
Abstract
Background:
Achilles tendinopathy can be a devastating condition in ballet dancers. Initial medical evaluation is frequently conducted by generalist physicians, who may lack the perspective of dance and sports medicine focused training and often prescribe complete rest for chronic overuse injuries. In order to provide targeted information about Achilles tendinopathy and the unique needs of elite athletes, such as ballet dancers, we designed an educational intervention that covers relevant anatomy, physiology, biomechanics, clinical presentation and evaluation, and recommendations for initial treatment and sub-specialty referral. The objectives of this study were to determine baseline understanding of Achilles tendinopathy by generalist physicians and to evaluate the efficacy of an educational intervention on their knowledge.
Methods:
This was a prospective pre- post-test study, to measure improvement in knowledge about Achilles tendinopathy. Emergency Medicine and Primary Care physicians participated in an educational intervention with didactic and hands-on components. Data were analyzed using a two-tailed t-test.
Results:
Twenty generalist physicians participated. There was significant improvement in their knowledge of Achilles tendinopathy for all our educational objectives (Pre-test: 59% correct answers; post-test: 79% correct answers; P < .0001; 95% CI: 6.32-10.78.).
Conclusions:
A brief educational intervention leads to increased knowledge of Achilles tendinopathy in generalist physicians. By increasing awareness of Achilles tendinopathy through a standard educational model, we propose that our curriculum can be portable and accessible to all health care providers who encounter dancers and other athletes with Achilles tendinopathy and may serve as a model for expanded education to generalists about other conditions commonly encountered in ballet dancers.
Keywords
Key Points
Dance athletes who suffer exacerbation of a chronic overuse injury may seek initial care from generalist physicians who often advise prolonged rest and cessation of dance.
Generalist physicians may not have adequate training to manage elite dance athlete chief complaints such as acute exacerbation of chronic Achilles tendinopathy.
A brief didactic and hands-on workshop improves knowledge and awareness for generalist physicians on evaluation and management of Achilles tendinopathy exacerbation in elite athletes until definitive care is arranged.
Introduction
The Achilles tendon is the largest and strongest in the human body and accounts for many incapacitating overuse injuries in dancers and other professional and recreational athletes.1,2 As a category, overuse injuries account for 40% to 50% of injuries to dancers, however, data on isolated Achilles tendinopathy are not readily available. 3 Ballet dancers who suffer from the spectrum of Achilles tendon injuries often present first to generalists, such as Emergency Medicine (EM) or Primary Care (PC) physicians, who may not be familiar with these conditions. We believe this may be most concerning for patients for whom the symptoms may be incapacitating for their professional careers.4 -7 Despite the high prevalence of these conditions, there is wide variability in the level of understanding of the evaluation and initial treatment by generalist physicians, especially from a dance or sports medicine perspective. The default recommendation “to withdraw completely from the activity that caused the injury” is impractical in this patient group.4 -8
In order to provide necessary information about the spectrum of Achilles tendinopathy and issues facing professionals and trainees who suffer from them, we developed a brief educational intervention for generalist physicians who are likely to be the first medical providers to evaluate acute exacerbations of these injuries. The intervention begins with a review of anatomy, physiology, biomechanics, clinical presentation and evaluation, and recommendations for initial treatment and referral strategies when evaluating athletes such as ballet dancers, in whom the condition is common. The objectives of this study were to: (1) determine baseline understanding of Achilles tendinopathy, including anatomy, physiology, risk factors, clinical evaluation and intial management by generalist physicians; (2) evaluate the efficacy of a didactic and hands-on practical educational intervention on their knowledge of evaluation and appropriate initial management.
Methods
Study Setting and Participants
The study took place at the Los Angeles County Harbor-UCLA Medical Center, a 450-bed public teaching hospital. Participants were trainees in the Department of Emergency Medicine, including PGY-2 and PGY-3 residents from EM, and PGY-3 PC residents from Internal Medicine and Family Medicine.
