussed to reach a consensus (Supplemental Material; Appendices 1 and 2).
The Newcastle Ottawa Scale 20 consists of 3 domains: selection (4 items, 4 points), comparability (1 item, 2 points), and outcomes (3 items, 3 points). The selection domain consists of the representativeness of the cohort, selection of the non-cohort group, ascertainment of exposure, and presence of outcome at the start of the study. The comparability domain compares the cohorts based on design or analysis. The outcomes domain consists of assessment of outcome, follow up times, and attrition rate. The overall quality is based off the number of points in each domain, that is, 3 or 4 points in selection and 1 or 2 points in comparability and 2 or 3 points in outcomes is of good quality. Zero or 1 point in any domain results in poor quality. 22
The AXIS 21 tool consists of 5 domains (20 points): introduction (1 point), methods (10 points), results (5 points), discussion (2 points), and other (2 points). The tool evaluates the clarity of aims, appropriateness of design, sample representativeness, validity of measurements, handling of bias, statistical transparency, consistency and completeness of results, discussion quality, limitations, conflicts of interest, and ethical approval. Each point is scored as yes (=1) or no/unclear (=0). A total score is often converted to a percentage, with ≥70% indicating high quality, 60% to 69.9% fair quality, and <60% low quality. 23
Effect Measures
Anatomical location was recorded and reported as nominal data, whereas prevalence, incidence, and severity were continuous data.
Synthesis Methods
The extracted information was used to tabulate baseline characteristics, number of overuse and total injuries, prevalence, incidence per 1000 hours, severity, and anatomical location of overuse injuries in male and female ballet dancers.
If prevalence was recorded, they were extracted to be used in the analysis. In instances where it wasn’t reported, prevalence was calculated by dividing the number of overuse injuries by the total number of injuries in male and female ballet dancers. 24 The synthesised result was re-expressed as an odds ratio through a random effects meta-analysis model. Confidence intervals and significance were also calculated.
For the incidence per 1000 hours of overuse injuries the data was extracted from the studies, if present. Otherwise, they were calculated using the number of overuse injuries/(dance exposure (hours) × 1000). The incidence per 1000 hours were re-expressed as log (incidence rate ratio) = log (female incidence rate/male incident rate) with standard error. Furthermore, a 2 one-sided test was also performed to determine significance.
For the anatomical location of overuse injuries in males and females a log odds ratio and confidence interval were used to analyse the difference between sex in 3 different categories: lower extremity, upper extremity, and other. A random effects model was used to calculate a log odds ratio and confidence interval.
Meta-analysis was conducted on sex differences in the prevalence, incidence per 1000 hours and anatomical location of overuse injuries using random effects model on Jamovi 2.4.14. 25 Heterogeneity (tau2) was estimated using the restricted maximum-likelihood estimator for prevalence, incidence per 1000 hours and anatomical location of injuries. 26 Additionally, the Q-test for heterogeneity and the I2 statistic was also calculated. 27
Reporting Bias Assessments
A funnel plot was generated to visualise if there was any publication bias in the studies included in the meta-analysis for prevalence, incidence per 1000 hours and anatomical location of overuse injuries. Studentised residuals were used to assess whether studies may be outliers alongside rank correlation and regression tests. 28 Funnel plot asymmetry was checked using the standard error of the observed outcomes as a predictor.
Certainty Assessment
The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) tool 29 was utilised to assess the certainty in differences between the prevalence, incidence, and anatomical locations of overuse injuries in male and female ballet dancers. Two independent reviewers (R.R., A.W.) assessed the certainty of the results and reached a consensus on any conflicts through discussion.
Results
Study Selection
Initially 437 studies were identified, and 173 duplicates were removed resulting in a total of 264 studies to be screened. One hundred and ninety-seven studies were removed in the Title and Abstract screening phase resulting in 68 studies included for full text screening. Sixty-six studies were screened but the full text for 2 studies30,31 could not be retrieved. A further 57 studies were then removed resulting in 9 studies15,32 -39 that met the eligibility criteria. Following the full-text review, 2 additional studies40,41 were added through citation searching, resulting in a total of 11 studies (n = 1650 dancers) included in this review. The screening process and reasons for exclusion are reflected in the PRISMA diagram in Figure 1.
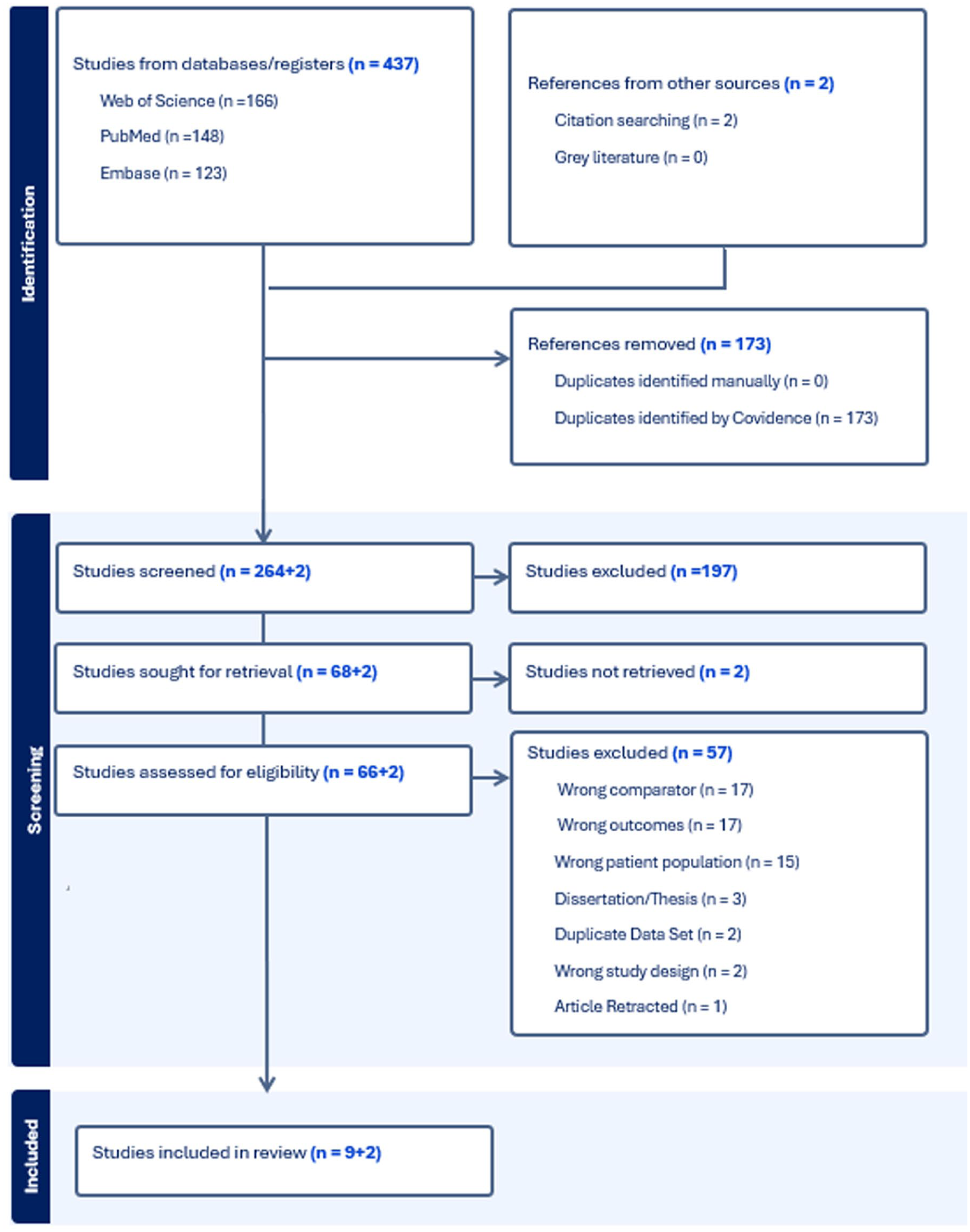
PRISMA flow diagram.
Baseline Characteristics of Included Studies
The 11 studies included both professional15,35,36,39 -41 and pre-professional ballet dancers,32 -34,37 with sample sizes ranging from 42 38 to 476. 33 One study 38 included both pre-professional and professional dancers. Four studies32 -34,37 had a higher proportion of female dancers in comparison to males. Sex-specific dance exposure wasn’t included in 4 studies.32,35,37,40 Furthermore, 5 studies15,32 -34,40 did not include age information of participants. Dance exposure varied greatly, ranging from 24 523 hours in pre-professionals 34 to 631 429 hours 15 in professionals. Table 3 depicts in detail all included studies’ characteristics.
Characteristics of Included Studies (n = 11). Descriptive Data on Study Design, Population Demographics, and Dance Exposure for Each Included Study.