Study Design
This was a prospective quasi-experimental educational research study design using a pre- and post-test to measure improvement in knowledge about Achilles tendinopathy and its initial evaluation and treatment. Participants were required to participate in the educational activity, as it was a component of the residency curriculum, however, they could opt-out of having their individual data analyzed. The study was determined to be exempt by the Institutional Review Board at the Los Angeles Biomedical Institute at Harbor-UCLA Medical Center.
Intervention
Objective test questions were developed by consensus of content experts and pilot tested for clarity and accuracy by board certified EM physicians. A pre- and post-test (Supplemental File 1) were created using the aforementioned questions that addressed the teaching objectives of the session. A 60-minute educational session was prepared by the authors and included basic information on anatomy and physiology, biomechanics, injury patterns, clinical evaluation, and early treatment priorities. The format combined a didactic component using Powerpoint slides (Supplemental File 2), followed by an interactive experience that enabled participants to practice examination and simple initial rehabilitation techniques on themselves and others (Figure 1).
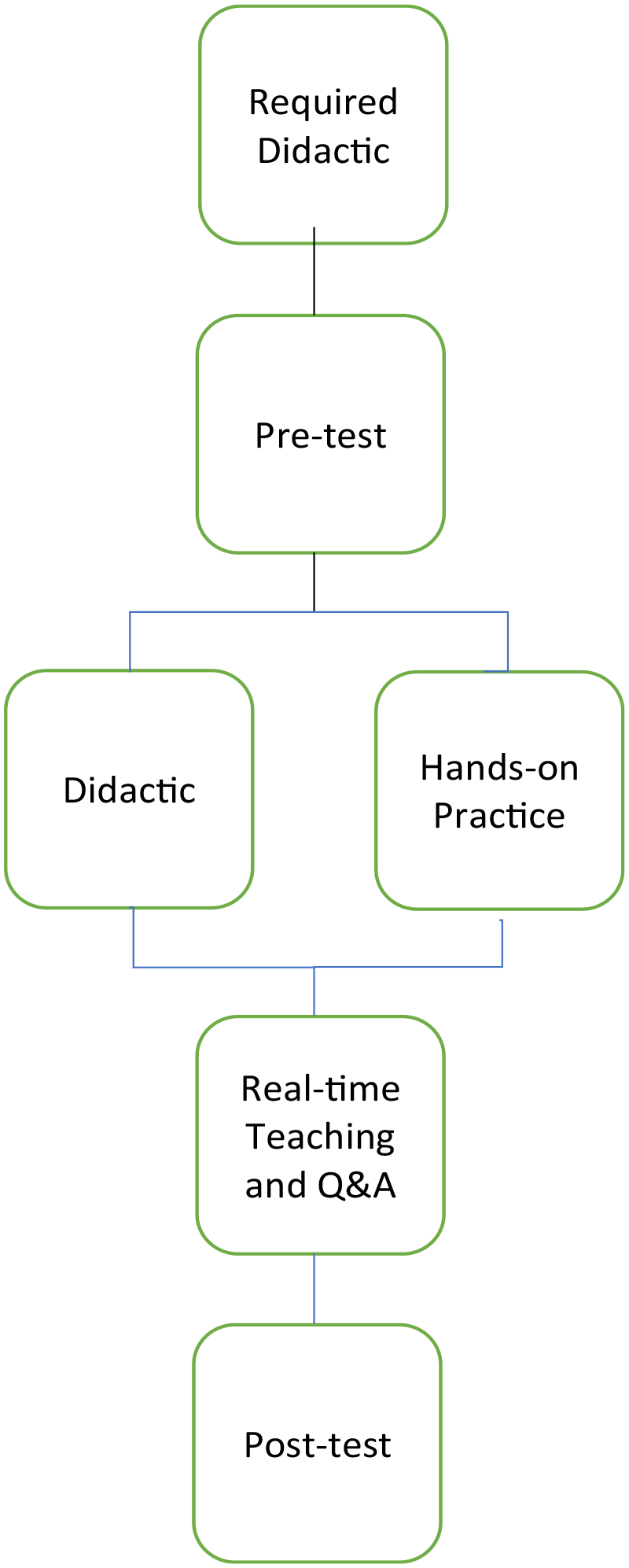
Flow chart of the educational intervention.
Data Analysis
Descriptive statistics are reported. De-identified, paired pre- and post-test differences were analyzed using a paired t-test with IBM SPSS, version 23 (Armonk, NY) and significance was set at P < .05.
Results
Twenty physicians (100%) participated in the intervention and allowed us to analyze their data. Knowledge of Achilles tendinopathy increased (pre-test: 59% correct answers; post-test: 79% correct answers; P < .0001; 95% CI: 6.32-10.78). All partipants demonstrated general proficiency in limited physical examination as observed by the workshop leaders.
Discussion
Overuse injuries such as Achilles tendinopathy are common in ballet dancers. Acute tendinitis may be accompanied by crepitus, localized swelling, and tenderness. While the acute condition may benefit from administration of non-steroidal anti-inflammatory drugs (NSAIDs), and Rest-Ice-Compression-Elevation (RICE), many who present with complaints related to the Achilles tendon have passed this acute injury phase and their tendons have disorganized collagen and other degenerative changes and tissue nodules 9 and the symptoms have become chronic and subject to acute exacerbation.
Although attention to proper technique and optimizing training conditions may reduce the incidence, intrinsic factors, nutrition, as well as the rigors of class, rehearsal, and performance schedules may trigger the condition to flourish in a dance athlete.3,9 -11 Upon discovery of initial symptoms, dancers may choose to “work through” the discomfort in an attempt to maintain physical conditioning and to remain competitive in their professional milieu. They may attempt self-designed remedies until their ability to function at their desired level becomes compromised. At this point, they may seek evaluation from a medical professional. In the current healthcare environment, this often begins with a visit to a PC or EM provider who performs an initial evaluation and recommendation for treatment. It is reasonable to assume that these providers should have an understanding of the dancers’ need for prompt return to training as well as a working knowledge of the evaluation and treatment options for Achilles tendinopathy.
Unfortunately, dance and sports medicine topics are not always a standard part of residency curricula, therefore, generalist physicians such as EM or PC physicians may lack targeted training in the etiology and treatment of conditions that commonly afflict ballet dancers, such as Achilles tendinopathy. For example, the “Model of the Clinical Practice of Emergency Medicine” lists tendon lacerations and Achilles tendon rupture as essential to core knowledge, but tendinopathy is not explicitly listed. 12 Based on our experience, frequent advice from non-specialist physicians to dancers who suffer from overuse injuries may include a recommendation to completely withdraw from the activity for a prolonged period of time or permanently. While this may be a reasonable solution for a casual athlete, it is potentially devastating, for a dancer to comply with this advice. For professional dancers and elite pre-professional dancers, adherence to conditioning and training routines is critical for career maintenance and advancement. After receiving a recommendation for lengthy complete rest, it is possible that the dancer will ignore the mandate for inactivity and continue their self-designed treatment regimen until their condition deteriorates or they have the opportunity to consult with a practitioner whose perspective is aligned with their needs. Continued stress and overuse can lead to progression and worsening of the condition. Thus, it makes sense for the initial treating physician to understand the motivation of the dancer as well as the pathophysiology and treatment of the disease process.
In most cases, complete rest is unnecessary.1,13 Abstaining from training can lead to career setbacks and progression in training, especially since the career in dance performance is time limited. Many exercises can be modified to reduce the strain on the tendon, while still promoting general athletic fitness and maintenance of technique. 14 Modifications to footwear may ameliorate symptoms, such as lessening circumferential constriction when tying pointe shoe ribbons (eg, elastic inserts on ribbons) or wearing appropriate and supportive footwear with or without orthotics when not dancing. Adjunctive physical therapy and dancer education can empower co-management of the disease process and build skill and knowledge in the interest of future injury prevention.