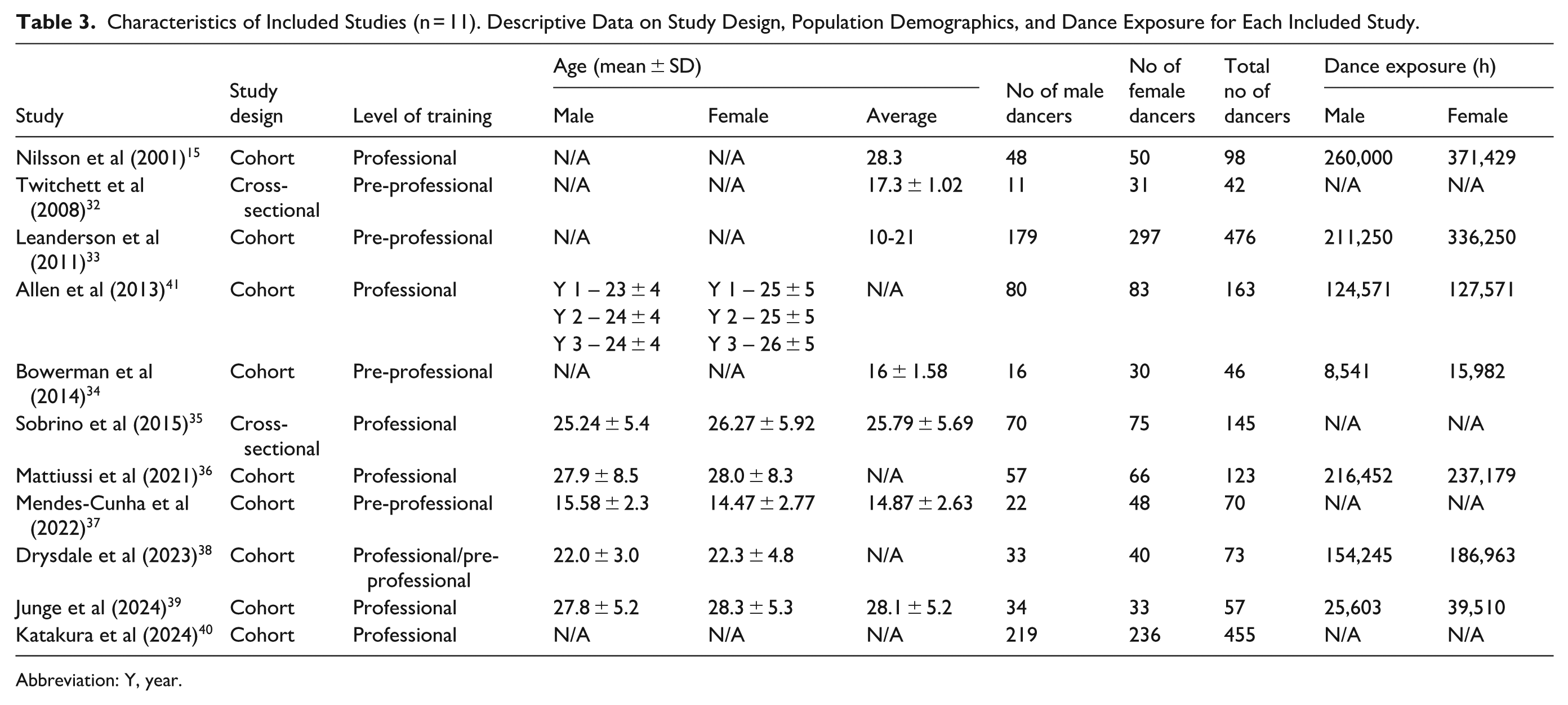
Abbreviation: Y, year.
Definition of Overuse Injuries
Across the studies, overuse injuries were defined as gradual onset15,32 -41 and not caused by an acute or traumatic event. The injuries were also defined as recurrent in type and location.15,35,37,38,41 Bowerman et al only studied overuse injuries. 34 The number of overuse and total injuries can be seen in Table 4.
Number of Overuse and Total Injuries. Summary of the Definition, Reporting, and Number of Overuse Injuries, Number of All Injuries, Stratified by Sex and Study.
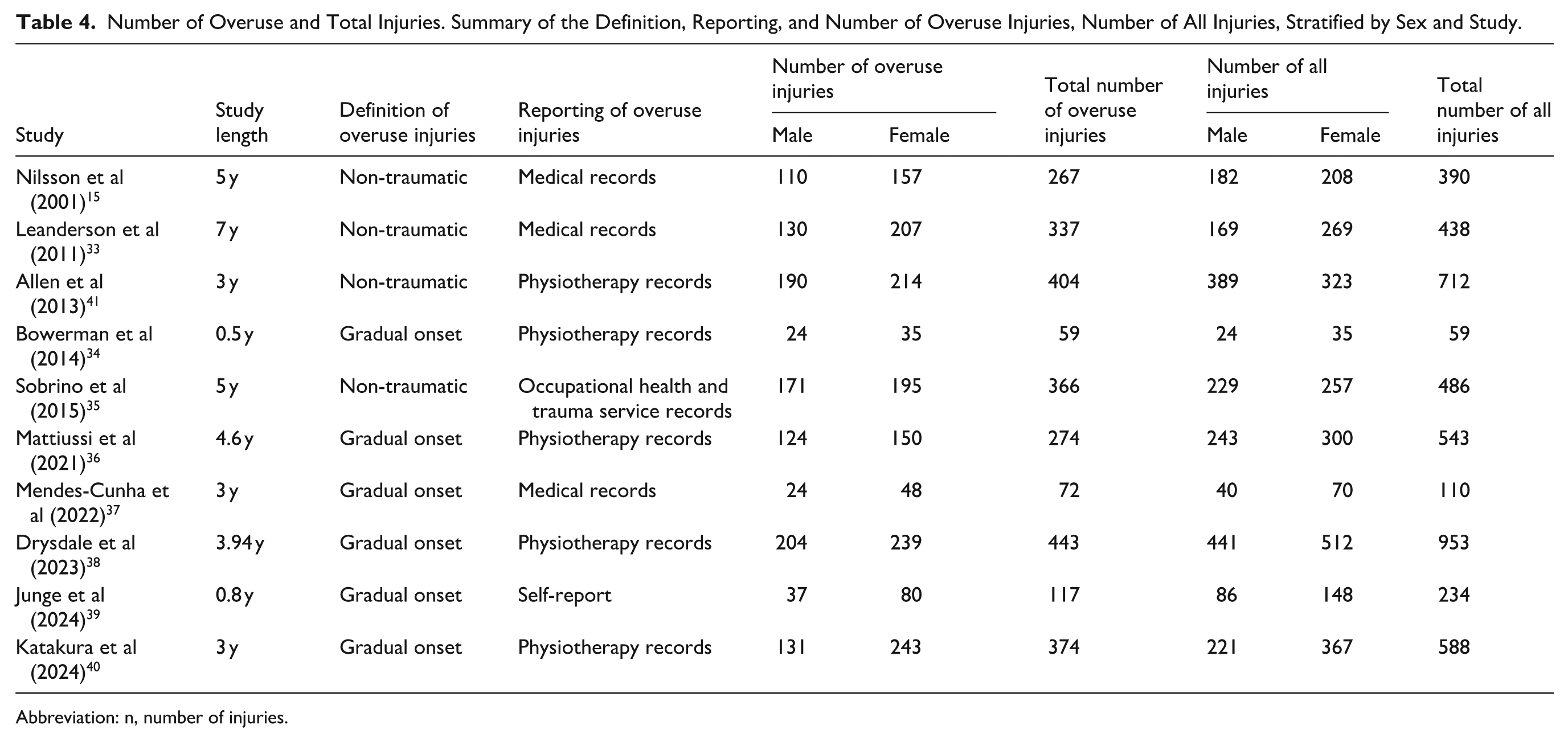
Abbreviation: n, number of injuries.
Risk of Bias and Quality Assessment
Nine studies15,33,34,36 -41 were evaluated using the Newcastle-Ottawa Scale (2000). The tool was modified so that items 2 and 5 were given a score of N/A due to the studies being single arm cohort studies, reducing the total points to 6. Eight studies15,33,34,36 -38,40,41 were deemed to be of good quality. One study 39 was deemed to be of poor quality. Junge et al 39 lost a point on items 3 and 6 as both the exposure and outcome data were collected through self-reporting. Furthermore, all studies except Allen et al 41 lost a point on item 4 – outcome of interest present at the start of the study; only Allen et al 41 explicitly stated that there were no injuries present at the start of the study.
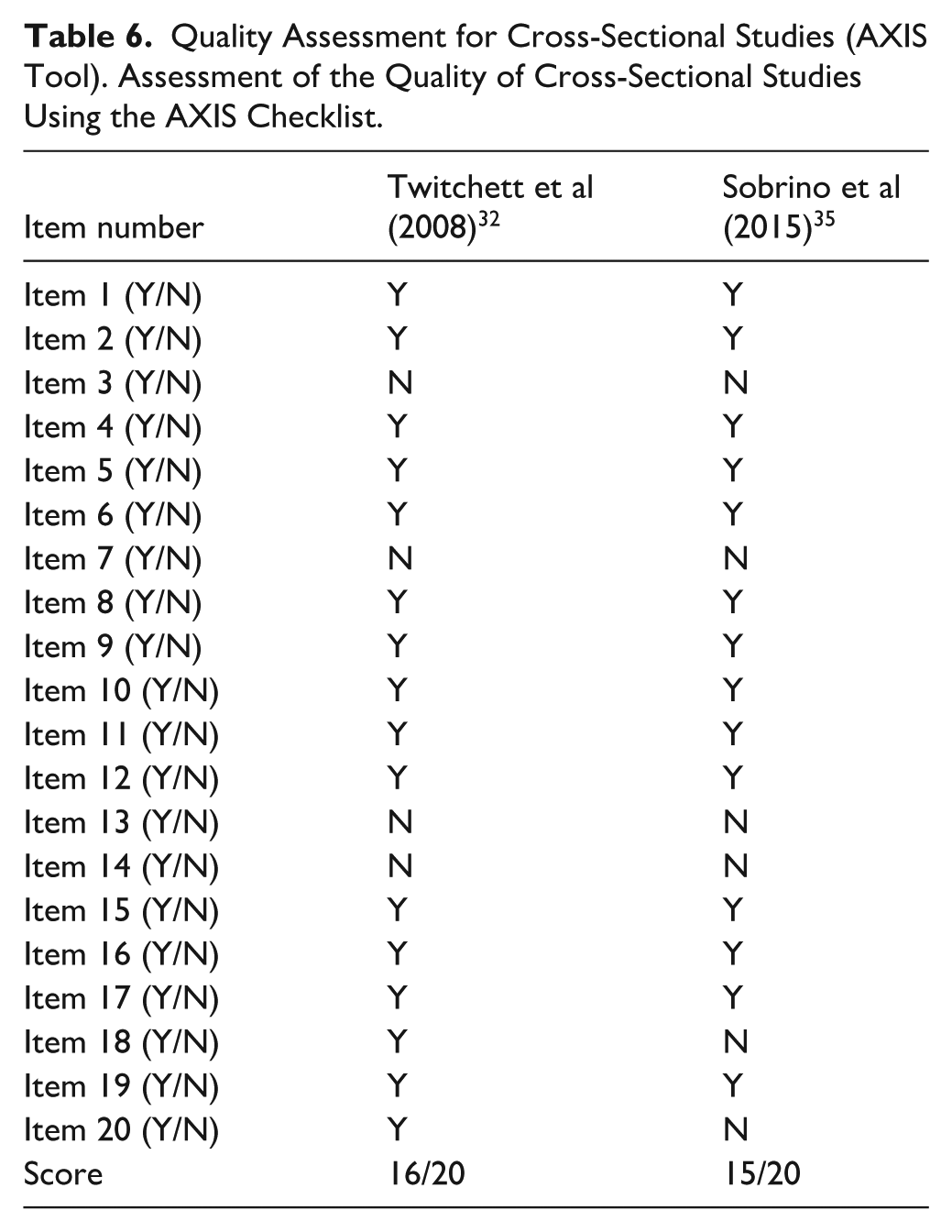
Two studies32,35 were assessed using the AXIS tool. The scores from the tool indicated that there were clear aims and objectives, and it also reflects that the study had strengths in design and result presentation. Both studies were of high quality as the scores are more than 70%. However, the tool also highlighted areas of the studies which was lacking such as justification of the sample size (item 3), selection process (item 6), and discussion of limitations (item 18). There was also a lack of information on funding sources (items 19) in both studies, but there was no information on conflict of interest (item 20) in Sobrino et al. 35 Furthermore, no information was present regarding non-responders (items 7, 13, and 14) in both studies (Tables 5 and 6).
Quality Assessment for Cohort Studies (Newcastle-Ottawa Scale). Appraisal of Methodological Quality of Cohort Studies Included in the Review.
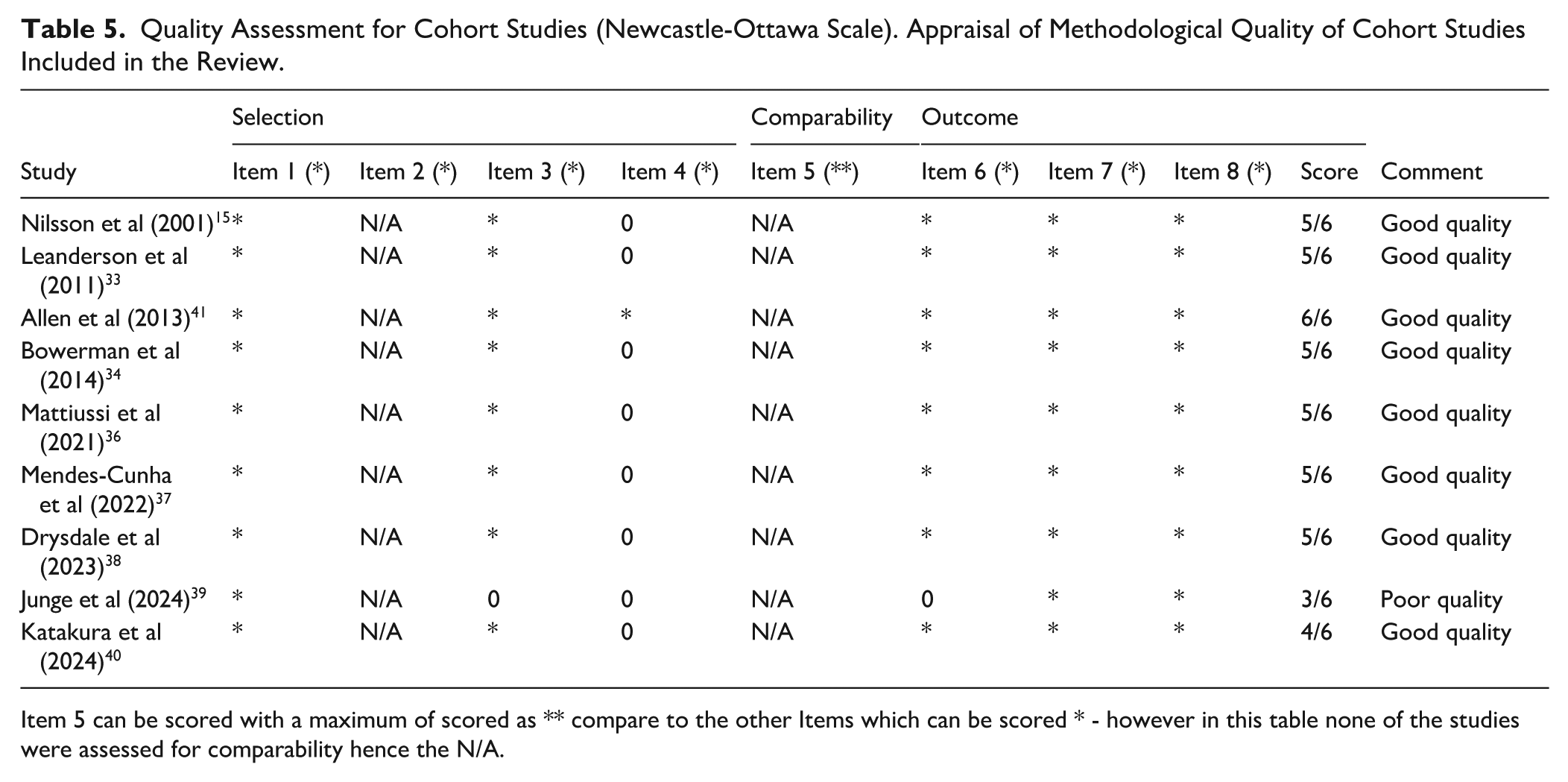
Item 5 can be scored with a maximum of scored as ** compare to the other Items which can be scored * - however in this table none of the studies were assessed for comparability hence the N/A.
Quality Assessment for Cross-Sectional Studies (AXIS Tool). Assessment of the Quality of Cross-Sectional Studies Using the AXIS Checklist.