Our data indicate that baseline knowledge of Achilles tendinopathy by generalist physicians is low. While all physicians study anatomy early in medical school, the prevalence of sports medicine focused training may not be a common component of residency training outside the traditional fields of Orthopedic Surgery, Rehabilitative Medicine, and dedicated Sports Medicine fellowships. Common recommendations for treatment of any soft tissue injury (acute or chronic) in the curricula of generalist specialties is RICE (Rest, Ice, Compression, and Elevation) and administration of NSAID’s. 5 While this may be appropriate advice for some acute soft tissue injuries, it is not a definitive cure for chronic overuse injuries in high level athletes.4 -6
After a brief educational intervention, EM and PC physicians demonstrated significantly improved knowledge about Achilles tendinopathy. This can improve their sensitivity to the needs of dance professionals and elite pre-professional trainees who seek initial care for this condition through their mandated medical insurance access to care. After completing the intervention, the physicians who participated were more cognizant about regional anatomy, biomechanics, and the pathophysiology of Achilles tendinopathy and overuse injuries. They understood how to perform a thorough and appropriate evaluation of the Achilles tendon and could then potentially advise dancers on initial rehabilitative measures while awaiting specialty consultation, if deemed necessary. It is unlikely that the generalist physician will serve as the definitive provider for dancers and other elite athletes with debilitating Achilles tendinopathy. However, they can initiate a treatment regimen that extends beyond complete rest in consultation with experts, and can play a key role in arranging timely referrals with specialists for prompt evaluation and the commencement of an appropriate rehabilitative program to professionals who are familiar with the unique needs of dancers.
Our study was conducted at a single institution, so the results may not be generalizable to all physicians. We did not measure longitudinal change in clinical behavior in our subjects when treating injured athletes that may have resulted from our intervention. Future study could involve the development and evaluation of a comprehensive curriculum for EM and PC physicians that aims to provide an overview of basic anatomy, biomechanics, treatment, referral guidelines, and injury prevention strategies for a variety of conditions that commonly affect dancers. This would ultimately benefit the overall health of dancers and their ability to train and perform at the highest possible level.
Practical and Clinical Applications and Implications
Understanding the needs of dancers who suffer from Achilles tendinopathy (as one example) may enhance the understanding of EM and PC physicians of the needs of dancers who have other overuse injuries that preclude their full participation in dance and may lead to earlier referral to physical therapy or another medical specialist who is well versed in dance related conditions. By providing this type of training, generalists may be more likely to consider early referral to physical therapy and adjunctive therapy and may be less likely to advise complete cessation of all dance activity for a prolonged period of time or recommend discontinuation of dance permanently.
Conclusion
A brief educational intervention led to increased knowledge of Achilles tendinopathy in generalist physicians. By increasing awareness of this disease entity through a standard educational model, and teaching strategies for treating and potentially preventing this wide-spread injury, we propose that our curriculum can be portable and accessible to all health care providers who encounter dance athletes who suffer from Achilles tendinopathy.
Supplemental Material
sj-doc-2-dmj-10.1177_1089313X241238814 – Supplemental material for An Achilles Tendinopathy Educational Intervention for Generalist Physicians Raises Awareness and Improves Knowledge for Treating Ballet Dancers
Supplemental material, sj-doc-2-dmj-10.1177_1089313X241238814 for An Achilles Tendinopathy Educational Intervention for Generalist Physicians Raises Awareness and Improves Knowledge for Treating Ballet Dancers by Wendy C. Coates and Leroy Sims in Journal of Dance Medicine & Science
Supplemental Material
sj-pptx-1-dmj-10.1177_1089313X241238814 – Supplemental material for An Achilles Tendinopathy Educational Intervention for Generalist Physicians Raises Awareness and Improves Knowledge for Treating Ballet Dancers
Supplemental material, sj-pptx-1-dmj-10.1177_1089313X241238814 for An Achilles Tendinopathy Educational Intervention for Generalist Physicians Raises Awareness and Improves Knowledge for Treating Ballet Dancers by Wendy C. Coates and Leroy Sims in Journal of Dance Medicine & Science
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.