Prevalence
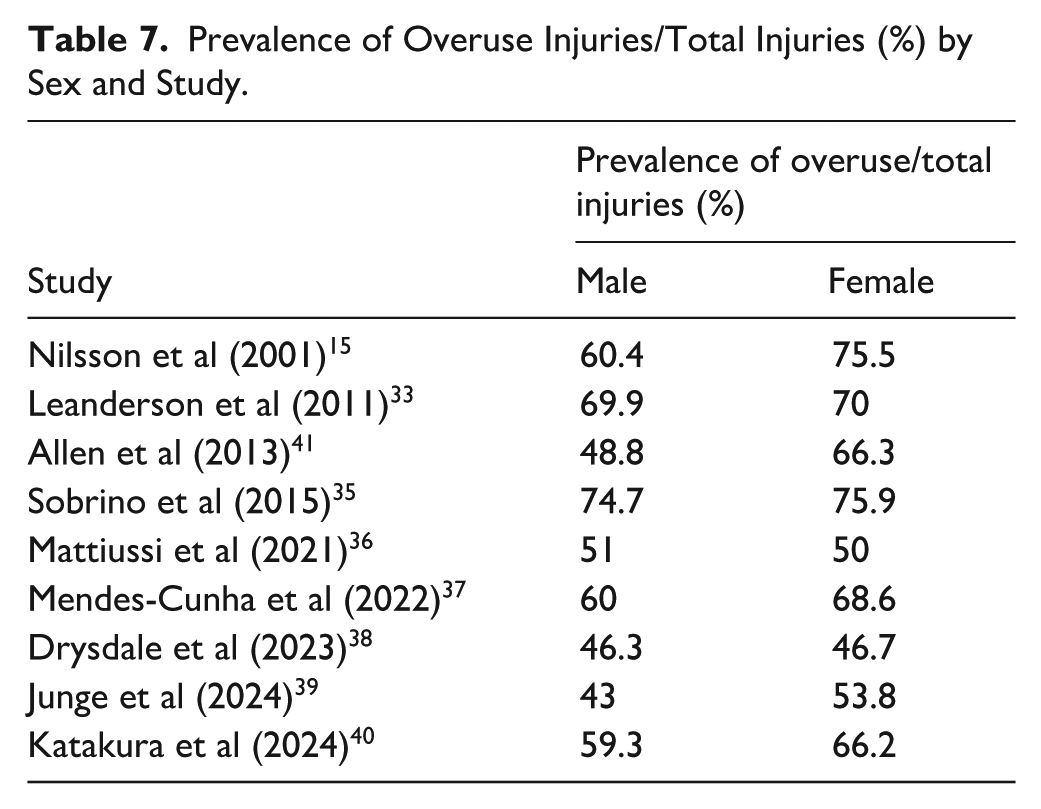
The prevalence of overuse injuries was calculated as a proportion over the total number of injuries from 9 studies.15,32 -37,40,41 This can be seen in Table 7. The overall sample consisted of professional (n = 1051) and pre-professional ballet dancers (n = 634). Drysdale et al 38 studied both professional and pre-professional dancers (n = 73). There appears to be a consistent pattern across most of the studies; the prevalence of overuse injuries was higher in female dancers in comparison to males across the studies except in Leanderson et al 33 and Mattiussi et al. 36
Prevalence of Overuse Injuries/Total Injuries (%) by Sex and Study.
A total of 9 studies15,32 -37,40,41 were initially included in the analysis using a random effect model. The observed log odds ratios ranged from −0.0412 to 0.7209, with the majority estimates being positive. The estimated average log odds ratio based on the random-effects model was = 0.2347 (95% CI: 0.0418-0.4276), and the average outcome differed significantly from 0 (z = 2.3844, P = .0171).
According to the Q-test, the true outcomes appear to be heterogeneous (Q(8) = 17.8674, P = .0222, tau2 = 0.0447, I2 = 54.5050%). A 95% prediction interval for the true outcomes is given by −0.2225 to 0.6920.
An examination of the studentised residuals revealed that 1 study (Allen et al 41 ) had a value larger than ±2.7729 and may be a potential outlier in the context of this model. The rank correlation and the regression test results were P = .6122 and P = .7681, respectively.
Therefore, the meta-analysis was conducted again after removing the identified outlier. 41 The revised forest plot can be seen in Figure 2 with 8 studies included.15,32 -37,40
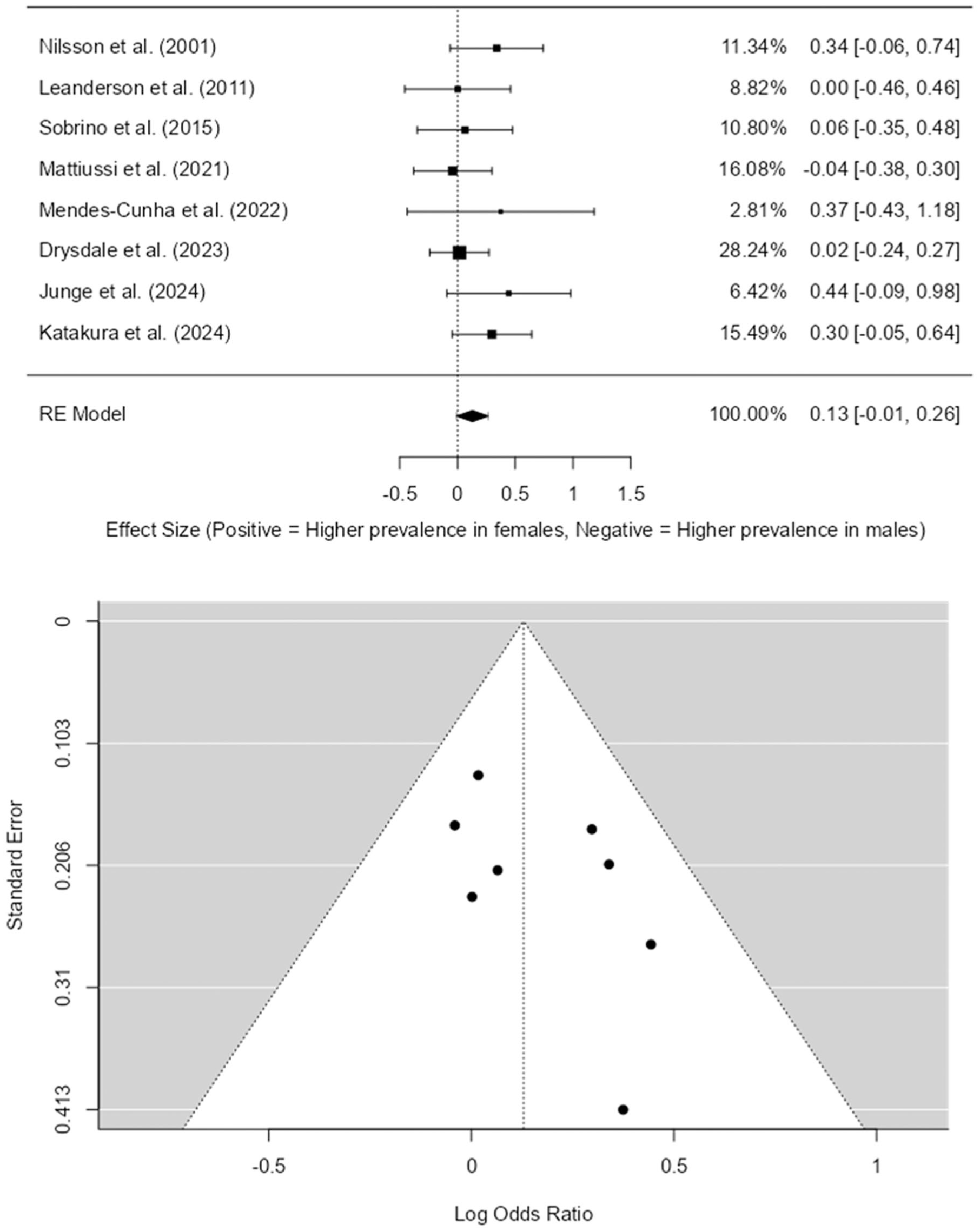
Forest plot and funnel plot – prevalence of overuse injuries in female versus male ballet dancers (outlier removed).
The observed log odds ratios ranged from −0.0412 to 0.4434, with many estimates being positive. The estimated average log odds ratio based on the random-effects model was = 0.1289 (95% CI: −0.0068 to 0.2645). Therefore, the average outcome did not differ significantly from 0 (z = 1.8618, P = .0626).
According to the Q-test, there was no significant amount of heterogeneity in the true outcomes (Q(7) = 5.7503, P = .5692, tau2 = 0.0000, I2 = 0.0000%).
An examination of the studentised residuals revealed that none of the studies had a value larger than ±2.7344 and hence there was no indication of outliers in the context of this model. Neither the rank correlation nor the regression test indicated any funnel plot (Figure 2) asymmetry (P = .2751 and P = .2023, respectively).
Incidence
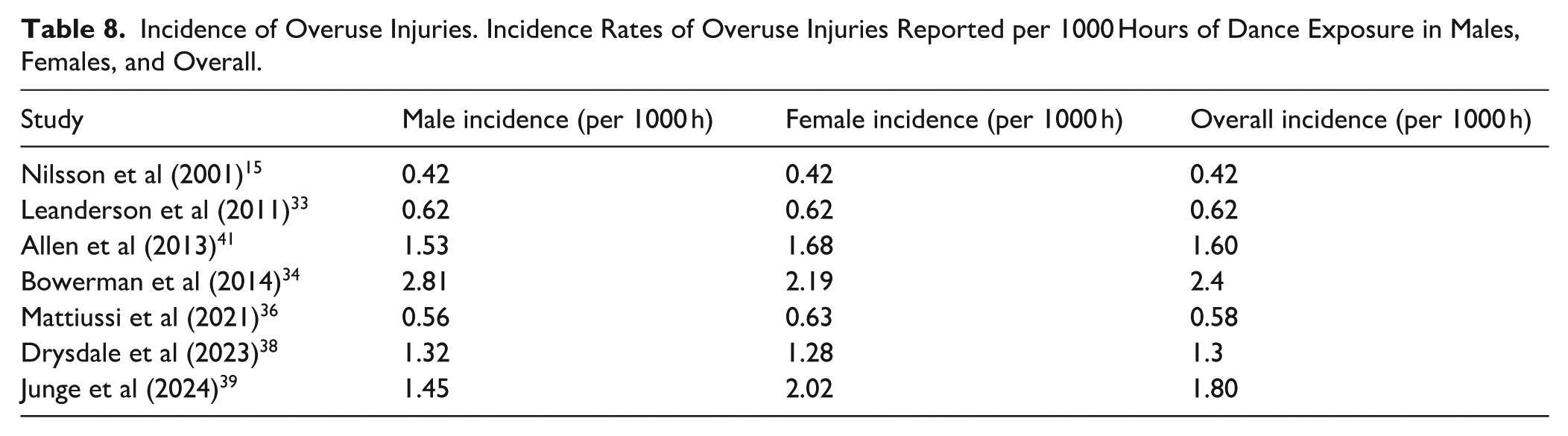
There was no consistent pattern amongst the studies in the incidence per 1000 hours; in 4 studies33,36,39,41 females had higher incidence, in 2 studies34,38 males had higher incidence, and in 1 study 15 there was no difference in the incidence. The incidence per 1000 hours in males, females, and overall is reported in Table 8.
Incidence of Overuse Injuries. Incidence Rates of Overuse Injuries Reported per 1000 Hours of Dance Exposure in Males, Females, and Overall.
Meta-analysis of incidence as log (incidence rate ratios) can be seen in Figure 3 as a forest plot.
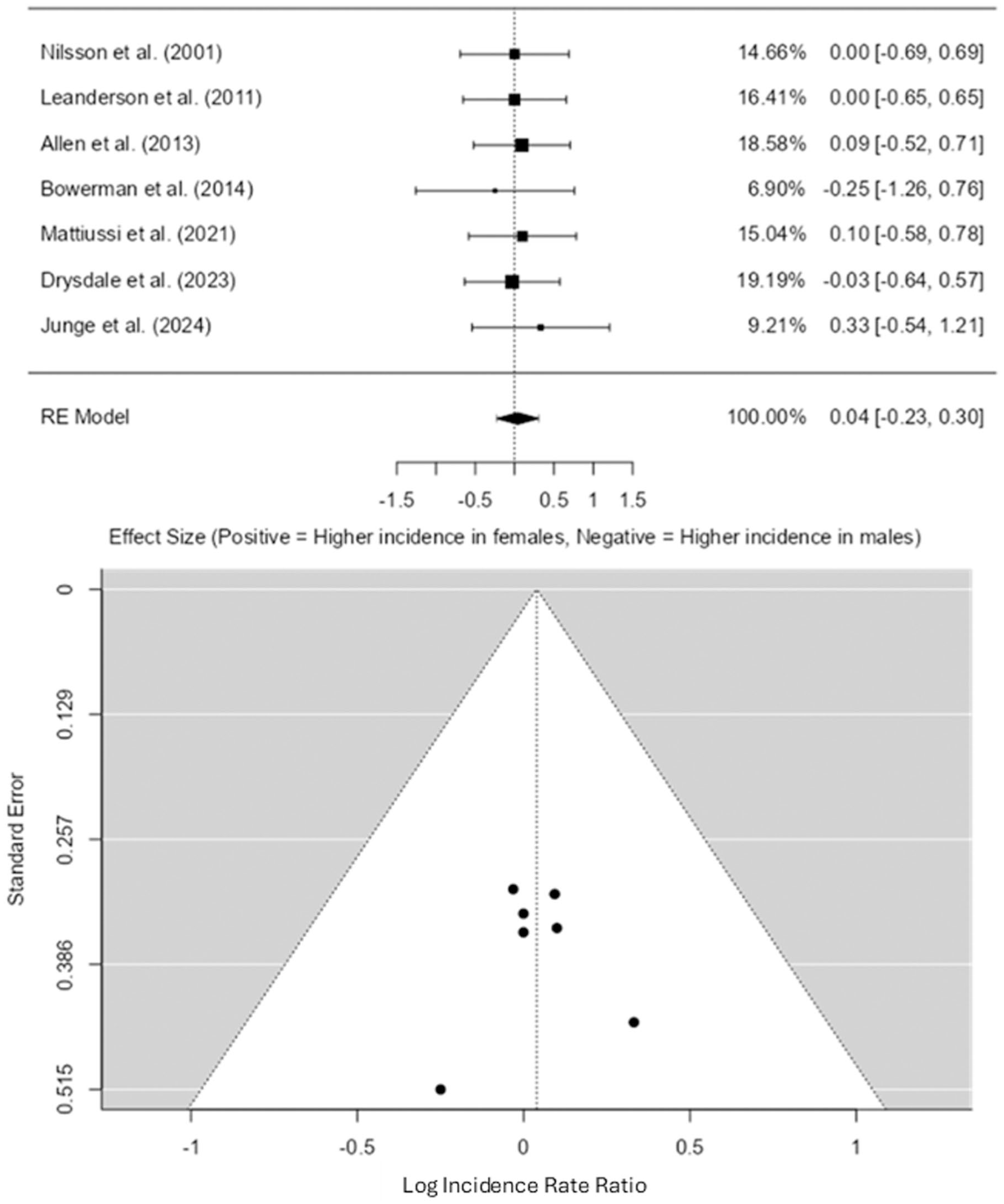
Forest plot and funnel plot – incidence of overuse injuries in female versus male ballet dancers.
A total of 7 studies15,33,34,36,38,39,41 were used in the random-effect meta-analysis. The log (IRR) ranged from −0.23 to 0.30. The overall effect estimate was 0.0398 (95% CI: −0.225 to 0.305) which was not statistically significant (P = .769).
The 2 one-sided tests, using bounds of −0.5 to 0.5 showed that equivalence test was significant (z = −3.402, P = .000334). The null hypothesis test was non-significant (z = 0.294, P = .769). This indicates that the observed effect is statistically not different from 0 and statistically equivalent to 0. Furthermore, according to the Q-test, there was no heterogeneity observed across the studies (Q(6) = 0.882, P = .990, tau2 = 0, I2 = 0%).
The funnel plot (Figure 3) did not reveal any signs of publication bias. This is supported by the Kendall’s tau (τ = 0.048, P = 1.000) and Egger’s regression intercept (−0.057, P = .955) test, which indicated no asymmetry in the distribution of effect sizes.
Severity
The severity of injuries was recorded in 2 studies32,41 (Table 9). Twitchett et al, 32 found that pre-professional female dancers experienced a greater number of days being lost due to overuse injuries compared to their male counterparts. Contrastingly, Allen et al, 41 reported that professional male ballet dancers experienced a longer duration of time lost to injury compared to females during the first and second year of the observation period. However, in the third year, female dancers had a greater number of days lost to overuse injuries.
Severity of Overuse Injuries. Average Time Loss Due to Overuse Injuries, Stratified by Sex.
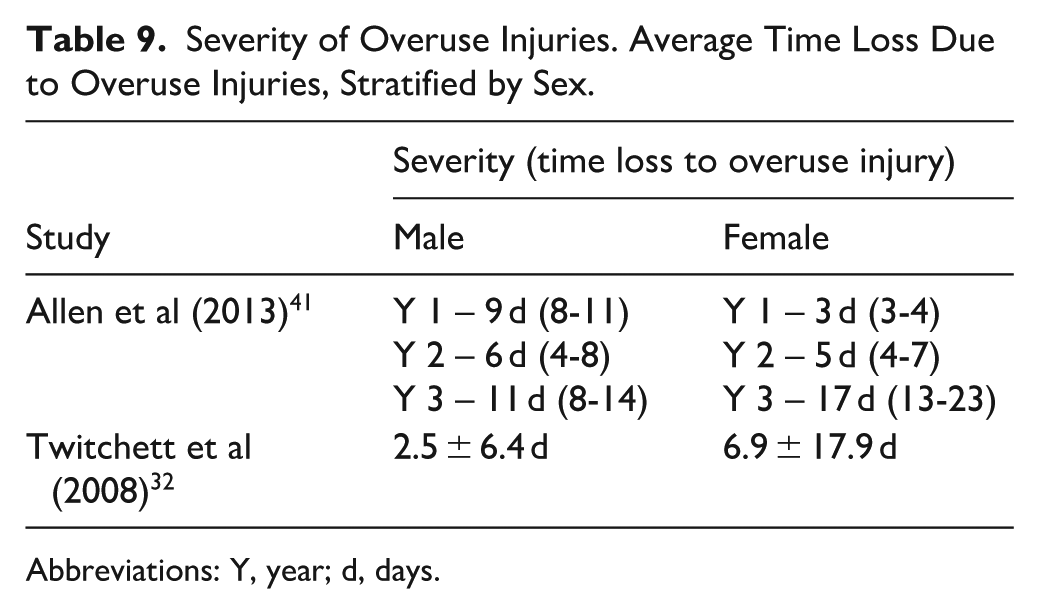
Abbreviations: Y, year; d, days.
Due to the limited number of studies, the methodological difference in reporting the severity, a range in 1 study and the standard deviation in another, they could not be pooled for further analysis.
Anatomical Location
Five studies15,33,35,37,38 reported on the anatomical location of overuse injuries and separated them by sex. To allow a synthesised manner of expressing the location, 3 major categories were formed in this review to describe the location of injuries. Lower extremity refers to injuries from the hip down to the feet. Upper extremity injuries were considered from the shoulder to the hands. The final category, “other” consisted of lower back, upper back, and neck injuries (Table 10).
Anatomical Location of Overuse Injuries. Distribution of Overuse Injuries by Anatomical Region and Sex.
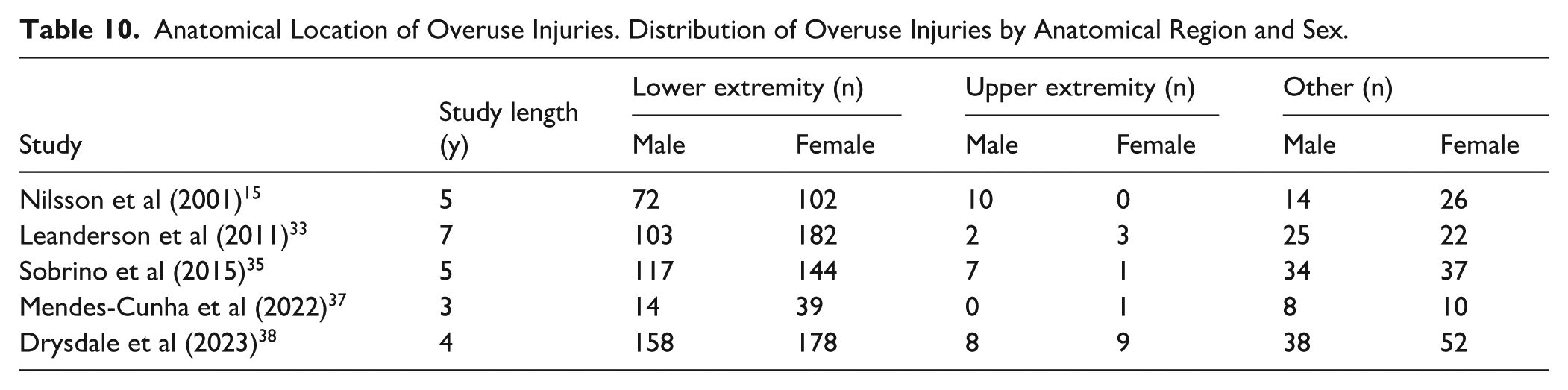
The foot and ankle complex were the most injured region in the “lower extremity” and the lower back was the most affected region in the “other” category. The least affected region of overuse injuries across all the studies15,33,35,37,38 was the upper extremity category, mainly in the shoulder.
Meta-analysis was conducted using a log odds ratio between females and males to explore significant differences at any of the 3 categories.
The first category was the lower extremity, and the results can be seen in Figure 4. The observed log odds ratios ranged from −0.1630 to 0.7061, with the majority of estimates being positive. The estimated average log odds ratio based on the random-effects model was = 0.2587 (95% CI: −0.0717 to 0.5891). The average outcome did not differ significantly from 0 (z = 1.5347, P = .1249). This indicates that there was no significant difference between females and males regarding the likelihood of overuse injuries in the lower extremities.
Forest plot and funnel plot – lower extremity overuse injuries in females versus males.
The Q-test for heterogeneity was not significant, but some heterogeneity may still be present in the true outcomes (Q(4) = 5.7378, P = .2196, tau2 = 0.0489, I2 = 35.1286%). A 95% prediction interval for the true outcomes is given by −0.2862 to 0.8036.
An examination of the studentised residuals revealed that none of the studies had a value larger than ±2.5758 and hence there was no indication of outliers in the context of this model. Neither the rank correlation nor the regression test indicated any funnel plot (Figure 4) asymmetry (P = .4833 and P = .1113, respectively).
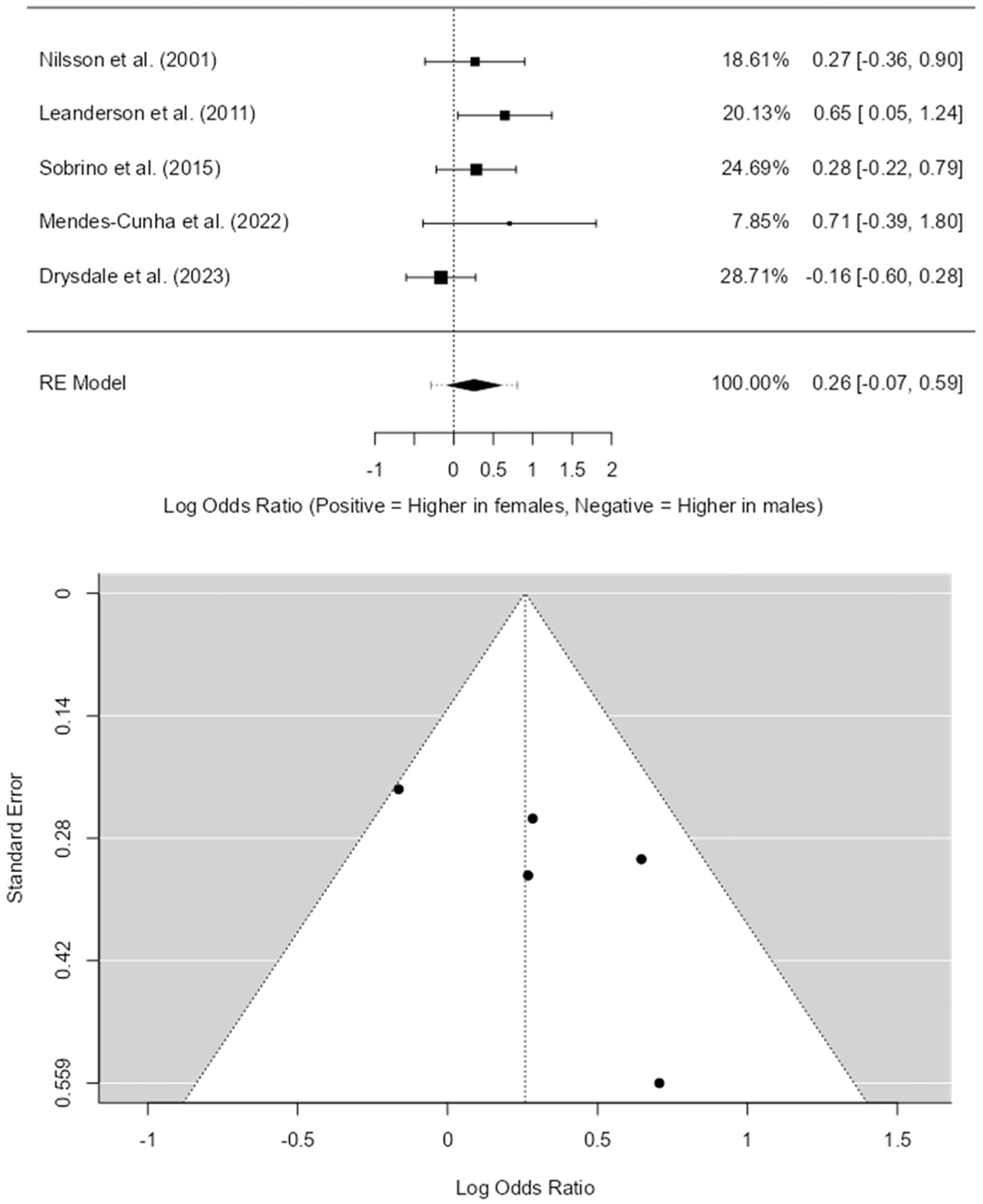
The second category was the upper extremity (Figure 5). The observed log odds ratios ranged from −3.4403 to 0.3102. The estimated average log odds ratio based on the random-effects model was = −0.8491 (95% CI: −2.0730 to 0.3748). The average outcome did not differ significantly from 0 (z = −1.3597, P = .1739). Therefore, whilst the average log odds ratio is negative, suggesting females may have fewer overuse injuries in the upper extremity than males, this difference is not statistically significant.
Forest plot and funnel plot – upper extremity overuse injuries in females versus males.
According to the Q-test, there was no significant amount of heterogeneity in the true outcomes (Q(4) = 7.7007, P = .1032, tau2 = 0.8837, I2 = 48.2250%). A 95% prediction interval for the true outcomes was given by −3.0610 to 1.3628.
An examination of the studentised residuals revealed that none of the studies had a value larger than ±2.5758 and hence there was no indication of outliers in the context of this model. Neither the rank correlation nor the regression test indicated any funnel plot (Figure 5) asymmetry (P = .2333 and P = .2367, respectively).
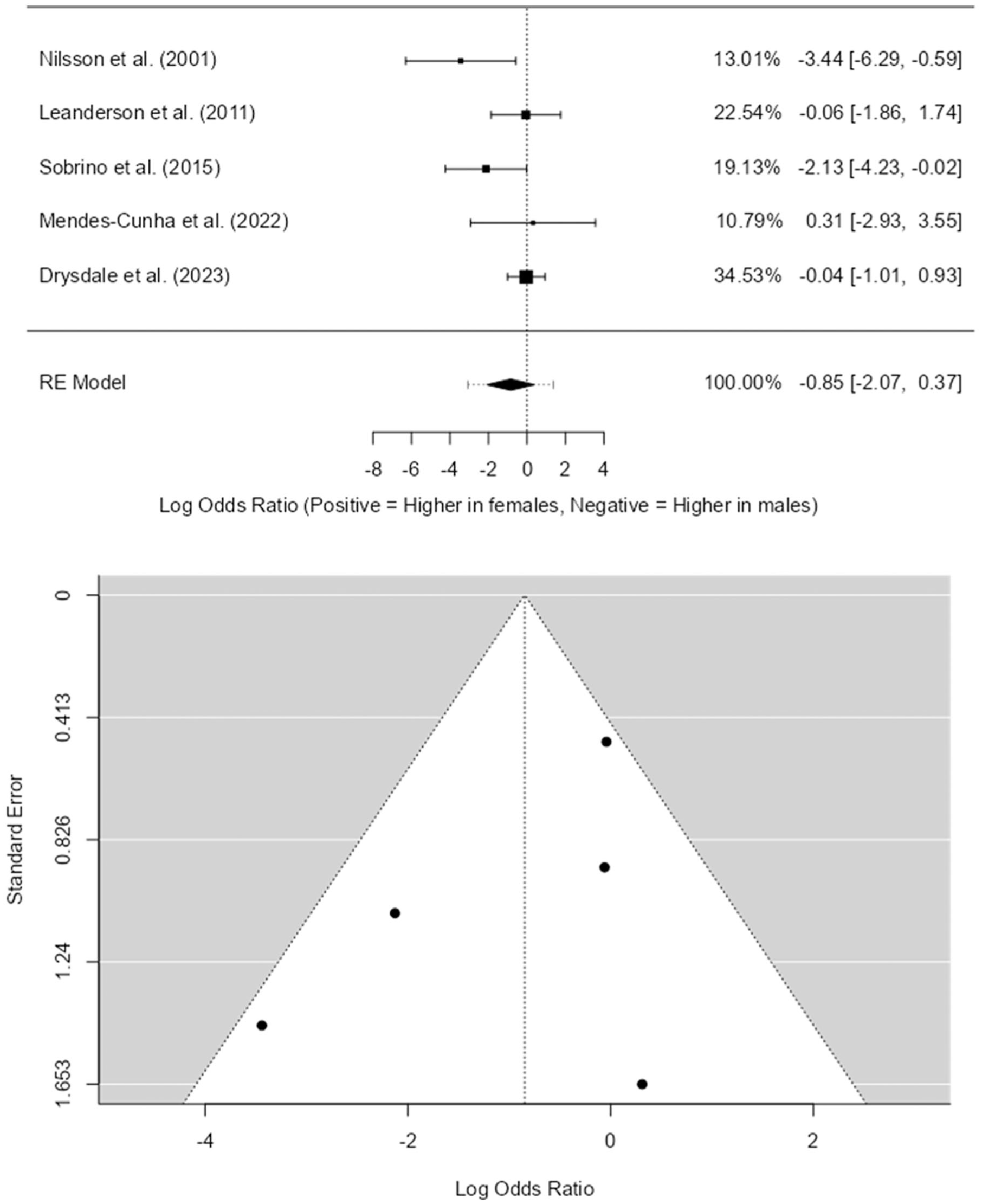
The final category was “other,” and the results can be seen in Figure 6. The observed log odds ratios ranged from −0.8267 to 0.4008. The estimated average log odds ratio based on the random-effects model was = −0.1247 (95% CI: −0.5444 to 0.2950). The average outcome did not differ significantly from 0 (z = −0.5825, P = .5602). Therefore, although females are slightly less likely than males to experience overuse injuries in the “other” regions, this difference was not significant.
Forest plot and funnel plot – “other” overuse injuries in females versus males.
The Q-test for heterogeneity was not significant, but some heterogeneity may still be present in the true outcomes (Q(4) = 8.5703, P = .0728, tau2 = 0.1185, I2 = 53.8343%). A 95% prediction interval for the true outcomes is given by −0.9192 to 0.6697.
An examination of the studentised residuals revealed that none of the studies had a value larger than ±2.5758 and hence there was no indication of outliers in the context of this model. Neither the rank correlation nor the regression test indicated any funnel plot (Figure 6) asymmetry (P = .8167 and P = .3044, respectively).
Certainty Assessment
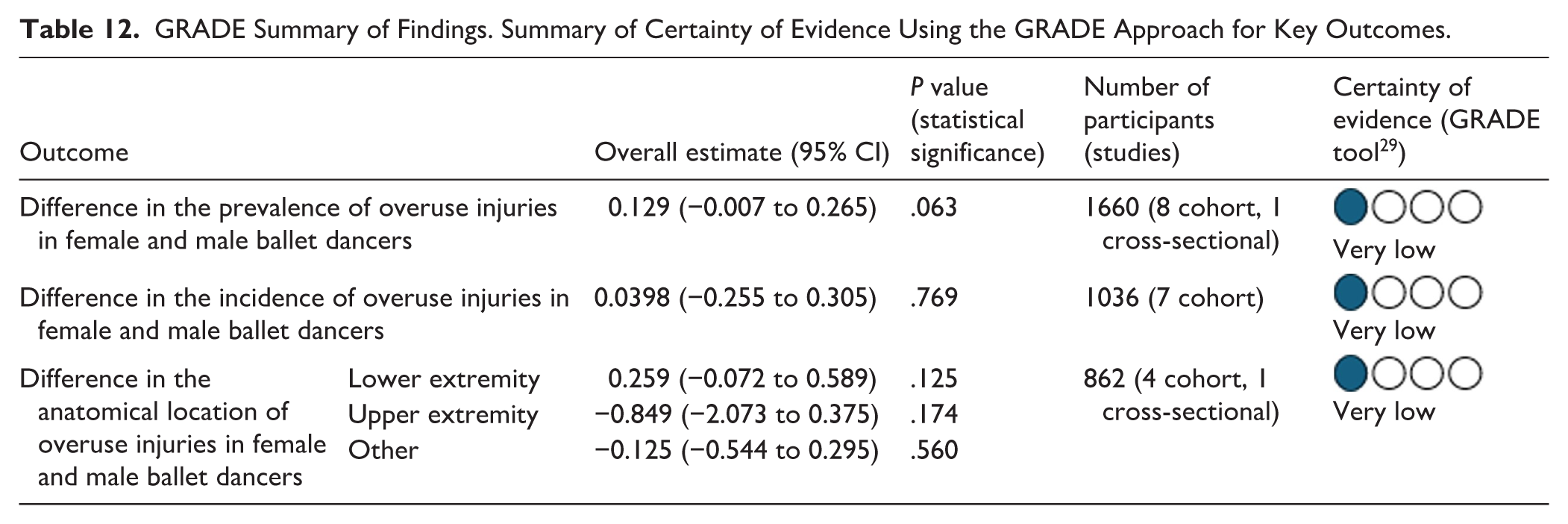
Certainty was assessed using the GRADE tool 29 for all outcomes that were meta-analysed. The outcome initially started with a low score of ++ due to the included studies being cohort and cross-sectional studies which were observational. One point was deducted due to imprecision. No further points were reduced or added to the synthesised results. This resulted in a final certainty level of very low according to the GRADE tool for prevalence, incidence, and severity.
Summary of Findings
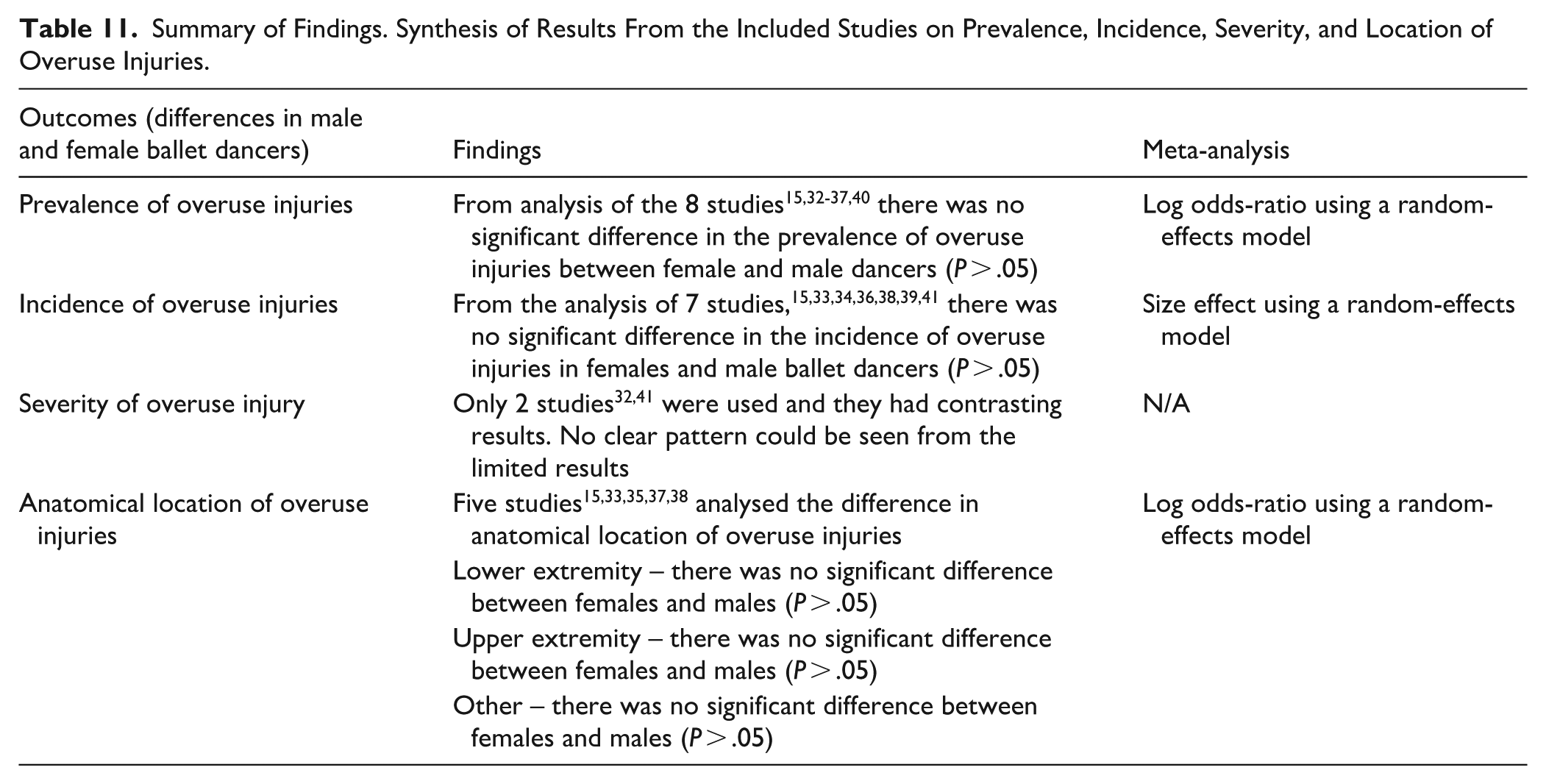
A summary of the main outcomes can be seen in Table 11. Meta-analysis of sex difference in prevalence, incidence, and anatomical location of overuse injuries in female and male ballet dancers can be seen in the GRADE summary table (Table 12).
Summary of Findings. Synthesis of Results From the Included Studies on Prevalence, Incidence, Severity, and Location of Overuse Injuries.
GRADE Summary of Findings. Summary of Certainty of Evidence Using the GRADE Approach for Key Outcomes.
Discussion
We critically reviewed the evidence published from 2000 onwards for differences in prevalence, incidence, severity, and anatomical location of overuse injuries between male and female ballet dancers. We included pre-professional and professional dancers only. Overall, the results indicated that there was no significant difference in the prevalence, incidence per 1000 hours and anatomical location of overuse injuries in females and male ballet dancers. Severity could not be meta-analysed due to limited number of studies.
Sex differences in overuse injury prevalence were analysed with a log odds ratio in 8 studies.15,32 -37,40 Meta-analysis showed that there was no significant difference in the prevalence of overuse injuries between males and females. This is in contrast with previous research, 9 that reported females having significantly higher prevalence of overuse injuries. However, Smith et al 9 included participants with varying levels of training, from amateurs to professionals. Our analysis revealed a consistent pattern across most of the studies; the prevalence of overuse injuries was higher in female dancers in comparison to males. However, meta-analysis did not find significant differences between sexes. This could imply that, more than intrinsic biological differences, common loading factors across both sexes, such as elevated training volumes, repetitive choreography, and accumulated mechanical stress may contribute more to increasing injury risk.
Incidence was included in 7 studies.15,33,34,36,38,39,41 Meta-analysis indicated that there was no significant difference in the incidence of overuse injuries between males and females. This suggests that both sexes develop new overuse injuries at similar rates over time. Despite established sex-based physiological differences, this parity may be explained by the standardised training conditions in ballet, where both male and female dancers are exposed to similarly high volumes of repetitive loading and exposure. 8
Severity was only included in 2 studies32,41 and showed no clear pattern. As there are no previous reviews which focussed solely on incidence of overuse injuries between male and female dancers, it is challenging to check the consistency and appropriateness of our results to current body of knowledge. However, this indicates the lack of literature and the need for more research regarding this specific epidemiological outcome.
Meta-analysis of the anatomical location of injuries included data from 5 studies.15,33,35,37,38 Results showed that there were no significant differences in the lower extremity, upper extremity, or “other” categories. However, it was observed that the foot and ankle injuries were the most affected region for overuse injuries in ballet dancers, consistent with previous research.4,11 The upper extremity region was the least affected in both male and female dancers, although males did have higher overuse injuries in this region, albeit not statistically significant. Lower extremity injuries, especially in the foot and ankle region 4 are likely due to technical components typical of the discipline, like dancing en pointe and jumps. Dancing en pointe is a classical feature of female ballet dancers whilst male dancers have roles of lifting and carrying female dancers, so require considerably more upper body strength and training reflected by male dancers experiencing more upper extremity injuries. Furthermore, Twitchett et al 42 found that ballet dancers spent jumping 4.99 seconds/minute when performing, indicating the burden on the lower limb and so making it more likely to be affected by overuse injuries, highlighting the importance of incorporating strength-specific training into their conditioning programmes. 43
Limitations
Overall, we identified a total of 11 studies15,32 -41 that focussed since 2000 on overuse injuries and sex differences. Future research would benefit from larger sample sizes and standardised methodologies for multiple epidemiological outcomes to reduce heterogeneity so that they can be analysed to their full extent and tested for significance.
The included studies15,32 -41 varied in their reporting of age and other baseline variables, and were frequently not distinguished by sex. No studies presented statistical comparisons of important characteristics like training volume, years of experience, or exposure hours between males and females, and 5 studies15,32 -34,40 completely excluded participant age. The absence of consistent demographic and exposure reporting constrains the interpretation of observed disparities in injury prevalence and hinders the adjustment for potential confounding variables. To ensure more thorough analyses and better understanding of any sex-related injury patterns, future research should guarantee thorough and sex-disaggregated reporting of participant variables, such as age, training load, and exposure measures.
Furthermore, the certainty of outcomes was found to be very low and therefore it is reasonable to state that findings should be taken with caution and so limits the confidence in the conclusion. This is important as the ability of this review is limited in terms of clinical implications such as influencing guidelines and prevention strategies in ballet dancers. This also signifies the need for further high-quality research on this topic.
Additionally, although it was not one of the outcomes of this study, future reviews could also analyse differences according to sex and level to increase the external validity of the current findings.
Practical and Clinical Applications and Implication
While the results of this review do not support prioritizing sex-specific traits at this point, additional research involving larger and more comprehensive datasets may help determine if such differences are present. At present, strategies for preventing and assessing injuries should mainly concentrate on common mechanical and training load elements that impact all dancers, while also being conscious of the importance of sex-specific factors.
These results can inspire improved clinical awareness and early screening by healthcare providers and dance educators, facilitating timely treatments that reduce injury incidence and improve performance lifespan. 41
Conclusion
This review found that there was no significant difference in the prevalence and incidence of overuse injuries between female ballet dancers and male ballet dancers (P > .05).
The most affected region of overuse injuries was found to be the foot and ankle complex in both male and female dancers. However, there was no significant difference in the anatomical location of overuse injuries between females and males. The results of our review should be interpreted with caution due to the very low certainty grade, and it is possible that future analyses will identify statistically significant sex differences as the number of high-quality research increases. Future studies should incorporate uniform methods in data collection which can allow further inferential analysis of other outcomes like severity. Long term longitudinal observations could also be conducted to understand the long-term impact of overuse injuries on male and female ballet dancers and how this might differ.
Supplemental Material
sj-docx-1-dmj-10.1177_1089313X251412479 – Supplemental material for Prevalence, Incidence, Severity, and Anatomical Location of Overuse Injuries in Male and Female Ballet Dancers: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-dmj-10.1177_1089313X251412479 for Prevalence, Incidence, Severity, and Anatomical Location of Overuse Injuries in Male and Female Ballet Dancers: A Systematic Review and Meta-Analysis by Rubaprthisan Rupendran, Arif Ahmad Wadud, Rosie Elizabeth Davis, Sophia Gita Taglia, Tobin Alexander Rusby and Manuela Angioi in Journal of Dance Medicine & Science
Footnotes
Acknowledgements
We would like to acknowledge all colleagues based at Sports and Exercise Medicine, William Harvey Research Institute, Queen Mary University of London.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon request. The protocol was registered on PROSPERO (ref: CRD420251104232).
Supplemental Material
Supplemental material for this article is available online.